Article Text

Abstract
Background: Severe duodeno-gastro-oesophageal reflux (DGOR) is a risk factor for oesophagitis and Barrett’s oesophagus. Patients with non-erosive reflux disease (NERD) have a slight increase in DGOR. Patients with gastro-oesophageal reflux disease (GORD), who are taking proton pump inhibitors (PPIs), still have reflux but of weakly acidic pH and persistence of bile. In these two groups of patients, heartburn might be due to increased oesophageal mucosal permeability and dilated intercellular spaces (DIS). We aimed to assess whether experimental short exposure of the oesophageal mucosa to bile acids, in low concentrations (at acidic, weakly acidic and neutral conditions) can increase mucosal permeability and provoke DIS.
Methods: Rabbit oesophageal mucosa was studied in diffusion and Ussing chambers. We assessed the effects of different solutions containing bile acids, applied to the mucosal side, on transepithelial electrical resistance (RT) and permeability to fluorescein. The diameter of intercellular spaces was assessed by using transmission electron microscopy.
Results: Incubation of oesophageal mucosa with acidic solutions (pH 2.0) containing a range of bile acids (0.5–5 mmol/l) markedly decreased RT and increased mucosal permeability. Weakly acidic solutions (pH 5.0), and to some extent neutral solutions (pH 7.4), containing some bile acids also decreased RT and increased permeability, although the effects were much less marked and in some combinations no effect was seen. Exposure to bile acids provoked DIS in acid and weakly acidic conditions but not in neutral (pH 7.4) solutions.
Conclusions: Experimental short exposure of the oesophageal mucosa to solutions with a bile acid concentration and acidity similar to that observed in the gastric contents of patients with NERD or ERD, and who are taking PPIs, may impair oesophageal mucosal integrity and even induce dilated intercellular spaces. Such a situation could, theoretically, underlie the occurrence and/or persistence of symptoms in these patients.
Statistics from Altmetric.com
Prolonged exposure of the oesophageal mucosa to bile acids, as occurs in duodeno-gastro-oesophageal reflux (DGOR), is important in the pathogenesis of erosive reflux disease (ERD), particularly of severe oesophagitis and Barrett’s oesophagus.1
Bilitec measurements showed that patients with non-erosive reflux disease (NERD) have less oesophageal exposure to bile as compared to patients with ERD, although bile exposure is significantly higher than that observed in asymptomatic healthy subjects.2 3
Duodenal bile may reflux into the oesophagus either mixed with gastric juice in a very acidic milieu or mixed with buffered gastric contents in a weakly acidic milieu. For example, in patients with gastro-oesophageal reflux disease (GORD), 60% of nocturnal bile reflux occurs at an oesophageal pH between 4 and 7.4 Patients with GORD who are taking proton pump inhibitors (PPIs) still have gastro-oesophageal reflux. However, most reflux is weakly acidic (pH 4–7) and may or may not contain bile.5 In a subgroup of these patients, persistent exposure to oesophageal bile in a weakly acidic milieu was probably responsible for symptoms that improved with pharmacological anti-reflux treatment.6
Current concepts in the pathophysiology of NERD involve peripheral factors in the oesophageal lumen (acid and non-acid reflux, gas and proximal oesophageal distension),7 8 mucosal changes9 and neural visceral hypersensitivity.10 11
The most reported histological change observed in the mucosa of patients with NERD is the presence of dilated intercellular spaces (DIS).12 13 Barlow and Orlando14 proposed the following model to explain the pathophysiology of symptoms in NERD: DIS enable the diffusion of refluxed gastric acid into the intercellular space. Then acid can reach and activate chemosensitive nociceptors whose signals are transmitted via the spinal cord to the brain for perception of symptoms.
DIS can also be involved in the pathogenesis of persistent symptoms in patients taking PPIs. Studies have shown that treatment with PPIs can reverse DIS in up to 70% of patients.15 16 Interestingly, patients with persistent symptoms while taking PPIs may still have DIS17 despite normalisation of exposure to oesophageal acid.
The occurrence of DIS is classically attributed to mucosal exposure to acid. This concept is based on experimental evidence18 and the response of humans to PPIs.15 19 However, other stimuli could affect intercellular adhesion mechanisms. This is the case with the exposure of the oesophageal mucosa to bile acids,20 alcohol21 and aspirin.22 A recent study in rats from our laboratory has shown that acute stress, by itself, can increase the permeability of the oesophageal mucosa and provoke DIS.23 It is known that exposure of the oesophageal mucosa to bile acids (in high concentration) can provoke significant changes,24 25 including erosions, cell destruction at the basal layer, and large intracellular vacuoles.26 The presence of DIS has not been formally evaluated. Previous studies have shown that bile acids decrease the mucosal electrical resistance and increase the net acid flux and permeability to hydrophilic molecules.20 27 28 Most of these studies, however, tested the effect of bile acids at higher concentrations (>5 mmol/l) and lower pH (1.5) than those commonly observed in the oesophageal lumen of patients with GORD. Only Lang et al29 investigated the effect of physiological concentrations of conjugated bile acids (1–3 mmol/l) at a pH range observed in humans. Studies analysing aspirated material from the oesophagus of patients with GORD show a higher concentration of both conjugated and unconjugated bile acids as compared to aspirated material from healthy volunteers.1 30
We hypothesised that even a short exposure of oesophageal mucosa to bile acids, in physiological concentrations (similar to that found in postprandial gastric contents31 32) may increase oesophageal mucosal permeability and induce DIS. Such a situation can occur during short periods of fasting acid DGOR and/or postprandial weakly acidic DGOR in patients with NERD or during weakly acidic reflux in patients with GORD who are taking PPIs.
The aim of our study was to test, in vitro, the effect of bile acids on the permeability of rabbit oesophageal mucosa and epithelial intercellular spaces, in acidic, weakly acidic and neutral conditions.
MATERIALS AND METHODS
Animals
Twenty-five adult New Zealand male rabbits were killed by a blow on the neck followed immediately by exsanguination. The complete oesophagus was excised, opened and stripped of its muscle layers in a paraffin tray containing carbogenated Krebs–Henseleit bicarbonate buffer (KHBB, pH 7.4 containing (in mmol/l): 118, NaCl; 4.7, KCl; 1.2, CaCl2; 1.2, MgSO4; 1.2, NaH2PO4; 25, NaHCO3; and 11, glucose). A single mucosal sheet was obtained, consisting of stratified squamous epithelium and underlying connective tissue.
Transepithelial electrical resistance
Oesophageal mucosal sections were cut and fixed in Ussing chambers with an opening of 0.5 cm2. The tissue was incubated at 37°C in carbogenated KHBB and the transmucosal potential difference was continuously monitored with Ag/AgCl electrodes. The basal transepithelial electrical resistance (RT) was calculated according to Ohm’s law from the voltage deflections induced by bipolar constant current pulses of 50 μA (every 60 s) with a duration of 200 ms applied through platinum wires (Mussler Scientific Instruments, Aachen, Germany). A correction for fluid resistance was made. After an equilibration period, the luminal side was exposed for 30 min to either a control solution (KHBB containing pepsin at pH 2.0, 5.0 and 7.4) or test solutions (identical to control) plus one of the following bile acids: glycocholic acid (GC), taurodeoxycholic acid (TDC) and deoxycholic acid (DC)). Bile acids were used in their sodium salt form (Sigma/RBI, Bornem, Belgium) at concentrations 0.5, 2 and 5 mmol/l. Control and test solutions contained pepsin 1 mg/ml (porcine pepsin A, 392 U/mg solid; Sigma/RBI). The RT was continuously recorded during the exposure time and expressed as Ω cm2. The effect of the different test solutions is expressed as the percentage change in RT relative to the control solution (KHBB pH 7.4) at 30 min.
Transepithelial permeability
Oesophageal mucosal sections of approximately 0.3 cm2 were cut and mounted in a diffusion chamber (Mussler Scientific Instruments) for measurements of permeability to fluorescein (375 Da) (Sigma/RBI). The diffusion chamber allowed exposure of the “luminal side” to different test solutions and regular sampling from the “serosal side” to detect the degree of mucosal permeability to fluorescein. Tissues were bathed in 37°C carbogenated KHBB (2 ml on each side) for 30 min. Then, the luminal side was exposed for 30 min to control and test solutions identical to those used in transepithelial electrical resistance measurements. After this period the solutions in the luminal side were replaced by a solution containing fluorescein 1 mg/ml. A 300 μl sample was taken from the serosal side of the diffusion chamber at 0, 30, 60, 90 and 120 min. The volume at both sides of the diffusion chambers was kept constant by adding normal KHBB. The permeability to fluorescein was measured using a fluorescence plate reader (Fluoroskan, Ascent; Thermo LabSystems, Zellik, Belgium). The fluorescence of the supernatant in the “serosal side” was measured using an excitation wavelength of 485 nm and an emission wavelength of 538 nm. The permeability to fluorescein was expressed as nmol/cm2.
Morphological studies
Following the permeability experiments in diffusion chambers, tissues were examined using both light microscopy and transmission electron microscopy (TEM) to assess the presence of erosions and diameter of intercellular spaces. Tissues were fixed in 4% (w/v) paraformaldehyde for light microscopy and in 2.5% (w/v) glutaraldehyde in phosphate buffer for TEM. Light microscopy was performed with the tissue embedded in paraffin. Transverse sections (5 μm) were stained using haematoxylin–eosin and von Gieson methods.
For TEM, tissues were post-fixed in 1% buffered osmium tetroxide at 4°C, and dehydrated through a graded alcohol series, then embedded in an epoxy resin. Ultrathin sections were post-stained with uranyl acetate–lead citrate. Specimens were examined and photographed using a Zeiss transmission electron microscope (Zeiss, Oberkochen, Germany). Three TEM photos/per animal were taken (magnification, ×4000) and analysed using custom-written image analysis software in IGOR Pro (WaveMetrics, Lake Oswego, Oregon, USA). Intercellular spaces were delineated between five and ten epithelial cells from the basal and lower prickle layers in each microphotograph.33 34 The intercellular space area was measured and related to the perimeter of the corresponding cells to obtain a relative measure of DIS.23 35 The morphological evaluations were performed by one of the investigators who was blinded to the type of mucosal exposure (test solution) and results of the permeability and resistance studies.
Statistics
All data are expressed as mean (with the SEM in parentheses). Single comparisons were performed by the paired or unpaired Student t test when appropriate. The effect of the different solutions on time–permeability curves was analysed using two-way repeated measures ANOVA. When the ANOVA test was significant, the Bonferroni test was used to determine the times with statistical significant difference. The correlation between changes in RT and permeability to fluorescein was tested using the Spearman and Pearson tests when appropriate. Significance was declared at p<0.05.
RESULTS
Transepithelial electrical resistance
Effect of acidic solutions (pH 2.0)
The basal oesophageal mucosa electrical resistance (RT) during exposure to control solution (KHBB pH 7.4) was 2089 (73) Ω cm2. Exposure of the mucosa to acidic solutions decreased the RT by 6.73 (1.96)% (p<0.01) (n = 16, N = 7; where n is the number of observations and N is the number of animals).
Adding bile acids to acidic solutions significantly reduced the mucosal electrical resistance. Relative to a basal RT during control solutions (KHBB pH 2.0), the addition of GC or TDC at 0.5 mmol/l reduced RT by 18.07 (4.07) and 17.25 (6.16)%, respectively. This effect was concentration dependent. With solutions of 2 mmol/l the reduction in RT was 47.45 (12.30) and 57.74 (11.67)%, and with solutions of 5 mmol/l the reduction in RT was 70.19 (8.89) and 78.63 (10.80)%, respectively (table 1).
Effect of weakly acidic solutions (pH 5.0)
Exposure of oesophageal mucosa to weakly acidic solutions increased the RT by 1.70 (0.50)% (p<0.01) relative to control solutions (KHBB pH 7.4).
Adding bile acids to weakly acidic solutions reduced the mucosal electrical resistance. Relative to a basal RT during control solutions (KHBB pH 5.0), the addition of bile acids at the lowest concentration (0.5 mmol/l) did not modify RT. However, a significant reduction in RT was observed with higher concentrations. Addition of TDC and DC at 2 mmol/l to weakly acidic solutions reduced RT by 6.0 (1.4) and 63.6 (6.4)%, respectively, whereas GC had no effect. Adding TDC, DC and GC at 5 mmol/l reduced RT by 69.0 (9.7), 92.6 (1.9) and 3.4 (0.6)%, respectively (table 2).
Effect of neutral solutions (pH 7.4)
Adding bile acids to neutral solutions reduced the electrical resistance of the mucosa. Relative to a basal RT during control solutions (KHBB pH 7.4), the addition of bile acids at the lowest concentration (0.5 mmol/l) did not modify RT. However, a significant reduction in RT was observed with higher concentrations. Addition of TDC and DC at 2 mmol/l to neutral solutions reduced RT by 12.04 (0.87) and 11.96 (1.35)%, respectively, whereas GC had no effect. Adding TDC, DC and GC at 5 mmol/l reduced RT by 52.21 (4.68), 94.27 (1.58) and 4.22 (0.55)%, respectively (table 3).
Transepithelial permeability
Effect of acid solutions (pH 2.0)
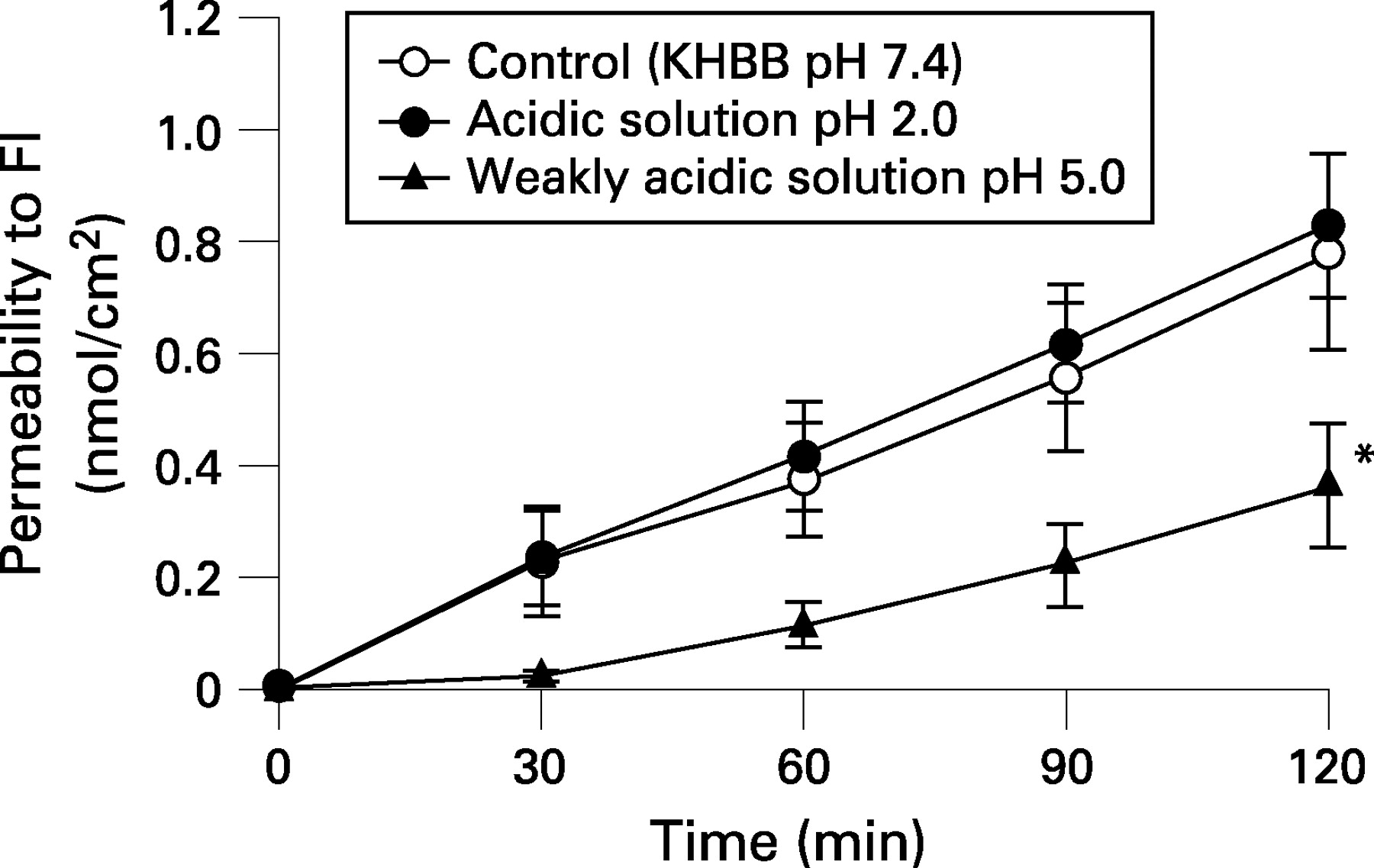
Acidic solutions did not modify mucosa permeability. After 120 min, the permeability to fluorescein was 0.78 (0.18) nmol/cm2 with acid and 0.84 (0.15) with control solutions (n = 14, N = 11, p = 0.49) (fig 1).

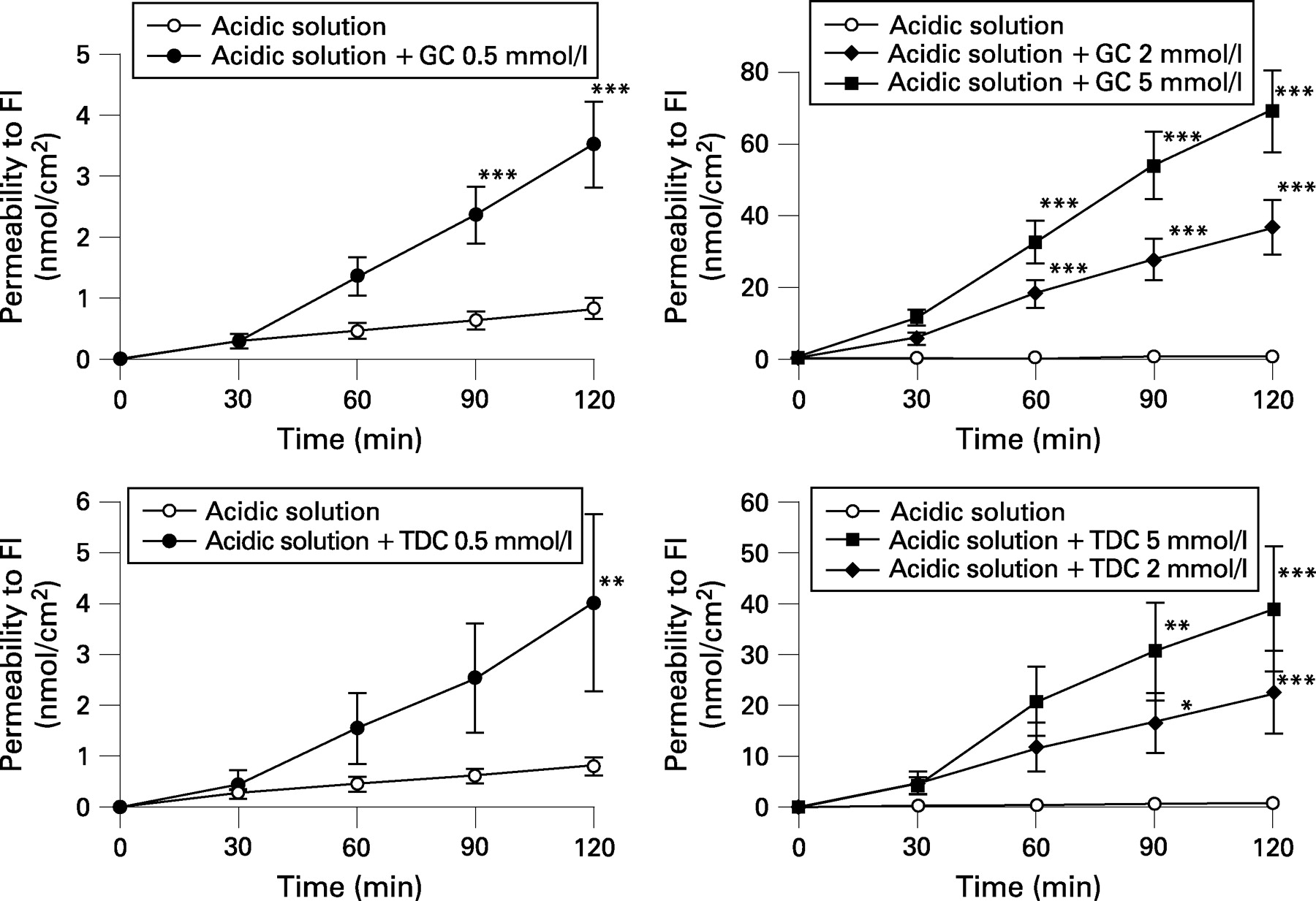
Addition of GC and TDC to acidic solutions caused a concentration dependent increase in the permeability of oesophageal mucosa to fluorescein (fig 2). Relative to a basal permeability during control acid solution (pH 2.0), the lowest bile acid concentration (0.5 mmol/l) of GC and TDC increased permeability 4 times and 5 times, respectively. At higher concentrations the change in permeability was very pronounced. With solutions of GC and TDC at 2 mmol/l, the permeability increased 44 and 25 times, respectively, and at a higher concentration (5 mmol/l) the increase in permeability was 83 and 47 times, respectively (table 4).

Effect of weakly acidic solutions (pH 5.0)
Weakly acidic solutions decreased oesophageal mucosal permeability to fluorescein. After 120 min, the permeability to fluorescein was 0.36 (0.11) nmol/cm2 with weakly acidic and 0.78 (0.18) nmol/cm2 with control solutions (n = 11, N = 10), (p<0.001) (fig 1).
Addition of bile acids to weakly acidic solutions also increased the permeability of oesophageal mucosa. This effect was significant but less marked than that observed with acid solutions. Relative to basal permeability during exposure to a control weakly acidic solution (pH 5.0) the lowest concentrations of TDC (0.5 mmol/l) increased permeability significantly (2 times), whereas GC and DC did not. At 2 mmol/l, TDC and DC significantly increased permeability (2.5 and 3.5 times, respectively), whereas GC had no effect. At 5 mmol/l TDC, DC and GC increased the permeability by 21, 8 and 2 times, respectively (fig 3 and table 5).

Effect of neutral solutions (pH 7.4)
Addition of bile acids to neutral solutions slightly increased oesophageal mucosal permeability. This effect was significant but less marked than that observed with weakly acidic solutions for most bile acid concentrations. Only DC 5 mmol/l provoked a similar change of permeability in weakly acidic and neutral conditions (table 6).
There was a significant inverse linear relationship between RT values and the permeability to fluorescein after exposure of the oesophageal mucosa to both acidic and weakly acidic solutions containing different concentrations of bile acids (r = 0.83 (p<0.05) for the acidic and r = 0.92 (p<0.001) for the weakly acidic conditions).
Morphological studies
Light microscopy showed no erosions or cell necrosis in mucosa exposed to acidic and weakly acidic solutions containing bile acids. Electron microscopy showed no increase in relative area of intercellular spaces after acid exposure compared to control (0.01 (0.01) μm and 0.03 (0.01) μm, respectively, p = 0.17, n = 3, N = 3; and after weakly acidic exposure, 0.03 (0.01) μm, n = 3, N = 3).
Acidic solutions with bile acids at 0.5 mmol/l did not provoke changes in intercellular spaces. However, at higher concentration (2 mmol/l) TDC provoked dilation of intercellular spaces of the basal layer (0.20 (0.05) μm, p<0.01, n = 3, N = 3) (fig 4) and GC widened intercellular spaces in the stratum corneum.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
In weakly acidic conditions, bile acids could also provoke DIS. At the concentrations of 2 and 5 mmol/l, DC enlarged the relative area of intercellular spaces to 0.10 (0.02) μm (p<0.05, n = 3, N = 3) and 0.08 (0.01) μm (p<0.01, N = 3), respectively. TDC provoked DIS to 0.16 (0.05) μm (p<0.05, n = 3, N = 3) at the highest concentration (5 mmol/l).
In neutral conditions (pH 7.4), bile acids did not provoke DIS. Intercellular spaces after exposure to DC and TDC at 5 mmol/l were 0.01 (0.01) μm (n = 3, N = 3) and 0.02 (0.01) μm (n = 3, N = 3), respectively (fig 4).
DISCUSSION
We hypothesised that short exposure of the oesophageal mucosa to solutions with acidity and bile acid concentration similar to that observed in postprandial gastric contents of patients with NERD or patients with ERD, receiving PPIs, may increase oesophageal mucosal permeability and induce dilated intercellular spaces (DIS). Such a situation could theoretically underlie the occurrence and/or persistence of symptoms in these patients.
The experimental work showed the following four effects. First, exposure of rabbit oesophageal mucosa to acid and weakly acidic solutions containing low concentrations of bile acids can provoke decreased mucosal electrical resistance and increased permeability with or without observable dilation of intercellular spaces. Second, the degree or type of disruption of epithelial integrity depends on the acidity, the concentration and type of bile acid in the solution. Third, the most striking effect on the three parameters studied (resistance, permeability and morphology) was observed after exposure to bile acids in acid pepsin solutions (pH 2.0). Bile acids in weakly acidic pepsin solutions (pH 5.0) had a much smaller effect than in acid solutions; however, this effect was consistent and statistically significantly higher than that observed with control solutions. Bile acids in neutral pepsin solutions (pH 7.4) had an even smaller effect than acid and weakly acidic solutions. They decreased electrical resistance, but they slightly increased permeability and did not provoke DIS. Finally, there are conditions with clear disruption of oesophageal functional integrity (decreased RT and/or increased permeability) without observable DIS.
Prolonged exposure of oesophageal mucosa to bile acids, due to DGOR, is important in the pathogenesis of ERD, particularly of severe oesophagitis and Barrett’s oesophagus.3 We wanted to assess the effect of short exposure and low bile acid concentrations on oesophageal mucosa, to simulate conditions similar to those observed in patients with NERD. The exposure time could be deduced from Bilitec studies. In patients with NERD the time of bilirubin exposure is approximately 3.0%. The bile acid concentration was deduced from oesophageal and gastric aspiration studies. In healthy volunteers, bile acids in oesophageal aspirates were almost undetectable and the concentration in patients with GORD increased without exceeding 1 mmol/l.1 30 36 37 Gastric bile acid concentration in healthy volunteers is between 0.3 and 2 mmol/l31 32 38 and in patients with erosive oesophagitis it can increase to 10 mmol/l.31
Based on this information, we used solutions with bile acid concentrations between 0.5 and 5 mmol/l. In contrast, most previous experimental studies on the effect of bile acids on oesophageal mucosa used higher concentrations (>5 mmol/l)20 27 39 and very acidic solutions (pH = 1.1), rarely observed in oesophageal pHmetries of patients with NERD. According with the pH of the refluxate, reflux is classified as “acid reflux” when refluxed gastric juice reduces the pH of the oesophagus to below 4, and “non-acidic reflux” when reflux episodes are above pH 4. “Non-acid reflux” is subdivided into “weakly acidic reflux” when the oesophageal pH is between 4 and 7, and “weakly alkaline reflux” when the nadir oesophageal pH is 7 or higher (Porto classification).
In patients with NERD, with normal or increased acid exposure, most reflux is acid and the exposure time to DGOR is around 3%.40 We also wanted to simulate conditions similar to those present in patients receiving PPIs. In this case, the oesophageal mucosa is mostly exposed to weakly acidic reflux with a pH between 4 and 6.5.41
The bile acids added to our experimental solutions were selected based on studies using oesophageal aspirates that showed increased GC, TC, cholic and TDC in patients with GORD and not taking PPIs. In patients receiving PPIs the oesophageal mucosa is exposed to weakly acidic reflux,41 and gastric bacterial overgrowth may result in increased concentration of unconjugated bile acids like DC.42 In our study we exposed the oesophageal mucosa to acid, weakly acidic and neutral solutions containing the conjugated bile acid GC, the unconjugated bile acid DC and the secondary bile acid TDC.
The functional integrity of the oesophageal epithelial barrier can be assessed by measuring transepithelial electrical resistance and mucosal permeability to hydrophilic compounds. We used the fluorescent molecule fluorescein (375 Da) to assess changes in paracellular permeability induced by the different test solutions. The same molecule and others of similar molecular weight were previously used for this purpose.43 44 Although the magnitude of changes was different, we found a good correlation between reductions in RT (measured in Ussing chambers) and increased permeability to fluorescein after mucosal exposure to both acid and weakly acidic solutions. It has been reported that the presence of DISs is associated with reduction in RT and increase in paracellular permeability.18 In our study, we could confirm such association using acidic solutions and weakly acidic solutions with bile acids at 2 and 5 mmol/l. Measurement of mucosal permeability is theoretically more meaningful and robust than measurements of electrical resistance. This is obvious in the intestinal epithelium. Rabbit oesophageal mucosa is composed of eight to ten layers of cells and the transepithelial electrical resistance is a reflex of the contribution of all the cellular layers: functional layer, prickle layer and basal layer. Changes that only affect the superficial functional layer may provoke a decrease in electrical resistance with small or no increases of trans-mucosal permeability. Although we found some discrepancies between RT and permeability in rabbit oesophageal mucosa, there was a statistically significant correlation between RT and permeability. Isolated RT changes were very rare. The relevance of isolated RT changes without permeability changes in the pathophysiology of GORD is not yet established.
We identified conditions with disruption of oesophageal functional integrity without observable DIS. For example, GC provoked significant changes in RT and permeability but never DIS. Furthermore, at pH 7.4 the highest concentration of TDC and DC produced an identical decrease in RT to that obtained with weakly acidic conditions (pH 5.0), but DIS were not induced. These results suggest that the absence of DIS cannot exclude the possibility of functional alterations in the oesophageal mucosa. The clinical relevance of an isolated functional dysfunction (decreased resistance and/or increased permeability) is unknown. However, our observations suggest that DISs are not the earliest sign of disrupted oesophageal mucosa integrity and an absence of DIS in biopsies from patients with heartburn or chest pain should not exclude the possibility that functional alterations in the oesophageal mucosa can be the origin of the symptoms.
We found that exposure of rabbit oesophageal mucosa to an acidic solution (pH 2.0), containing 1 mg/ml of pepsin, only slightly decreased RT; however, the addition of bile acids consistently provoked a further significant decrease in RT and increase in permeability. This effect was observed even with the lowest bile acid concentration (0.5 mmol/l). Our results showed that short exposure to acid solutions containing concentrations of bile acids similar to those observed in gastric contents in healthy subjects31 can significantly disrupt oesophageal mucosal integrity, probably by altering the intercellular cell-to-cell proteins (desmosomes and tight junctions) or intercellular glycoconjugates.43 45 Both complexes have a crucial role in maintaining the integrity of the epithelium against penetration of fluids and solutes from the lumen sealing the intercellular spaces.46
Exposure of rabbit oesophageal mucosa to weakly acidic solutions, without bile acids, slightly increased RT and decreased permeability. Whether such solutions might have a protective effect, ie, an internal barrier strengthening defence mechanism during physiological reflux, is unknown and further experiments are currently under way to clarify this finding. The effect of weakly acidic solutions was much less marked than that observed with acid solutions requiring higher concentrations of bile acids. The unconjugated bile acid DC and the secondary conjugated TDC induced a clear decrease in RT at 2 and 5 mmol/l. However, those concentrations are within the range expected to be found in postprandial gastric contents of patients with NERD or in patients taking PPIs. Interestingly, the effect was clearly observed with the unconjugated bile acid DC, which is increased in aspirates of patients taking PPIs,42 who frequently have weakly acidic reflux (pH between 5 and 7). These findings suggest that DC might play a significant role in persistence of altered integrity of the oesophageal mucosa in these patients. The difference in magnitude of effect observed with solutions at pH 2 and 5 could have been due to lower activity of pepsin at higher pH. However, previously performed pilot experiments, with and without pepsin, showed no difference in the effect of bile acids on RT.
We found a reduced effect of bile acids in neutral conditions (pH 7.4) provoking significantly smaller changes than those observed when tested in acid and weakly acidic solutions. Only at high concentrations they decreased electrical resistance, but they slightly increased permeability and did not provoke DIS. These results suggest that the magnitude of the effect of short exposure of oesophageal mucosa depends on the acidity, concentration and type of bile acids. It is important to acknowledge, however, that weakly alkaline reflux might be frequent in patients after gastrectomy, but is very rare in patients with NERD or in patients taking PPIs.41
Dilatation of intercellular spaces (DIS) is the most consistent histological feature reported in 41–100% of patients with NERD9 47 and it is suggested to be primarily due to oesophageal mucosa contact with intraluminal acid.15 18 A large study, including 103 patients with NERD, designed to assess reversibility of DIS after 4 weeks of acid suppression therapy with PPIs or ranitidine, showed a reduction (from 76% to 53%) in the prevalence of DIS.16 In addition, patients with NERD in whom oesophageal acid exposure was normalised with long-term PPI treatment but who remained symptomatic, still had DIS.17 These observations suggest that other factors present in the refluxate (not only acid), may be potential effectors in the development of DIS.
We recently observed that acute stress can induce DIS23 and our current experimental data show that bile acids can induce DIS both in acidic and weakly acidic conditions. Furthermore, other agents present in gastric contents such as trypsin and lipase may be candidates to produce DIS.25 Therefore, it is plausible that weakly acidic reflux containing bile acids might be involved in the development of DIS in humans.
Based on our experimental findings, we could speculate on mechanisms involved in symptoms generation or persistence of symptoms in patients with NERD or patients with ERD refractory to PPIs. Duodeno-gastric bile reflux occurs in normal subjects, especially postprandially31 38 48 and at night.36 49 Bilitec monitoring showed that patients with NERD have a slight increase in oesophageal bile exposure2 3 and patients with GORD who are taking PPIs may still have significant oesophageal bile exposure in a weakly acidic environment.6 The results of the present experimental in vitro study suggest that short exposure of the oesophageal mucosa to bile acids in acidic conditions can be enough to provoke dilated intercellular spaces and allow passage of acid or other luminal substance through the mucosa. Similarly, but to a lesser extent than acid, exposure of oesophageal mucosa to bile acids in weakly acidic conditions can impair oesophageal mucosal integrity. Whether such alterations are followed by stimulation of afferent nerves requires further investigation.
In conclusion, the present study showed that bile acids under acidic and weakly acidic conditions can compromise the functional integrity of the oesophageal mucosa and, thereby, can theoretically play a role in the generation of symptoms in patients with NERD and GORD refractory to PPIs.
Acknowledgments
We would like to thank Dr J Van Pelt, Mrs R Renwart and Mrs C Armee for excellent technical support.
REFERENCES
Footnotes
Funding: This work was supported by a “Geconcerteerde Onderzoeksactie” grant from the Catholic University of Leuven, Belgium. RF is postdoctoral fellow, FWO (Research Foundation, Flanders).
Competing interests: None.
Ethics approval: The procedure was approved by the ethics committee for animal experiments of the Catholic University of Leuven, Belgium, on 26 March 2007.
Linked Articles
- Digest