Article Text

Abstract
Backgound and aims: A subset of functional dyspepsia (FD) patients report meal-related symptoms, possibly representing a pathophysiologically homogeneous subgroup. The aim of the present study was to establish the time-course of symptoms in relation to meal ingestion, and to assess the relationship between self-reported meal-related symptoms and pathophysiological mechanisms in FD.
Methods: 218 FD patients (149 women, mean (SEM) age 39 (1) years) filled out a symptom questionnaire, including meal-induced aggravation. All patients underwent a gastric emptying breath test with severity (0–4) scoring of six symptoms (pain, fullness, bloating, nausea, burning and belching) at each sampling (15 min interval for 4 h). In 129 patients, gastric sensitivity and accommodation were assessed by barostat.
Results: The intensity of each FD symptom was significantly increased 15 min after the meal, compared with the premeal score, and remained elevated until the end of the measurement period (all p<0.05). The time-course of individual symptoms varied, with early peaks for fullness and bloating, intermediate peaks for nausea and belching, and late peaks for pain and burning. Meal-induced aggravation was reported by 79% of patients, and in these patients postprandial fullness, which peaked early, was the most intense symptom. In patients without self-reported meal-induced aggravation, epigastric pain, which had a delayed peak, was the most intense symptom and they had a lower prevalence of gastric hypersensitivity (27.5% vs 7.7%).
Conclusion: Meal ingestion aggravates FD symptoms in the vast majority of patients, with symptom-specific time-courses. Postprandial fullness is the most severe symptom in patients reporting aggravation by a meal, while it is pain in those not reporting meal-related symptoms.
Statistics from Altmetric.com
Functional dyspepsia (FD) was defined by the Rome II criteria as a clinical syndrome characterised by chronic or recurrent symptoms centred in the upper abdomen, in the absence of underlying organ disease that is likely to explain the symptoms.1 The symptom complex includes epigastric pain, bloating, postprandial fullness, early satiety, nausea, vomiting, belching and anorexia. Although this is not a compulsory criterion according to the Rome II definition, FD symptoms are often related to a meal.1 In the Rome III criteria, the number of FD symptoms has been reduced to only four, and the relationship with ingestion of a meal has been proposed as a distinguishing feature for FD subgrouping.2
The timing of FD symptoms in relation to a meal has not been studied in great detail. However, systematic studies of dyspeptic symptoms in the general population revealed that the majority of subjects report induction or worsening of symptoms by ingestion of a meal.3 ,4 It remains to be elucidated which symptoms of the dyspepsia symptom complex are related to meal ingestion, and through which mechanism this is occurring.
The pathophysiology of FD is unknown, and several putative mechanisms have been put forward.5 In tertiary care FD, pathophysiological mechanisms associated with the dyspeptic symptom pattern, and therefore likely to be involved in symptom generation, are delayed gastric emptying, impaired gastric accommodation to a meal and hypersensitivity to gastric distention.6–13 By their designation, impaired gastric accommodation and delayed gastric emptying are associated with ingestion of a meal. Similarly, gastric distention occurs most readily during the postprandial state. Hence, these pathophysiological mechanisms could be involved in the generation of meal-related symptoms. Based on studies in tertiary care dyspeptic patients and in asymptomatic obese subjects, symptom intensity 30 min postprandially was found to be influenced by age, fasting gastric volumes and gastric emptying rate.14 ,15 However, these studies used a liquid nutrient challenge meal of variable size, and meal size was also found to be an important determinant of postmeal symptoms, and the studies did not provide details on the evolution of the intensity of different symptoms after ingestion of the meal.
The present study aimed at increasing our understanding of the relationships of symptoms to meal ingestion in FD. First of all, we wanted systematically to investigate and quantify the occurrence and the postprandial time-course of FD symptoms in relation to ingestion of a standardised meal. Secondly, we studied the differences in pattern and timing of symptoms, and the associated pathophysiological mechanisms, in FD patients with or without a self-reported relationship between ingestion of a meal and symptoms.
MATERIALS AND METHODS
Controls
Twenty-eight healthy volunteers (mean (SEM) 28 (1.3) years) were recruited for this study. None of the subjects had symptoms or a history of gastrointestinal disease or drug allergies, nor were they taking any medication. Written informed consent was obtained from each participant. The protocol was approved by the Ethics Committee of the University Hospital.
FD patients
Consecutive new patients with a diagnosis of FD were recruited for the study. All patients presented to the general gastroenterology outpatient clinic or to the motility outpatient clinic because of unexplained dyspeptic symptoms, and underwent careful history taking and clinical examination, upper gastrointestinal endoscopy, routine biochemistry and upper abdominal ultrasound. Inclusion criteria were the presence of dyspeptic symptoms for at least 12 weeks in the last 12 months, in the absence of organic, systemic or metabolic disease, according to the Rome II criteria.1 Two or more dyspeptic symptoms had to be scored as moderate or severe on a dyspepsia symptom questionnaire (see below), and a negative result had to be onbtained on 4-item heartburn word–picture questionnaire.7–9 ,13 ,16 ,17 Exclusion criteria were predominant heartburn, the presence of oesophagitis, gastric atrophy or erosive gastroduodenal lesions on endoscopy, heartburn as a predominant symptom, a history of peptic ulcer, major abdominal surgery, underlying psychiatric illness and the use of non-steroidal anti-inflammatory drugs, steroids or drugs affecting gastric acid secretion. During upper gastrointestinal endoscopy, biopsy specimens were taken from the antrum and the corpus to stain with cresyl violet for the presence of Helicobacter pylori. In patients with relevant or severe epigastric burning on the symptom questionnaire, 24-hour oesophageal pH monitoring was performed and found to be normal (<4% of time pH below 4). Patients with a weight loss of >5% of their initial body weight were assessed by a psychiatrist to rule out anorexia nervosa. All drugs potentially affecting gastrointestinal motility or gastric acid secretion were discontinued at least 1 week prior to the gastric emptying study. Informed consent was obtained from each participant and the Ethics Committee of the University Hospital had approved the study protocol.
Symptom questionnaire
Each patient completed a dyspepsia questionnaire as previously reported and validated.7–9 ,13 ,16 ,17 The patient was asked to grade the intensity (0–3; 0 = absent, 1 = mild, 2 = moderate and 3 = severe, interfering with daily activities) of eight different symptoms (epigastric pain, bloating, postprandial fullness, early satiety, nausea, vomiting, belching and epigastric burning) over the last 3 months. Subsequently, the patient was requested to indicate whether or not symptoms were usually induced or aggravated by ingestion of a meal. Patients were also instructed to identify the single most bothersome symptom on this list of eight symptoms (only one choice was allowed). In addition, the questionnaire also registered the amount of weight lost since the onset of the symptoms. The study population does include patients whose characteristics were already included in previous analyses and publications. However, the present study investigates a specific question that has not been addressed before in this patient population, and all data for the present study, including the assessment of timing and pattern symptoms in relation to meal ingestion, were prospectively collected, and have not been the subject of any previous publication.
Gastric emptying studies
Gastric emptying rates for solids (in all patients and all healthy controls) and liquids were determined using the [14C]octanoic acid and [13C]glycin breath test.9 ,18–20 This test has previously been extensively validated.18 ,19 The test meal consisted of 60 g of white bread, an egg, the yolk of which was doped with 74 kBq of [14C]octanoid acid sodium salt (DuPont, NEN Research, Boston, Massachusetts, USA), and 300 ml of water in which 100 mg of [13C]glycin (99% enrichment; Isotec, Miamisburg, Ohio, USA) was dissolved. All meals were consumed within a 10 min period. The total caloric value of the test meal was 250 kcal (14 g of proteins, 26 g of carbohydrates and 10 g of fat). Breath samples were taken before the meal and at 15 min intervals for a period of 240 min postprandially. At each sampling point, the subject exhaled into two different containers for measuring exhaled 13C and 14C, respectively. One was a liquid scintillation vial containing 2 ml of 1 M hyamine hydroxide and 2 ml of ethanol together with one drop of thymolphthalein solution. This amount of hyamine is neutralised by 2 mM CO2. The end point of neutralisation is indicated by decoloration of the indicator. After decoloration, 10 ml of scintillation cocktail (Hionic Fluor, Packard) was added and radiation was determined by liquid scintillation spectrometry (Packard Tri-Carb Liquid Scintillation Spectrometer, model 3375, Packard Instrument Company, Downers Grove, Illinois, USA). For 13C measurements breath was collected by blowing directly into a tube.
At each breath sampling, the patient was asked to grade the intensity (0–3; 0 = absent; 1 = mild, present in a non-bothersome intensity; 2 = relevant, clearly present and bothersome but not of such intensity that it would interfere with normal daily activities; and 3 = severe, clearly present and of such intensity that it would interfere with normal daily activities) of six different symptoms (epigastric pain, bloating, postprandial fullness, nausea, belching and epigastric burning). We have previously shown the reproducibility of gastric emptying and meal-related symptom testing in patients with dyspepsia and gastroparesis.21
Gastric sensitivity and accommodation studies
Gastric sensitivity and accommodation testing using a gastric barostat was performed in all patients recruited from the motility outpatient clinic (n = 126). Patients who underwent a gastric barostat study reported higher weight than those who did not (6.3 (0.7) kg vs 3.8 (0.6) kg, p<0.01), but demographic features, including body weight and body mass index, and symptom patterns were comparable between both subgroups. Following an overnight fast of at least 12 h, a double-lumen polyvinyl tube (Salem sump tube 14 Ch., Sherwood Medical, Petit Rechain, Belgium) with a finely folded adherent plastic bag (1200 ml capacity; 17 cm maximal diameter) was introduced through the mouth and secured to the subject’s chin with adhesive tape. The position of the bag in the gastric fundus was checked fluoroscopically. The polyvinyl tube was then connected to a programmable barostat device (Synectics Visceral Stimulator, Stockholm, Sweden). To unfold the bag, it was inflated with a fixed volume of 300 ml of air for 2 min with the study subject in a recumbent position, and again deflated completely. The subjects were then positioned in a comfortable sitting position with the knees bent (80°) and the trunk upright in a specifically designed bed.
After a 30 min adaptation period, minimal distending pressure (MDP) was first determined by increasing the intrabag pressure by 1 mm Hg every 3 min until a volume of ⩾30 ml was reached,7 ,8. This pressure level equilibrates the intra-abdominal pressure. Subsequently, isobaric distentions were performed in stepwise increments of 2 mm Hg starting from MDP, each lasting for 2 min, while the corresponding intragastric volume was recorded. Subjects were instructed to score their perception of upper abdominal sensations at the end of every distending step, using a graphic rating scale that combined verbal descriptors on a scale graded 0–6.7 ,8 The end point of each sequence of distentions was established at an intrabag volume of 1000 ml, or when the subjects reported discomfort or pain (score 5 or 6). After a 30 min adaptation period with the bag completely deflated, the pressure level was set at MDP+2 mm Hg during at least 90 min. After 30 min, a liquid meal (200 ml, 300 kcal, 13% proteins, 48% carbohydrates, 39%, Nutridrink, Nutricia, Bornem, Belgium) was administered. In all patients, gastric tone measurement was continued for 60 min after the meal.
Data analysis
The results of the 13CO2 and 14CO2 breath tests were expressed as the percentage 13CO2 and 14CO2, respectively, excreted per hour by calculating procedures described elsewhere. For both carbon labels, CO2 production was assumed to be 300 mmol/m2 of body surface per hour. Gastric half emptying time (t1/2) was calculated from the 13CO2 and 14CO2 excretion curves as previously described.18 ,19 We have previously validated this test against the gold standard of scintigraphy.18 ,19
Symptom scores were obtained before and for 4 h after the standardised meal. For each symptom, a meal-related severity score was obtained by adding scores at all time points. A cumulative meal-related symptom score was obtained by adding individual symptom severity scores. We calculated the time to postprandial symptom peak for each patient for each of the six symptoms. The highest 15 min symptom score during the 240 min postprandial measurement time was determined for each symptom. The time to postprandial symptom peak was defined as the postprandial time span before the patient indicated the highest 15 min symptom score for the first time during the measurement period.
In the gastric sensitivity studies, for each 2 min distending period, the intragastric volume was calculated by averaging the recording. Perception threshold was defined as the first level of pressure and the corresponding volume that evoked a perception score of ⩾1. The discomfort threshold was defined as the first level of pressure and the corresponding volume that provoked a score of ⩾5. Hypersensitivity to gastric distention was defined as a discomfort threshold below the mean–2SD in healthy volunteers (<6.6 mm Hg).8 Gastric tone before and after administration of the meal was measured by calculation of the mean balloon volume for consecutive 5 min intervals. The meal-induced gastric relaxation was quantified as the difference between the average volumes during 30 min before and 60 min after the administration of the meal. Impaired accommodation to a meal was defined as a meal-induced relaxation below the mean–2SD in healthy volunteers (<64 ml).7
Statistical analysis
Meal-related intensity scores were compared between different symptoms. Different curve models (including linear, parabolic, sigmoidal, hyperbolic, exponential, logarithmic, polynomial, trigonometric and power exponential models) were evaluated for goodness of fit of the time after the meal versus symptom intensity curves. The lowest sum of squared errors was used as a measure for the best fit.
Patients were subdivided according to whether or not they indicated that meal ingestion induced or aggravated their symptoms. Demographic variables, perception and discomfort threshold to gastric distention, compliance, and t1/2 for solid and liquid gastric emptying in both group were compared using Student t test. Symptom score data and time to symptom peak data were analysed and compared between patient groups, using a Mann–Whitney test for non-parametric analysis of unpaired non-normally distributed data. A Fisher exact test was used in the univariate analysis. The sex distribution, prevalence of hypersensitivity to gastric distention, impaired accommodation, weight loss >5% of original body weight, delayed gastric emptying and the presence of acute onset of symptoms and of H pylori infection in both patient groups were compared by χ2 testing.
Results are expressed as the mean (SEM). Differences were considered to be significant at the 5% level.
RESULTS
Patient selection and characteristics
Two hundred and eighteen consecutive FD patients (149 women, 69 men, mean age 39 (1) years, body mass index 22.0 (0.3) kg/m2) were eligible for the study. Table 1 summarises the symptom pattern in the patient group as assessed by the questionnaire. Fullness and bloating were the most prevalent symptoms, present in 90%, and 89%, respectively, of the patients. Weight loss in excess of 5% of the original weight body was present in 111 patients (51%). Only eight patients (4%) were H pylori positive. Six H pylori-negative patients had a history of previous successful eradication of H pylori.
Solid gastric emptying was measured in all subjects, and liquid emptying was assessed simultaneously in 198 patients. Solid emptying was delayed in 20% of the patients, and 31% had delayed liquid emptying. Gastric barostat studies to assess gastric sensitivity and accommodation to a meal were performed in 129 patients recruited from the motility clinic. Hypersensitivity to gastric distention was present in 23% of the patients, and 30% had impaired gastric accommodation.
Meal-related symptom scores
Figure 1 summarises the results of meal-related symptom score measurements in healthy controls and in FD patients. In healthy controls, fullness and bloating were significantly increased over baseline from 15 to 150 and 180 min, respectively, after the meal. The intensities of the other symptoms did not increase significantly over baseline. In FD patients, symptom intensity scores are characterised by a rapid increase after meal ingestion to reach a peak intensity, which is followed by a gradual decrease. At the end of the measurement period (240 min), none of the symptoms had returned to baseline value. For each individual symptom, the symptom intensity score 15 min after the meal is already significantly increased compared with the premeal score (time 0), and this significant elevation is maintained until the end of the measurement period (240 min) (all p values<0.05). Only one patient did not report any increase in symptom intensities throughout the postprandial assessment period. Symptom assessment for 4 h postprandially after the currently used meal showed that moderate to severe symptom intensities (scores of ⩾2) were elicited in 94% of the patients. At least moderate symptom intensities for ⩾2 symptoms occurred during the postprandial period in 200 patients (92%).
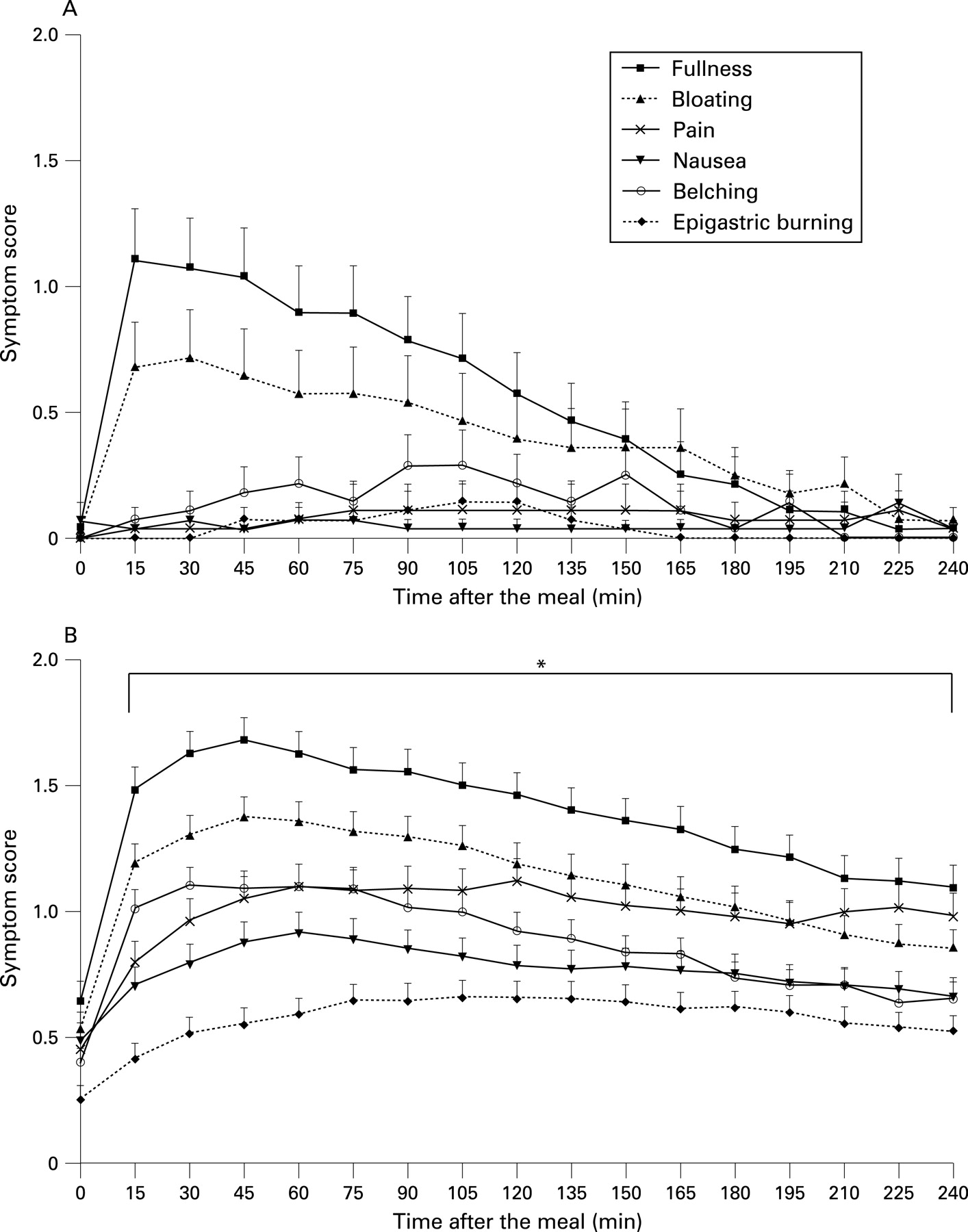
In healthy controls, meal-related symptom intensities were 8.7 (1.9) for fullness, 6.5 (2.1) for bloating, 1.3 (1.2) for pain, 0.9 (0.6) for nausea, 2.2 (0.9) for belching and 0.7 (0.5) for epigastric burning. Table 2 summarises the numerical data on meal-related symptom intensities for individual symptoms in patients, which were significantly higher than in controls for all symptoms (all p<0.001). The highest symptom intensities were recorded for fullness and bloating, and the lowest score was recorded for epigastric burning. Not all symptoms occurred during the measurement period in all patients. Only 12.3% of the patients did not report any postprandial fullness, while up to 47.2% did not report any symptoms of epigastric burning.
Curve fitting revealed two different patterns of evolution of symptom intensities after the meal. For postprandial fullness, a power law with exponential cut-off and with offset (y = C × x(−T) × e(−x/K) + d) provided the best fit (sum of squared absolute errors 0.005, C = 0.383; T = −0.336; K = 139.937; d = 0.647). The same curve type also provided the best fit for bloating (sum of squared absolute errors 0.002, C = 0.217; T = −0.455; K = 112.917; d = 0.535), for nausea (sum of squared absolute errors 0.008, C = 0.042; T = −0.685; K = 99.842; d = 0.497) and for belching (sum of squared absolute errors 0.005, C = 0.233; T = −0.404; K = 108.262; d = 0.403). In these equations the values of T and also of K determine the time to peak. Differences in these values reflect a different time course, especially for nausea compared with the other three symptoms.
For epigastric pain, a sigmoid function with offset (y = a/(1.0 + e(−(x−b)/c)) + d) provided the best fit (sum of squared absolute errors 0.037, a = −0.846; b = 7.029; c = −8.730; d = 1.040). The same curve type also provided the best fit for epigastric burning (sum of squared absolute errors 0.026, a = −0.646; b = 2.938, c = −15.215, d = 0.613).
Calculation of the time to postprandial symptom peak confirmed the presence of different time patterns. Symptom peaks for postprandial fullness and bloating occurred ∼40 min after the meal, which was significantly earlier than for other symptoms. Symptom peaks for epigastric pain and epigastric burning occurred significantly later than other symptoms, while symptom peaks for nausea and belching displayed an intermediate time course (table 2).
Relationship between gastric emptying rate and meal-related symptom scores
Solid gastric emptying was delayed in 44 patients (20.2%). Demographic characteristics and body mass index did not differ between both groups, but patients with delayed gastric emptying had significantly higher meal-induced fullness, bloating, pain and nausea (table 3). Delayed liquid emptying was present in 60 patients (28%), but only the severity of meal-induced nausea was significantly higher in patients with delayed liquid emptying.
Characteristics of FD patients with or without self-reported meal-related symptoms
One hundred and seventy-three patients (79%) indicated that their symptoms were aggravated or induced by ingestion of a meal, while 45 patients (21%) denied such a relationship. Table 4 summarises the demographic and clinical features of patients with or without self-reported meal-induced symptoms. There was no significant difference between both groups in demographic characteristics or prevalence of acute onset of their dyspeptic symptoms or proportion of pain- or discomfort-predominant patients. However, the prevalence of weight loss in excess of 5% of original body weight and the amount of weight loss since the onset of symptoms was significantly higher in FD patients with meal-related symptoms, who had a significantly lower body mass index than those with meal-unrelated symptoms.
On the dyspepsia symptom questionnaire, patients with self-reported meal-related symptoms had a significantly higher prevalence of epigastric pain, postprandial fullness and bloating. Similarly, the prevalence of relevant or severe epigastric pain, postprandial fullness and bloating was significantly higher in patients with self-reported meal-related symptoms (fig 2A).
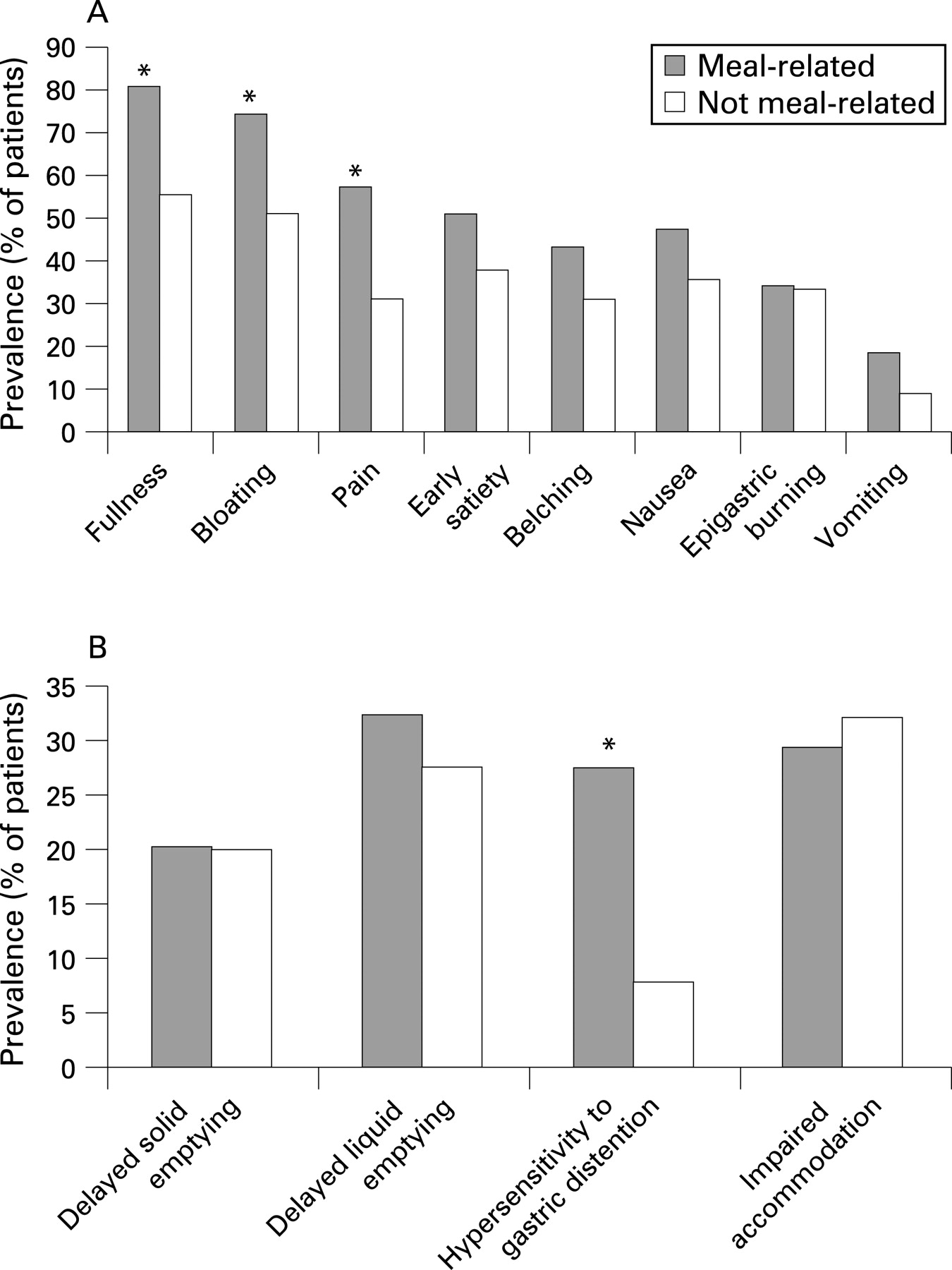
Figure 2B summarises the pathophysiological characteristics of patients with or without self-reported meal-related symptoms. Patients with meal-related symptoms had a lower discomfort threshold (12.4 (1.2) mm Hg vs 9.7 (0.4) mm Hg above MDP, p = 0.01) and a higher prevalence of gastric hypersensitivity (7.7% vs 27.5%, p<0.05). Gastric accommodation (150.7 (24.0) ml vs 144.7 (13.8) ml, NS), gastric emptying rate (liquid t1/2 59.9 (3.6) min vs 68.5 (2.6) min, NS; solid t1/2 91.3 (8.9) min vs 92.6 (5.6) min, NS) and the prevalence of impaired accommodation (32% vs 29%, NS), and delayed liquid or solid gastric emptying (28% vs 32% and 20% vs 20%, respectively, NS) did not differ between both groups.
Meal-related symptom scores in FD patients with or without self-reported meal-related symptoms
Patients with self-reported meal-related symptoms had significantly higher meal-induced fullness and bloating compared with those without self-reported meal-related scores (table 5). Fullness and bloating had the highest meal-related symptom scores in patients with self-reported meal-related symptoms, whereas patients without self-reported meal-related symptoms reported the highest meal-related scores for pain (table 5). In addition, the time-course of symptoms after ingestion of a standard meal for patients with or without self-reported meal-related symptoms showed significant increases in symptom intensity after a meal in both groups (fig 3). The early postprandial rise in symptom intensity, especially for bloating and fullness, is less prominent in patients without self-reported meal-related symptoms, but significant increases are seen for most symptoms throughout the post-meal period. Furthermore, the time to postprandial symptom peak did not differ significantly for any symptom between patients with or without meal-related symptoms (table 5). Hence, relative symptom intensities, rather than a different timing or pattern of symptoms after a meal, seem to determine whether or not patients perceive their symptoms as meal-related.

{kind=link}
{kind=link}
{kind=link}
DISCUSSION
FD is often considered a heterogeneous disorder, in symptom spectrum as well as in underlying pathophysiological mechanisms.5 Recent epidemiological studies suggest that a large subset of subjects with dyspeptic symptoms report a relationship of symptoms to meal ingestion, whereas another important subgroup does not indicate such a relationship.3 ,4 The relationship between meal ingestion and FD symptoms has received little attention in the literature. While no data have been reported for solid meals, Hausken et al reported the occurrence of symptoms in all patients within 1 min after ingestion of a liquid meal.22 Delgado et al found that symptom intensity at a fixed time point 30 min after a challenge meal was associated with meal volume, fasting gastric volume and gastric emptying rate.14 ,15 It is unknown whether meal-related symptoms are associated with specific FD symptoms, or with specific types of underlying pathophysiological disturbance.
In order to elucidate the timing, prevalence and severity of FD symptoms, we systematically quantified the occurrence and severity of symptoms in 218 FD patients after ingestion of a standardised solid meal. We found that symptoms in FD patients as a group are characterised by a significant rise in intensity, immediately after the ingestion of a meal. This significant elevation in symptom intensity was maintained throughout the 4 h postprandial measurement period, and during this interval the intensity of none of the six symptoms that were assessed had returned to baseline. Curve fitting revealed two different types of evolution of symptoms after a meal, with epigastric burning and pain best described by a sigmoid curve pattern, and fullness, bloating, nausea and belching following a power law with exponential cut-off. Curve descriptors for the power law differed between fullness/bloating and nausea/belching. The time to reach maximum symptom intensity varied for different symptoms, with an early peak of fullness and bloating, a later peak of nausea and belching, and an even later peak of epigastric pain and burning. Although not every symptom occurred in all patients, most patients reported more than one symptom, and the meal-induced rise was a consistent finding in all but one patient. These data therefore convincingly demonstrate that symptoms are meal related in the vast majority of FD patients. We also studied the occurrence of postprandial symptoms after the same test meal in healthy volunteers. This induced only mild and transient fullness and bloating, with a return to baseline after 150–180 min, while significant increases in other symptoms were not induced by the meal. These observations therefore suggest that prolonged induction of epigastric symptoms after meal ingestion is a feature of FD, and not of health.
The pathophysiology of FD is incompletely understood, and several mechanisms have been implicated, including delayed gastric emptying, hypersensitivity to gastric distention, impaired gastric accommodation or H pylori infection. Recent, large studies suggest a significant but weak association between delayed solid gastric emptying and symptoms of postprandial fullness, nausea or vomiting in FD.6 ,9–13 In the present study, the standardised meal was the [13C]octanoic acid, [14C]glycin breath test meal, and breath samples were collected throughout the measurement period. In this close temporal setting, we observed that patients with delayed solid gastric emptying reported higher scores for meal-related fullness, bloating, nausea and pain. However, we did not observe any difference in timing of the postprandial symptom peak between FD patients with delayed or normal gastric emptying time for solids or liquids. Taken together, these observations seem to argue against an important role for delayed gastric emptying in the pathogenesis of meal-related symptoms. Although scintigraphy is often considered the gold standard for measurement of the gastric emptying rate, the breath test we used has been validated against scintigraphy.18 ,19 A number of different curve fit models have been proposed to analyse the results of gastric emptying breath tests,23 but it is highly unlikely that the use of a different mathematical analysis would have resulted in a differential association of symptoms with half emptying times in the current analysis. However, the current analysis, which only used the half emptying time as a measure of emptying kinetics, does not exclude a possible contribution of other specific aspects or phases of the emptying process, such as the lag phase, or regional emptying kinetics. Moreover, the analysis does not take into account the variation of the symptom intensities over time during the emptying process. Extensive analyses of the correlation between meal-induced symptoms and the emptying process are required, but addressing these issues is beyond the scope of the present study.
Epidemiological studies both in the USA and in Europe have shown that 40–50% of subjects with dyspeptic symptoms indicate that their symptoms are meal related.3 ,4 The present study confirms that such a disctinction is also present in FD patients seen at a specialised referral centre. The higher prevalence of meal-related symptoms in the current tertiary care patient sample may reflect referral bias due to the higher prevalence of weight loss in meal-related FD on one hand, and due to the tradition of motility research in our centre on the other hand.
It has been suggested that different pathophysiological mechanisms and genetic predispositions might underlie meal-related and meal-unrelated dyspeptic symptoms,2 ,3 ,23 and that subdividing patients according to whether or not symptoms are meal related might be clinically meaningful.2 We systematically assessed this in the present study, and found that 79% of the patients reported that their symptoms were meal related. These patients had suffered more weight loss and were more likely to have hypersensitivity to gastric distention compared with patients without self-reported meal-related symptoms, where the prevalence of gastric hypersensitivity was very low. However, the prevalence of other putative pathophysiological mechanisms such as delayed solid or liquid gastric emptying, and impaired accommodation to a meal, did not differ between both groups. The most consistent difference between patients with or without self-reported meal-related symptoms was a higher reporting of postprandial fullness and bloating, both on symptom questionnaires and during assessment of meal-related symptoms, in patients who reported meal-related symptoms. However, systematic analysis of the occurrence and severity of symptoms after ingestion of a standardised meal revealed that meal ingestion significantly increased dyspeptic symptoms, even in those patients who did not report meal-induced aggravation on a questionnaire.
In contrast, the symptom with the highest intensity in the 4 h postprandial assessment window was different in both groups: postprandial fullness in patients who reported meal-related symptoms and epigastric pain in patients reporting meal-unrelated dyspeptic symptoms. These observations agree with a previous study in the general population where the presence of meal-related dyspeptic symptoms was positively associated with the postprandial fullness score and negatively with the epigastric pain score.4 They are also in support of the Rome III FD subdivision into postprandial distress syndrome (meal-related dyspeptic symptoms, characterised by postprandial fullness and early satiation) and epigastric pain syndrome (meal-unrelated dyspeptic symptoms, characterised by epigastric pain and epigastric burning).2 Hence, it seems that the nature of the most intense symptom is a determinant of whether or not an FD patient perceives symptoms as meal related or not. Although all symptoms increase after a meal, the early meal-related peak of a symptom such as postprandial fullness may render recognition of the relationship with the ingested meal obvious. In contrast, for epigastric pain, which rises at a different and slower rate after a meal, and which reaches a peak only late after meal ingestion, the relationship with the meal may be much less obvious to the patient.
The present study has a number of limitations. First of all, patients were recruited from a tertiary centre with specific interest in motility, and this may contribute to the symptom pattern, the large proportion of patients reporting meal-related symptoms and the low prevalence of H pylori infection. A second limitation is the lack of prolonged symptom recording in the preprandial phase. While it is true that symptoms may fluctuate over time during fasting, addressing this aspect was not the aim of the study. On the other hand, a follow-up of symptoms for 4 h after a relatively small meal may include fasting state symptoms, and this is supported by the rise of symptoms of epigastric pain and burning in the second half of the measurement period. A third limitation is that overlap with irritable bowel syndrome (IBS) was not taken into account in the analysis of the symptom pattern, while a subset of IBS patients also report aggravation of symptoms by ingestion of a meal.24 Furthermore, we did not assess the influence of variations in composition or caloric contents of the meal. Finally, the design of the study required conscious oral ingestion of the meal. It is unknown whether similar symptom evolution would occur if the meal was administered blindly—for example, via a nasogastric tube. All these aspects are beyond the scope of the present study, but will be addressed in future research.
In conclusion, we showed that the vast majority of FD patients have meal-related symptoms. Although all symptoms are significantly increased by meal ingestion, the time course after the meal varies between individual symptoms. The timing of meal-related symptoms does not differ between patients with a normal or delayed gastric emptying rate for solids or liquids, but symptom severity is higher in those with delayed emptying. The major distinction between patients with and without self-reported meal-related symptoms is the type of symptom that has the highest intensity. The highest symptom intensity after a meal is for postprandial fullness in those who report meal-related symptoms, and epigastric pain in those reporting meal-unrelated symptoms. These observations support the Rome III subdivision into postprandial distress syndrome and epigastric pain syndrome.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: The protocol was approved by the Ethics Committee of the University Hospital
Ethics approval: Written informed consent was obtained from each participant.