Article Text

Abstract
Many of the symptoms characteristic of the functional gastrointestinal disorders (FGID) are consistent with dysfunction of the motor and/or sensory apparatus of the digestive tract. Those aspects of sensorimotor dysfunction most relevant to the FGID include alterations in: gut contractile activity; myoelectrical activity; tone and compliance; and transit, as well as an enhanced sensitivity to distension, in each region of the gastrointestinal tract. Assessment of these phenomena involves a number of techniques, some well established and others requiring further validation. Using such techniques, researchers have reported a wide range of alterations in sensory and in motor function in the FGID. Importantly, however, relationships between such dysfunction and symptoms have been relatively weak, and so the clinical relevance of the former remains unclear. Moreover, the proportions of patients in the various symptom subgroups who display dysfunction, and the extent and severity of their symptoms, require better characterization. On a positive note, progress is occurring on several fronts, especially in relation to functional dyspepsia and irritable bowel syndrome, and based on the data gathered to date, a number of areas where further advances are required can be highlighted.
- motility
- sensation
- gastrointestinal tract
- functional gut disorders
- functional dyspepsia
- irritable bowel syndrome
- visceral hyperalgesia
- Rome II
Abbreviations used in this paper
- FGID
- functional gastrointestinal disorders
- MMC
- migrating motor complex
- IBS
- irritable bowel syndrome
Statistics from Altmetric.com
- motility
- sensation
- gastrointestinal tract
- functional gut disorders
- functional dyspepsia
- irritable bowel syndrome
- visceral hyperalgesia
- Rome II
Motility of the digestive tract encompasses the phenomena of myoelectrical activity, contractile activity, tone, compliance, and transit. In the functional gastrointestinal disorders (FGID), various types of dysmotility have been documented repeatedly, and most likely reflect dysfunction at one or more levels of the brain–gut axis. Patients with FGID also exhibit sensory afferent dysfunction, manifest as an altered sensitivity to stimuli such as distension of the gut, and selectively affecting the visceral territory.
Digestive tract sensorimotor physiology and pathophysiology
BASIC CONCEPTS AND DEFINITIONS RELEVANT TO THE FGID
Motility
In the various regions of the gastrointestinal tract, muscle layers of the gut wall and their innervation are adapted and organized to subserve the motor functions of that region. Along the gastrointestinal tract, the gut interacts with the central nervous system through either somatic or autonomic neurons, and communication between various parts of the gut is facilitated by the transmission of myogenic and neurogenic signals longitudinally along the gut, as well as by reflex arcs transmitted through autonomic neurons (fig1).
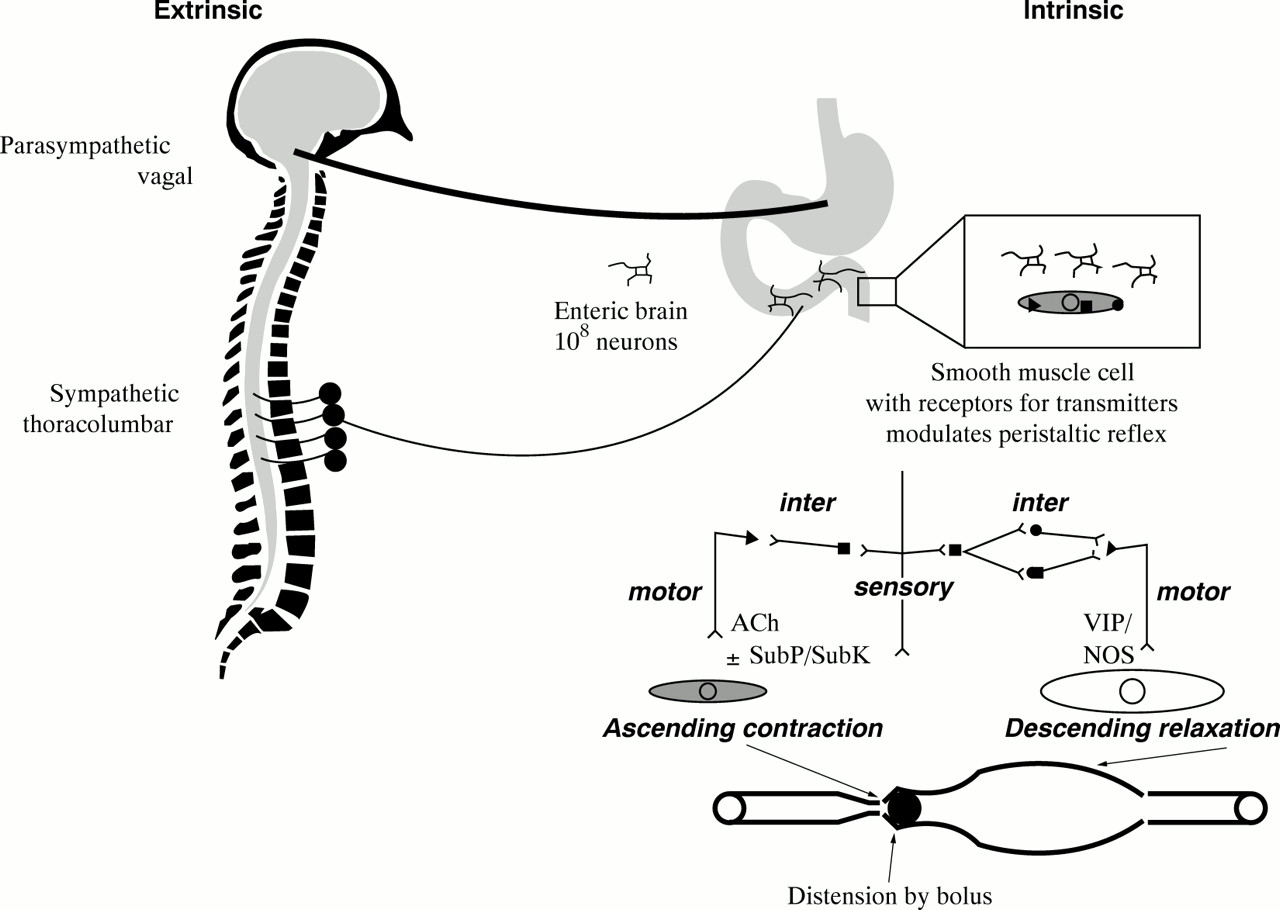
Extrinsic and intrinsic control of gastrointestinal motility. The extrinsic sympathetic and parasympathetic supply to the gut modulates the function of the enteric brain located in ganglionated plexi along the gastrointestinal tract. Transmitters released from the enteric neurons, which are the intrinsic neural control of the gut, modulate the peristaltic reflex. The major transmitters in the peristaltic reflex are shown on the right, acetylcholine (ACh) and substance P (SubP) are the predominant excitatory neurotransmitters, and vasoactive intestinal polypeptide (VIP) and nitric oxide are the predominant inhibitory neurotransmitters. SubK, substance K; NOS, nitric oxide synthase. (Reproduced with permission, Ann Rev Med 1999 (in press).)
Contractile activity and tone—Gastrointestinal contractions may be classified on the basis of their duration; contractions may be of short duration (phasic contractions), or may be more sustained (tone). In the small intestine, a phasic contraction is usually defined as a contraction whose duration does not exceed the span of a slow wave cycle; however, some longer lasting motor events are also considered phasic—for example, prolonged propagated contractions. A more prolonged state of contraction, referred to as tone, may be clearly recognized in some regions such as the proximal stomach (accommodation response to a meal) and the colon (response to feeding). Tone may also be a feature of sphincteric regions.
The spatial organization of contractions differs at all levels of the gastrointestinal tract. The stomach and small intestine display different patterns of contractility during fasting and postprandial states.1 In the fasted state, motor activity is highly organized into a distinct and cyclically recurring sequence of events known as the migrating motor complex (MMC). The MMC, which has been the subject of intensive study over several decades, consists of three distinct phases of motor activity that occur in sequence and migrate slowly along the length of the small intestine. Each sequence begins with a period of motor quiescence (phase 1), is followed by a period of apparently random and irregular contractions (phase 2), and culminates in a burst of uninterupted regular phasic contractions (phase 3 or activity front) (fig 2). Individual cycles last between one and two hours, originate in the stomach or, most frequently, the duodenum or proximal small intestine, and migrate aborally. The maximum frequency of contractions in these organs is most commonly observed during phase 3 of the MMC. If food is ingested, the cyclical pattern is abolished, or at least suppressed, and replaced, in the stomach by regular antral contractions, and in the small bowel, by irregular, random contractions which may be sustained for 2.5–8 hours, depending on the size and nature of the meal (fig 2). Thereafter, the fasted pattern resumes, or recurs, when a substantial part of the meal has emptied from the small bowel.
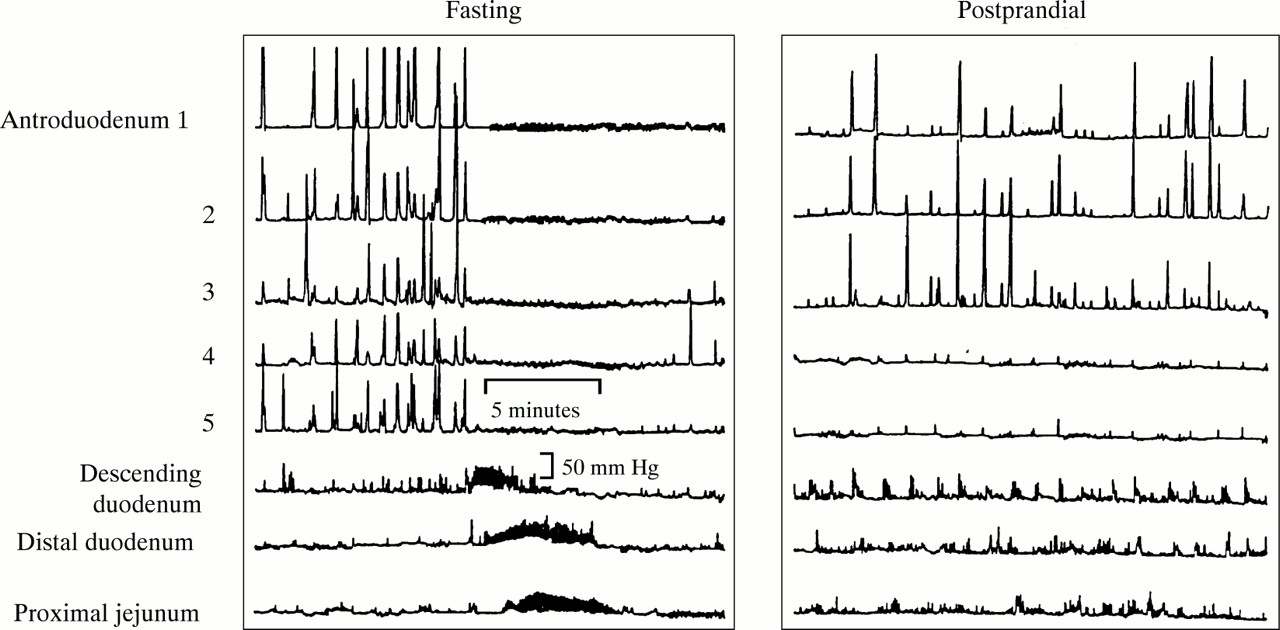
Example of fasting and postprandial motility in a healthy subject. Note the activity front (phase 3 of the migrating motor complex) during fasting (left panel) and the sustained but irregular contractile phasic pressure activity postprandially. (Reproduced with permission, Ann Rev Med 1999 (in press).)
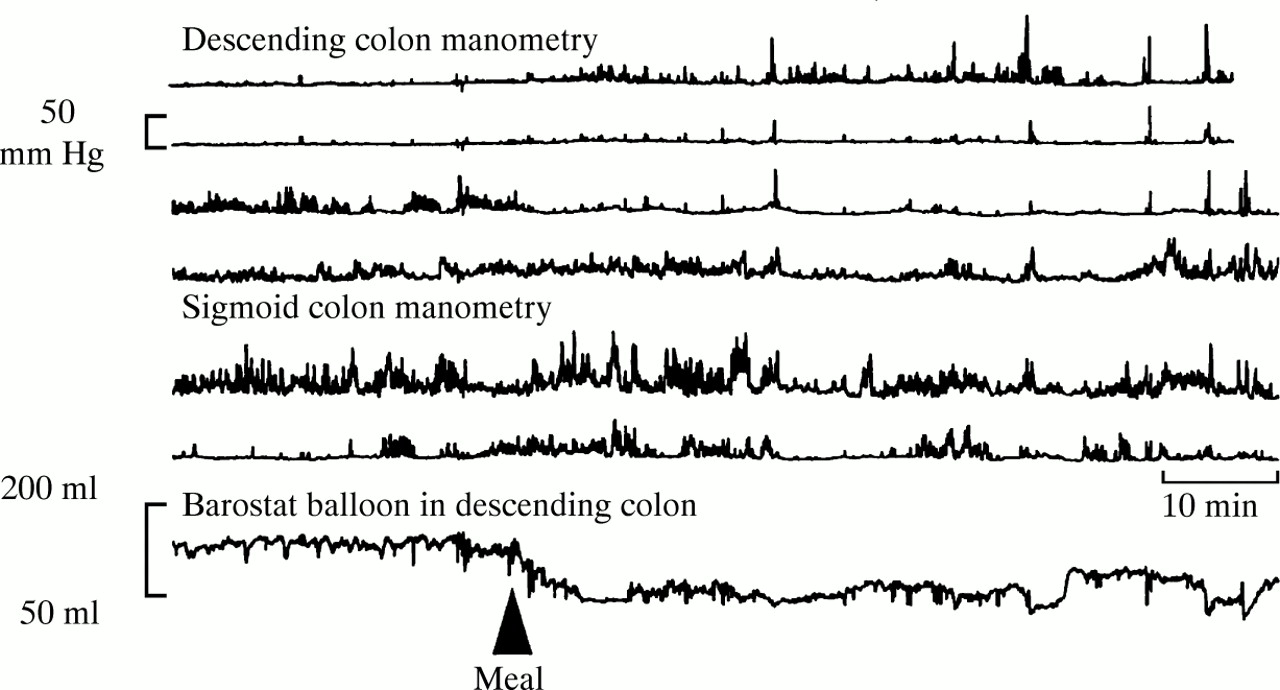
The colon displays several forms of contractility2: the most prominent of these are irregular contractions and high amplitude propagated contractions, associated with electrical activities called short and long spike bursts.3 The high amplitude propagated contractions are pressure events which sweep through the colon propelling contents from the ascending or transverse colon to the sigmoid colon or rectum. Prolonged recordings of colonic motility have shown that these contractions occur more often in the morning and during the postprandial period.4 ,5 The other motor events in the colon appear to propel contents over short distances in either an orad or an aborad direction, and their primary function appears to be to facilitate mixing. Accommodation and storage, essential functions of the colon, are at least partly mediated by colonic tone. Fluctuations in tone, however, also facilitate distribution of material in the colon, and alter thresholds for perception of luminal distension. Tone demonstrates considerable diurnal variation, increasing slowly following a meal, relaxing during sleep, and increasing dramatically upon waking (fig 3)6; these variables also influence phasic activity similarly.
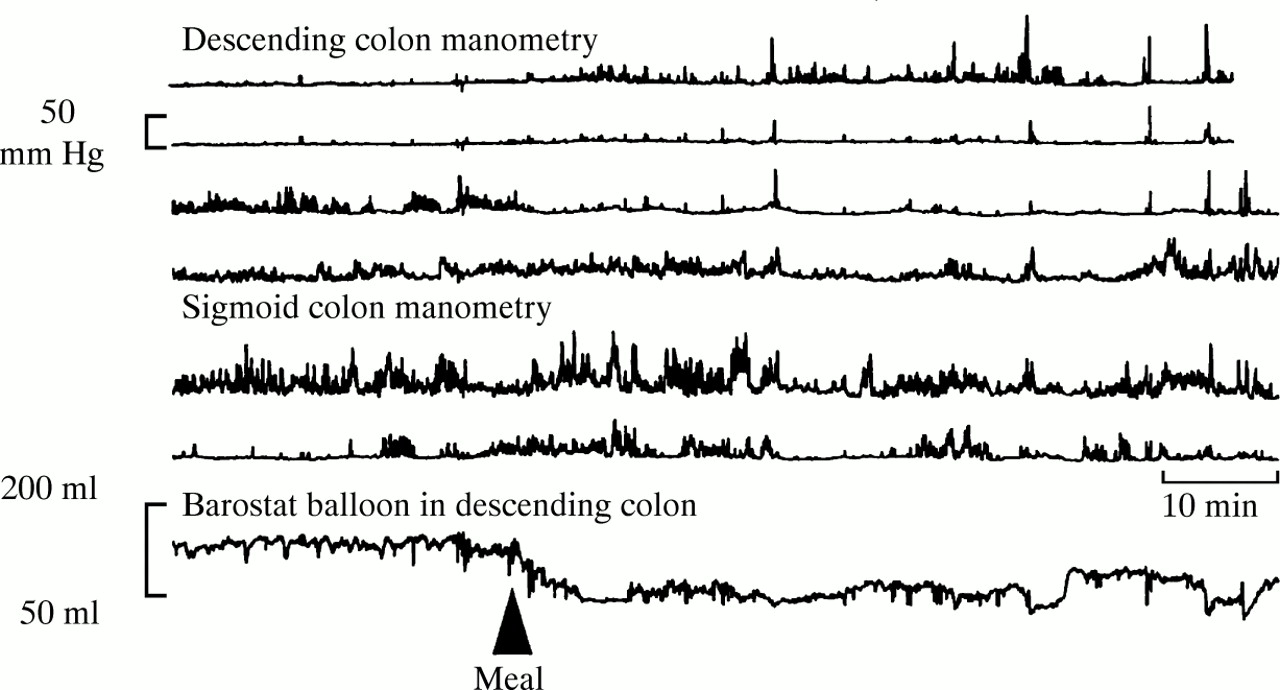
Colonic motility measured by means of manometry and barostatically controlled balloon in a healthy subject. Note the postprandial increase in phasic pressure activity in the descending colon, and the reduction in balloon volume, signifying an increase in colonic tone.
Compliance and related phenomena—Compliance refers to the capability of a region of the gut to adapt to an imposed intraluminal pressure; it is expressed as the ratio dV:dP and is obtained from the pressure–volume curve (fig4). Compliance reflects the contributions of several factors, including the capacity (diameter) of the organ, the elastic properties and muscular activity of the gut wall, and the elasticity of surrounding organs. The interpretation of compliance measurements remains controversial because compliance is also influenced by the type of distension, and—when phasic distension is applied—by the number of distension steps. Therefore, compliance should be compared between studies only when it has been measured in a similar way.

Compliance curve (dV:dP) drawn for human colon in a healthy subject.
Another phenomenon related to compliance is wall tension. This reflects the force acting on the gut wall and results from the interaction between intraluminal content and the reaction of the muscular and elastic properties of the wall. Gut sensation depends at least in part on wall tension; in the whole gut segment, tension is operationally defined by Laplace’s law (T = PR/2 for a sphere; T = PR for a cylinder, where T refers to wall tension, P is intraluminal pressure, and R is the radius). Assessment of wall tension may therefore be important in the interpretation of results of tests of sensation.
Transit—Transit refers to the time taken for food or other material to traverse a specified region of the gastrointestinal tract. It reflects the combined effects of the various phenomena outlined earlier. Factors influencing transit include the physical nature of the meal (e.g., solidv liquid emptying from the stomach), the composition of the meal (e.g., fat content or osmolality of the liquid phase), whether the marker used to measure transit is inert or part of the meal, the relation of marker ingestion to the interdigestive motility state in the small intestine, and the state of cleansing of the colon. Summaries of transit measurements commonly used include the half-emptying time (t½) for stomach (fig 5) and colon, and also the amount emptied from the stomach at two and four hours, and the mean transit time through the colon.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Gastric emptying of solids measured using scintigraphy: note the delay in gastric emptying t½ in a symptomatic diabetic patient compared with an asymptomatic patient and a healthy subject.
Sensation
Most stimuli in the gut are not consciously perceived. Sensitivity is an ambiguous term that has been used to refer to both conscious perception of gut stimuli and to afferent input within gastrointestinal sensory pathways, whether related to perception or to reflex responses. The term of most relevance to the FGID is the subjective experience of conscious perception. Several other terms however, borrowed from the field of somatic sensitivity, have been applied to studies of the FGID (reviewed by Mayer and Gebhart7). Hypersensitivity is the excessive perception of gut stimuli, or excessive afferent responses to stimuli. Hyperalgesia is a behavioral, perceptual or neurophysiologically induced sensation perceived as being painful—that is, greater in intensity and duration than normal. Allodynia reflects the painful sensation of a previously painless stimulus. The appropriateness of these terms to the field of visceral sensitivity in the FGID has still to be established.
SENSORIMOTOR DYSFUNCTION IN SELECTED FGID
Functional dyspepsia
It is now established that gastrointestinal sensorimotor dysfunction is present in a proportion of patients with functional dyspepsia; most studies have evaluated the stomach and small bowel, using a wide range of techniques. Table 1 summarizes the major findings from such gastric studies. In the stomach, the well-documented postprandial antral hypomotility is consistent with scintigraphic studies revealing delayed gastric emptying. It should be noted, however, that excessive postprandial antral distension in functional dyspepsia can impede the lumen-occlusive nature of normal antral contractions, thereby producing a false impression of antral hypomotility on manometric recordings. Regional gastric motor dysfunction can be assessed using a number of different techniques and remains an area of active interest. Myoelectric dysrhythmias appear to be an electrophysiological marker predictive of gastric stasis8—such dysrhythmias potentially may inhibit the development of normal postprandial peristalsis, thereby producing gastroparesis; alternatively, normal gastric slow waves may fail to link to, or couple with, abnormal circular muscle activity, resulting in electromechanical dissociation and gastroparesis.9
Alterations in gastric motility and sensation in functional dyspepsia (FD)
Small intestinal dysmotility, with or without associated gastric dysmotility, has also been described in patients with functional dyspepsia. Both conventional stationary and ambulatory antroduodenal and duodenojejunal manometric techniques have been used in various studies. Motor abnormalities have included the absence, or a reduced incidence, of MMC cycles, aberrant propagation of phase 3 of the MMC, a longer duration of MMC phase 2 motor activity, a higher prevalence of burst activity, and an abnormal postprandial motor response. The significance, however, of these types of alterations is still to be established.
The phenomenon of gastric hypersensitivity has now assumed a central role in the putative mechanisms of symptom generation in patients with functional dyspepsia, and is the area most likely to yield most definitive information on the pathogenesis of this disorder (table 1). Moreover, both the cold pressor test and transcutaneous electrical nerve stimulation have shown somatic sensitivity to be normal in patients with functional dyspepsia,10 ,11 supporting the concept of selective visceral hypersensitivity. Whether such sensory dysfunction extends beyond the stomach in patients with functional dyspepsia is controversial. For example, increased gastric but normal duodenal sensitivity was shown in a specific subset of patients with functional dyspepsia predominantly complaining of postcibal bloating,11 whereas other studies have reported an increased perception of small intestinal distension in these patients.12 ,13
Irritable bowel syndrome
The extensive literature on gastrointestinal motility in patients with irritable bowel syndrome (IBS) has been accrued over many years. More sophisticated measurement techniques developed over the past 10 years, however, have enabled better characterization of altered motor patterns in IBS. Most studies utilizing the more invasive measurement techniques, particularly the earlier studies, have been undertaken in the colon (especially the distal colon) and rectum because of their greater accessibility. Table 2 summarizes the major findings from relevant studies of colorectal dysmotility in IBS and related functional bowel disorders.
Alterations in colorectal motility and sensation in irritable bowel syndrome (IBS), and other functional bowel disorders
The small intestine in IBS has been explored in relatively few studies. However, as with functional dyspepsia, a range of subtle alterations in small bowel interdigestive motor activity has been documented, including alterations in the periodicity of interdigestive cycles, small differences in MMC phase 3 duration and propagation velocity, and variations in MMC phase 2 contractile patterns. Such alterations, however, have not been confirmed in all studies of small bowel manometry in IBS, and so their clinical significance remains uncertain. In postprandial jejunal motor recordings in patients with IBS, no major alterations have been observed; some patients have a shorter duration of the fed pattern and a higher amplitude and frequency of contractions than healthy subjects, but the initial response of the small intestine to food appears intact. Small bowel transit time has been variably reported as normal or rapid in patients with diarrhea-predominant IBS.
A proportion of patients with IBS displays an increased conscious perception to painful distensions in the small bowel and colon, and in some studies, an increased perception of apparently normal motor events in the gut. Such hypersensitivity to distension has been well documented in both the distal colon and more proximal colonic segments in patients with IBS (table 2). Although reports of pain from balloon distension studies can be influenced by response bias,15the low thresholds for balloon distension occur even when controlling for neuroticism.16 Furthermore, patients with IBS have normal16 or even increased thresholds17 for painful stimulation of somatic neuroreceptors. It is unclear whether the novel reports of alterations in cerebral blood flow in these patients18 ,19 provide mechanistically important insights; such descriptive observations require validation in large patient groups. There is evidence that visceral hypersensitivity in patients with IBS may also affect different levels of the small bowel20-22; whether the ileum22 exhibits greater or lesser hypersensitivity than the jejunum in IBS is not established. Patients with IBS display a distorted referral pattern of gut sensations, and perceive intestinal distensions more diffusely over the abdomen than healthy controls.7 ,23-25
Clinical implications of sensorimotor dysfunction in the functional gastrointestinal disorders
Documentation of sensorimotor dysfunction in at least some patients with FGID gives rise to four main questions relevant to clinical practice. These are (a) what are the possible mechanisms of such dysfunction; (b) what are the relationships between sensorimotor dysfunction and symptoms; (c) what is the role of current tests of sensorimotor function in helping to establish a diagnosis of FGID; and (d) can treatment of specific types of sensorimotor dysfunction lead to clinical improvement? Only limited data are currently available in each of these areas.
PUTATIVE ORIGINS OF SENSORIMOTOR DYSFUNCTION IN THE FGID
Alterations in gut motor activity in the FGID may arise from a number of putative mechanisms. These include: (1) enteric mechanisms such as motor dysfunction associated with minor degrees of inflammation and consequent changes in neurotransmitter release26 ,27; (2) local reflex mechanisms, occurring in response to specific nutrients such as lipid,28 or in response to mechanical distension11; (3) extrinsic neural mechanisms such as abnormalities in extrinsic autonomic innervation29; and (4) central mechanisms, whereby higher neural centers modulate peripheral intestinal motor activity.30
Similar mechanisms have been advanced to account for the enhancement of visceral sensation in the FGID.7 ,31 These include: (1) altered receptor sensitivity at the viscus itself, occurring through recruitment of silent nociceptors or peripheral sensitization in response to ischemia or inflammation; (2) increased excitability of the spinal cord dorsal horn neurons, where repeated distension of the intestine produces central (spinal) hyperalgesia, with enhanced intensity and expanded somatic referral of the visceral stimulus; and (3) altered central modulation of sensation, involving psychological influences on the interpretation of these sensations,32 or altered central regulation of ascending signals from the dorsal horn neurons in the spinal cord. Because the mechanisms of central interpretation of afferent signals are not known, it is not clear whether psychological or neurophysiological mechanisms work singly or in concert in the conscious perception of incoming signals.
RELATIONS BETWEEN SENSORIMOTOR DYSFUNCTION AND SYMPTOMS
Studies have generally shown a disappointing lack of correlation between sensorimotor dysfunction and symptoms in the FGID, and so the clinical relevance of sensorimotor dysfunction in such patients is unclear. Recently, however, with the use of more sophisticated techniques, some potentially important correlations between sensorimotor dysfunction and symptoms are beginning to emerge, especially in relation to functional dyspepsia—for example, between gastric stasis and postprandial fullness, nausea and vomiting33-35; between impaired gastric accommodation and early satiety36; and between antral widening and the degree of early postprandial discomfort.37 ,38
TESTS OF SENSORIMOTOR FUNCTION IN THE DIAGNOSIS OF THE FGID
Although each one of the techniques to assess motility can provide important information regarding the motor functions of the digestive tract, none has enabled characterization of definitively “abnormal” motor patterns in patients with FGID. In one study of patients with severe motility-like functional dyspepsia—for example, despite the use of prolonged recordings and advanced computer-aided analysis, and the demonstration of seemingly abnormal motor patterns, it was not possible to identify a specific small intestinal motor pattern which enabled discrimination between patients and those with other disorders, or even with healthy individuals.39 Likewise, based on the data outlined earlier, it is clear that the currently available tests to assess gut sensation do not enable a positive diagnosis of the FGID. Thus, in IBS it is not yet possible to define “abnormal” values, namely the rectal pressure which can characterize hypersensitive patients, due to the lack of large studies in healthy subjects. In functional dyspepsia, gastric distension data from large numbers of patients and controls are currently not available, although a recent study has described the lower range of normal for the distending pressure that induces discomfort in healthy subjects.36Another problem is that there seems to be little specificity of the responses to distension tests between the FGID subgroups, or to the organ considered most relevant in the pathophysiology of the syndrome, namely the stomach for functional dyspepsia, or the colon and rectum for IBS.
Despite this, several of the techniques are well standardized and interpretable in the clinical context; these include radio-opaque marker transit, anorectal manometry, scintigraphic gastric emptying assessment, and antroduodenal manometry. An important role for such tests in clinical practice is to enable identification of disturbances that indicate the likely presence of another specific disorder. Such disturbances40 include: (1) the low amplitude contractions (postprandial small intestinal contractions <20 mm Hg at manometry) suggestive of an infiltrative disorder of gastrointestinal smooth muscle, or other severe enteric myopathic disorder, which would exclude the diagnosis of FGID; and (2) findings such as an abnormal propagation of the MMC, hypercontractility (bursts and sustained uncoordinated pressure activity), and a failure of development of the fed response, which are indicative of a neuropathic disorder.
If such clearly abnormal findings are not identified, what then is the clinical relevance of other more subtle alterations in sensorimotor function in a patient with FGID? Currently, alterations in transit, and to a lesser extent manometric alterations, provide objective proof of dysfunction and invite trials of specific drug therapies to attempt to correct the dysfunction. In the case of other tests, particularly those that assess perception, or assess reflex responses such as gastric accommodation or the colonic response to feeding, further research to evaluate their specificity and predictive value, and to increase their precision, is required. The expectation is that more precise identification of such physiological alterations will facilitate the recognition of further patient subgroups deserving a directed therapeutic approach, such as the role of impaired gastric accommodation in functional dyspepsia and its potential reversal by fundus-relaxing drugs.36
PHARMACOTHERAPY OF SENSORIMOTOR DYSFUNCTION IN THE FGID
Modulation of sensorimotor function can be accomplished by a range of interventions aimed at different levels of the brain–gut axis. In terms of pharmacotherapy, a range of medications is available potentially to restore some of the alterations in motor function identified in the FGID.41-46 Most evidence for the efficacy of such medications is available for those which improve disordered gut transit, such as delayed gastric emptying, and delayed or accelerated colonic and/or small bowel transit, and to a lesser extent altered contractile activity such as antral hypomotility or an exaggerated colonic motor response to feeding (reviewed in47-49). Other classes of drugs are currently under evaluation; these include drugs inhibiting contractile activity in the gut such as the selective muscarinic antagonists (e.g., darifenacin), MK2-antagonists, beta 3-adrenoreceptor agonists, and gut selective calcium channel blockers (e.g., pinaverium bromide), and agents with potential for stimulation of motor activity and transit (e.g., loxiglumide, acting via blockade of cholecystokinin A-receptors, and 5-HT4 agonists). Little evidence is available for modulation of other components of dysmotility such as alterations in tone or compliance, although several drugs under evaluation (e.g., sumatriptan, clonidine and buspirone) appear to be capable of inducing relaxation of the proximal stomach.36 ,50 ,51
Substances that may influence sensation by acting at peripheral, spinal, supraspinal, or even several levels of brain–gut interaction have been considered in detail by Bueno et al.52 Most of these compounds have undergone only limited, if any, testing in humans and in the FGID. The specific 5-HT3 receptor antagonists such as ondansetron and granisetron, and the somatostatin analog octreotide, may have peripheral visceral antinociceptive actions and represent promising classes of agents acting in peripheral sites. The κ opioid receptor angonist fedotozine is another drug that can affect sensory thresholds to gastric and colonic distension in humans, and which has been shown to improve symptoms in functional dyspepsia and IBS.53Compounds modulating visceral sensitivity by acting centrally (and also peripherally) include low dose tricyclic antidepressants and adrenoreceptor agonists such as clonidine. The serotonin reuptake inhibitors have not been the subject of a systematic study in functional dyspepsia or IBS. Tricyclic antidepressants are superior to placebo for improving the symptoms of abdominal pain, nausea, and diarrhea in IBS54 ,55 and functional dyspepsia,56 but their precise sites of action are unclear.
Recommendations for further research
Further work is needed in many areas to tackle the clinical implications of sensorimotor dysfunction in the FGID: in particular, advances in the four main areas discussed earlier are of crucial importance. Firstly, a greater understanding of enteric neural control and modulation, and the mechanisms for dysfunction, will depend, to a large extent, on continuing advances in the basic science arena—for example, the electrophysiology of individual enteric neurons, identification of neurotransmitters, receptor subtypes, and their inter-relationships; the integration of specific neurons into the programs of motor and secretory activity; and the relationships between the enteric immune system and nervous system. Relevant to the latter is further characterization of the interactions between the enteric nervous system and its local environment, such as luminal content, hormonal fluctuations, presence of inflammation, etc. Alterations in central nervous system control are clearly of major importance, including the role of autonomic dysfunction in the FGID; in particular, evaluation of abdominal autonomic function, using more specific tests, is required. The interaction between central trigger factors, including psychological factors, and peripheral trigger factors requires greater exploration, at both the basic and whole organ level. Human physiological studies looking at more specific hypotheses can then be undertaken.
Secondly, in order to determine relationships between symptom subgroups, individual symptoms and sensorimotor dysfunction, the patient populations under study require strict definition. For example, the relevance of the predominant alteration of bowel habit in IBS, such as diarrhea, constipation, and associated changes in stool form and consistency, and also the presence or absence of concomitant dyspeptic symptoms, is yet to be established in the context of sensorimotor dysfunction. Cross-correlation of physiological dysfunction with symptoms may only be possible if the particular symptoms experienced by the patient at the time of investigation are evaluated and accounted for in the analyses. Due regard for the severity and extent of such symptoms may then facilitate further studies assessing the natural history of sensorimotor dysfunction and its relationship to the natural history of symptoms—that is, why the clinical spectrum ranges from individual syndromes with minor, intermittent, and transient symptoms originating in a single gut region, to more extensive, consistent, and chronic symptomatology involving multiple overlapping syndromes with symptoms presumably originating from multiple (more generalized) gut foci.
Thirdly, it is clear that new approaches and methods are required to study sensorimotor dysfunction, in order to overcome the considerable limitations of the current techniques. The specificity and predictive value of physiological testing can only be improved on the basis of the development of novel, validated, technologies. Thus, more sophisticated techniques to assess compliance and wall tension, and to assess more precisely the flow of luminal content, and gas, are required.57 New techniques for brain imaging and spinal monitoring are required to attempt to discriminate between patients with FGID who display gut hypersensitivity due to sensitization of primary visceral afferents and/or the spinal cord, from patients who have aberrant brain processing of sensations.58 At the same time as the development of more sophisticated technology, such tests, together with existing techniques, need to be standardized to enable the completion of multicenter studies and to facilitate comparability of data between laboratories.59 In this regard also, the development of minimally or non-invasive techniques of investigation, which can function as true surrogate markers of sensorimotor dysfunction, and which can be repeated in patients after various therapeutic maneuvers, is particularly important.
Fourthly, the main challenge for pharmacological research in the FGID over the next decade will be the development of new drugs to relieve specific sensorimotor dysfunctions, and it is hoped, to thus relieve specific symptoms. The increasing interest in visceral afferent pathways has resulted in the identification of a number of neurotransmitters involved in the processing of information from the gut to the brain, and these may affect sensitivity.52 It is important to note, however, that almost all of these neurotransmitters act on both the afferent and the efferent pathways, so caution is necessary in defining the mechanisms of drug action. In functional dyspepsia, the targets for restoring normal sensitivity and improving postprandial symptoms are most likely to be facilitation of accommodation and reduction of afferent hypersensitivity; the latter is clearly a more difficult task than the former. In the investigation of new drugs to modulate visceral sensitivity, the influence of alterations in compliance, tone, and wall tension are important areas. It should be noted that the actions of new drugs in these areas, however, may be due to effects on gut motor activity, either stimulation or inhibition. Only when documentation of correction of abnormal, or restoration of normal, sensorimotor function can be reliably achieved, will it be possible to determine whether such correction is related to improved clinical outcomes in the FGID. Moreover, the interaction between such pharmacologic approaches and psychosocial approaches requires further study. Assuming progress can be made in each of the above areas, and against the backdrop of the recent substantial gains, cautious optimism in regard to the future of neurogastroenterology studies in the FGID seems justified.
Abbreviations used in this paper
- FGID
- functional gastrointestinal disorders
- MMC
- migrating motor complex
- IBS
- irritable bowel syndrome