Article Text

Abstract
Background: Synchronous occurrence of intraductal papillary mucinous neoplasm (IPMN) and ductal carcinoma of the pancreas has been reported. Branch duct IPMNs with lower likelihood of malignancy are not submitted to resection but are followed-up, so ductal carcinoma may develop during the follow-up. The development of ductal carcinoma of the pancreas during follow-up of branch duct IPMNs was investigated.
Methods: 60 patients with branch duct IPMN who had an intraductal tumour of <10 mm on imaging examinations and a negative result for malignancy on cytological examination of the pancreatic juice were investigated. They were followed-up mainly by ultrasonography (US), and additionally by endoscopic ultrasonography (EUS), CT, magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP) with cytological examination of the pancreatic juice for an average period of 87 months.
Results: Ductal carcinoma of the pancreas distinct from IPMN developed in 5 of 60 (8%) branch duct IPMNs during follow-up. The 5-year rate of development of ductal carcinoma was 6.9% (95% CI 0.4% to 13.4%), the incidence of ductal carcinoma was 1.1% (95% CI 0.1% to 2.2%) per year and the standardised incidence ratio of development of ductal carcinoma was 26 (95% CI 3 to 48). Patients >70 years old developed ductal carcinoma significantly more frequently than those under 69. Four of five ductal carcinomas identified during follow-up were resectable. Cancer developed in IPMN in 2 of 60 (3%) branch duct IPMNs during follow-up.
Conclusions: During follow-up of branch duct IPMNs, ductal carcinoma of the pancreas not infrequently developed distinct from IPMN. In the follow-up of IPMN, special attention should be paid to the development of ductal carcinoma of the pancreas.
Statistics from Altmetric.com
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas is a unique clinicopathological entity characterised by cystic dilatation of the main or branch pancreatic ducts, mucus production and intraductal papillary growth.1–5 According to the site of the IPMN, it is classified into two types: main duct IPMN and branch duct IPMN.6 The World Health Organization (WHO) defined IPMN as an intraductal mucin-producing neoplasm with tall columnar mucin-containing epithelium with or without papillary projections, which shows a wide spectrum of histological differentiation from hyperplasia, adenoma, carcinoma, to invasive carcinoma, which is a so-called adenoma–carcinoma sequence.7 ,8 The prognosis of IPMN is favourable compared with that of ductal carcinoma of the pancreas if it is resected while it is still an intraductal carcinoma.4 ,5
Current issues in the management of branch duct IPMN are the selection of candidates for surgical resection and development of intraductal papillary mucinous carcinoma during follow-up of IPMN that was not resected.6 The third issue is the development of independent ductal carcinoma of the pancreas during follow-up of IPMN. Recently, synchronous or metachronous occurrence of IPMN and ductal carcinoma of the pancreas has been reported.9–12 However, there have been few instances in the literature describing the development of ductal carcinoma of the pancreas during follow-up of IPMN. As the prognosis of IPMN is favourable compared with that of ductal carcinoma, the prognosis of the patient with IPMN is dependent on the ductal carcinoma that may occur during the follow-up. In the present study, we investigated the development of ductal carcinoma of the pancreas during follow-up of branch duct IPMN.
PATIENTS AND METHODS
Branch duct IPMN was radiologically defined as dilated branch ducts with a minimum size of 10 mm connecting to the main duct. In all IPMNs, mucus in the main duct or branch ducts was identified by endoscopic retrograde cholangiopancreatography (ERCP). Patients with branch duct IPMN underwent ultrasonography (US), endoscopic ultrasonography (EUS), CT or magnetic resonance cholangiopancreatography (MRCP). They also underwent cytological examination of the pancreatic juice, which was performed with pancreatic juice collected at ERCP by a thin catheter inserted into the main duct or branch ducts. Sixty patient with branch duct IPMNs that had a lower likelihood of malignancy were investigated. Patients with branch duct IPMNs with an intraductal tumour, which is commonly termed a mural nodule, of <10 mm and who did not have malignant cells in the pancreatic juice were included. Those with branch duct IPMNs that had an intraductal tumour of ⩾10 mm or malignant cells in the pancreatic juice were excluded as these tumours were submitted to resection. Clinical characteristics of the patients with branch duct IPMN are summarised in table 1.
These patients with IPMN were followed-up mainly by US every 3 or 6 months. The average follow-up period was 87 months. During observation by US, optional imaging examinations such as EUS, CT or MRCP were performed when enlargement of the main duct, branch ducts, intraductal tumour or pancreatic tumour was seen. During observation, additional cytological examination of the pancreatic juice or endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) was performed when the main duct, branch ducts or intraductal tumour enlarged remarkably, or a pancreatic tumour was detected. When the occurrence of a ductal carcinoma distinct from IPMN or cancer in IPMN was confirmed, surgical resection was recommended.
Development of ductal carcinoma distinct from IPMN or cancer in IPMN was analysed by the Kaplan–Meier method. Statistical analysis was performed by the log-rank test to compare differences in development rate between the subgroups of IPMN. The confidence interval of the annual incidence of development of cancer was estimated by assuming a Poisson distribution. The incidence of pancreatic cancer in a control group matched for age and gender over the follow-up period was calculated, with age- and gender-specific mortality of pancreatic cancer recorded in the Vital Statistics of Japan in 2006 published by the Ministry of Health, Labor and Welfare. Mortality of pancreatic cancer was substituted for incidence of pancreatic cancer considering its devastatingly poor prognosis.
RESULTS
Changes in characteristics of branch duct IPMNs found by imaging examinations during follow-up
Changes in the characteristics of branch duct IPMN found by imaging examinations during follow-up are shown in table 2. Of 60 branch duct IPMNs, the sizes of the main duct were <4 mm in 35 (58%) and between 5 and 9 mm in 25 (42%) at initial examination. The main ducts were <4 mm in 28 (47%), between 5 and 9 mm in 27 (45%) and >10 mm in 5 (8%) at the latest examination. The sizes of the branch ducts were <29 mm in 48 (80%), between 30 and 39 mm in 8 (13%) and >40 mm in 4 (7%) at initial examination. The branch ducts were <29 mm in 28 (47%), between 30 and 39 mm in 21 (35%) and >40 mm in 11 (18%) at the latest examination. The sizes of the intraductal tumour were <4 mm in 57 (95%) and between 5 and 9 mm in 3 (5%) at initial examination. The tumours were <4 mm in 52 (87%), between 5 and 29 mm in 7 (12%) and >10 mm in 1 (2%) at the latest examination.
Development of ductal carcinoma of the pancreas distinct from IPMN during follow-up
Ductal carcinoma of the pancreas distinct from IPMN developed in 5 of 60 (8%) patients with branch duct IPMNs during follow-up. The 5-year rate of development of ductal carcinoma analysed by the Kaplan–Meier method was 6.9% (95% CI 0.4% to 13.4%), which is shown in fig 1. The incidence of ductal carcinoma was 1.1% (95% CI 0.1% to 2.2%) per year. The expected incidence of pancreatic cancer in the control group matched for age and gender was calculated to be 0.045% per year. The standardised incidence ratio was 26 (95% CI 3 to 48).

The clinicopathological features of the pancreata that had harboured branch duct IPMN and developed ductal carcinoma distinct from IPMN during follow-up are summarised in table 3. These IPMNs were in the head in three, in the body in one and in the tail in one patient. At the initial diagnosis of IPMN, the widths of the main duct were 3 mm in four and >4 mm in one patient. They did not enlarge during follow-up, except for one in which the width of the main duct was 8 mm. The sizes of the dilated branch ducts were <29 mm in four and >30 mm in one patient at initial diagnosis. They did not enlarge in two and did enlarge in three patients. At initial diagnosis an intraductal tumour of 5 mm was detected in one patient, and during follow-up an intraductal tumour of 5 mm appeared in another patient. Periods from the initial diagnosis of IPMN to the development of ductal carcinoma ranged from 18 to 112 months. Ductal carcinomas occurred in the head in two, in the body in two and in the tail in one pateint. They were detected by US in two and by CT in two patients. In the remaining patient, an upstream dilatation of the main duct shown by MRCP suggested ductal carcinoma. Malignancy was confirmed by cytological examination of the pancreatic juice in three, EUS-FNA in one and US-FNA in one patient. The sizes of the ductal carcinomas were <19 mm in two and >20 mm in three patients. They were at stage III in three and stage IVA in two patients according to the UICC classification. Four were identified at a resectable stage; two were successfully resected and two were not because of the age of the patients. The ductal carcinoma in the remaining patient was detected at an unresectable stage.
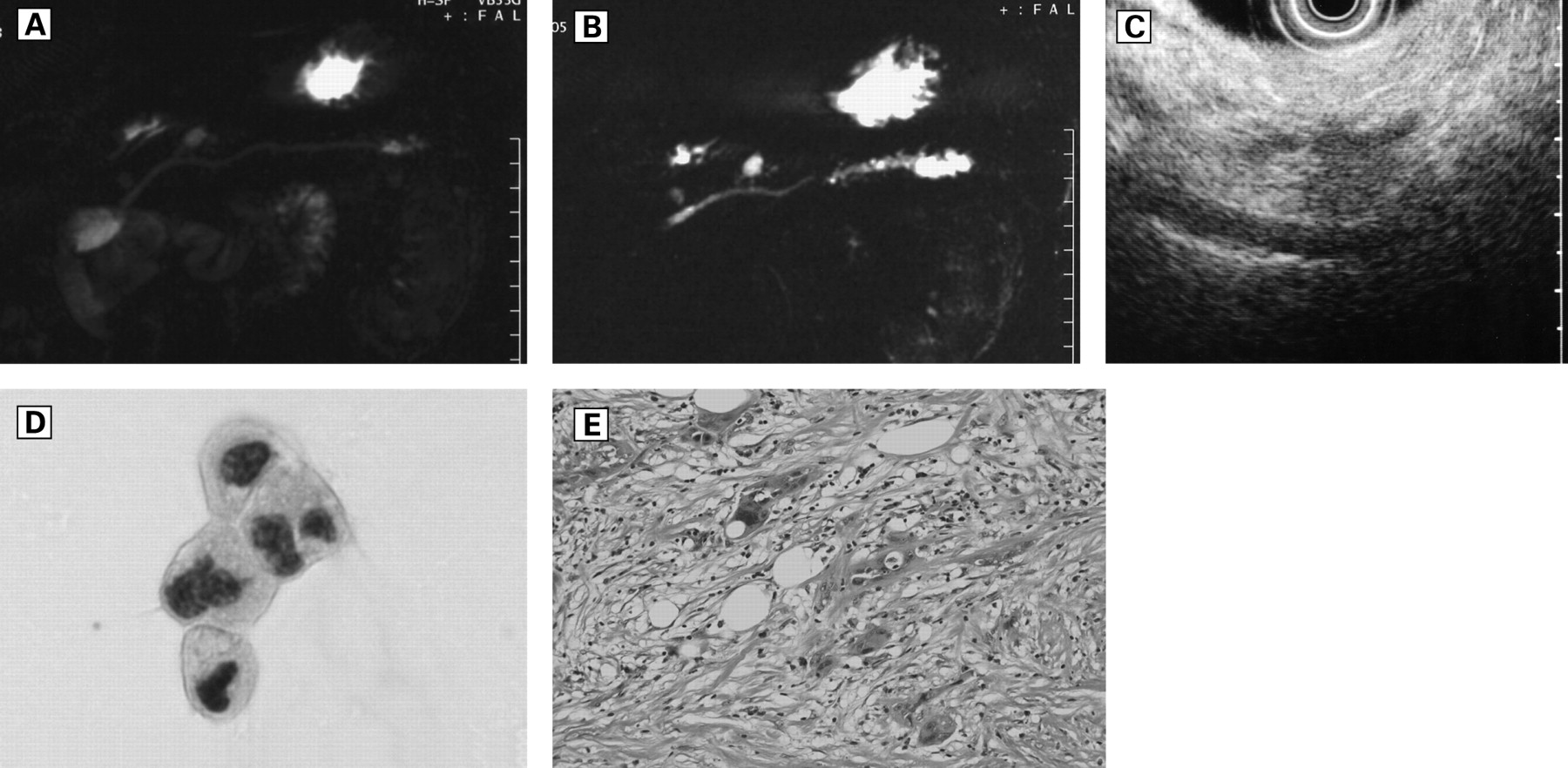
MRCP detected a branch duct IPMN in a 69-year-old male patient (fig 2A). At 112 months after the initial diagnosis, stenosis and upstream dilatation of the main duct were shown by MRCP (fig 2B). EUS showed a low echoic tumour in the tail of the pancreas (fig 2C). ERCP and cytological examination of the pancreatic juice were performed, which suggested pancreatic carcinoma (fig 2D). Surgical resection was performed and pathological examination of the resected specimen revealed a ductal carcinoma (fig 2E).

{kind=link}
{kind=link}
A comparison of the development of ductal carcinoma distinct from branch duct IPMN between subgroups of IPMN
The development of ductal carcinoma in subgroups of branch duct IPMN was analysed by the Kaplan–Meier method (table 4). In patients >70 years old, the 5-year rate of development of ductal carcinoma was 19.4% (95% CI 2.3% to 36.5%), which was significantly more frequent than that in patients under 69 years old. Female patients, those with a branch duct IPMN with a main duct of <3 mm and those with an intraductal tumour of >3 mm developed ductal carcinoma more frequently than the remaining patients. These differences did not reach statistical significance.
Patients with branch duct IPMNs that developed intraductal papillary mucinous carcinoma during follow-up
During follow-up of the 60 patients with branch duct IPMNs, cancer developed in the neoplasms themselves in two patients (3%). One was resected successfully and pathological examination of the resected specimen disclosed an intraductal papillary mucinous carcinoma. In the other case, an intraductal tumour developed to >10 mm, but the patient refused further examinations or surgical resection. Subsequently, she developed multiple lung metastases and died of cancer.
DISCUSSION
In the present study, we followed-up 60 patients with branch duct IPMNs for an average period of 87 months and detected ductal pancreatic carcinoma distinct from IPMN in 5 of 60 patients (8%). The 5-year rate of development of ductal carcinoma was 6.9% (95% CI 0.4% to 13.4%), the incidence of ductal carcinoma was 1.1% (95% CI 0.1% to 2.2%) per year and the standardised incidence ratio of development of ductal carcinoma was 26 (95% CI 3 to 48).
There have been few investigations on the development of ductal carcinoma of the pancreas during follow-up of IPMN, but several reports described the synchronous or metachronous occurrence of ductal carcinoma and IPMN. Sohn resected 60 IPMNs of the pancreas and discovered infiltrating adenocarcinoma in the remnant pancreas in two patients (3%).9 These two patients had undergone margin-negative pancreaticoduodenectomy for the IPMN, and the second primary cancer was detected ∼10 years after the resection. Komori reported a patient who developed ductal carcinoma in the remnant pancreas 9 years after the resection of an intraductal papillary mucinous carcinoma in the pancreatic head.10 Yamaguchi found ductal carcinoma of the pancreas in 7 of 76 patients (9%) with IPMN.11 They consisted of five patients who harboured IPMN and ductal carcinoma synchronously, one patient who developed ductal carcinoma 4 years after the resection of IPMN, and one patient who developed ductal carcinoma 7 years after the resection of synchronous IPMN and ductal carcinoma. All the IPMNs were branch duct IPMNs with an average size of 30 mm. Three were located in the head, two in the body and three in the tail of the pancreas. All of them were adenomas with moderate dysplasia. Kamisawa reported two patients who had IPMN and ductal carcinoma synchronously and one patient who developed ductal carcinoma 3 years after the initial diagnosis of IPMN.12 These were branch duct IPMNs, located in the pancreatic head, and ranged from 1.5 to 3.0 cm. Recently, Tada followed-up 197 cystic lesions of the pancreas including 80 branch duct IPMNs and 117 non-IPMN cysts for an average period of 3.8 years, and found five ductal carcinomas between 14 and 60 months after the diagnosis of cystic lesions.13 In two patients, ductal carcinomas were <2 cm, arising in apparently different sites from the cystic lesion. In one patient, ductal carcinoma developed around the pre-existing cystic lesion. In the remaining two patients, the tumours were too large to evaluate any local relationship between carcinoma and cystic lesion. Thus IPMN may be an indicator of a precancerous state of the pancreas, and ductal carcinoma not infrequently occurred in the pancreas distinct from IPMN.
The mechanism of development of ductal carcinoma in the pancreas harbouring IPMN has not been clarified, but a K-ras mutation may play an important role. The mutation, which is frequently detected in ductal carcinoma,14 ,15 was also present in IPMN.16 ,17 In addition, it was also found in flat or papillary mucous cell hyperplasia, which is one of the bases of histological differentiation in the adenoma–carcinoma sequence of IPMN.18 The mucous cell hyperplasia was not exclusive to IPMN, but all types of hyperplasia such as non-papillary, papillary and atypical hyperplasia were frequently found in the pancreas harbouring ductal carcinoma.19 In the pancreas harbouring IPMN, such a mucous cell hyperplasia that harboured a K-ras mutation and was not identified by imaging examinations might be a background for the development of ductal carcinoma of the pancreas.
A recent investigation of the immunohistochemical mucin expression pattern in pancreatic neoplasms suggested a close relationship between IPMN and ductal carcinoma.20 This investigation divided IPMN into three subgroups on the basis of MUC1 and MUC2 staining: expressing MUC2 alone, coexpressing MUC1 and MUC2, and expressing predominantly MUC1. The largest group of IPMNs expressed MUC2 alone, which was specific to IPMN. On the other hand, a minority of IPMNs expressed predominantly MUC1, which was expressed particularly in ductal carcinoma, suggesting that, even if not all, a small group of IPMNs were closely related to ductal carcinoma. This speculation was supported by the tubular pattern of the invasive component shown by histological examination in MUC1-positive IPMNs.
In IPMN, besides synchronous or metachronous occurrence of ductal carcinoma of the pancreas, high incidences of additional primary cancer have been described.12 ,21–23 According to these studies, 10–35% of patients with IPMN had previous, concomitant or subsequent primary malignancies of other organs. Such extrapancreatic cancers included stomach, colorectal, biliary tract and lung cancers. Development of multiple primary malignancies can be explained by the inheritance of a predisposing genomic defect, or field carcinogenesis, which means that organ systems that have developed a neoplasm are likely to develop multiple and independent neoplasms because all cells have been exposed to carcinogens to similar extents. Another reason may be a more favourable prognosis of IPMN. Patients with neoplasms with a more favourable prognosis will survive longer and have more cancers throughout their lifetime, because older age is naturally associated with more cancers. These explanations may be true for the occurrence of ductal carcinoma of the pancreas in patients with IPMN.
The international consensus guidelines published in 2006 recommended surgical resection of branch duct IPMNs with a higher likelihood of malignancy.6 Predictors of malignancy in branch duct IPMN were branch ducts of >30 mm,24–29 35 mm,30 40 mm31 or 50 mm,32 and a mural nodule, which is termed an intraductal tumour in the present study, of >5 mm,28 10 mm31 ,32 or sizes not described.25–27 ,29 ,30 ,33 Thus predictive criteria for malignancy in branch duct IPMN are numerous and controversial. Cytological examination of the pancreatic juice is a useful diagnostic option in the prediction of malignancy not only in main duct IPMN34 ,35 but also in branch duct IPMN,36 which is recommended in the management of branch duct IPMNs.6 Yamaguchi reported a sensitivity of ∼50% for malignancy in branch duct IPMN,36 which was equal to the result of our investigation (data not shown). In the present study, we followed-up branch duct IPMNs that did not have an intraductal tumour of more than 10 mm and malignant cells on cytological examination of the pancreatic juice. During follow-up of IPMNs for an average period of 87 months, only 2 of 60 patients with IPMN developed intraductal papillary mucinous carcinoma. This frequency of development of intraductal papillary mucinous carcinoma is as low as those found in recent follow-up studies,13 ,24 ,37 ,38 which indicated that our follow-up criteria for IPMN were quite reasonable.
It had been expected that ductal carcinoma of the pancreas which develops during follow-up of IPMN could be detected at an early stage as the patients had been under close surveillance by periodical imaging examinations every 3 months. In the present study, four of five ductal carcinomas detected during follow-up were resectable, but all of them were advanced cancers. A follow-up study of 197 cystic lesions of the pancreas by Tada detected five ductal carcinomas, but only two of them were resectable.13 Another follow-up study by Allen of 369 cystic lesions of the pancreas detected eight ductal carcinomas, but only three of them were resectable.39 These results indicated that the detection of ductal carcinoma at an early stage was still difficult even under close surveillance by imaging examinations, suggesting that the identification of a higher risk group for the development of ductal carcinoma would be necessary.
We tried to determine the clinical subgroups of IPMN that were at higher risk for the development of ductal carcinoma. In the present study, patients over 70 years old developed ductal carcinoma significantly more frequently than younger patients. Female patients, and those with IPMN with a main duct of <3 mm or an intraductal tumour of >3 mm developed ductal carcinoma distinct from IPMN more frequently than the remaining patients, although the difference was not significant. Recent reports on synchronous or metachronous occurrence of IPMN and ductal carcinoma described that such patients were elderly, male and had branch duct IPMNs.11–13 They did not describe the widths of the main duct, but the sizes of dilated branch ducts were smaller, ranging from 15 to 40 mm,11 from 15 to 30 mm,12 and from 10 to 40 mm.13 These results were consistent with those of our present investigation except for the predisposition of male patients to the development of ductal carcinoma. Although it is unknown why such patients with IPMN developed ductal carcinoma more frequently, in the follow-up of IPMN it should be remembered that these patients with IPMN are at higher risk for the development of ductal carcinoma.
In conclusion, patients with a branch duct IPMN that had a lower likelihood of malignancy not infrequently developed ductal carcinoma distinct from IPMN during observation. In the follow-up of branch duct IPMN, special attention should be paid to the occurrence of ductal carcinoma distinct from IPMN. A follow-up examination system for IPMN should be established so that such ductal carcinoma could be detected while it is resectable.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Ethics approval was obtained for this study.