Fortnightly Review: A rational approach to the management of hepatitis C infection
BMJ 1996; 312 doi: https://doi.org/10.1136/bmj.312.7027.357 (Published 10 February 1996) Cite this as: BMJ 1996;312:357
- G M Dusheiko, reader in medicinea,
- S Khakoo, research fellowa,
- P Soni, South African MRC fellowa,
- L Grellier, British Digestive Foundation research fellowa
- Correspondence to: Dr Dusheiko.
Abstract
Key messages
Summary points
The natural course of chronic hepatitis C is not fully defined
A range of disease exists—from mild asymptomatic infection with few consequences to serious disease with dire sequelae
Pretreatment assessments of viral load and genotype or serotype may help in predicting response
It is difficult to indicate the prognosis for younger patients with mild disease; they may need to be considered for treatment, so that the opportunity to avoid later disease is not forfeited
It is not yet clear whether patients who are more responsive to interferon have a better prognosis
Hepatitis C infection may cause a benign, asymptomatic disorder with an indolent course—but it may also cause progressive liver disease, cirrhosis, and primary liver cancer. The illness has a complex natural course and the ultimate, long term prognosis for patients with chronic hepatitis is difficult to predict. The morbidity is affected by many interactive factors, including age at acquisition, concomitant alcohol abuse, gender, coexisting viral disease, and the host immune response. Several viral factors, including the level of viraemia, hepatitis C virus genotype, and degree of viral diversity, may also affect the rate of progression.
Some patients respond to interferon alfa, and possibly the curtailment of viral replication in responsive patients improves the long term prognosis. It is not easy to chart the prognosis for patients seen at a single visit, however, as the disease progresses at variable rates. This uncertain rate of progression means that the indications for treatment remain undefined. There is no general consensus. Many patients with hepatitis C will not have a durable response to interferon alfa and there is an argument for selecting patients to improve response rates. This strategy may avoid the likelihood of later disease—and, as cirrhosis is irreversible, treating comparatively mild, early disease in younger patients to prevent cirrhosis is a rational objective. This begs the question whether patients who respond to interferon have a better prognosis. But the answer is not yet known and cannot be determined without prolonged prospective study.
We put forward three strategies which could be considered to optimise management and avoid ineffective, inappropriately expensive treatment while avoiding forfeiting the opportunity to treat early and mild disease to prevent progression.
Virology of hepatitis C
Hepatitis C virus is a positive stranded RNA virus of 9379 nucleotides. The gene product is a viral polyprotein precursor of 3011 amino acids. The structural proteins are derived from the 5' end of the genome and non-structural proteins from the 3' end. Hepatitis C virus is classified within the Flaviviridae family but comprises a heterogeneous group of RNA viruses. Current patterns of hepatitis C virus classification are based on genetic relatedness.
The most widely used nomenclature comprises six major genetic groups and a number of recognised subtypes that are more closely related.1 2 The known types have been numbered from 1 and the subtypes a, b, and c in order of discovery. Genotypes 1a, 1b, 2a, 2b, and 3a are the most prevalent in blood donors and patients with chronic hepatitis C from countries in western Europe and the United States. There is a trend for comparatively more frequent infection with type 1b in southern Europe. Epidemiological differences in age distribution of major types and the risk factors associated with particular genotypes have become apparent. In Europe type 3a is comparatively more common in young people with a history of intravenous drug use. Type 1b accounts for most infections in people aged 50 or more. Type 4 infection is the most prevalent in Egypt and many parts of the Middle East and Africa.
There is particular interest in the biological significance of hepatitis C genotypes and in examining the possibility that different genotypes may respond differently to interferon alfa. The complexity of the infecting viral quasispecies in individual patients may also be important.
Diagnosis of hepatitis C
There are still no tests for antigens of hepatitis C virus in serum. Infection is usually diagnosed by detecting hepatitis C virus antibodies based on immunoassay detection of antibody recombinant hepatitis C virus antigens. Commercially available second and third generation immunoassays for hepatitis C antibody are based on detection of antibodies to c100-3 derived from the NS3/NS4 region and other antigens expressed in yeast or Escherichia coli; these include the 22 kDa core protein of hepatitis C virus and a second series of non-structural antigens from the NS3, NS4, and NS5 regions. More recent assays indicate that anti-E2 (antibody to the second envelope protein) is present in most viraemic carriers.3 IgM antibody tests have also been developed, but at present there are no antibody patterns which differentiate persistent viraemia from an episode of resolved viraemia.
The most widely used supplemental tests for confirming antibody to hepatitis C virus are the recombinant immunoblot assay, in which hepatitis C virus structural and non-structural antigens are separately fixed to a nitrocellulose filter, and the matrix assay. Though important for confirming the specificity of a hepatitis C antibody test in blood donors, results of confirmatory tests are almost invariably positive in hepatitis C antibody positive patients with chronic hepatitis.
Supplemental testing may occasionally be required to confirm a hepatitis C antibody positive assay result in a hepatitis C virus RNA negative patient in whom treatment with interferon is contemplated.
Hepatitis C virus RNA
Detection of hepatitis C virus RNA necessitates amplification of the circulating viral RNA by using the principle of the polymerase chain reaction. Polymerase chain reaction primers for the 5' non-coding region are chosen because of relative conservation of this region. Hepatitis C virus RNA is usually but not always detectable in hepatitis C antibody positive patients with abnormal serum alanine and aspartate aminotransferase activities. A small proportion of patients even with advanced disease may have abnormal serum aminotransferase activity but have a negative hepatitis C virus RNA polymerase chain reaction because of intermittent viraemia or a hepatitis C virus concentration below the level of sensitivity of the assay.
Hepatitis C virus RNA, however, can also be found in patients with normal serum alanine aminotransferase activity. Testing for hepatitis C virus RNA is required to distinguish resolved from active infection in hepatitis C antibody positive patients with normal serum aminotransferase activities. Other assays for hepatitis C virus RNA detection, including Amplicor (Roche) and NASBA (nucleic acid amplification system), are being utilised. The usual sensitivity of a nested polymerase chain reaction is 100-1000 copies per ml. A proportion of hepatitis C antibody negative, immunosuppressed, haemodialysed, or agammaglobulinaemic patients with chronic non-A non-B hepatitis may be hepatitis C virus RNA positive.
Quantifying hepatitis C virus RNA
Improved methods of measuring hepatitis C virus concentrations are now more widely used. One method uses oligonucleotide probes complementary to the 5' non-translated region and core regions to capture hepatitis C virus RNA, then branched oligonucleotides to amplify the signal. The detection limit of this assay is 350000 copies per ml. The branched chain DNA assay measures type 1 hepatitis C virus concentrations more efficiently than type 2 or 3, so that differences in serum concentrations of hepatitis C virus RNA in patients infected with type 1, 2, or 3 are probably not significant when the different efficiency of measurement is allowed for. A new version of this assay corrects this variance. Other quantitative methods have been developed, including a biotinylated colorimetric assay, which uses an internal standard in a non-competitive amplification assay (Amplicor monitoring; Roche). The detection limit of this assay is 1000 copies per ml.
Genotyping
Several methods of genotyping have been utilised to group different isolates of hepatitis C virus based on either restriction fragment length polymorphism, type specific polymerase chain reaction, hybridisation to type specific oligonucleotide specific probes, or sequencing. New serotyping assays, based on homologous reaction between type specific antibody in the serum and peptide bound to a solid phase, can detect all six major types by using peptides derived from the NS4 region.
Though an inherently greater pathogenicity of type 1 hepatitis C virus has been implied in patients, these studies have not always been based on follow up or appropriately controlled to account for influences of several interdependent variables and cofactors. Moreover, several clinical investigations have recorded severe and progressive liver disease after infection with each of the well characterised genotypes (1a, 1b, 2a, 2b, 3a, 4a, 5, and 6), so there is little evidence so far for variants of hepatitis C virus that are completely non-pathogenic.
Hepatitis C virus variation and disease
Homologous populations of hepatitis C virus have been observed at the beginning of infection in patients whose later contagion includes a heterogeneous viral population (a quasispecies). In particular, high rates of sequence change have been detected in the hypervariable parts of the genome encoding the envelope glycoproteins. The mechanisms operating to drive these changes and their clinical significance are complex and poorly understood. At least part of the pathogenesis of the disease seems to be jmmune mediated. There may be a correlation between a CD4 T cell response to core and a benign course of infection in viraemic carriers or response to interferon.4
Counselling patients with chronic hepatitis C
Doctors and health care nurses frequently have to counsel patients. A crucial aspect of the care of patients with chronic hepatitis C is to weigh the long natural course of the disease and the risk of cirrhosis against the restricted efficacy of current treatments and the potential for eradicating active hepatitis C infection.
GENERAL ADVICE
Patients with hepatitis C require advice about the natural course of the infection. The doctor should endeavour to establish the duration of the disease, though this is not always possible. A history of intravenous drug use or a blood transfusion in the past is relevant. Patients require information about staging of the disease and should have appropriate assessment by the range of diagnostic tests. The doctor or counsellor should avoid increasing the patient's anxiety without understating the disease and should try to elicit the patient's concerns. The patient may need to be informed briefly of the chronology of the disease, including the dates of discovery of the virus (1988-9), the development of diagnostic tests, and measures to eliminate hepatitis C virus from the blood supply and factor concentrates. Patients with coexistent hepatitis B or HIV are a particular problem.
The salient features of serum alanine aminotransferase measurements, antibody tests, hepatitis C virus RNA, genotypes, and hepatitis C virus RNA concentrations should be explained in simple terms. It should be pointed out that the infection is usually monitored by serum alanine aminotransferase measurements, but the problems associated with assessing the disease by this route alone require explanation. The indications for liver biopsy and its possible risks and discomfort must be explained. Informed patients in many centres are confused by the fact that genotyping or serotyping and quantitative RNA measurement are not routinely available.
Young patients without clinical evidence of cirrhosis should be told of the generally indolent nature of the infection and that they have many decades of productive life ahead. Patients should be advised of the different indications for treatment with interferon alfa and the physician should review details of the subcutaneous route of administration, duration of treatment, and factors that are believed to enhance or negate response; give a realistic appraisal of sustained response rates; and describe the side effects and clinical monitoring of treatment. It is important that patients should become partners to the decision to treat. They can also be informed about national trials in progress. There are no consensus data to assess mortgage and life insurance risk, but patients can be informed that they are insurable, if with a possible weighting.
ALCOHOL
There is evidence that alcohol and hepatitis C may synergistically aggravate hepatic injury, and drinking excess alcohol is therefore discouraged.5 6 A minimum safe level has not been established; small amounts of alcohol would not be considered inadvisable for patients with mild chronic hepatitis.
TRANSMISSION AND INFECTIVITY
Specific questions are often asked about the transmissibility of hepatitis C. The patient should be advised not to donate blood. Patients can be told that the parenteral route is the most important route of transmission and that the virus is not easily transmitted by any other route. The route of infection can be difficult to ascertain in up to a third of patients. The precise mechanism of much community acquired disease is uncertain, but transmission by injection or medical treatments—for example, of schistosomiasis—and possibly dental treatments may plausibly have increased the pool of infected patients in southern Europe and Egypt.7 Transmission in saliva (or saliva containing blood) and by a human bite has been reported.8
There are no vaccines available to protect contacts of patients with hepatitis C. However, secondary transmission should be fairly easy to prevent. The role of intrafamilial transmission requires clarification but is comparatively rare. Simple precautions to prevent inadvertent and inapparent parenteral transmission include avoiding sharing razors and toothbrushes and carefully bandaging cuts and wounds.
SEXUAL TRANSMISSION
Sexual transmission has been described but is a comparatively inefficient and infrequent route. The overall hepatitis C virus infection rate is higher in sexually promiscuous groups. In northern European societies most sexual partners of hepatitis C antibody positive people test negative for the antibody. Transmission may be more likely after prolonged contact with patients who have high levels of viraemia—for example, those who are both HIV and hepatitis C antibody positive.9
It is prudent to test regular sexual partners for hepatitis C antibody but to advise that the risk of transmission is low. There is no logic for couples in longstanding relationships to begin barrier sexual practices after the diagnosis. Hepatitis C virus has been found in menstrual blood and sexual contact should be precluded for several days after menstruation. Young adults who are sexually active could be told of the advisability of using condoms for all casual sexual contact.
MOTHER TO INFANT TRANSMISSION
Mother to infant transmission of hepatitis C virus has been recorded but seems to be unusual. Differences in the rate of maternal-infant transmission between different countries remain unexplained, and the importance of this route in perpetuating the reservoir of human infection is unknown, though it could be relevant. Maternal-infant transmission is more likely in mothers with hepatitis C virus RNA concentrations higher than 107 genomes per ml. Though patients should be informed of the fairly low risk of transmission, it should be explained to those wanting children that perinatal transmission cannot categorically be excluded. The risk may be determined by the level of viraemia, but other factors could be involved. Couples can make an informed decision in the light of the available data and subsequent litigation therefore avoided. Though hepatitis C virus RNA has been found in breast milk, infection of infants by breast feeding has not been reported. Persistent hepatitis C virus RNA has been found in the absence of hepatitis C antibody in newborn babies of antibody positive women, suggesting the possibility of seronegative hepatitis C virus infection.10 11 12 This observation requires careful validation.
Surgeons and other health care professionals
Transmission of hepatitis C virus from infected surgeons to patients has been verified by molecular epidemiological evidence. It is unknown whether higher levels of viraemia and particular forms of surgery are associated with a greater likelihood of transmission. In Britain and the United States surgeons and obstetricians (and presumably also phlebotomists and nurses) are allowed to continue unrestricted practice unless they have been shown to have transmitted infection to a patient. The rationale of this policy is likely to be challenged soon. Is advice on double gloving for infected surgeons enough? Probably more reports will emerge as awareness increases. Surgeons should know that these guidelines may not protect against litigation should they be implicated in transmitting hepatitis C; hence they should seek written assistance from their occupational health physicians and medical defence unions. Antiviral therapy may be effective in reducing viraemia, which could prevent loss of their livelihood.
Interferon alfa ACUTE HEPATITIS C
Acute icteric hepatitis C has become comparatively rare in northern Europe. The acute course of hepatitis C virus infection is clinically mild and often inapparent. Subclinical disease is common. Only one quarter of cases are icteric, and the peak serum alanine aminotransferase activities are less than those in acute hepatitis A or B. The mean incubation period of hepatitis C is 6-12 weeks. During the early clinical phase the serum alanine aminotransferase activity may fluctuate and may become normal or near normal, making the determination of true convalescence difficult. Diagnosis in these cases requires confirmation by hepatitis C virus RNA testing. Severe or fulminant hepatitis C is rare but may occur, particularly in leukaemia and in patients with transplants after withdrawal of chemotherapy.
Treatment of chronic hepatitis C with interferon alfa
Advantages
Inhibits hepatitis C virus replication in some patients with chronic disease
Sustained response in some patients
Important component of combined antiviral treatment
Can improve histological hepatitis
Disadvantages
Given by injection
Low sustained response rates in many patients with type 1 hepatitis and higher levels of viraemia
High relapse rates
Side effects
Neutralising antibodies in some patients
Relative expense
Treatment
Serum aminotransferase activities decline from the peaks encountered in the acute phase of the disease but remain two to eight times normal. They should be measured periodically (monthly to three monthly). If the patient remains viraemic with raised serum alanine aminotransferase activity treatment is indicated. The decision to treat patients with normal serum alanine aminotransferase activity who remain viraemic is more difficult and possibly should be based on biopsy findings as well as the likelihood of response. Several therapeutic trials of interferon alfa for acute hepatitis C have been completed. Most indicate that amelioration of the severity of the chronic hepatitis lesion or even a reduction in the rate of chronic disease is possible with at least six months of treatment. Thus if a diagnosis can be made and the patient does not seem to be convalescing two to four months after the onset of infection interferon alfa can be considered at a dose of 3-6 MU three times weekly for at least six months.
CHRONIC HEPATITIS C
Most patients with chronic hepatitis C are asymptomatic or only mildly symptomatic. Fatigue is the most common complaint. Most patients do not give a history of acute hepatitis or jaundice. There may be no abnormal physical findings. With more severe disease spider angiomas, palmar erythema, hepatomegaly, and systemic manifestations of hepatitis C—for example, cryoglobulinaemia—may be found. Serum alanine aminotransferase activity may fluctuate over time and may even be intermittently normal. Other patients have a sustained increase in serum aminotransferase activities. With the development of cirrhosis an enlarged liver and spleen may be evident and weakness, wasting, oedema, ascites, and variceal haemorrhage become progressive problems. Older patients may present for the first time with complications of cirrhosis or even hepatocellular carcinoma.
Approach when hepatitis C virus RNA testing is not available
When hepatitis C virus RNA testing is not available the minimalist scheme for treatment suggested in figure 1 may suffice. If the serum alanine aminotransferase activity is normal the patient should be monitored for one to three months to assess the trend in activity. However, viraemia is not uncommonly found in patients with normal enzyme activity and it is not possible to distinguish persistent from resolved infection unless hepatitis C virus RNA can be tested (fig 1).

Approach to treatment if hepatitis C virus RNA testing is not available
{kind=link}
With use of this minimalist approach patients with raised serum alanine aminotransferase activity and chronic hepatitis could be considered for antiviral therapy. Serum aminotransferase activities, bilirubin concentration, alkaline phosphatase activity, and prothrombin time should be measured. In patients whose lifestyle or geographic origin suggests that they are at risk of other viral infections hepatitis B surface antigen and HIV infection should also be considered. In equivocal cases the diagnosis of chronic hepatitis C may still require confirmation and careful exclusion of all other causes of raised serum alanine aminotransferase activity, including obesity, alcoholism, inborn errors of metabolism, drug induced hepatotoxicity, and disease of the biliary tract.
Because autoimmune hepatitis is treated differently it is particularly advisable to exclude this diagnosis by excluding from treatment patients with high titres of smooth muscle or liver and kidney microsomal antibodies. The dividing line between this disease and chronic hepatitis C is not always clear, as a high proportion of patients with hepatitis C have low titres of smooth muscle and antinuclear antibodies.13 14 15 Thyroid disease must be excluded by measuring thyroxine and thyroid stimulating hormone concentrations and antithyroid antibodies.
Patients can be managed or even given antiviral therapy without a liver biopsy. However, this leaves several questions unanswered, as there is currently no substitute for liver biopsy to ascertain the grade (severity and extent of hepatic inflammation) or stage (fibrosis) of the disease. Asymptomatic cirrhosis may be present.
A characteristic histological pattern of mild chronic hepatitis with portal lymphoid follicles and varying degrees of lobular activity is found in many patients. Serum alanine aminotransferase activity is used to assess response, and if values have not become normal in two or possibly three months, then treatment is stopped. Most responsive patients will have responded within this period. Large placebo controlled studies indicate that around half of patients have normal serum aminotransferase activities after six months of interferon alfa 3 MU three times a week.16 17 After treatment for six months half of the initial responders will promptly relapse. Some 15-20% of unselected patient have a prolonged biochemical response to treatment and do not relapse when interferon is stopped.18 Patients should be monitored every one to four weeks during treatment and have their blood counts and serum aminotransferase activities measured at these intervals. Thyroid function values should be measured before, during, and at the end of treatment.19 20 21 22
The patterns of response vary. Some patients may have a partial response with improvement but not return to normal of serum aminotransferase activities. A proportion of patients may show a good initial response to treatment but then have an increase in serum alanine aminotransferase activity again despite continuing treatment. Possibly some of these patients develop neutralising interferon antibodies or interferon resistance. A proportion of patients with chronic hepatitis C have chronic disease with features of autoimmune hepatitis which is provoked by interferon alfa. This phenomenon is unusual and not common enough to suggest that hepatitis C is an autoimmune disease or that corticosteroids are a first line treatment for hepatitis C. HLA typing may indicate this predisposition.15
Approach when hepatitis C virus RNA testing is available
A more comprehensive approach to treatment should use hepatitis C virus RNA to define patients with normal serum alanine aminotransferase activity who are none the less viraemic to monitor antiviral therapy and measure virological response (fig 2). Thus liver biopsy should be considered in patients with raised serum aminotransferase activity or a positive hepatitis C virus RNA test result; this second group of patients may have accrued appreciable liver damage but have intermittently abnormal alanine aminotransferase values. Liver biopsy may help to optimise the dose and judge a virological response to treatment.
Serum hepatitis C virus RNA may become undetectable in patients who have normal aminotransferase activities after four to eight weeks of interferon alfa. Serum aminotransferase activities usually relapse in patients who remain hepatitis C virus RNA positive at the end of treatment—but some patients may remain positive for a period despite normal serum aminotransferase values. Undetectable hepatitis C virus RNA at the end of treatment does not preclude a relapse in serum aminotransferase activity in patients after stopping interferon, but it lessens this probability.23 24
The sensitivity of tests for hepatitis C virus RNA is an issue which requires more careful standardisation than is applied at present. There are inadequate data to indicate (a) whether patients with normal aminotransferase activities and negative for hepatitis C virus RNA at six months should continue treatment to prevent relapse (probably) and (b) whether patients with normal aminotransferase activities and positive for hepatitis C virus RNA at six months will become negative for hepatitis C virus RNA if treatment is extended beyond six months (unlikely). The logic of individually tailoring the antiviral dose to the level of viraemia or adapting the dose of interferon to hepatitis C virus RNA status after eight weeks is being tested.25
Measures to improve responsiveness to interferon alfa need consideration. It is not certain whether initiating treatment with 3 MU is optimal. Longer treatments or induction with a higher dose (5-6 MU) may be more effective, as there is evidence for dose responsiveness. Prolonging treatment for a year or longer results in lower relapse rates.26 However, relapses still occur after higher doses and patients have more side effects at higher doses. Giving a second course of treatment with a different interferon may be useful in some patients.
Approach when hepatitis C virus RNA measurement and genotyping or serotyping are available
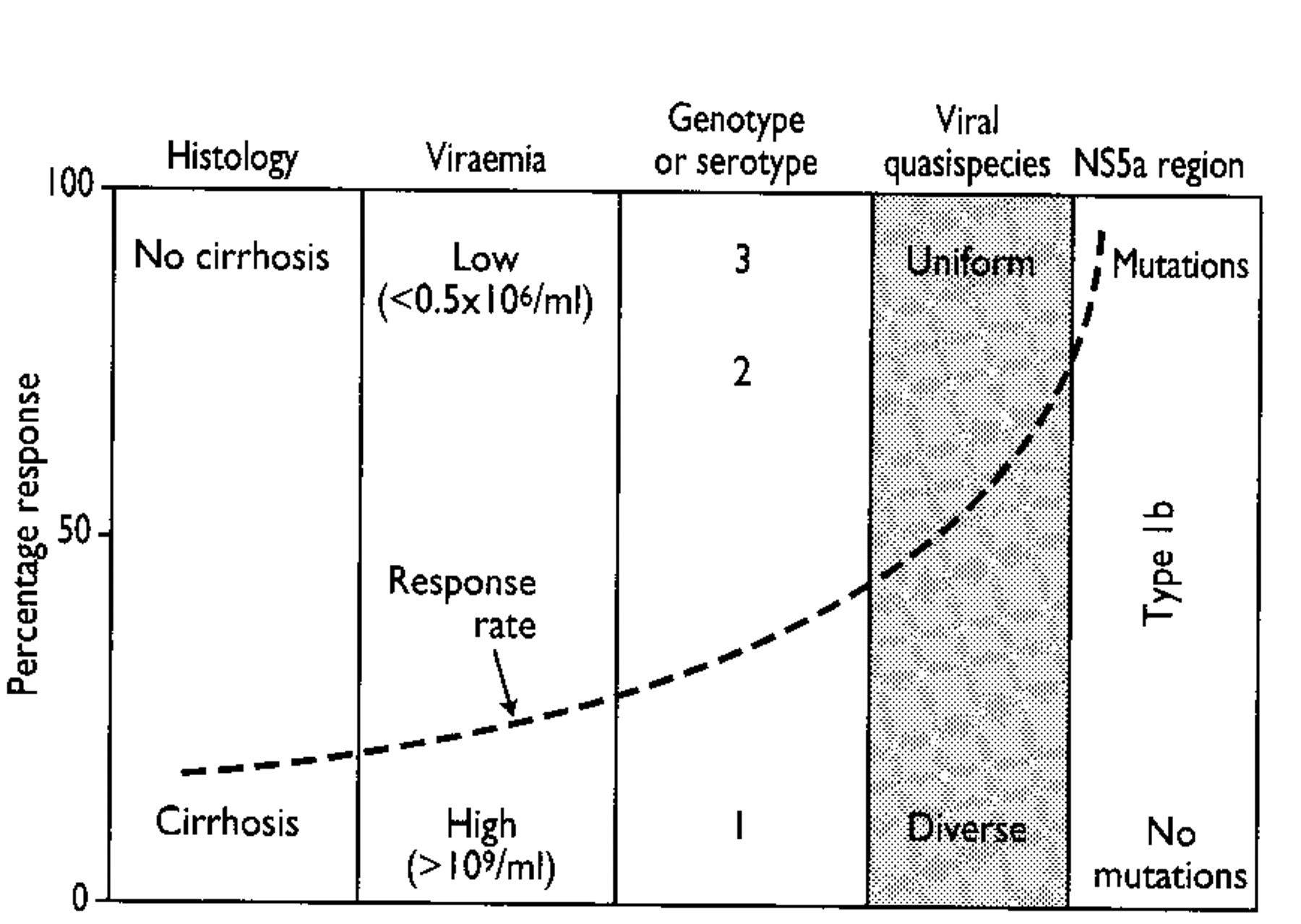
Because long term response rates to treatment have been disappointing, a third approach could be to improve response rates by categorising patients as “good” or “poor” responders according to the known host and viral determinants of response to interferon. This approach is shown in figure 3. Several workers have suggested that patients with types 2 and 3 infection are more likely to have a sustained response to treatment than patients with type 1 (and possibly type 4).27 Types 1a and 1b infection are equally resistant to interferon. Long term responses are also higher in patients with lower circulating levels of virus measured by branched chain DNA assay or competitive polymerase chain reaction.28 29 Patients with fewer than 106 copies of hepatitis C virus RNA per ml are more likely to sustain responses (though the precise cut off has not been determined). Within genotypes response rates may be higher for patients with lower virus concentrations and less advanced disease. Younger patients and patients without fibrosis or cirrhosis are also more responsive to treatment.30 The mechanisms by which different genotypes might differ in responsiveness to treatment remain obscure.

Approach to treatment if hepatitis C virus RNA measurement and genotyping or serotyping are available
{kind=link}
With this approach the patient's genotype or serotype and level of viraemia should be measured before considering treatment. As subtypes are not important, serotyping will suffice for most patients. Patients in the good response group could be offered interferon alfa. Treatment for one year should be considered to reduce relapse rates. Patients in the poor response group require a different or additional treatment—for example, within a trial of combination antiviral agents. Though emerging evidence implies that genotyping or serotyping and measurement of viraemia may become a necessary part of the pretreatment assessment of patients, we are not yet at a point at which interferon can be proscribed for patients with type 1 infection, except possibly in older patients with advanced cirrhosis. However, patients should at least be forewarned that response rates in this group in previous trials have been low.
Higher sustained response rates should be the objective, and selection of patients will improve treatment results. This approach thereby applies evidence based treatment to obviate future disease and prioritise the provision of interferon alfa. The known data have significant microeconomic and macroeconomic consequences. The issue remains complex, as the improved responsiveness in patients with lower viral loads begs the question of whether these patients ultimately have less severe disease. This cannot be answered now, but it is correct to point out that the prevalence of cirrhosis is not significantly different in patients with types 1 and 4 versus types 2 and 3 hepatitis C and there are no completely non-pathogenic genotypes of hepatitis C. New research is needed to concentrate on bettering responsiveness in demonstrably unresponsive patients.
Importantly, patients with normal serum alanine aminotransferase activities before treatment may develop an exacerbation after failed interferon treatment. The mechanism is unknown but could be a result of displacement of interferon sensitive clones. There is thus good reason for selecting responsive patients if patients with normal serum alanine aminotransferase activity (but who are hepatitis C virus RNA positive with chronic hepatitis) are to be considered for treatment.
Patients with homogenous circulating quasispecies are also more likely to respond to treatment. Though this has been incompletely studied, in some cases it mirrors a shorter duration of infection. Recent molecular evidence indicates that an interferon sensitive region can be defined in the NS5a region in patients with type 1b infection. Patients with more amino acid mutations in the NS5a gene (region 2209-2248) were more likely to have a complete response than patients with wild type 1b (fig 4).31
Nomogram indicating likelihood of sustained response to interferon alfa. Type 1b infected patients with more amino acid changes in NS5a region are more likely to respond. Hepatitis C virus concentrations associated with response are 10-fold lower when measured by Amplicor monitoring assay (5x104)
{kind=link}
When can treatment be considered successful? Accepted criteria have not been established, but it is reasonable to infer that patients with normal serum alanine aminotransferase activity and negative for hepatitis C virus RNA a year after stopping interferon, with histologically improved disease activity, have had a meaningful response. Responsive patients usually exhibit histological improvement, and sustained clearance of hepatitis C virus RNA is the most likely outcome to have tangible benefit in patients who have not developed cirrhosis. The potential benefit of maintenance treatment for patients who respond but relapse after stopping treatment is being examined.
A recent report has suggested that histological improvement can be observed in treated patients in the absence of a biochemical response.32 This effect could be the result of a separate anti-inflammatory and antifibrogenic effect of interferon alfa but requires confirmation of long term benefit before it could be considered an objective of interferon treatment.
Interferon for cirrhosis
Patients are at risk of sequelae once cirrhosis has developed. Hence treatment with interferon alfa should be targeted to patients before cirrhosis occurs. Recently, several small trials have suggested that interferon improves liver function and reduces the incidence of hepatocellular carcinoma in patients with cirrhosis due to hepatitis B or C.33 There are reservations about the conclusions drawn from this limited experience. There is little information regarding potentially injurious exacerbations of the hepatitis C (or B) after transient suppression in patients given intermittent treatment. There is also little information regarding the toxicity of interferon in patients with advanced liver disease; dose-response studies have not been completed. None the less, this could be a potentially important treatment if the antiproliferative, antifibrogenic, and immunomodulatory properties of interferon alfa can be proved to play a part in preventing malignant transformation. Though these data are interesting, further trials are necessary before advising this measure.
Treatment of other special groups
The treatment of special groups, including children, patients with systemic manifestations, patients having renal dialysis, HIV positive patients, and patients with transplants, is beyond the scope of this article. These patients are often difficult to treat, but sustained responses can occur. Cirrhosis due to hepatitis C has become an important indication for liver transplantation, and the number of patients given transplants for decompensated hepatic disease has increased in the past five years. It has become apparent that recurrence of hepatitis C virus infection is almost universal. Thus though the recurrence is usually associated with comparatively mild disease, follow up of these patients has been short, and severe sequelae, including cirrhosis, may become more common with time. The most promising treatments are ribavirin and interferon used together.
Side effects of interferon alfa
Early
Flu-like illness, chills, fever, malaise, muscle aches, headache
Poor appetite
Later—common
Weight loss
Increased need for sleep
Psychological side effects (irritability, anxiety, depression)
Hair loss
Thrombocytopenia, leucopenia
Unusual or severe
Seizures
Acute psychosis
Bacterial infections
Autoimmune reactions
Hyperthyroidism or hypothyroidism or transient thyroiditis
Rare
Proteinuria
Myocardiopathy
Rashes
Interstitial lung disease
Retinal changes
Ototoxicity
Ribavirin and combination antiviral therapy
Ribavirin is an oral guanosine analogue.34 There have been several multicentre trials of ribavirin for hepatitis C. Though the drug suppresses serum alanine aminotransferase activity in chronic hepatitis C, it has little antiviral activity and is associated with mild haemolytic anaemia.35 Recent small trials of interferon alfa combined with ribavirin have suggested that higher sustained responses occur with the combination.36 The mechanism of this synergy is unknown, but trials being conducted world wide should be completed in 1996 and 1997. Combination therapy may improve response rates and reduce relapse rates in transient responders. It is not clear whether poor responders—that is, patients with high levels of viraemia and genotype 1—will respond well to this combination. The main reported side effects of ribavirin include haemolytic anaemia, metallic taste, dry mouth, flatulence, dyspepsia, nausea, headache, irritability, emotional lability, fatigue, insomnia, rashes, and myalgia. Mild reversible anaemia is common. Modest increases in urate have been reported. The interactive toxicity of ribavirin and interferon also needs further study.
Other treatments
Several agents have been utilised in addition to other interferons, such as consensus interferon and interferon beta. Ancillary treatments include ursodeoxycholic acid,37 38 non-steroidal anti-inflammatory agents, N-acetyl cysteine,39 iron depletion,40 41 42 43 44 and interferon and thymosin. Though improvement in serum alanine aminotransferase activity can result with these treatments, the long term benefit of these strategies is unknown.
Patients who do not respond to treatment present a difficult management problem. For these patients better antiviral agents will be required. Several new compounds to meet this need are being developed. The focus of these programmes is to produce drugs to inhibit enzymes of hepatitis C virus replication (serine protease, helicase, or polymerase inhibitors) or to inhibit hepatitis C virus translation. The screening of new drugs will be greatly facilitated by growing hepatitis C in tissue culture. It will be years before these compounds enter phase III trials. Suppressive treatment will be the likely goal with these agents. In the interim “curative” treatment with interferon alfa can be achieved in some patients.
Vaccine development is proceeding. The main antigenic differences in hepatitis C, particularly in the envelope region, mean that a polyvalent vaccine will be required. Core E1, E2, and NS2 genes have been expressed in a recombinant vaccinia vector to infect HeLa cells and the extracted glycated E1 and E2 proteins used to vaccinate chimpanzees. More cross challenge and isolate specific experiments will be required. Injection of naked DNA generates antiger for presentation by major histocompatibility complexes and a CD8 T cell response. This approach has been explored in several different models.