Article Text

Abstract
Background:: Standard triple therapies are the most used treatment in clinical practice. However, a critical fall in the H pylori eradication rate following these therapies has been observed in the last few years. The sequential regimen is a novel, promising therapeutic approach.
Objectives:: To evaluate the available data on the sequential therapy regimen.
Methods:: A pooled-data analysis of all studies on the sequential regimen was performed. The eradication rate was calculated according to gastroduodenal pathology, proton pump inhibitor used, antibiotic resistance, as well as setting (paediatric or geriatric patients). Compliance, side effects, and cost implications were also evaluated.
Results:: Overall, more than 1800 patients have been treated with the sequential regimen. Such a therapy was superior to 7–10 days triple therapies in paediatric, adult and elderly patients, achieving an eradication rate constantly higher than 90% at ITT analysis. Although primary clarithromycin resistance reduced the efficacy of such a therapy, a success rate significantly higher than that observed with the standard 7–10 days triple therapies was found.
Conclusion:: The 10-day sequential treatment regimen achieves higher eradication rates than standard triple therapies.
- CagA, cytotoxin-associated gene A
- ITT, intention to treat
- PP, per protocol
- PPI, proton pump inhibitor
Statistics from Altmetric.com
Twenty-five years since the discovery of H pylori, treatment remains a challenge for the clinicians and no proposed therapy regimen has been able to eradicate the infection in all treated patients. Seven day triple therapies (proton pump inhibitor, clarithromycin plus amoxicillin or metronidazole) as suggested in the European guidelines,1 are the most used treatments in clinical practice, being currently prescribed by 85%, 84% and 67% of primary-care physicians in Italy, Israel and US, respectively.2–4 However, recent data suggest that the efficacy of these therapies is decreasing worldwide.5,6,7,8,9,10,11,12 Indeed, the success rate in most European and Asian countries, as well as in the US and Canada, has declined to unacceptable levels with > 1 in 5 patients failing eradication therapy, and cure rates as low as 20–45% have been recently reported.13,14 This phenomenon has been largely related to a worldwide increase of bacterial resistance, particularly against clarithromycin – the key antibiotic in the H pylori treatment.15 Therefore, an increasing number of patients actually require a second or further therapeutic attempt to eradicate the infection, this has also substantial economic implications.
The updated European guidelines confirmed the use of a standard seven day triple therapy in those areas where clarithromycin resistance is lower than 15−20%, while a prolonged 14 day regimen or a 10−14 day quadruple therapy should be administered when bacterial resistance is higher.16 However, several studies found that the eradication rates achieved with these therapies are far from satisfactory. A meta-analysis has clearly shown that the 14-day triple therapy offers only a modest improvement over the seven day regimen in terms of H pylori eradication rates (5?8%), in spite of a twofold increase in the treatment cost.17 In Italy, a recent multicentre study involving 906 patients with duodenal ulcer failed to show even a modest therapeutic gain, H pylori infection being cured in 79.7% and 81.7% of patients receiving a seven day or a 14 day triple therapy, respectively.18 Another Italian study, enrolling 486 patients, found an eradication rate as low as 52–57% following 1-week standard triple therapies, only increasing to 56−70% when the same regimens were prolonged to 14 days.19 As far as the quadruple therapy is concerned, a meta-analysis failed to find a significant difference in the success rate between seven day quadruple and standard triple therapies as a first-line treatment.20 In addition, bismuth salts are no longer available in several countries, including Italy, so that the quadruple therapy is not feasible worldwide.
All these observations suggest that other therapeutic approaches to cure H pylori are needed, the best first-line treatment being still regarded as the best “rescue” therapy.21 The most obvious question to be addressed is whether a first-line therapy regimen more effective than the suggested 14 day triple or quadruple therapies is already available. In 2000, we performed the first pilot study using a novel, 10 day sequential regimen, achieving a very high eradication rate.22 In the following years, several therapeutic trials have compared this sequential regimen with the standard 7−10 day triple therapies, supporting the efficacy of the new treatment even against clarithromycin resistant strains. In order to definitely understand whether such a novel therapy is ready to be used as first-line treatment in clinical practice, we reviewed the published studies on the sequential regimen performing a pooled-data analysis of the available results.
THE SEQUENTIAL REGIMEN: FROM BENCH TO THE BEDSIDE
The sequential regimen is a simple dual therapy including a proton pump inhibitor (PPI) plus amoxicillin 1 g (both twice daily) given for the first five days followed by a triple therapy including a PPI, clarithromycin 500 mg, and tinidazole (all twice daily) for the remaining five days.22 We conceived such a novel therapeutic combination based on a previous observation that the eradication rate achieved by 14 days dual therapy followed by seven days triple therapy in eradication failure patients was significantly higher than that obtained when inverting such treatment sequence (97.3% vs 81.6%).23 At this point, we speculated that a dual therapy followed by a triple therapy was able to eradicate the infection in a very large number of patients. In order to apply this observation to clinical practice, we needed to simplify such a therapeutic combination. For this reason, we decided to reduce each treatment schedule to five days. Indeed, it was known that a dual therapy (PPI plus amoxicillin) administered for less than seven days was able to achieve a cure rate up to 50%,24 and that the efficacy of a triple therapy (PPI, clarithromycin and tinidazole) was inversely related to the bacterial load with higher eradication rates being achieved in those with a low bacterial density in the stomach.25–27
Therefore, we pioneered a 10 day sequential regimen consisting of a short, initial dual therapy with amoxicillin aiming to lower the bacterial load in the stomach in order to improve the efficacy of the immediately subsequent short course of triple therapy. Moreover, the initial use of amoxicillin may offer another essential advantage for H pylori eradication. It has been found that regimens containing amoxicillin prevent the selection of secondary clarithromycin resistance.28 Indeed, it is known that bacteria can develop efflux channels for clarithromycin, which rapidly transfer the drug out of the bacterial cell, preventing binding of the antibiotic to the ribosome.29–31 It has been speculated that the disruption of the cell wall caused by amoxicillin prevent the development of efflux channels by damaging the cell wall of the bacterium.
In the first pilot study22 a very high eradication rate (98%) was achieved with the sequential regimen, and such an unexpectedly remarkable result was virtually duplicated in a further, two centres, pilot study.32 These findings suggested that the basic theory of the sequential combination of antibiotics was successful when applied to clinical practice, initiating a number of trials on the use of such a therapy regimen, which have been published in the last 6 years. The sequential therapy scheme is provided in fig 1.

The sequential therapy regimen.
THE OVERALL ERADICATION RATE
In table 1 a descriptive analysis of the 15 available studies on the sequential therapy is provided.22,32–45 Of them, two are pilot studies22,32 and 13 are randomised trials, including eight monocentre and seven multicentre-trials, which have been performed in nine different units throughout Italy. All but two of these trials have been published as a full paper.33,36 A further study on the sequential regimen is available, but it was not included, representing a post hoc analysis of a previous trial.46 As shown in table 1, the sequential regimen achieved H pylori eradication in 1687/1805 treated patients, with an overall eradication rate of 93.5% at intention to treat (ITT) analysis. The eradication rate was consistently higher than 90% for all but one small study performed in children.44
Overall eradication rate following sequential therapy at intention to treat (ITT) and per protocol (PP) analysis
COMPARISON WITH STANDARD 7−10 DAY TRIPLE THERAPY
A head-to-head comparison between the sequential regimen and a standard 7-day triple therapy has been performed in 8 randomised trials.33,34,36,39–43 At ITT analysis, the infection was cured in 1073/1145 (93.7%) patients and in 878/1156(75.9%) patients following the sequential regimen and the seven day triple therapy, respectively. The difference was significant (93.7% vs 75.9%; p<0.001).
A head-to-head comparison between the sequential regimen and the standard 10 day triple therapy has been performed in four randomised trials.38,39,43,45 At ITT analysis, the infection was cured in 354/379 (93.4%) patients and in 309/388 (79.6%) patients following the sequential regimen and the 10 day triple therapy, respectively. The difference was significant (93.4% vs 79.6%; p<0.001).
ERADICATION RATE IN PEPTIC ULCER AND NON-ULCER DYSPEPSIA PATIENTS
Some data suggest that following standard triple therapies the eradication rate in non-ulcer dyspepsia tends to be lower than in peptic ulcer patients.47 The head-to-head comparison between sequential regimen and standard triple therapy (7−10 days) in these two patient sub-groups are available in four studies.32,34,38,39 Overall, the H pylori infection was cured in 199/204 (97.5%) peptic ulcer patients and in 496/540 (91.7%) non-ulcer dyspepsia patients with sequential regimen, and in 217/293(74.1%) and 433/576 (75.2%)patients, respectively, following a triple therapy. The difference between sequential and standard therapy was significant in both patients with peptic ulcer (97.5% vs 74.1%, p<0.001) and in patients with non-ulcer dyspepsia (91.7% vs 75.2%, p<0.001). The eradication rate did not differ between peptic ulcer and non-ulcer dyspepsia matched sub-groups following either sequential or standard therapy.
ROLE OF DIFFERENT PROTON PUMP INHIBITORS
Different PPIs have been used in the sequential combination. Bacterial eradication was achieved in 271/287 (94.4%) patients following the omeprazole-based regimen,22,32,33 in 133/146 (91.1%) patients with pantoprazole,45 in 1011/1086 (94.4%) patients with rabeprazole,34,35,37–41,43 and in 272/286 (95.1%) patients with the esomeprazole.36,42,44 The success rate among the different PPIs used was not significant. No data with lansoprazole are available.
ERADICATION RATE IN CHILDREN
The eradication rate following standard seven day triple therapy in children is known to range from 68%–75%.48,49 To date, two small trials performed in the same centre are available on the use of sequential regimen in dyspeptic children (median age: 12.3 years; range 3.3−18).40,44 In the first randomised study,40H pylori infection was cured in 36/38 (94.4%) and in 28/37 (75.7%) children following the sequential and seven day triple therapy, respectively (p = 0.02). In the second study,44 the bacterial eradication was achieved in 33/40 (82.5%) children receiving the sequential regimen (with or without a probiotic supplementation). Therefore, the cumulative analysis found that H pylori infection was cured in 69/78 (88.5%) treated children.
ERADICATION RATE IN OLDER PATIENTS
The results of Italian studies, overall enrolling 387 patients, showed that H pylori eradication in older patients was 79.3% following the standard seven day triple therapy.50–52 To date, only one randomised study involving 179 peptic ulcer geriatric patients (mean age: 69.5 years; range: 65–83) is available on the use of sequential regimen.43 At ITT analysis, the infection was cured in 84/89 (94.4%) and in 72/90 (80%) patients following the sequential and the seven day triple therapy, respectively (p = 0.008).
FACTORS AFFECTING ERADICATION RATE
Several factors have been found to affect the efficacy of standard triple therapies, such as bacterial resistance to antibiotics,15 compliance to therapy,21 bacterial load in the stomach,25–27 CagA status,38 smoking habit,53 and gastroduodenal pathology.48 However, among these factors, both bacterial clarithromycin resistance and patient compliance to the therapy play a major role in predicting the therapeutic outcome.15 In detail, primary clarithromycin resistance is regarded as the main factor affecting the efficacy of treatment, reducing the success rate of standard triple therapies to mean values as low as 18−44%.54
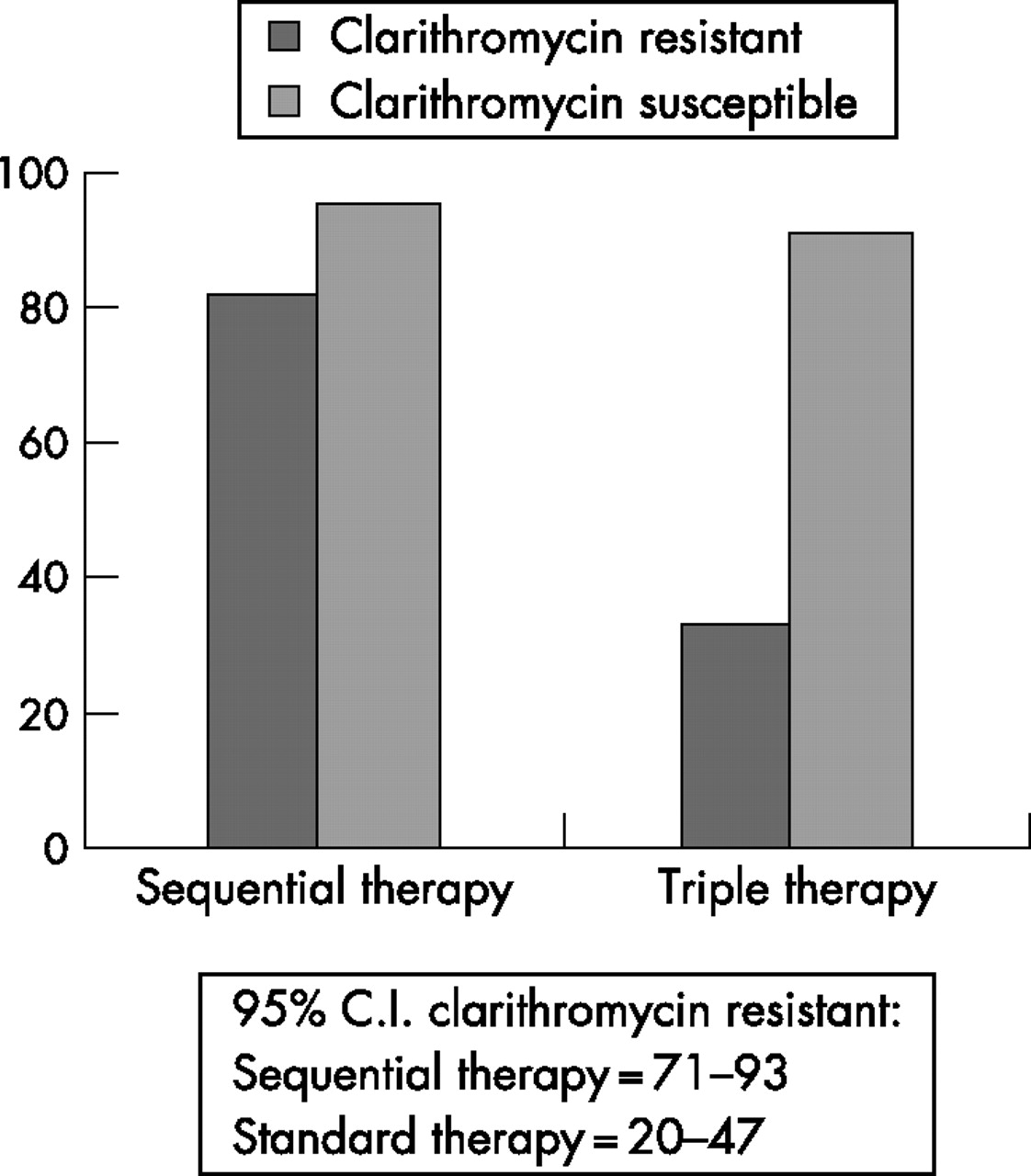
Data on primary clarithromycin resistance and H pylori eradication following the sequential regimen are available in three trials.34,45,46 Overall, the infection was cured in 41/50 (82%) patients and in 16/48 patients (33.3%) infected with clarithromycin (with or without metronidazole) resistant strains following the sequential and standard triple therapy, respectively (fig 2). Therefore, a significantly higher eradication rate was achieved following the sequential therapy as compared to the 7−10 day triple therapies (82% vs 33.3%; p = 0. 001). In detail, the sequential regimen was much more effective than triple therapy even in those patients harbouring a clarithromycin resistant strain due to the A2143G point mutation, which was found to play a major role in reducing the eradication rate of triple therapy.46
{kind=link}
{kind=link}
H pylori eradication following either sequential or standard therapy regimen according to clarithromycin resistance. Cumulative data of three studies.
Data on metronidazole resistance and H pylori eradication following the sequential regimen are available in two trials.34,45 Overall, the infection was cured in 68/71 (95.8%) patients and in 46/59 (78%) patients infected with metronidazole resistant strains following the sequential and standard triple therapy, respectively. Therefore, despite of inclusion of tinidazole, the sequential regimen achieved a significantly higher eradication rate as compared to the tinidazole-free, 7−10 day triple therapies (95.8% vs 78%; p = 0.005).
Other studies found that, unlike the standard triple therapy, the cure rate achieved by the sequential therapy is not significantly affected by the gastroduodenal pathology (peptic ulcer versus non-ulcer dyspepsia), bacterial strain (CagA positive versus negative), bacterial load in the stomach (low versus high), and smoking habit.38,43
COMPLIANCE AND SIDE-EFFECTS
Compliance to the therapy is another major factor influencing the therapy outcome. Generally, a good compliance is defined as consumption of more than 90% of the prescribed drugs. Full data on the patient compliance and side-effects incidence are available in 8 trials comparing the sequential and triple therapies.29,31,34,41–43,45 Overall, no difference emerged between the two treatments, a good compliance to the therapy being observed in 1004/1085 (92.6%) patients receiving the sequential regimen and in 1203/1280 (94%) patients treated with a triple therapy. In the same studies, the incidence of side-effects was 9.9% and 9.8%, respectively. The most frequent side-effects complained are listed in table 2. Overall, side-effects required the interruption of therapy in only 3/1085 (0.003%) and in 9/1280 (0.007%) patients receiving sequential and triple therapy, respectively. All these observations suggest that the sequential regimen and standard triple therapy are characterised by a similar patient compliance, incidence of side-effects, and therapy interruption rate.
List of side-effects reported in adult patients treated with the sequential regimen
COST IMPLICATIONS
Since H pylori infection is a widespread disease, the cost of therapy is surely a matter of concern. The overall cost of management largely depends on the efficacy of first-line therapies. Indeed, the failure of an initial therapy requires both a generally more costly and less effective further attempt and an additional post-therapy test to check for the bacterial eradication. Consequently, the ideal treatment for H pylori infection is a cheap, highly effective first-line therapy.55 The pharmaceutical cost of sequential therapy in Italy is nearly €30 higher than seven day triple therapy, but €34 lower than 10 day triple regimen.35,37 Moreover, tinidazole has recently become available in the US, where the cost of the 10 day sequential therapy is nearly $30 lower than that of the 10 day triple therapy.45 This economic advantage is further strengthened by the consideration that a first-line therapy with the sequential regimen is 15−20% more effective than standard 7−10 day triple therapies.
LIMITATIONS
The main disadvantage of the sequential regimen is that it includes amoxicillin and, therefore, it is not suitable for patients with a penicillin allergy. However, such a limitation also applies for one of the standard triple therapies suggested in the European guidelines, which are the most currently used first-line therapy regimens in the clinical practice both in Europe and US.1–5
Another limitation is that data regarding the efficacy of the sequential regimen came only from Italian studies. Hence, it is unknown whether the same performance would occur in other countries. Recent data suggest that prevalence of primary clarithromycin resistance is elevated in Italy, with values as high as 24%.46,56,57 Therefore, at least a similarly high success rate may be expected in those countries where a similar (or lower) H pylori clarithromycin resistance is present. Of note, preliminary data of an ongoing pilot, observational study performed in the clinical practice in Spain found a ‘per protocol’ eradication rate of 90.7%.58
RESCUE THERAPY AFTER SEQUENTIAL REGIMEN FAILURE
When a novel therapy for H pylori eradication is suggested for clinical practice, it is of paramount importance to identify a second-line therapy which may be used in the event of failure. A levofloxacin-amoxicillin-based triple therapy has been proved to be acceptably effective as second- or even third-line therapy.59–61 Two recent meta-analyses showed a higher eradication rate of this regimen as compared to standard quadruple therapy as a retreatment.62,63 We recently performed a pilot study on 35 patients who failed the sequential regimen.64 Following a 10 day triple therapy with rabeprazole 20 mg, levofloxacin 250 mg and amoxicillin 1 g, all twice daily, H pylori infection was successful cured in 30 patients, accounting for a 85.7% (95% CI = 74 to 97) eradication rate at ITT analysis. These data seem to indicate that levofloxacin-amoxicillin triple therapy is a suitable therapeutic approach for second-line treatment in sequential therapy failure patients. Therefore, the 10 day sequential regimen plus the 10 day levofloxacin-based triple therapy appears to be a convincing ‘therapeutic package’ for H pylori management in the clinical practice.
CONCLUSIONS
Standard triple therapies are the most used treatment in the clinical practice.1–5 However, a critical fall in the H pylori eradication rate following these therapies has been observed in the last few years.18,19 This finding is most likely a result of an increased clarithromycin resistance. Indeed, a large study performed in 14 European countries showed a primary clarithromycin rate as high as 20% even in children.65 Similarly, recent Italian studies found a prevalence rate ranging from 16.9% to 31.5% in adults.45,46,56,57 To improve the efficacy of triple therapy in those areas with >15−20% primary clarithromycin resistance, the use of 14-day regimen or a 10−14 day quadruple therapy has been recently proposed in the updated European guidelines.16 However, as mentioned, quadruple therapy is no more feasible in Italy, and the prolonged 14-day triple therapy has an unfavourable cost-efficacy ratio.20 In recent years, very few potential agents with a bactericidal action against this bacterium have been identified.66
The sequential regimen is a novel therapeutic approach based on a different combination of the available antibiotics, and more than 1800 patients have been treated with such a therapy. It is the only therapeutic regimen that has been proven to be superior to 7−10 day triple therapies in large, multicentre, randomised trials. Moreover, the sequential regimen has achieved an eradication rate consistently higher than 90% at ITT analysis in all but one small study performed in children. Primary clarithromycin resistance seems to be the only factor reducing the efficacy of this therapy regimen. However, even in these patients, an acceptable >75% eradication rate can be achieved following the sequential therapy, a success rate significantly higher than that observed with the standard 7−10 day triple therapies (<35%).34,45,46
The attention towards the sequential therapy regimen is increasing in literature. Several authoritative experts have defined such a therapeutic approach as “appealing”,67–74 and the International panel of the European guidelines advised that “sequential therapy deserves further evaluation in different regions”.16 Finally, the sequential regimen has been given equivalent status to standard 7–14 triple therapies as first-line treatment in the updated Italian guidelines on H pylori management.75 We therefore encourage gastroenterologists to validate the sequential therapy in other geographical areas where data is still lacking.
REFERENCES
Footnotes
-
Published Online First 13 June 2007
-
Competing interests: D. Vaira holds stock options for Meridian Bioscience, Cincinnati, Ohio, USA.
Linked Articles
- Digest