Article Text

Abstract
Background and aims: Empiric proton pump inhibitor (PPI) trials have become increasingly popular leading to gastroenterologists frequently evaluating gastro-oesophageal reflux disease (GORD) patients only after they have “failed” PPI therapy. Combined multichannel intraluminal impedance and pH (MII-pH) monitoring has the ability to detect gastro-oesophageal reflux (GOR) episodes independent of their pH and evaluate the relationship between symptoms and all types of GOR. Using this technique, we aimed to characterise the frequency of acid and non-acid reflux (NAR) and their relationship to typical and atypical GOR symptoms in patients on PPI therapy.
Methods: Patients with persistent GORD symptoms referred to three centres underwent 24 hour combined MII-pH monitoring while taking PPIs at least twice daily. Reflux episodes were detected by impedance channels located 3, 5, 7, 9, 15, and 17 cm above the lower oesophageal sphincter (LOS) and classified into acid or non-acid based on pH data from 5 cm above the LOS. A positive symptom index (SI) was declared if at least half of each specific symptom events were preceded by reflux episodes within five minutes.
Results: A total of 168 patients (103 (61%) females and 65 (39%) males; mean age 53 (range 18–85) years) underwent combined MII-pH monitoring while taking PPIs at least twice daily. One hundred and forty four (86%) patients recorded symptoms during the study day and 24 (15%) patients had no symptoms during testing. Sixty nine (48%) symptomatic patients had a positive SI for at least one symptom (16 (11%) with acid reflux and 53 (37%) with NAR) and 75 (52%) had a negative SI. A total of 171 (57%) typical GORD symptoms were recorded, 19 (11%) had a positive SI for acid reflux, 52 (31%) for NAR, and 100 (58%) had a negative SI. One hundred and thirty one (43%) atypical symptoms were recorded, four (3%) had a positive SI for acid reflux, 25 (19%) had a positive SI for NAR, and 102 (78%) had a negative SI.
Conclusion: Combined MII-pH identifies the relation of reflux of all types to persistent symptoms and the importance of NAR in patients taking PPIs.
- MII-pH, multichannel intraluminal impedance and pH
- LOS, lower oesophageal sphincter
- TLOSR, transient lower oesophageal sphincter relaxation
- GOR, gastro-oesophageal reflux
- GORD, gastro-oesophageal reflux disease
- PPI, proton pump inhibitor
- SI, symptom index
- SAP, symptom association probability
- NAR, non-acid reflux
- multichannel intraluminal impedance and pH
- gastro-oesophageal reflux disease
- non-acid reflux
Statistics from Altmetric.com
- MII-pH, multichannel intraluminal impedance and pH
- LOS, lower oesophageal sphincter
- TLOSR, transient lower oesophageal sphincter relaxation
- GOR, gastro-oesophageal reflux
- GORD, gastro-oesophageal reflux disease
- PPI, proton pump inhibitor
- SI, symptom index
- SAP, symptom association probability
- NAR, non-acid reflux
Patients with symptoms thought to be secondary to reflux are treated empirically with proton pump inhibitors (PPIs), and those who fail to respond are referred to a centre to evaluate their persisting symptoms on therapy. A normal pH test (that is, normal distal oesophageal acid exposure with a negative symptom index) off therapy is a strong indicator that the patient does not have gastro-oesophageal reflux disease (GORD) but an abnormal pH test off therapy does not explain why the patient has symptoms on therapy. Conversely, an abnormal pH test on therapy can be used to support ongoing acid reflux causing the residual symptoms but a normal pH test on therapy prompts the question of whether residual symptoms could be due to non-acid reflux (NAR) not detected using conventional pH monitoring.
It has been shown that even though up to 90% of patients with erosive oesophagitis achieve endoscopic healing, 35% or more still have persistent symptoms despite PPI therapy.1 Reviewing the available technologies to detect GORD, a panel of experts in gastro-oesophageal disorders concluded: “reflux is best detected by impedance and its acidity characterised by pH-metry”.2 Indeed, combined multichannel intraluminal impedance and pH (MII-pH) has the ability to detect reflux episodes independent of the pH of the refluxate by changes produced by bolus presence in the oesophagus and classify it as acid or non-acid by concomitantly recorded pH. In patients with ongoing symptoms on PPI therapy, combined MII-pH, in contrast with conventional pH, offers a more complete evaluation of the relationship between symptoms and gastro-oesophageal reflux (GOR, both acid and non-acid).3,4 MII-pH testing for GORD has also been shown to be reproducible for all types of reflux.5,6 The aim of our study was to clarify the relationship between typical and atypical GOR symptoms and reflux episodes (acid and non-acid).
MATERIALS AND METHODS
The Institutional Review Board at the three participating centres (Medical University of South Carolina, Cleveland Clinic Foundation, and Catholic University of Leuven, Belgium) approved this retrospective analysis of prospectively collected data.
Patient population
Starting January (Medical University of South Carolina) and July 2002, all patients with persistent symptoms, despite PPI therapy, referred to the oesophageal laboratory underwent combined MII-pH monitoring. Prior to the study, patients and/or the referring physician were contacted by the gastroenterology fellow to ensure that the patient had been on at least twice daily PPI for at least a month or more prior to testing. Based on symptoms, patients were categorised as having typical GORD symptoms (heartburn, regurgitation, or chest pain) or atypical symptoms (cough, hoarseness, abdominal discomfort, nausea, belching, throat discomfort, mucous, globus, hiccups, wheeze, and sour taste).
Patients presented to the oesophageal laboratory after at least four hours of fasting. The combined MII-pH probe was placed in reference to the manometrically located proximal border of the lower ooesophageal sphincter (LOS) using a station pull through technique. On completion of the manometry a 2.1 mm MII-pH cathteter was passed transnasally and the oesophageal pH sensor was positioned 5 cm above the LOS. The configuration of the catheter allowed monitoring changes in intraluminal impedance at 3, 5, 7, 9, 15, and 17 cm above the LOS. In addition, pH was monitored at 5 cm above and 10 cm below the LOS.
Patients then underwent 24 hour MII-pH monitoring and diaries were provided for patients to record symptoms during the study period. Data from the impedance channels and pH electrodes were sampled at a frequency of 50 Hz and stored on a portable data recorder (Sleuth; Sandhill Scientific, Inc. Highlands Ranch, Colorado, USA). At the end of the 24 hour recording period, data were transferred and analysed manually using dedicated software (Bioview Analysis; Sandhill Scientific Inc.). Tracings were reviewed and timing of meals, changes in body position, and the time of symptoms recorded were compared with the information written in the diaries. Meal periods were marked and excluded from the analysis. Liquid containing reflux episodes (liquid only and mixed gas-liquid) were identified by previously described criteria7 as a retrograde 50% decline in impedance from baseline in at least two sites. Gas only reflux episodes (simultaneous increase in impedance >3000 Ω in any two consecutive sites with one site having an absolute value >7000 Ω) were not included in the analysis. Impedance detected reflux episodes were classified as acid if the pH sensor recorded a decline in pH to below 4 or as non-acid if the pH remained above 4 during bolus presence time in the oesophagus. The group of NAR episodes includes reflux episodes classified in other publications as “weakly acidic” and “weakly alkaline”.2 We prefer using “acid” versus “non-acid” as this separation allows a better contrast in the implication and therapeutic approach from the gastrointestinal perspective.
Combined MII-pH data allowed separation of symptoms into those associated with acid reflux, NAR, or not associated with reflux. The primary endpoint for the study was the symptom index (SI). A symptom was considered to be associated with reflux if a reflux episode was detected five minutes prior to the time of the symptom. SI was defined as the number of symptoms associated with reflux divided by the total number of symptoms. Separate SIs were determined for each individual symptom if patients recorded different types of symptoms. A positive SI (+SI) was declared if ⩾50% (that is, at least half of symptoms associated with reflux).8 The symptom association probability (SAP) was calculated by dividing the 24 hour pH data into two minute segments. Each of the two minute segments was studied whether reflux occurred in it and if a symptom occurred during the segment. A 2×2 table was made in which the number of two minute segments with and without reflux and with and without symptoms were tabulated. The probability of the distribution of symptoms and reflux episodes in two minute windows was then calculated to determine if it could have occurred by chance (χ2 test); SAP = 1−p. SAP was positive if >95%.9 Patients were considered to have an overall positive SI or SAP if at least one symptom was positive.
Abnormal distal oesophageal acid exposure on therapy was defined as pH>1.6 in the upright position and >0.6 in the recumbent position.10 Meals were excluded from the analysis. Tracings obtained during the study were also interpreted using a dedicated software program (Bioview Analysis; Sandhill Scientific Inc.). Each study was read twice, first by the gastroenterology fellow and then by the consultant gastroenterologist.
Statistical analysis
Data were analysed using the SPSS 12.0 Basic software package of statistical programs. The χ2 test was used for comparison between typical and atypical symptom groups. Significance was established at p<0.05.
RESULTS
The study included 168 patients (103 (61%) females and 65 (39%) males; mean age 53 (range 18–85) years) from three centres who underwent ambulatory combined MII-pH monitoring while taking at least twice daily PPI from January 2002 until October 2004. Mean study duration was 20.0 hours. Patients recorded between one and four types of symptoms: 42 (29%) recorded one type of symptom, 50 (35%) recorded two different types of symptoms, 48 (33%) recorded three different types of symptoms, and only four (3%) patients recorded four different types of symptoms. From the 168 patients monitored, 144 (86%) recorded symptoms during the study day and 24 (14%) patients had no symptoms during testing. Of the 302 symptoms recorded, 171 (57%) were typical GORD symptoms and 131 (43%) atypical symptoms (table 1⇓). Of the 168 patients studied on twice a day therapy, 18 (11%) had abnormal distal oesophageal acid exposure.
Symptom analysis using symptom index (SI) and symptom association probability (SAP) for each symptom
Reflux episodes
In the 168 patients, 5571 liquid containing events were recorded. Among these, 967 (17.3%) were acid and 4604 (82.7%) non-acid. Among NAR episodes, 4138 (89.8%) were “weakly acid” and 466 (10.2%) “weakly alkaline”. The numbers of reflux episodes (fig 1⇓) were analysed. Forty eight or more was used as the abnormal number of reflux episodes. The median number of total reflux episodes was 25 (25th–75th percentile 10–45). The median number of reflux episodes for acid was 1 (25th–75th percentile 0–5) and for non-acid 20 (25th–75th percentile 9–38).

Number of reflux episodes (normal <48) during 24 hour multichannel intraluminal impedance and pH monitoring
Symptom index
One hundred and seventy one (57%) typical and 131 (43%) atypical GORD symptoms were recorded. Sixty nine (48%) symptomatic patients had a positive SI (16 (11%) with acid reflux and 53 (37%) with NAR) and 75 (52%) had a negative SI (fig 2⇓). Of patients with typical symptoms on study day, 19 (11%) had a positive SI for acid reflux, 52 (31%) for NAR, and 100 (58%) had a negative SI. Of the patients with atypical symptoms on study day, four (3%) had a positive SI for acid reflux, 25 (19%) had a positive SI for NAR, and 102 (78%) had a negative SI. Typical symptoms were more likely to be associated with reflux compared with atypical symptoms (p<0.01).

Multichannel intraluminal impedance and pH monitoring using the symptom index (SI).
Symptom association probability
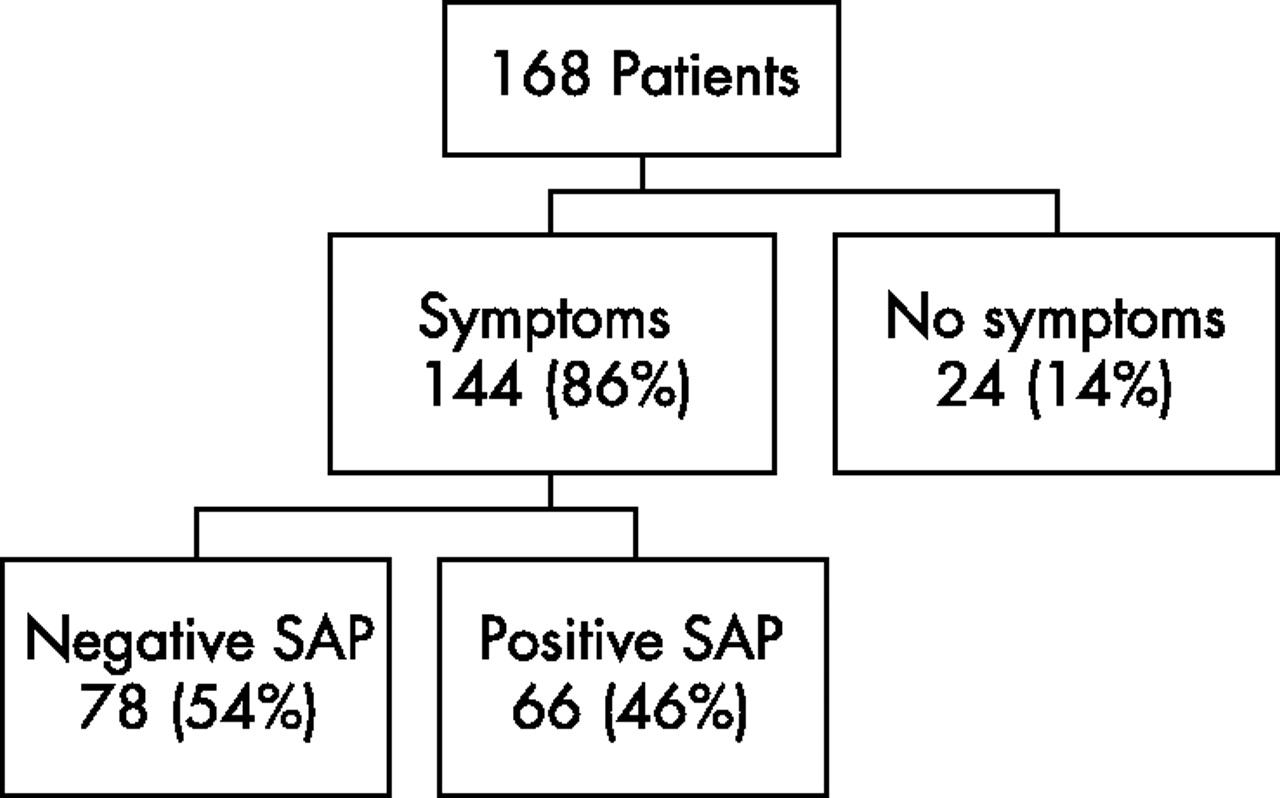
Of the 144 symptomatic patients, 66 (46%) had a positive SAP and 78 (54%) had a negative SAP (fig 3⇓). Of patients with typical symptoms on study day, 60 (35%) had a positive SAP with acid/NAR and 111 (65%) had a negative SAP. Of patients with atypical symptoms on study day, 31 (24%) had a positive SAP with acid/NAR and 100 (76%) had a negative SAP. Agreement between SAP and SI was poor (kappa = 0.3) with a sensitivity of only 51% and specificity of 78%.
{kind=link}
{kind=link}
{kind=link}
Multichannel intraluminal impedance and pH monitoring using the symptom association probability (SAP).
DISCUSSION
The results of this multicentre study indicate that 37% of patients on at least twice daily PPIs with study day symptoms had a positive SI for NAR. These patients would have been interpreted as negative if they were studied using conventional pH only. We also found that symptoms after acid reflux on at least twice daily PPI occurred in a minority of patients (11%) and 52% of patients on at least twice daily PPI with study day symptoms had a negative SI during the 24 hour MII-pH study. This finding is important in the overall management of these patients as an alternative diagnosis rather than GORD can be sought.
We reported on the types of reflux temporally related to symptoms on PPI therapy. Using MII-pH, we were able to characterise the type of reflux (non-acid and acid) associated with the symptom (typical or atypical). Typical GORD symptoms on PPI therapy were more likely to be associated with a positive SI, primarily non-acid (42%), compared with atypical symptoms (22%) which were more likely to be associated with no reflux. Using MII-pH in patients presenting with atypical symptoms appears to be best used to exclude GORD as the cause.
Acid reflux related to symptoms was reported in only a small number of patients. These results are similar to our previous analysis of 100 patients.11 A previous report by Shay et al showed a similar frequency of patients with NAR associated symptom but a higher frequency (22%) of patients with symptoms associated with acid reflux.12 This finding is likely related to the frequent (48%) addition of a nighttime H2 receptor antagonist to PPI therapy in our report. In this study, 10% of the patients on a PPI twice daily only had a positive SI for acid reflux compared with none in the combination therapy group. This was not statistically significant as the number of patients analysed was too small, probably causing a type II error. The results from this study showed that this additional therapy achieved significantly better overall gastric acid control with less NAR, a finding supported by previous studies.13–,15
The accuracy of MII in detecting individual reflux events was evaluated by Shay et al. They studied 10 GORD patients and 10 normal volunteers using MII-pH in combination with manometry. Patients had 30-fold more reflux episodes than volunteers and MII detected 95% of all reflux events identified by pH-metry or manometry alone.16
The effects of omeprazole were studied by Vela et al in 12 patients who underwent two two hour postprandial studies using impedance pH monitoring before and after therapy. The results showed that postprandial reflux was primarily NAR, especially on omeprazole, and that these episodes were detected by MII but not by pH. They also found that symptoms occurred with both acid and NAR and concluded that patients with persistent symptoms despite acid suppression should be further evaluated using MII-pH.17
The number of reflux episodes in the present study was lower than that found in a previous report of normal volunteers quite likely due to PPI therapy.11 The mechanism for this may be inhibition of acid causing a decrease in gastric volume and distension resulting in fewer transient lower oesophageal sphincter relaxations (TLOSRs).
At present there are few pharmacological agents available for the treatment of NAR. Vela et al studied the effect of baclofen, a γ-aminobutyric acid B agonist, on acid and NAR and their associated symptoms in the postprandial period. They demonstrated that baclofen, which inhibits TLOSRs, decreased the number of acid and NAR episodes as well as the number of associated symptoms.18,19 Baclofen can be used as a therapeutic option; however, its use is limited because of side effects. Fundoplication has been used as a treatment for patients with acid reflux and has been shown to be both effective and safe with long term control.20,21 At present, we are accumulating data on patients with persistent symptoms with a positive SI evaluated using MII-pH for either acid or NAR referred for a fundoplication.22 Initial data have shown that a positive SI for non-acid or acid reflux using MII-pH predicts a successful response to antireflux surgery.
SAP has been used in many studies in the final analysis of patients with GORD symptoms and takes into account the total number of reflux events. In our study, the kappa score between these two indices was poor at only 0.3, showing little concordance between SI and SAP. Outcome studies in patients with discordance between the SI and SAP using MII-pH are needed. The use of SI with a five minute window is particularly appropriate for the work described in this report as we just completed an analysis of reflux/symptom relationships that indicated that time to symptoms is significantly longer for NAR than for similar symptoms with acid reflux. The recent PPI outcomes publication by Taghavi et al showed the SI to be more specific than SAP, and in our study one could argue in favour of better specificity.23
In conclusion, the results from our 168 patients showed that those with symptoms on PPI therapy continued to have reflux, either acid or non-acid. The advantages of 24 hour impedance-pH include the ability to simultaneously assess the adequacy of acid suppression, analyse persistent symptoms association with acid or NAR despite heavy acid suppression, and measurement of reflux episode frequency. Combined multichannel intraluminal impedance and pH clarifies the mechanisms underlying persistent symptoms during PPI therapy and shows that clinical presentation, not pH alone, is not sufficient to identify the presence or absence of reflux causing symptoms. The management of these patients needs to be further evaluated with outcome studies involving medical or surgical approaches.
REFERENCES
Footnotes
Published online first 23 March 2006
Conflict of interest: None declared.
Oral presentation at the 69th Annual Meeting of the American College of Gastroenterology, Orlando, FL, October, 2004