Article Text

Abstract
Background/Aims: Whether a life-long gluten-free diet (GFD) is necessary in all children with diagnosed coeliac disease (CD) remains debated. To address this question, a retrospective analysis of the clinical and biological status of adult coeliac patients diagnosed in childhood, who remained on a normal diet after gluten challenge and were clinically silent, was carried out.
Methods: Patients aged 18–65 years with CD diagnosed in childhood were included. Clinical status, gluten intake, biological parameters of malabsorption, bone mineral density, human leucocyte antigen (HLA) genotype, serological markers of CD, and histological and immunohistochemical parameters in duodenal biopsies were recorded.
Results: Sixty-one patients had resumed a normal diet and were asymptomatic. Forty-eight showed different degrees of villous atrophy (silent CD), while 13 had no detectable atrophy (latent CD) on duodenal biopsies. Latent CD patients had significantly less osteopenia/osteoporosis (1/9 (11%) vs 23/33 (70%), p<0.001)), and lower T cell receptor (TCR) αβ+ intraepithelial T cell counts (38±20 vs 55±15, p<0.01) than silent CD patients. The mean age at diagnosis and first GFD was lower in latent than in silent patients (14.4±5 vs 40.1±47 months, p<0.05). Latent patients did not differ significantly from the seven control patients on a long-term GFD, except for a higher frequency of CD-specific serum antibodies. However, two latent patients relapsed clinically and histologically during subsequent follow-up.
Conclusions: Long-term latency developed in about 20% of CD patients who remained symptom free after gluten reintroduction. This latency can be transient and thus a regular follow-up is mandatory. In silent patients, the increased risk of osteoporosis substantiates the need for a GFD.
- AGA, anti-gliadin antibody, AST, aspartate transaminase
- BMD, bone mineral density
- BMI, body mass index
- CD, coeliac disease
- CGFD, complete gluten-free diet
- EMA anti-endomysium antibody
- GFD, gluten-free diet
- HLA, human leucocyte antigen
- IEL, intraepithelial lymphocyte
- TCR, T cell receptor
- TGA, anti-tissue transglutaminase antibody
Statistics from Altmetric.com
- AGA, anti-gliadin antibody, AST, aspartate transaminase
- BMD, bone mineral density
- BMI, body mass index
- CD, coeliac disease
- CGFD, complete gluten-free diet
- EMA anti-endomysium antibody
- GFD, gluten-free diet
- HLA, human leucocyte antigen
- IEL, intraepithelial lymphocyte
- TCR, T cell receptor
- TGA, anti-tissue transglutaminase antibody
Coeliac disease (CD) is a chronic inflammatory enteropathy induced by dietary exposure to gluten, developing in genetically susceptible individuals and characterised by the presence of villous atrophy associated with various degrees of malabsorption. Typical clinical manifestations of CD include chronic diarrhoea, weight loss and anaemia, while its atypical forms, now more frequently observed especially in adolescents and adults, are manifested by irritable bowel-like or dyspepsia-like symptoms, or extradigestive symptoms (bone pains and fractures, infertility, buccal aphtosis, polyneuropathia). According to ESPGAN criteria,1 CD is defined as a permanent state of intolerance to gluten which requires a life-long gluten-free diet (GFD). This diet, in the vast majority of cases, leads to disappearance of clinical symptoms, recovery of normal duodenal histology, disappearance of serological stigmata of CD and prevention of CD complications.2,3 In contrast, lack of adherence to a strict GFD is considered the main reason for poorly controlled disease with an increased risk of malabsorption syndrome, osteoporosis4 and intestinal lymphoma.3,5 A GFD, however, although safe and efficient, is very restrictive, resulting in social burden and poor compliance. Therefore, the question still remains of whether the maintenance of a life-long GFD is necessary in all coeliac children or whether in some of them a gluten-containing diet can be safely reintroduced. Indeed, some data indicate that in some patients diagnosed in childhood who remained on a gluten-containing diet after gluten challenge, no clinical or histological relapse occurred.6–9 Most of these studies suffered, however, either from a small number of patients included, or from a relatively short duration of follow-up after gluten reintroduction. Moreover, in most of them, evaluation was mainly limited to the assessment of CD serology and histology of duodenal biopsies, and no attempt was made to identify predictive factors of development of tolerance to gluten.
The aim of this long-term retrospective follow-up study was to analyse clinical, biological and histological features of adult patients with CD diagnosed in childhood who, after gluten challenge, showed a good clinical tolerance and remained on a normal diet until adulthood. Having observed that some of the patients became latent, that is, presented a normal/subnormal duodenal histology on a gluten-containing diet at adulthood, we further tried to identify factors associated with this latency. In addition, we compared clinical and biological parameters between these latent patients and seven control patients who had been continuously kept on a GFD since diagnosis.
MATERIALS AND METHODS
Patients
The study was designed as a retrospective follow-up of adult patients with CD diagnosed in childhood, who abandoned a GFD. According to the accepted rules of the management of CD in children, after a period of from one to several years of a GFD introduced immediately after diagnosis, gluten challenge was systematically performed in all asymptomatic children. The particularity of our cohort was that in the case of a good clinical tolerance to the challenge, patients were allowed to consume gluten, even in the presence of histological relapse. In consequence, only the children with clinical relapse after the first gluten challenge (∼50% of the total population) returned to a GFD, while the remaining children were allowed a normal diet. Our study was focused on this specific group of patients. All of them but two were diagnosed and followed-up until adulthood in the Department of Pediatric Gastroenterology in the Necker Hospital and thereafter at the Georges Pompidou European Hospital in Paris, where they entered a local register of adult CD patients and were recruited for the study based on two criteria: CD diagnosed in childhood and adherence to a normal diet. The diagnosis of CD was based on the presence of duodenal villous atrophy, and/or positivity of specific CD serum antibodies, and clinical symptoms of gluten intolerance with clear improvement after introduction of a GFD.1 When the initial histology was not available, only patients with histologically proven villous atrophy later during follow-up were included. All patients had been diagnosed before the age of 8, except four diagnosed at the ages of 12, 13, 15 and 16, respectively, but with overt CD symptoms several years before diagnosis. Evaluation at adulthood was performed between 1997 and 2002 in patients aged 18–65 years who had been on a normal diet for at least 2 years. The threshold of 2 years was chosen following the accepted, although not proven, “two-year rule” for relapse after gluten challenge, according to which mucosal relapse usually occurs within 2 years after initiating the challenge.10
Collection of data
Data recorded for each patient included age, sex, medical history, associated diseases, clinical symptoms, gluten intake and history of GFD, in particular the age of the first introduction of a GFD, the total duration of a GFD and duration of the normal diet before evaluation. Current gluten consumption was calculated by a dietician experienced in CD, based on quantification of gluten ingestion per day assessed prospectively for a 7 day period. Physical examination with body mass index (BMI) assessment was performed. Nutritional status was defined as normal for BMI ⩾18.5 and <25, while the first, second and third degrees of malnutrition were defined as BMI ⩾17 and <18.5, ⩾16 and <17, and ⩾13 and <16, respectively. Patients were considered overweight if BMI was comprised between 25 and 30, and obese if BMI was superior to 30.1 Blood tests included measurements of the levels of haemoglobin, ferritin, vitamin B12, folic acid, calcium, albumin and transaminases. Bone mineral density (BMD) was measured using dual energy x-ray absorbitometry (DXA) at lumbar spine, left femoral bone and left femoral neck. BMD results were reported as mean mineral density at the chosen site. The presence or absence of osteopenia/osteoporosis was defined on the basis of the Z-score, which represents the number of standard deviations from the corresponding mean normal BMD value for gender and age. The following World Health Organization (WHO) diagnostic criteria were used: osteopenia, BMD >1 but <2.5 SD; and osteoporosis, BMD ⩾2.5 SD.11 Serological tests included detection of CD-specific IgA antibodies—that is, anti-gliadin (AGA), anti-endomysial (EMA), anti-tissue transglutaminase (TGA), and autoantibodies (anti-nuclear, anti-smooth muscle, anti-LKM1, anti-LC1, anti-thyroglobulin and anti-thyroperoxidase). Human leucocyte antigen (HLA)-DRB1 and DQB1 genotyping was performed by means of hybridisation with sequence-specific oligonucleotides following amplification by PCR, using the InnoLipa HLA genotyping test (Abott, France).12 The activity of CD was assessed by histology and immunohistochemistry in duodenal biopsies obtained during upper endoscopy. At least 4–6 duodenal biopsies were fixed in 10% formalin, embedded in paraffin and stained with H&E for standard examination. Villous atrophy was assessed according to Oberhuber et al’s13 modification of the Marsh classification,14 and graded as absent, partial or severe (subtotal/total) villous atrophy. Immunohistochemistry was performed on frozen duodenal biopsies using monoclonal antibodies directed against CD3 (UCHT1, dilution 1/1200), CD8 (DK25, dilution 1/400) (Dako, A/S, Glostrup, DK), β F1 (8A3, dilution 1/150), T cell receptor (TCR) δ1 (5Α6Ε9, dilution 1/100) (T Cell Sciences, Cambridge, MA, USA), and a three-stage indirect immunoperoxidase technique.15 The percentage of intraepithelial lymphocytes (IELs; number of IELs per 100 epithelial cells) labelled with various antibodies was established on well-orientated serial sections by counting at least 500 enterocytes in the surface epithelium.
Statistical analysis
Statistical analysis was performed using the SAS package (SAS Institute Inc., Cary, NC, USA). The results are presented as median or mean±SD for quantitative variables and as percentages for non-quantitative variables. Comparisons between the groups were performed using analysis of variance and non-parametric tests (Wilcoxon test) for quantitative variables, and Fischer exact test for non-quantitative variables. The differences were considered significant for p<0.05.
RESULTS
Description of the complete cohort followed-up since childhood
Seventy adult patients with CD diagnosed in childhood, who underwent clinical and biological evaluation at adulthood between 1997 and 2002, were identified in the cohort of adult CD patients followed in the George Pompidou European Hospital in Paris. From those, nine patients were on a GFD at the time of evaluation: seven had been on a strict GFD since the diagnosis and served as a control group; two other patients on a GFD for 2 years before evaluation were excluded from the study. Thus, 61 CD patients on a normal diet (38 women, 23 men, median age at evaluation 26 years, range 17–53 years) at the time of evaluation were included (fig 1). From this cohort, 17 patients had temporarily resumed a GFD during adolescence to prevent growth retardation, and had subsequently returned to a normal diet. Data concerning the history of GFD, clinical, biological and histological features of these 61 patients are summarised in tables 1, 2, 3 and 4.
History of gluten-free diet and clinical features of coeliac patients diagnosed in childhood, maintained on a normal diet until adulthood
Selected laboratory tests and bone mineral density in coeliac patients on a normal diet (mean (SD (% of abnormal)))
Coeliac disease-specific antibodies and autoantibodies in coeliac patients diagnosed in childhood and maintained on a normal diet until adulthood (no. positive/no. tested (% of positive)
Histology of duodenal mucosa in coeliac patients diagnosed in childhood and maintained on a normal diet until adulthood

The study cohort. GFD, gluten-free diet; ND, normal diet.
As indicated (table 1), almost half of the patients presented minor clinical symptoms, mainly episodic abdominal pain and bloating. These symptoms, however, did not interfere with the daily life of the patients and were not intense enough to prompt the patients to return to a GFD. About half of the patients presented levels of haemoglobin and serum ferritin inferior to normal, but in most cases the deficit was very small (table 2). Importantly, 60% of patients presented osteopenia or osteoporosis on at least one site, indicating that bone demineralisation is frequent in clinically asymptomatic or pauci-symptomatic CD (table 2). The majority of the patients (>80%) had at least one CD-specific antibody (table 3). Noticeably, results of duodenal histology allowed two groups of patients inside the cohort to be distinguished: the first group, with different degrees of villous atrophy, and a second group, with no detectable atrophy (table 4). These two groups, respectively classified as silent and latent CD, were therefore subsequently compared.
Comparison between patients without atrophy (latent CD group, n = 13) and with atrophy (silent CD group, n = 48) (tables 1–5)
DRB1 and DQB1 allelic distribution in latent and silent coeliac disease patients
History of GFD
Latent CD patients were younger at diagnosis and initiation of GFD than silent CD patients (p<0.05). No significant difference was detected between these two groups with regard to the duration of the first GFD, total duration of GFD and current gluten consumption (table 1).
Clinical symptoms
Twenty-four out of 48 silent CD patients and 8 out of 13 latent CD patients presented minor clinical symptoms, mainly abdominal pain and bloating, without significant differences between the two groups (table 1).
Nutritional status
The mean BMI did not differ significantly between the groups and was in the normal range both in latent and in silent CD patients (table 1). Among latent CD patients, one patient was overweight, while the remaining 12 patients had a normal nutritional status. In the silent CD group, the nutritional status was more variable: out of 48 patients, 7 presented the first degree of malnutrition, one with the third degree of malnutrition, five were overweight and one was obese.
Biological signs of malabsorption
No significant difference was found in the biological markers of malabsorption (haemoglobin, plasma ion, ferritin, albumin, and serum folic acid, vitamin B12 and calcium levels) between the latent and silent CD patients (table 2).
Bone mineral density
Decreased BMD was observed more frequently in silent than in latent CD patients. Eight out of nine studied patients from the latent CD group had a normal BMD in all three sites, while one patient presented a moderately decreased density in one site (lumbar spine, Z-score: 1.2). In the silent CD group, 10 of 33 studied patients had a normal BMD in all three sites, whereas 23 patients (70%) had a decreased BMD in at least one site. The difference between latent and silent CD patients was statistically significant (p<0.001). Similarly, mean BMD was lower in the silent than in the latent CD group in lumbar spine (p<0.06), total femoral bone (p<0.04) and femoral neck (p<0.03) (table 2). Furthermore, silent patients with subtotal atrophy tended to have a lower BMD in total femoral bone and femoral neck than silent patients with partial atrophy, although the differences were not statistically significant (p = 0.09) (fig 2).

Bone mineral density (BMD) in coeliac patients with normal mucosa (NM), partial villous atrophy (PVA) or subtotal or total villous atrophy (S-TVA): BMD is decreased in patients with villous atrophy. #p<0.05, *p<0.03 as compared with the NM group, §p<0.03 as compared with the NM group and p = 0.09 as compared with the PVA group.
Liver enzymes
One patient from the latent CD group and 9 patients out of 39 from the silent CD group had mild elevation of transaminases, the difference being statistically non-significant. Although the mean levels of aspartate aminotransferase (AST) (25±2 IU) were higher in silent than in latent CD patients (17±3 IU, p<0.03), mean values in both groups were within the normal range (table 2).
Autoimmunity
In the latent CD group, serum autoantibodies were found in one patient, while in the silent CD group, they were present in 7 out of 42 patients (table 3). The difference between the two groups was not statistically significant.
CD-specific serum antibodies
As expected, CD-specific antibodies were more frequently positive in silent than in latent CD patients (table 3). Interestingly, in the group of silent patients, AGA were more frequently found in patients with subtotal to total villous atrophy (78%) than in those with partial atrophy (37%, p<0.008), while no significant difference was found in the positivity rate of EMA (83 vs 85%) or TGA (90 vs 60%) between these subgroups.
Duodenal histology and immunohistochemistry
By definition, all 13 latent CD patients had a normal mucosal architecture. All 48 silent CD patients presented various degrees of villous atrophy: 25 had subtotal to total atrophy, while 23 patients had partial atrophy. IEL counts were increased in all silent patients and in 11 of 13 latent patients. Silent CD patients had higher total counts of CD8+/TCRαβ+ IELs than latent CD patients. TCRγδ+ IEL counts were increased in both groups compared with non-coeliac controls, but there was no difference between the two groups. Accordingly, the proportion of TCRγδ+ lymphocytes among CD3+ IELs was higher in latent than in silent CD patients (p<0.01) (table 4).
HLA typing
Ninety-two percent of patients were DQ2 positive (DRB1*03-DQB1*0201 or DRB1*07-DQB1*0201), all the remaining patients being DQ8 positive (DRB1*04-DQB1*0302) (table 5). The proportion of patients with two copies of HLA DQ2 (DRB1*03-DRB1*03 or DRB1*03-DRB1*07) was 17% in the latent CD group and 42% in the silent CD group, but the difference was not statistically significant.
Comparison between latent CD patients and patients who have always adhered to a GFD
An important question is whether the patients who became latent despite gluten consumption differ from those who have continuously been following a strict GFD since diagnosis. To address this question, we compared clinical and biological data between the group of latent CD patients (n = 13) and the group of seven patients on a GFD since diagnosis (continuous gluten-free diet (CGFD) group). Six out of these 7 patients had a normal duodenal architecture while one had partial villous atrophy. No significant difference was found in terms of clinical symptoms (5 of 13 patients from the latent CD group and 2 of 7 patients from the CGFD group presented very mild clinical symptoms), nutritional status (BMI = 21.4±2.6 and 21.3±2.8, in the latent and CGFD patients, respectively), blood tests (haemoglobin, 13.5±1.6 and 13.5±1.8 g/100 ml; ferritin, 57±61 and 59±107 µg/l; vitamin B12, 405±215 and 378±235 ng/l; albumin, 42.7±4 and 45.3±8 g/l; calcaemia, 2.28±0.09 and 2.28±0.17 mmol/l, folic acid: 7.4±2.9 and 11±6 µg/l), BMD (BMD of lumbar column = 0.99±0.08 and 0.90±0.13, BMD of total femoral bone = 0.98±0.13 and 0.86±0.02; BMD of femoral neck = 0.90±0.01 and 0.87±0.08, for the latent and CGFD groups, respectively), or presence of serum autoantibodies (1/6 CGFD patients and 1/13 latent CD patients were positive for at least one serum autoantibody). The CD-specific antibodies were, however, more frequently positive in latent CD patients than in the CGFD group. Five out of 13 latent patients were positive for at least one antibody: two were positive for both EMA and TGA, two for EMA only, and one for TGA only. In contrast, only one out of the 7 patients on a GFD had both EMA and TGA. The same patient had partial villous atrophy, suggesting non-strict adherence to the diet. Immunohistochemical data were not available in CD patients on a GFD.
Follow-up of latency
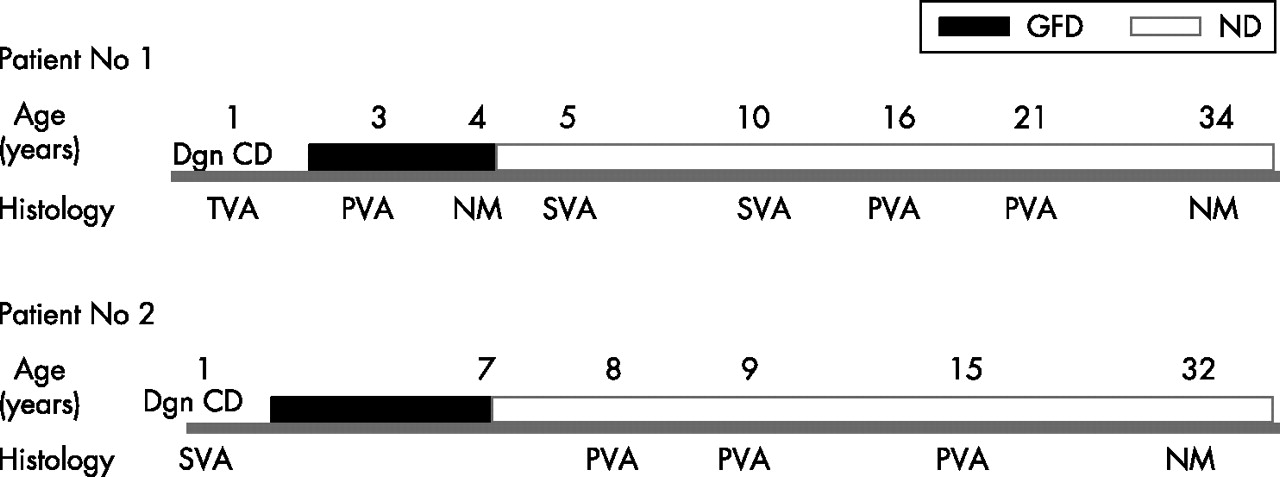
In 13 latent patients, the time period between the last biopsy showing villous atrophy and the first evidence of histological remission varied from 3 to 21 years (mean, 11±5 years; median, 13 years). In most patients, the lack of prospective regular histological follow-up did not allow determination of the exact time of histological recovery. In two patients, however, several consecutive biopsies were available. In the first female patient (fig 3A), villous atrophy was confirmed 1, 2 and 8 years after gluten reintroduction. A normal mucosa was observed for the first time 25 years after gluten challenge, indicating that recovery had occurred between 8 and 25 years after gluten reintroduction. In the second female patient (fig 3B), total villous atrophy was observed 1 and 6 years after gluten challenge, then partial villous atrophy was observed in two consecutive examinations, 12 and 17 years after gluten challenge. Finally, a normal duodenal mucosa was observed after 30 years, indicating that recovery from atrophy occurred somewhere between 17 and 30 years on a normal diet.
{kind=link}
{kind=link}
{kind=link}
Follow-up in two patients with CD diagnosed in childhood who developed histological tolerance to gluten on a normal diet. GDF, gluten-free diet; ND, normal diet; Dgn CD. diagnosis of coeliac disease; TVA, total villous atrophy; SVA, subtotal villous atrophy; PVA, partial villous atrophy; NM, normal mucosa. In both patients, a gradual histological recovery could be observed on a gluten-containing diet.
For four patients, data from the subsequent (post-study) follow-up are available: while two patients still presented a normal mucosa, 5 and 4 years, respectively, after diagnosis of latency, two of them had relapsed clinically and histologically 3 years after the last observation of normal histology. The first one admitted a change in dietary habits with a marked increase in gluten consumption, while the second one reported increased professional stress due to change of employment.
DISCUSSION
This study provides a detailed analysis of the long-term evolution at adulthood of CD patients diagnosed in childhood who remained symptom free after resuming a normal diet. Our results indicate that the majority of patients, despite their good clinical tolerance of a normal diet, presented different degrees of villous atrophy and increased risk of osteopenia/osteoporosis. Up to 20% of the patients, however, progressively reversed from active CD to a stage resembling latent CD characterised by histological recovery, absence of clinical or biological evidence of malabsorption but persistence of serological markers of CD and/or increased numbers of IELs. The relapse observed in two patients underscores the similarities to latent CD and stresses the need for a careful follow-up.
According to the original EPSGAN criteria, gluten challenge was performed in all coeliac children after a 1–4 year period of GFD to confirm the diagnosis of CD definitely.10 After challenge, children were classically advised to return to a GFD. An alternative, although controversial, strategy was to allow a normal diet in children who remained symptom free despite histological relapse. In our cohort, these asymptomatic children represented about 50% of the initial population, a proportion also observed in other cohorts.16 Due to the fact that they were consuming gluten, they were subjected to a thorough follow-up, and the majority of them were available for analysis at adulthood. This gave us an exceptional opportunity to study the outcome of the coeliac children kept on a normal diet until adulthood. The issue is important given the increasing number of asymptomatic patients discovered by serological testing. It remains unclear whether these patients may be allowed to consume gluten, without increasing their risk of CD complications, or whether they should be advised a GFD, the benefit of which may be difficult to perceive and accept.
Histological examination and serological tests allowed us to divide the 61 patients on a long-term normal diet into two groups: a large group of 48 patients with partial to subtotal villous atrophy who were almost always positive for EMA and/or TGA, and a second smaller group of 13 patients with normal or subnormal villous architecture, 60% of whom did not have increased levels of EMA and TGA. There was no significant difference between both groups with respect to clinical symptoms, nutritional status or biological parameters of malabsorption. A poor correlation between clinical symptoms and presence of villous atrophy in CD patients on a normal diet has already been reported.17 Yet, typically patients with active CD present biological signs of malabsorption, particularly anaemia and iron deficiency,18,19 that were not observed in our cohort. Elevation of liver enzymes is frequent in active CD. 20–22 Accordingly, significantly higher levels of serum AST in patients with villous atrophy as compared with those without atrophy were found. Yet, the increase observed in nine patients with villous atrophy remained very moderate. The most important difference was the high rate (60%) of osteopenia/osteoporosis in patients with villous atrophy, with a tendency to lower BMD indexes in patients with subtotal than partial villous atrophy. This is in agreement with a large amount of data from the literature showing that BMD is reduced in children and adults with CD,23–25 with an increased risk of osteoporotic fracture26 and of severe osteopenia27 that can be corrected by a well-conducted GFD.24,28–31 The exact risk of functional complications remains controversial32 and none was observed in our series of silent patients. Furthermore, there was no significant difference in BMD between the patients who did or did not adhere to a GFD during adolescence (data not shown). A recent report suggests that a few years on a GFS during childhood may reduce the severity of CD at adulthood.33 The mildness of clinical and biological symptoms in the present series of patients confirms this hypothesis. Nevertheless, our results indicate that in most patients, clinical tolerance does not reflect a real tolerance to gluten and that a GFD is advisable in asymptomatic adult patients with villous atrophy to prevent complications.
Histological remission was observed in a group of 13 patients on a long-term normal diet. Although our cohort may not be representative of all coeliac patients, and certainly larger European studies would be necessary to evaluate the frequency of latent CD, the proportion of latent CD patients found in our study is similar to that previously reported. Thus, in a large series of 91 children with one or more interruptions of GFD, Shmerling et al observed that 6 patients retained a normal mucosa after 2–6 years off the diet.8 Maki et al also reported that 4 out of 29 CD patients had not relapsed 2 years after a late gluten challenge performed in the post-pubertal period.9 More recently, Bartella et al observed that 7 out 38 patients with dermatitis herpetiformis did not relapse upon gluten reintroduction after several years on a GFD.34 Schmitz et al were the first in 1984 to describe spontaneous histological recovery during normal diet in three female coeliac patients with CD diagnosed in childhood.35 The same group subsequently showed in 1993 that among 34 asymptomatic CD children returned to a normal diet, four had recovered a fully normal and six a partially normal villous architecture 5–13 years later.7 The current study strengthens these observations and confirms that spontaneous histological remission can occur in up to 20% of asymptomatic patients with CD diagnosed in childhood who resumed a normal diet containing approximately 10 g of gluten per day. Since this group represented approximately 50% of the initial population, remission might occur in up to 10% of cases of CD diagnosed in childhood. Importantly, thorough assessment indicated that the latter patients who have now reached adulthood do not differ significantly, in terms of clinical symptoms, biological tests of malabsorption and BMD, from a small group of control CD patients on a GFD since diagnosis, and thus have no sequelae of CD. These results raise several questions. First, does histological remission indicate full and definitive recovery of immunological tolerance to gluten? Up to 40% of patients still had one or two serological positive markers. The numbers of IELs were decreased as compared with silent patients. More importantly, the numbers of CD8 TCRαβ IELs, known to be exclusively increased in active CD15 and to participate in epithelial damage in active CD, were markedly decreased.36,37 Yet, the number of TCRγδ IELs remained elevated. One experimental study has suggested the protective role of this lymphocyte subset against intestinal epithelial damage induced by TCRαβ lymphocytes.38 Other studies have provided contradictory results on their possible role in oral tolerance.39,40 In CD, the mechanisms that drive the expansion of TCRγδ IELs, as well as the function(s) of this lymphocyte subset at the different phases of CD remain elusive. The combination of positive serological markers and elevated counts of TCRγδ IELs is, however, strongly reminiscent of latent CD. Thus, in individuals at risk of CD but with normal histology, these two markers are highly predictive of the future onset of active CD.41–43 Noticeably, two patients relapsed clinically and histologically during the follow-up subsequent to this study, confirming that histological remission does not indicate permanent tolerance but should rather be viewed as a return to latent CD that does not require a GFD but imposes the need for a careful surveillance. The natural history of CD may thus include the alternations of spontaneous remissions and relapses, driven by some external, dietary, stress or perhaps infectious factors. Definitive recovery, however, cannot be excluded in some of our patients. Only a longer (life-long) follow-up of a large group of latent patients will allow definition of whether CD can be “transient”.
A second important question concerns the factors that promote return to latent disease. The only significant factor in our study was an early CD diagnosis and consequently the early exclusion of gluten from the diet. Early CD diagnosis was also noted as one factor associated with the lack of relapse in patients with dermatitis herpetiformis that resumed a normal diet after prolonged gluten avoidance.34 Studies showing that delayed introduction of gluten into infant diets reduces the incidence of childhood CD are in line with our results.44 Yet, how early GFD in our patients may promote progressive silencing of the disease despite continuous antigen exposure remains intriguing. Patients who recover may have a higher threshold of immune reactivity to gluten that allows the immune balance to reverse toward tolerance. It has recently been suggested that the HLA-DQ2 gene dose is directly related to the magnitude and breadth of gluten-specific T cell responses.45 Accordingly HLA-DQ2 homozygosity has been associated with severe CD complicated by low or high grade lymphoma,46 while homozygosity for the DQB*0201 allele has been associated with more severe grades of villous atrophy and slower recovery after GFD.47 In our cohort, the prevalence of DQ2 homozygosity was indeed lower in patients with latent CD (17%) than in patients with silent villous atrophy. Yet, probably due to the small numbers of individuals, the difference did not reach significance. The contribution of other unknown genetic factors to shaping the immune response to gluten is also possible.
In conclusion, this study indicates that up to 10% of CD patients diagnosed in childhood can spontaneously recover a normal villous architecture after a long period of normal diet without retaining any clinical or biological sequelae of CD. The persistence of immunological stigmata of CD and the risk of relapse indicate, however, that this remission state must not be considered as a definitive recovery but as a return to latency that requires a regular follow-up. Most of the patients with CD diagnosed in childhood who resumed a normal diet, however, have an active CD at adulthood, even in the absence of symptoms. These patients should be screened for the presence of villous atrophy and osteopenia, and should be advised to return to a GFD in the case of persisting villous atrophy.
REFERENCES
Footnotes
-
Published Online First 15 February 2007
-
Competing interests: None declared.