Article Text

Abstract
Several features of the irritable bowel syndrome (IBS) suggest involvement of the emotional limbic system in the brain. Abnormalities which upregulate afferent (sensory) signal intensity anywhere in this system, from the gastrointestinal tract to the brain, could induce hypersensitivity, leading to the pain and discomfort that characterise IBS and other functional disorders. Functional gastrointestinal disorders are likely to be heterogeneous given the complexity of the afferent system, and a number of different perturbations are possible. Intestinal hypersensitivity to pain and discomfort and associated reflex alterations in motility might explain the symptoms of functional bowel diseases.
- irritable bowel syndrome
- anterior cingulate nucleus
- thalamic pathways
- dorsal horn neurones
- ACC, anterior cingulate cortex
- CNS, central nervous system
- CRF, corticotrophin releasing factor
- DRG, dorsal root ganglia
- FMRI, functional magnetic resonance imaging
- IBS, irritable bowel syndrome
- PET, positron emission tomography
Statistics from Altmetric.com
- ACC, anterior cingulate cortex
- CNS, central nervous system
- CRF, corticotrophin releasing factor
- DRG, dorsal root ganglia
- FMRI, functional magnetic resonance imaging
- IBS, irritable bowel syndrome
- PET, positron emission tomography
SUMMARY
Several features of the irritable bowel syndrome (IBS) suggest involvement of the brain's emotional limbic system: higher prevalence of anxiety and psychosocial stressors, augmented intestinal stress responses, and response to centrally acting medication. Recent brain imaging data suggest pathways involved in visceral pain perception overlap with limbic pathways, which may explain how psychological factors interact with IBS. Intestinal discomfort reaches awareness via neural connections termed the “brain-gut axis”. Abnormalities which upregulate afferent (sensory) signal intensity anywhere in this system could induce hypersensitivity, pain, and discomfort. These include stimulus amplification in the intestinal tract prior to the primary afferent nerve or hyperresponsiveness of the afferent nerve itself. Abnormalities in the dorsal horn of the spinal cord may explain the widened viscerosomatic referral patterns seen in IBS. Descending mechanisms of pain inhibition may also be compromised. Impaired endogenous opiate mediated inhibition of the primary afferent nerve could fail to suppress afferent messages from the gastrointestinal tract. In the brain, increased thalamic activation has been seen in IBS which could indicate increased afferent output from lower levels. Activation of the anterior cingulate cortex, the limbic centre that encodes pain suffering, appears to be enhanced in IBS, especially under the influence of anxiety. Psychological factors could augment pain processing at the anterior cingulate, the area of convergence of the pain and emotional systems. Factors which upregulate gut sensitivity are also likely to affect motility, either by augmented central autonomic outflow or peripheral sensory-motor reflexes.
INTRODUCTION
Gastrointestinal sensory disorders are commonly referred to as gastrointestinal motility disorders or functional gastrointestinal disorders. Over stimulation of the sensory limb of the multiple sensorimotor reflexes that exist in the gastrointestinal tract triggers a motor response, and for this reason sensory abnormalities often coexist with motor disturbances. Both sensory and autonomic control of gastrointestinal motility are thought to be modulated by the central nervous system (CNS).
IBS is the most commonly encountered functional gastrointestinal disorder. It is characterised by symptoms, defined by the Manning and Rome criteria, which are accompanied by hypersensitivity to distension of the rectum, colon, and small intestine, abnormal motor patterns in the small and large intestine, and increased intestinal reactivity to psychosocial stressors.1–5 There is a notable increase in the prevalence of significant psychosocial stressors among patients with IBS who seek medical care.6
The other two relatively common functional gastrointestinal disorders are functional dyspepsia and non-cardiac chest pain. These disorders share the same motor, sensory, and psychosocial patterns described for IBS. It is not surprising therefore that some patients have symptoms of more than one of these disorders at one time, switch from one disorder to another over time, and some have visceral hypersensitivity in multiple organs at the same time.7
SENSORY FEATURES OF FUNCTIONAL GASTROINTESTINAL DISORDERS
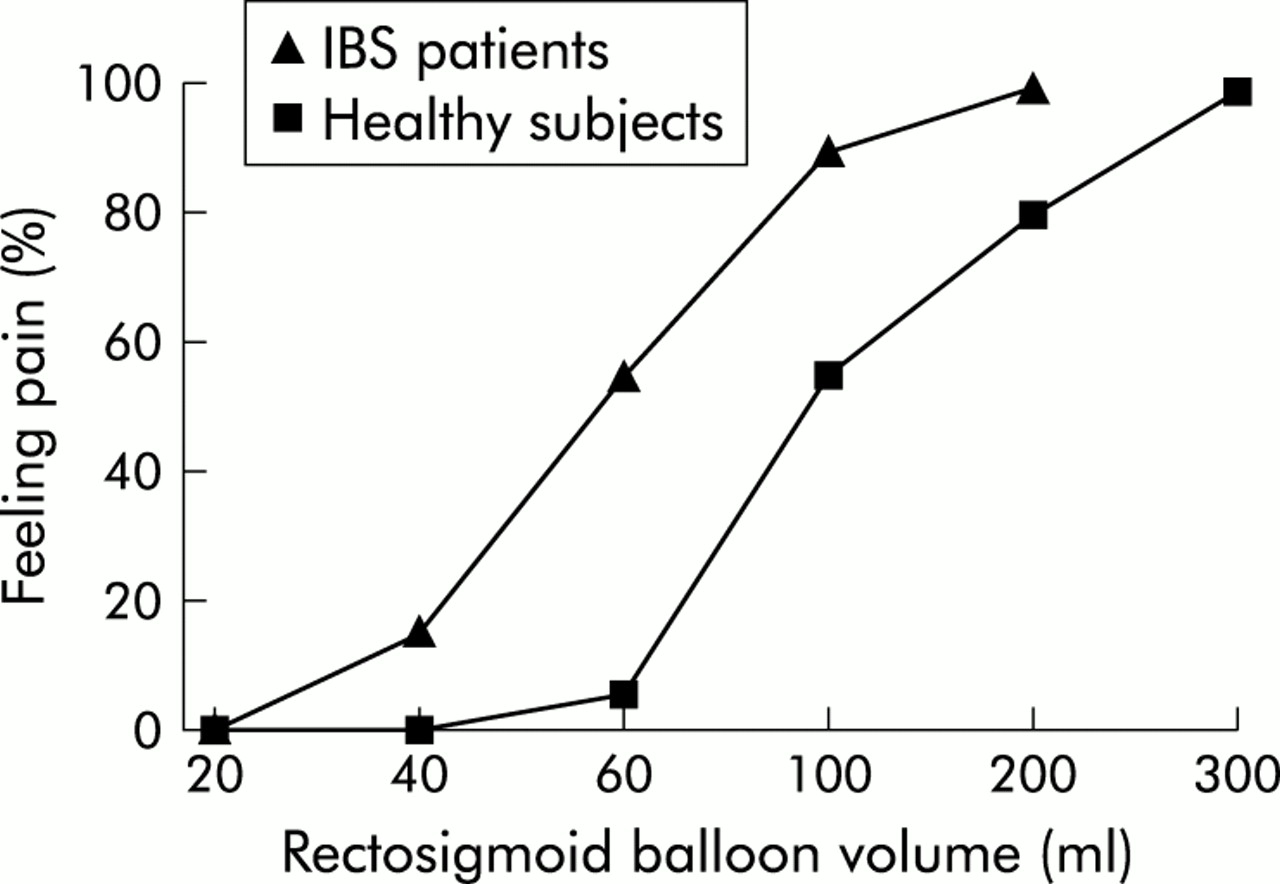
Hypersensitivity to visceral distension has been widely demonstrated in IBS (fig 1).3,4,8,9 The hypersensitivity appears relatively specific for pain and discomfort rather than for non-noxious sensations such as stool and gas, and is seen whether measured by volume of distension, pressure of distension, or wall tension.3 Rapid phasic distension is more likely to detect intestinal hypersensitivity than gradual distension.
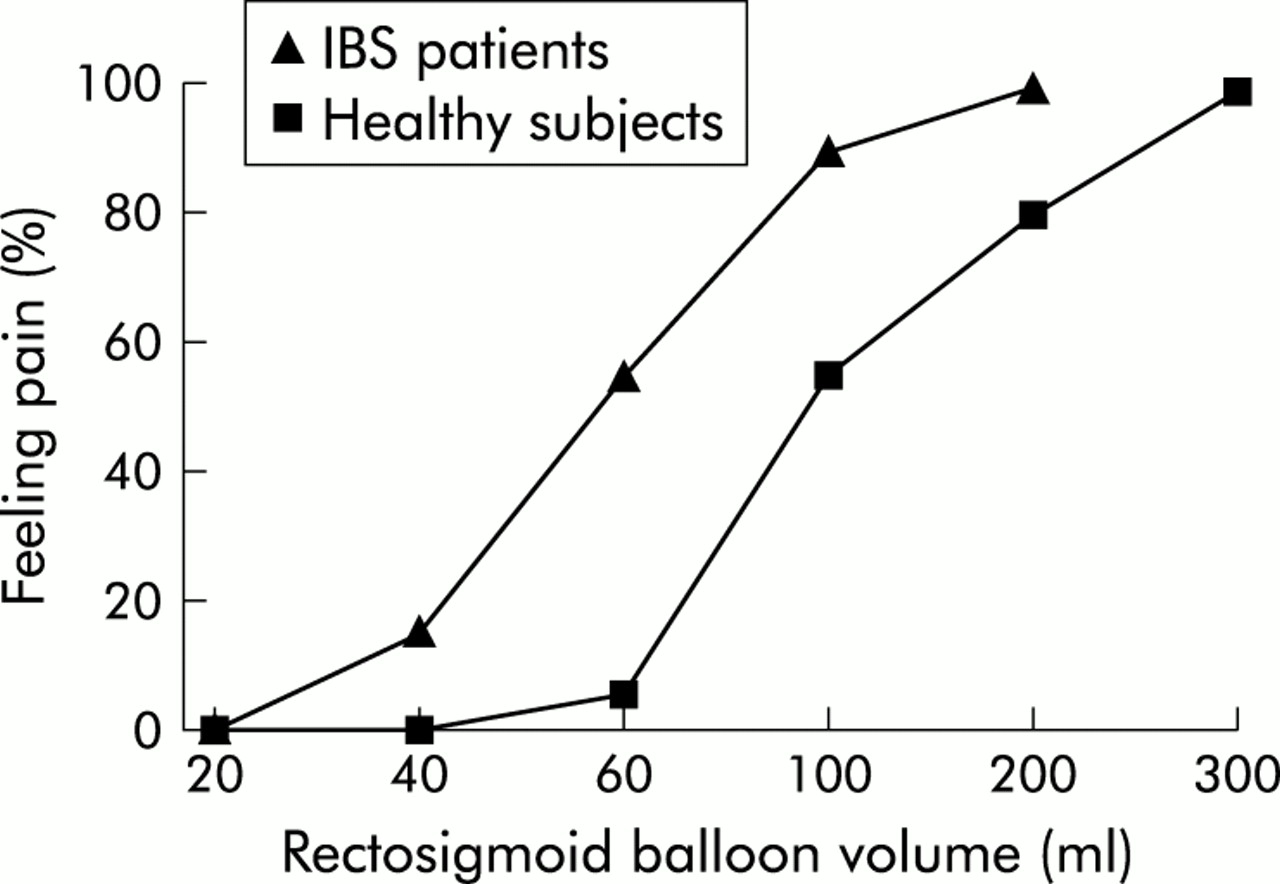
Comparison of hypersensitivity in patients with irritable bowel syndrome (IBS) and healthy subjects.
While some investigators have suggested that response bias and selective attention to intestinal sensation account for hypersensitivity in IBS, a study which carefully sought to exclude these biases found low pain thresholds in half of the subjects with IBS.10 Patients with functional dyspepsia and non-cardiac chest pain also report pain at lower pressures and volumes than healthy controls, or disease controls who suffer from non-functional upper abdominal pain.11,12
Intestinal sensation is, in general, less localised than somatic sensation. Referral of intestinal sensation to somatic dermatomes occurs when there is colocalisation of visceral and somatic afferent terminals in the same spinal cord dorsal horn lamina. Rectal distension induces sensations in the rectal and suprapubic areas of healthy volunteers. In patients with IBS, it induces sensations which are more widespread involving both rectal and suprapubic areas, as well as a variety of more superior abdominal dermatomes (fig 2).3 These abnormalities are also found in patients with functional dyspepsia.12,13

Sensation of pain induced by rectal distension is more widespread in patients with irritable bowel syndrome (IBS) compared with healthy (control) subjects.
In one study, sensory abnormalities, either low pressures for reporting initial pain or discomfort or aberrant viscerosomatic referral patterns, were seen in 93 of 100 patients with IBS. Those who did not have hypersensitivity (approximately one third) described the sensations induced at each distending pressure as being more intense than those of controls. Some of these patients returned for subsequent rectal sensitivity testing. This group of patients were asked to record symptom severity on each testing day. The study showed that there was a significant correlation between change in symptoms over time and change in lowest pressure inducing pain.3 Given the high prevalence of sensory abnormalities in IBS, and the correlation of sensitivity with symptoms, sensory abnormalities may be considered to be a biological marker of the disorder. Similar findings in the oesophagus and stomach of patients with non-cardiac chest pain and functional dyspepsia suggest that these disorders are very similar, and may even be variable presentations of the same disorder.
However, the exact causes or triggers of intestinal hypersensitivity are unknown; infections, stresses, and surgical procedures all play a role. Repetitive painful distension of the sigmoid colon in patients with IBS has been found to induce even lower pain thresholds during subsequent rectal distension testing. This form of sensitisation is not seen in normal volunteers.14 It is possible therefore that patients with IBS are more prone than normal subjects to neural “wind up” by noxious stimuli, such as intestinal spasm or distension. Psychosocial stressors may also induce hypersensitivity in these subjects.
PSYCHOLOGICAL FEATURES OF FUNCTIONAL GASTROINTESTINAL DISORDERS
There is a clear increase in the prevalence of current psychological distress among patients who seek medical care for IBS. Symptoms of anxiety, depression, and global psychological symptoms are commonly encountered in this population, and several studies have demonstrated higher levels of physical and sexual abuse among IBS patients compared with patients in other medical clinics.15,16 Patients with IBS who do not present for care generally have a normal psychological profile, although some surveys show increased psychosocial distress of intermediate severity.6,17
Certainly, practitioners are familiar with many patients who present with functional bowel illness due to increased symptom severity which corresponds well to acute psychosocial stressors. It is also recognised that symptoms often remit as the psychosocial stress is improved, and persist if stressors persist.18 Similar findings have been described in patients with functional dyspepsia.
However, psychosocial stressors also acutely affect gastrointestinal motility and sensation in control subjects without IBS. Volunteers experience altered gastrointestinal motor function during periods of stress, whether it be dichotomous listening tasks, driving in traffic, or fear of cancer.19,20 Dichotomous listening tasks designed to be stressful also increase the sensitivity of the colon to balloon distension in normal volunteers compared with relaxing music.21 It is conceivable therefore that patients with IBS “over respond” to psychological stressors. One study in patients with IBS demonstrated an increase in psychological as well as colonic motor response to criticism and delay.5
It is possible therefore that chronic or severe stress may result in long lasting changes in the CNS which themselves provoke the symptoms of IBS. In animal models, infant-maternal separation and electrical shock stress create chronic colonic hypersensitivity and hypercontractility resulting in diarrhoea.22,23 As patients with IBS are known to have a higher than normal prevalence of past or current physical and sexual abuse, it can be postulated that severe stress such as sexual abuse has the potential to induce chronic visceral hypersensitivity and anxiety.
BRAIN-GUT PATHWAYS THAT MAY MEDIATE VISCERAL HYPERSENSITIVITY IN GASTROINTESTINAL SENSORY DISORDERS
The gastrointestinal tract has a dual sensory innervation comprising the vagal/sacral or parasympathetic system and the spinal afferents traditionally called the sympathetic nervous system. Vagal/sacral afferents are thought to mediate non-noxious sensations, including local reflexes such as gastric accommodation and the gastrocolic reflex, whereas the spinal afferents are thought to mediate noxious sensations.24–26 Several lines of evidence support this separation of function.
Spinal nociceptors are wide dynamic range neurones which are capable of coding high intensity stimuli such as pain. These nerve terminals are located in the muscularis and serosa of the gut where distension and stretch might cause them to become activated in painful conditions. By contrast, vagal terminals are located more superficially, primarily in the mucosal and submucosal regions where lower intensity stimuli such as stroking or nutrient contact might cause activation. The concept of viscerosomatic referral, which only occurs with higher intensity stimuli such as pain, would require colocalisation of visceral and somatic terminals. This occurs in the dorsal horn of the spinal cord where only the spinal afferents terminate. These spinal afferents travel along blood vessels, through intestinal ganglia to the dorsal root ganglion cell body, and on to a synapse in laminae I, II, and V of the dorsal horn of the spinal cord.27 Given the abnormalities of referral in IBS, lack of improvement following vagotomy, and the general concepts of visceral nociception, the spinal afferent nerve system is strongly implicated as the first limb of the brain-gut pathway that mediates hypersensitivity and pain in IBS. The primary spinal afferent may in itself become hypersensitive or stimulators of this afferent may increase.
There is also evidence suggesting that IBS symptoms are triggered by peripheral factors such as inflammation or mast cell activation.28,29 This possibility is supported by studies showing that specific antagonists of 5HT3 receptors, which act peripherally at the enteric nervous system and probably on the spinal afferent, have been shown to significantly improve symptoms of IBS.26,30
The spinal cord is also a candidate for dysfunction in IBS. The widened referral patterns of visceral stimuli seen in patients with IBS are likely to be mediated at this level. In the dorsal horn of the spinal cord, ascending neurones interact with a number of spinal afferents, only some of which carry painful signals. Neuroplastic changes have been shown to occur at the spinal level in response to cutaneous pain and tissue injury. This causes some of the silent afferent nociceptors to become active; it increase the number of spinal levels which an individual nociceptor may activate and it lowers the thresholds for firing of the primary afferent nerve. These changes are associated with upregulation of N-methyl d-aspartate receptors, in part stimulated by the release of substance P from primary afferents.31
The second order neurone in the afferent pathway has a cell body in the dorsal horn and sends its ascending signal via one of three tracts. The classical ascending pathway is either the spinothalamic or spinoreticular pathway. However, recent evidence also implicates the dorsal columns in visceral nociception.32 Nociception is thought to involve both a lateral system, predominantly the spinothalamic tract, and a medial system, principally the spinoreticular pathway.27 The lateral system is thought to encode pain location, classification, and intensity whereas the medial system encodes pain suffering and emotional content. The lateral system has a third order neurone in the ventroposterior thalamus which relays afferent signals to the sensory cortex. In the case of somatic sensations, this pathway leads to the parietal sensory cortex. The visceral sensory cortex is thought to be the insula, which is a temporal lobe invagination that is activated by taste, smell, and intestinal distension.33,34 The lateral system can code both painful and non-painful sensations, as well as the type and location of stimulus. The medial pain system probably ascends from the brain stem reticular activating system area in the medulla and pons where the spinoreticular pathway terminates. The third order neurones from the brain stem send relays to the medial and intralaminar nuclei of the thalamus. From the intralaminar nuclei, ascending pain message spreads bilaterally to the prefrontal cortex, including the anterior cingulate cortex (ACC) (fig 3).35

Pathways involved in pain control. CNS, central nervous system; DRG, dorsal root ganglia.
The ACC is thought to be critical in coding pain suffering. Several human studies have shown that responses of the anterior cingulate nucleus to visceral distension correlate well with subjective pain intensity.34,36 Surgical lesions of this area do not remove the sensation of pain (which can be coded by the lateral pain system) but they remove the associated emotional content and suffering. Patients after cingulotomy describe the pain as present but not bothersome. The ACC is thought to act as an integrating centre which has wide inputs and outputs. Pain related stimuli are likely passed on from here to the prefrontal cortex where pain memory, interpretation, response, and other higher executive functions occur. The anterior cingulate is also part of the emotional limbic system, termed the “papez circuit”.37 The limbic system mediates both positive and negative emotions, as well as flight or fight autonomic responses. Abnormalities in the cingulate and other parts of the limbic system have been described in depression and anxiety.38 The intersection of the limbic system and medial pain system at the ACC may therefore have implications for patients with IBS and other stress related pain disorders.
Pain also triggers autonomic changes (including gastrointestinal motility and secretion) which ultimately are mediated by the hypothalamus. Intermediate autonomic effector areas include the insular cortex (especially the anterior segment) and the orbitofrontal cortex, which are considered to be paralimbic areas. It is possible that these areas are also stimulated by the ACC.39,40
BRAIN IMAGING IN IBS PATIENTS
Recent data indicate that patients with IBS have abnormalities in CNS processing of visceral pain. These studies generally use regional cerebral blood flow as a marker of brain activity in the corresponding area. Blood flow can be estimated by emission of positrons from injected isotopes but this method is associated with a delay of at least a minute to summate the signal. Functional magnetic resonance imaging (FMRI) can be used in an alternative way to measure increases in local oxygenated haemoglobin as an indirect measure of flow. This method responds within five seconds of brain activation.
Silverman et al published the first study using positron emission tomography (PET) to measure CNS activation in response to anticipated or actual painful stimulation in six patients with IBS patients and in six controls.36 Brain activation responses in patients with IBS were primarily in the prefrontal cortex while controls showed increased activation of the ACC.36 One interpretation is that loss of anterior cingulate activation results in failure to inhibit pain, and increases pain perception in the prefrontal cortex. A subsequent FMRI study showed that non-painful and painful rectal distending stimuli resulted in activation of the thalamus, insula, anterior cingulate, and prefrontal cortex. In patients with IBS (n=16), but not controls (n=18), there was greater thalamic and anterior cingulate activation with painful compared with non-painful stimuli. In a direct comparison, more active pixels were seen in the ACC of patients with IBS than in controls during painful stimuli (fig 4).34

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Activation of the anterior cingulate cortex insula and thalamus following rectal distension in patients with irritable bowel syndrome (IBS) and healthy volunteers. The red spots show areas of high activation.
Subsequent studies using the same method suggest that anterior cingulate activation in response to pain is markedly increased by anxiety, and when this is factored out, IBS patients have similar ACC responses to pain as controls. By contrast, thalamic activation is not influenced by anxiety and remains increased in patients with IBS, possibly reflecting an increased afferent signal to the thalamus.41 A later preliminary study using PET and the same stimulation paradigms as the Silverman paper36 confirmed that increased thalamic activation in IBS is accompanied by reduced anterior cingulate activation.42
Differences in the techniques of measuring CNS flow, distension paradigms, anticipation effects, mood of the subjects, and sex could explain differences in the anterior cingulate activation in these studies.43,44 Nevertheless, both the PET and FMRI data demonstrate abnormalities in the ACC where normal correlations between pain and activation are lost and responses to rectal pain are abnormal. Two reports using different imaging techniques have also demonstrated thalamic hyperreactivity to visceral pain in IBS. Functional brain imaging therefore supports the hypothesis of an increased afferent signal between the periphery and the thalamus, and an alteration in ACC response to pain in patients with IBS.
THE BRAIN-GUT CONNECTION
An interesting model of IBS is the stress induced gastrointestinal dysfunction that occurs in rodents. Water avoidance stress in rats and mice stimulates increased colonic motility and faecal pellet output, as well as decreased gastric and small bowel transit.45 This effect is in a large part mediated by corticotrophin releasing factor (CRF), presumably released by the hypothalamus.46 Specific antagonists of CRF block these motility abnormalities.
Patients with IBS have been shown to have augmented colon motor responses to peripherally infused CRF,47 and gastrointestinal sensitivity is known to be affected by CRF, as evidenced by the fact that peripheral infusion of CRF increases intensity ratings in response to rectal distending stimuli.48 This response may occur via stimulation of the locus coeruleus which increases sensitivity to somatic afferent stimuli and also possibly to visceral stimuli.49 The hypothalamic stress response is likely to be triggered by limbic circuits which mediate stress responses. The amygdala, which is part of the limbic system, is known to regulate release of hypothalamic CRF.50
The fact that pain can be actively inhibited by the brain is well described in life threatening situations, suggesting that a pain inhibitory pathway also exists. Mice can be bred for stress induced analgesia or hyperalgesia, and the more “stoic” mice have been shown to have greater concentrations of opiate receptors in the cortex and reticular activating system. This form of stress induced analgesia is blocked by the opiate antagonist naloxone.51 Descending enkephalin containing analgesic neurones from the rostroventromedial medulla terminate presynaptically on primary spinal afferents, inhibiting them from depolarising the dorsal horn neurone. Abnormalities in pain inhibition may therefore explain chronically painful conditions such as IBS.
As mentioned earlier, repetitive painful stimulation of the sigmoid colon significantly reduces rectal pain thresholds in IBS, thereby “sensitising” patients to subsequent stimulation.14 This response is not seen in controls, and may be due to failure of the descending pain inhibitory processes in IBS. Such a mechanism could be due to inadequacy of the endogenous opiate pathway from the reticular activating system to the dorsal horn. Recent data showing that exogenous opiate infusion normalises hypersensitivity to rectal distension in patients with IBS supports this concept.52
CONCLUSIONS
A network of afferent (sensory) neural connections from the gastrointestinal tract to the brain encode both non-painful and painful stimuli. Abnormalities which upregulate afferent signal intensity at any one or several sites in this system are likely to mediate gastrointestinal hypersensitivity leading to the pain and discomfort that characterise IBS and other functional disorders.
In pathophysiological terms, perturbations in stimulus amplification in the gut prior to the primary afferent nerve, or hyperresponsiveness of the afferent nerve itself, could lead to hypersensitivity. Abnormalities in the dorsal horn of the spinal cord are described in animal models of sensitisation, and fit with the widened viscerosomatic referral patterns seen in functional gastrointestinal disorders. Lack of endogenous opiate mediated inhibition of the primary afferent nerve in the dorsal horn may result in failure to downregulate afferent messages from the gastrointestinal tract, leading to sensitisation.
Increased thalamic activation described in IBS may be a reflection of increased afferent signal from the periphery. Abnormalities in brain activation in IBS, particularly in the medial pain system, have recently been described although these may relate to comorbid psychological symptoms which amplify visceral pain centrally.
Functional gastrointestinal disorders are likely to be heterogeneous given the complexity of the afferent system, and a number of different perturbations are possible. Visceral hypersensitivity is likely to trigger increased efferent stimuli to the gut due to centrally mediated autonomic changes. Hypersensitivity may also alter motility by augmenting intestinal afferent-efferent reflexes. In summary, intestinal hypersensitivity to pain and discomfort and associated reflex alterations in motility might explain the symptoms of functional bowel diseases.