Article Text

Abstract
Background: Our aim was to assess the relationship between gastric motor and sensory function and symptom patterns in community subjects and patients with functional dyspepsia (FD) or irritable bowel syndrome (IBS).
Methods: We recruited 291 asymptomatic blood donors, 151 symptomatic blood donors (recurrent abdominal pain or discomfort), and 40 patients with FD or IBS. Abdominal symptoms were assessed using the bowel disease questionnaire (BDQ) and, in addition, the most bothersome symptom complex identified (dysmotility-type, ulcer-type dyspepsia, or IBS). Gastric emptying time (GET (t1/2, min)) was measured by 13C-octanoic breath test and a nutrient challenge performed. Twenty randomly selected asymptomatic blood donors, 48 symptomatic blood donors (30 FD, 18 IBS), and 40 patients (23 FD, 17 IBS) had additional function testing.
Results: GET (t1/2) was significantly (p<0.05) longer in blood donors with FD symptoms (99 (6) min) and FD patients (110 (12) min) compared with asymptomatic controls (76.7 (7) min), but was not significant in IBS blood donors or patients. Overall, 25 of 48 blood donors with symptoms and 18 of 40 patients had slow gastric emptying. GET was most delayed in subjects with predominantly dysmotility-type symptoms (167 (36) min v controls; p<0.01). Symptom intensities after a nutrient challenge were significantly higher in FD patients and symptomatic blood donors compared with asymptomatic controls; 14 of 48 blood donors with symptoms and 16 of 40 patients had a symptom response to the nutrient challenge exceeding the response (mean (2SD)) of healthy asymptomatic controls.
Conclusion: Gastric emptying and the global symptom response to a standardised nutrient challenge are abnormal in population based (non-health care seeking) subjects with dyspepsia.
- BDQ, bowel disease questionnaire
- FD, functional dyspepsia
- FGID, functional gastrointestinal disorder
- GET, gastric emptying time
- IBS, irritable bowel syndrome
- GORD, gastro-oesophageal reflux disease
- functional dyspepsia
- irritable bowel syndrome
- gastric emptying
- consulters
- non-consulters
Statistics from Altmetric.com
- BDQ, bowel disease questionnaire
- FD, functional dyspepsia
- FGID, functional gastrointestinal disorder
- GET, gastric emptying time
- IBS, irritable bowel syndrome
- GORD, gastro-oesophageal reflux disease
Functional gastrointestinal disorders (FGID) are clinical syndromes defined by chronic or recurrent abdominal symptoms without identifiable cause using conventional diagnostic measures.1 Functional abdominal symptoms are highly prevalent in the general population; many do not seek health care but the intensity of symptoms may be one factor promoting the seeking of medical assistance.2 In functional dyspepsia (FD) and irritable bowel syndrome (IBS), symptoms are frequently related to meals and can include abdominal pain, bloating, early satiety, fullness, belching, and nausea.1 The aetiology of FD is unknown but various pathophysiological mechanisms may account for them. Impaired meal induced relaxation of the proximal stomach,3,4 visceral hypersensitivity to distension,3,5,6 gastric motor abnormalities,7 as well as disturbed central nervous function8,9 have all been implicated as important pathophysiological mechanisms causing dyspeptic symptoms, but overlap is frequent.
It has been demonstrated that approximately 40% of patients with FD have impaired gastric emptying, and this has been linked to fullness.10 Boeckxstaens and colleagues11,12 reported impaired ability to drink a normal nutrient meal volume but did not find a correlation between drinking capacity and specific dyspeptic symptoms. On the other hand, Tack et al recently reported a correlation between impairment of meal induced proximal stomach relaxation and a drink test in FD.13 However, it is not known if these pathophysiological abnormalities are associated with symptom clusters, as defined by the Rome I criteria. In addition, previous studies may have been biased because they focused on patients referred to tertiary referral centres, presumably for refractory symptoms. Data on the relationship between disturbed gastrointestinal motor and sensory abnormalities in patients not referred to tertiary centres are lacking and similarly, no population based data are available.
Our aims in the present study were: (a) to determine the relationship between gastric motor abnormalities and an abnormal nutrient drink test in a population based sample of subjects with and without symptoms, and in patients evaluated in a tertiary care centre; and (b) to assess whether specific functional gastrointestinal disturbances are related to the most bothersome symptoms in the population. We hypothesised that (1) gastric emptying would be delayed in patients and this would be more likely in subjects with predominantly dysmotility-type symptoms and (2) the global symptom response to a standardised nutrient challenge would be increased in subjects with dyspeptic symptoms and in symptomatic patients with FD.
MATERIAL AND METHODS
Subjects
The study protocol was approved by the Institutional Review Board of the University of Essen. During an eight week period, 442 consecutive blood donors were recruited for the study. After giving informed consent, all volunteers underwent a physical examination and laboratory screening (sedimentation rate, red and white blood cell count, transaminases, gamma glutamyltransferase, hepatitis B and C antibodies, as well as HIV antibodies). In addition, 10 ml of blood were taken for determination of Helicobacter pylori antibodies (ELISA, Freiburg, Germany). Preparation of the antigen was performed according to the method previously described by Blaser and Duncan.14 The cut off value was set at 10 IU/ml.
Subjects receiving any medication over an eight week period prior to blood donation (that is, antibiotics, antacids, prokinetics, proton pump inhibitors, H2 receptor antagonists, or non-steroidal anti-inflammatory drugs), those with a history of abdominal or gynaecological surgery, gastrointestinal cancer, peptic ulcer disease, and isolated or predominantly symptoms of gastro-oesophageal reflux disease (GORD) were identified by interview prior to blood donation and excluded from the study (n = 8). A randomised screening for drugs and narcotics was performed; 10 subjects refused to participate in the study. Therefore, out of a population of 460 consecutive healthy blood donors, 442 (96.1%; 241 female) participated in the trial. A flow chart of patient selection and study days is shown in fig 1.

Study population. FGID, functional gastrointestinal disorders; FD, functional dyspepsia; IBS, irritable bowel syndrome.
Forty consecutive patients (27 female, aged 27–40 years) with either FD or IBS referred to our institution for evaluation and treatment served as positive controls. Standardised workup included upper gastrointestinal endoscopy, abdominal sonography, and laboratory testing. Colonoscopy was also performed in all subjects aged >45 years and those with concomitant IBS symptoms.
Assessment of abdominal symptoms
To assess abdominal symptoms and intensity, all study participants were given a German version of the bowel disease questionnaire (BDQ15), as described previously.16 This was completed prior to participation in the study. Study subjects were requested to grade the intensity of their symptoms (if any) on a scale ranging from 1 (mild) to 4 (extreme). All subjects were categorised according to the Rome II criteria by the same physician (SH) based on symptoms that were identified by the patient as the most bothersome17 (that is, IBS; or ulcer-type, dysmotility-type, or non-specific FD). During the nutrient drink test on study day 2, symptoms (pain, fullness, nausea) were analysed by a symptom score on a visual analogue scale (range 0–100 mm).
Study protocol
Function testing was performed on two separate days at least seven days apart. Tests were performed in random sequence. On one study day, gastric emptying time (GET) was quantified with an 13C-octanoic acid breath test according to the method of Ghoos and colleagues.18 All tests were performed after an overnight fast. The test meal consisted of a scrambled egg with yolk doped with 100 mg 13C-octanoic acid. The egg was ingested with two slices of white bread and 10 g of margarine (total caloric load 300 kcal), and immediately followed by 150 ml of water. After two hours, subjects were given another 150 ml of water. Before the test, a breath sample was taken for baseline measurements. In the following four hours, breath samples were taken every 10 minutes during the first two hours and every 15 minutes for the last two hours of the test. Delayed gastric emptying was defined as a t½ greater than the 95% confidence interval (CI) in healthy volunteers.18
On another day, a standardised 600 ml nutrient challenge (Fresubin; Fresenius, Germany; caloric density 1.5 kcal/ml: 3.8 g protein, 13.8 g carbohydrate, 3.4 g fat/100 ml) was performed and symptoms (nausea, fullness, pain) assessed using a visual analogue scale (range 0–100 mm) with “0” = no symptoms or discomfort and “100” = very severe pain or discomfort. All subjects were asked to drink 200 ml of the liquid meal every five minutes and reported their symptoms after a total of 600 ml (or the maximum ingested volume if subjects did not tolerate 600 ml). We have shown previously that symptom response at a cumulated volume of 600 ml is significantly correlated with the gastric volume threshold for discomfort measured with a barostat device.19
Statistical analyses
Primary outcome variables were gastric emptying (t½, min) and symptom response to the nutrient challenge (600 ml).
Means (SD) for symptom intensity were calculated and groups compared. Analyses of variance were used for differences between blood donors with versus without symptoms and subgroups and patients from the outpatient clinic with regard to their symptoms. Log transformation was conducted prior to analysis if indicated. Alpha adjustment for the primary two target variables was applied. Analyses were conducted in a hierarchical manner (that is, differences in the primary outcome were initially tested in symptomatic versus asymptomatic subjects). Further comparisons were done only if the initial comparisons yielded significant differences.
All p values calculated were two tailed; an α <0.05 was considered significant for primary parameters. All further (exploratory) analyses were considered significant at an α level of 5%. Statistical analyses were performed using the Statistical Analysis System (SAS, release 6.12; SAS Institute Inc., Cary, North Carolina, USA20).
A sample size of at least 20 healthy subjects and at least 40 subjects with symptoms were needed to yield differences of more than 20% for the primary outcome variables with an α level of 0.025 and a β level of 0.80.
RESULTS
Overall, data from 442 blood donors (241 females, 201 males; aged 18–68 years) and 40 consecutive patients (27 females, 13 males; aged 23–70 years) with chronic abdominal symptoms but no anatomical or biochemical abnormalities to explain their symptoms (positive controls) were available. Due to an incomplete questionnaire with more than 25% missing data, one female blood donor could not be analysed and another 15 (10 female) blood donors with symptoms could not be classified for the same reason. Thus 136 subjects with recurrent abdominal symptoms were available for further evaluation.
Gastrointestinal symptoms
A total of 151 healthy blood donors (34.2% (95% CI 29.7–38.6)) reported abdominal pain or discomfort on more than six occasions during the previous 12 months. Thirty seven blood donors (24.5% (95% CI 17.6–31.4)) identified IBS symptoms as the most bothersome symptom complex while the remainder reported predominantly symptoms consistent with FD (n = 21 ulcer-type 13.9% (95% CI 8.4–19.4); n = 49 dysmotility-type 32.5% (95% CI 25.0–39.9); n = 29 non-specific dyspepsia 19.2% (95% CI 12.9–25.5)). Fifteen blood donors (9.9% (95% CI 5.7–15.9)) reported recurrent abdominal symptoms but were not analysed further due to lack of additional information. Twenty five of 37 blood donors (67.6% (95% CI 50.2–82.0)) with IBS symptoms were female. In contrast, FD symptoms were predominantly reported by males (57.6% (95% CI 47.2–67.4)).
Twenty subjects (12 female) without any abdominal symptoms and 50 subjects with relapsing upper abdominal symptoms consistent with FD or IBS were randomly recruited from the blood donor population. Two refused to participate, leaving 68 subjects (43 women, 25 men; age range 19–68 years). In addition, we studied 40 consecutive patients with chronic abdominal symptoms lasting for more than five years, consistent with FD or IBS, as a control group (27 women, 13 men; aged 23–70 years). The distribution of FD and IBS, based on the predominant symptom complex, as well as sex and age distribution are presented in table 1.
Frequency of abdominal symptoms, sex, and age distribution in healthy blood donors and positive controls (patients)
Gastric emptying time
Comparison of healthy controls with patients/blood donors with symptoms
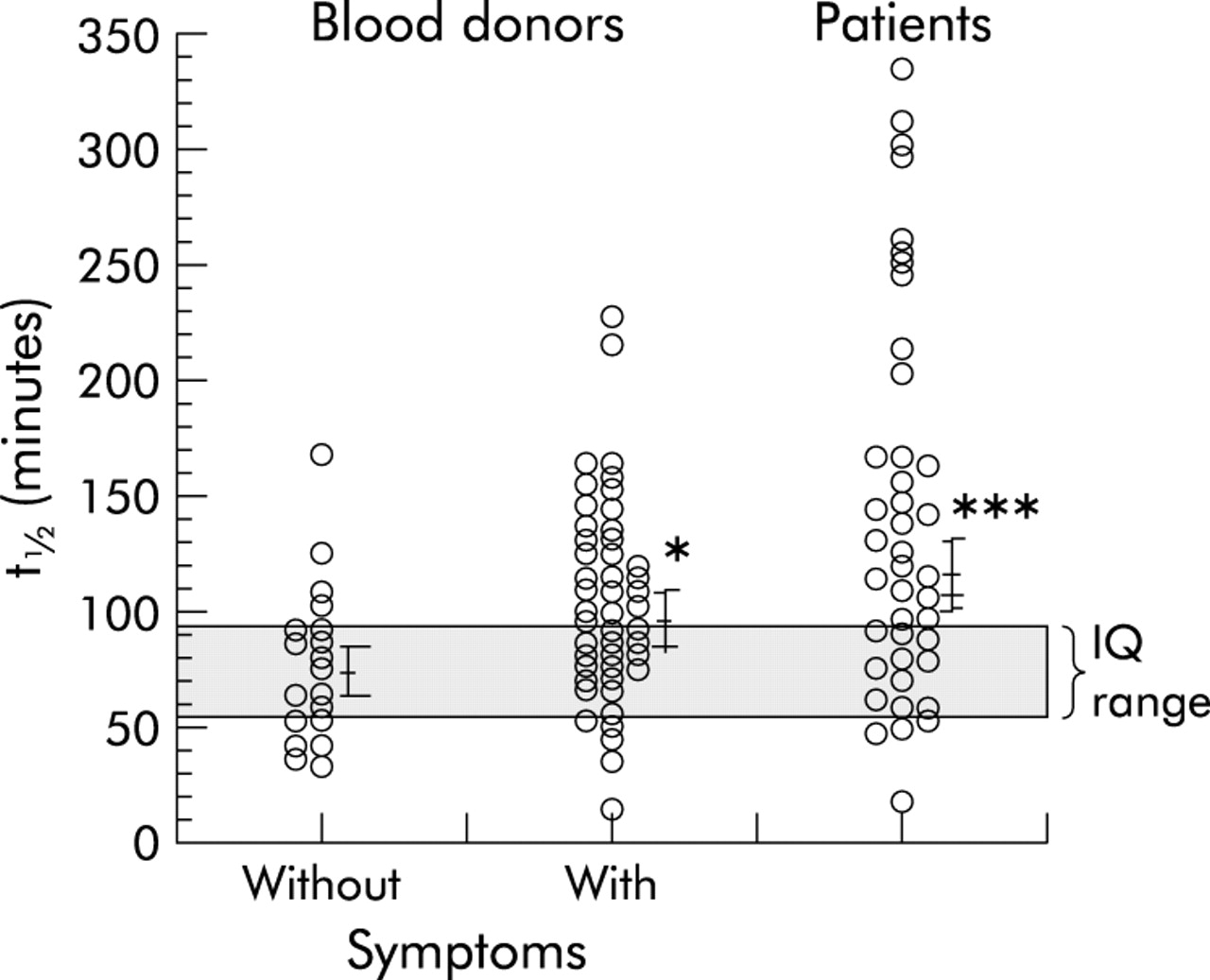
Overall, gastric emptying was significantly longer in blood donors with abdominal symptoms compared with asymptomatic controls (99 (6) v 76 (7) minutes; p<0.01). Similarly, GET was significantly delayed in patients compared with controls (110 (12) v 76 (7) minutes; p<0.01) (table 2, fig 2). Nine of the investigated patients and two of the blood donors with symptoms had a GET exceeding 200 minutes, identifying a subgroup of FD patients with severely delayed GET. Overall, 25 of 48 blood donors with symptoms (52%) and 18 of 40 patients with FD or IBS (45%) had a gastric emptying rate that was not within the normal range (mean (2SD)) of healthy asymptomatic controls (tables 2, 3). Furthermore, comparing gastric emptying in subjects with FD (patients and blood donors) with healthy controls yielded a significantly delayed gastric emptying time (109 (15) v 76 (7) minutes; p<0.01). Similarly, GET was delayed in subjects with IBS (patients and blood donors) compared with healthy controls (97 (14) v 76 (7) minutes; p<0.01).
Gastric emptying time (GET, t1/2 (minutes)) of patients versus blood donors
Proportion of patients with delayed gastric emptying (GET, t1/2 (minutes) >mean of health asymptomatic controls (2SD)) and augmented symptom response after 600 ml of nutrient challenge (VAS mm >healthy asymptomatic controls (2SD))

Gastric emptying time (t1/2 in minutes) of healthy blood donors with versus those without gastrointestinal symptoms, and of patients (*p<0.025, ***p<0.001 v asymptomatic controls). Interquartile (IQ) range is given for healthy controls.
Symptom type
Mean GET was significantly delayed in blood donors with dysmotility-type and ulcer-type dyspepsia, but not in IBS, compared with asymptomatic controls. Similarly, patients with dysmotility-type dyspepsia and IBS had delayed GET but there was no significant abnormality in patients with ulcer-type dyspepsia (table 2). Overall, 11 of 22 patients with dysmotility-type or ulcer-type symptoms (50%), and seven of 17 patients with IBS symptoms (41%) had gastric emptying above the normal range of healthy asymptomatic controls (table 3).
Nutrient challenge
With the exception of two patients with dysmotility-type symptoms, all study subjects ingested 600 ml. These two patients ingested 520 and 500 ml, respectively, and symptom responses were otherwise recorded according to the protocol.
Comparison of blood donors with symptoms, patients, and healthy controls
Intensities of pain, fullness, and nausea for the various study groups are shown in fig 3. Blood donors with gastrointestinal symptoms as well as the patient population had significantly higher symptom scores than healthy controls. Overall, 14 of 48 blood donors with symptoms and 16 of 40 patients with FD or IBS had a symptom response to the standardised nutrient challenge that exceeded the response (mean (2SD)) of healthy asymptomatic controls (table 3).

Symptoms after a 600 ml liquid load in blood donors (BD) with symptoms (n = 48), healthy controls (n = 20), and patients (n = 40). Self reported symptoms (visual analogue scale, VAS (mm)). ***p<0.001 versus asymptomatic controls.
Symptom type
Blood donors with dysmotility-type dyspepsia had significantly higher symptom scores for “fullness” than controls, and patients with dysmotility-type dyspepsia also scored significantly higher for “fullness” but also for “nausea” than controls (fig 4). Blood donors with ulcer-type dyspepsia scored higher for “fullness” versus controls. Patients with ulcer-type dyspepsia scored higher for “pain” versus controls (fig 4). Blood donors with IBS symptoms had higher “pain” scores than controls, and patients with IBS symptoms had even higher scores for “pain”.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intensity of gastrointestinal symptoms after a 600 ml liquid nutrient load in groups stratified based on their predominant symptom. Self reported symptoms (visual analogue scale, VAS (mm)). IBS, irritable bowel syndrome. *p<0.05 versus asymptomatic controls.
Helicobacter pylori prevalence
A positive IgG antibody titre for H pylori was found in 50% (95% CI 45.3–54.7) of the blood donor population. In blood donors with abdominal symptoms, 47.1% (95% CI 34.8–59.6) tested positive for H pylori. In contrast, only 19.4% (95% CI 7.5–37.5) of patients tested positive for H pylori.
Neither gastric emptying nor responses to nutrient ingestion were associated with H pylori status (data not shown).
DISCUSSION
In this combined population of patients with FD and IBS seen at a tertiary referral centre and non-health care seeking subjects with FD or IBS-symptoms, abnormalities of gastric emptying and symptomatic responses to nutrient stimulation were observed and linked to the predominant symptom pattern. Subjects with predominantly dysmotility-type symptoms were characterised by delayed gastric emptying. Subjects with ulcer-type symptoms were more likely to have an augmented pain response to nutrient challenge, suggesting an abnormality of (afferent) sensory function.
It is intriguing that abnormalities of function were found in subjects that had not sought medical attention. Previous studies on gastric emptying and sensory function have been conducted in tertiary referral settings10,18,21 and the prevalence of delayed gastric emptying in FD has been reported as 20–40%.12,22 However, the observed abnormalities of function may not represent a specific feature of patients seen at tertiary referral centres but could be due to referral bias. As we found very similar results in both population based subjects and patients, our data suggest that disturbances of gastric function are not due to referral bias. Whether the observed differences in gastric emptying are of clinical significance remains controversial. Indeed, while we were able to identify statistically significant differences and may even have found a subgroup of FD patients with severely delayed GET (>200 minutes), individual values overlapped considerably. It has been reported recently that early satiety was associated with early distal redistribution of the liquid phase and fullness was associated with late proximal retention.23 However, Piessevaux and colleagues23 reported similar intragastric distribution of a solid test meal in healthy controls and FD patients. The same group reported an association of delayed gastric emptying of liquids with postprandial fullness and with severe early satiety.22 Thus it might be argued that even small differences in gastric emptying are related to different pathophysiological mechanisms in a subgroup of FD patients. Thus the data are consistent with the concept that alterations in gastric emptying play a role in the manifestation of symptoms in a subgroup of patients with FD, while other factors may also be important.
It has been reported that non-consulters usually have lower symptom intensities,2 and in the present study abnormalities of function were more prevalent and severe in our patient controls. While numerically the proportion of blood donors and patients with abnormal sensory or motor function was not substantially different, patients had more severe disturbances in function compared with blood donors with symptoms. This may point to the fact that the severity of the functional abnormality determines the severity of symptoms and in turn the likelihood of health care utilisation. Recently, Koloski et al24 analysed potential predictors of health care seeking behaviour for IBS and FD. They reported that factors other than psychological morbidity, including symptom severity and frequency, were important for health care utilisation. However, there is still an ongoing debate about the relationship between mental health and health care utilisation. Anxiety in particular has been reported to be associated with FD patients25–28 but to our knowledge no previous study has assessed the correlation between mental health and visceral nociception.
On the other hand, previous studies were unable to demonstrate an association between normalisation of gastric emptying and improvement in symptoms.29–32 Thus while on the one hand it might be argued that abnormalities of gastric emptying can be directly associated with symptoms, it may be that disturbances in gastric emptying are simply a marker for other underlying abnormalities but are not directly relevant for manifestation of symptoms.
We studied a sample of blood donors that should be representative of the general population as well as patients referred to a tertiary referral centre. It is possible that our subjects were not representative of the population of patients in general. However, the distribution of symptom types, and the overlap of symptoms in our study population was very similar to patterns of symptoms reported previously in other patient populations.2,33–35
We wanted to non-invasively assess sensory dysfunction in dyspepsia. Barostat studies are now considered the gold standard for assessment of visceral sensory function. However, the invasive nature of barostat studies clearly limits usability and may cause selection bias. Thus non-invasive methods have been reported to assess accommodation, such as ultrasound studies for the proximal stomach, which are labour intensive and require specialised equipment.36 Three dimensional single photon emission computed tomography of the gastric wall was developed for quantification of accommodation but this requires expensive equipment and specialised software and is associated with radiation exposure.37 Recently, hyper caloric drinking tests have been reported to be useful in assessing gastric accommodation.3,11,13 Some groups have reported high reproducibility and correlation with barostat3,13,19 while others did not find symptom concordance.11 We used the standardised nutrient challenge for assessment of sensory function. In a previous study,19 we have validated the approach; we compared this methodology with the “gold standard” barostat technique and could demonstrate that symptom responses were significantly correlated with the results of barostat testing. To our knowledge there are no studies that have compared fractional nutrient challenge with bolus drinks. We decided to use a fractional test because this better reflects real life and should be suitable for assessing mechanosensory function. However, we cannot argue that one method is superior to another with regard to discrimination of patient groups; further investigations regarding this issue are needed. In this context, it must be taken into consideration that the liquid nutrient challenge empties from the stomach into the duodenum and thus a concomitant delay in gastric emptying could affect the results. Noteworthy, gastric emptying delivers, on average, between 1 and 1.5 kcal per minute into the duodenum. Hence the relatively small amounts emptied into the duodenum should not have substantially influenced our results. Study subjects ingested the target volume of 600 ml within 15 minutes and caloric density was 1.5 kcal/ml. Therefore, it is highly unlikely that a disturbance in gastric emptying would have affected the results. Indeed, others have validated similar methodology.13 On the other hand, disturbed fundic relaxation38,39 could also have affected our findings, with antral distension occurring as a consequence of a diminished volume response of the proximal stomach.40 This in turn may have caused the augmented global symptom response observed in a subset of subjects. Other studies with nutrient test meals have used different caloric loads or time intervals over which the meal was ingested.13 As we have previously validated our methodology19 and our results are in line with other findings in consulters and non-consulters investigated with either a liquid meal13 or by barostat,6 we conclude that differences in the methodology are unlikely to have substantially affected the results.
Assessment of symptoms and categorisation of patients is a key issue. Importantly, in this study strict criteria were applied for assessment of the most bothersome symptom pattern for the first time. Dysmotility-type dyspepsia was linked to delayed gastric emptying. We also found a higher symptom score for fullness and nausea in patients with dysmotility-type FD after a nutrient load. We cannot determine whether delayed emptying of the test meal caused an augmented symptom response or whether visceral sensitivity or fundic disaccomodation contributed to the altered symptom response. A combination of various mechanisms is most likely the explanation of the remarkable overlap of symptoms.41,42 Interestingly, patients with predominantly ulcer-type dyspepsia also scored higher for fullness. This also argues in favour of a common mechanism in the various disease subgroups. We did not find any significant differences between blood donors and patients with IBS symptoms, most likely due to the small sample size.
GORD frequently overlaps with FD and, even in the absence of mucosal lesions, GORD can be the cause of upper abdominal symptoms. Thus this issue needs careful consideration. In the present study, however, patients with a history of structural lesions such as peptic ulcers or other peptic lesions, were not eligible for participation in the study. Furthermore, all patients with GORD symptoms only or patients with predominantly GORD symptoms were excluded. Thus it is reasonable to assume that our findings are not due to contamination of our study population with GORD patients.
In blood donors, the prevalence of H pylori was 48%. Thus it cannot be excluded that H pylori associated structural lesions were present as the cause of symptoms in at least some controls. However, it is unlikely that this would have influenced our results as previous studies in H pylori positive blood donors rarely found peptic ulcers.43 In addition, such effects would most likely only have blunted any differences. Furthermore, in line with previous findings, H pylori was neither associated with a specific symptom pattern16 nor did we observe any differences between H pylori positive and negative subjects regarding gastric emptying and the symptomatic response to the test meal. Our findings related to gastric emptying and H pylori are in line with most investigations in patients44,45 but not all.46 Thus the observed association of symptom patterns with abnormalities of function appears to be reasonable robust.
While 19% of patients tested positive for H pylori, slightly more than half of the blood donors tested positive for H pylori IgG antibodies. The significant difference between our blood donor population and patients might be explained by the efforts of referring physicians to treat symptoms by H pylori eradication that failed to control symptoms. Thus the positive control (patients) may represent a group of patients who are refractory to conventional therapeutic measures. This must be kept in mind when differences in primary outcome parameters are being considered.
In summary, abnormalities of gastric emptying and augmented symptom responses to a standardised nutrient challenge (reflecting abnormalities of sensory function, disturbances of fundic relaxation, or both) were highly prevalent in blood donors with relapsing unexplained gastrointestinal symptoms and patients with functional gastrointestinal disorders. Disturbances in function however were more severely impaired in patients compared with non-health care seeking blood donors with symptoms.