Article Text

Abstract
Background: Gastric sensorimotor dysfunction, psychosocial factors and somatisation are all implicated in symptom generation in functional dyspepsia (FD).
Aim: To determine the relative contribution of each of these factors to overall dyspeptic symptom severity and weight loss in FD.
Methods: In 201 consecutive tertiary care patients with FD (mean age 40.1 (SD 12.6) years), gastric sensorimotor function was studied using barostat (sensitivity, compliance and accommodation). Psychosocial factors (depression and anxiety disorders, positive and negative affect, perceived stress, alexithymia and history of abuse), somatisation and co-morbid irritable bowel syndrome (IBS) and chronic fatigue symptoms were assessed using self-report questionnaires. Variables were correlated with dyspepsia symptom severity (DSS) and weight loss. Hierarchical multiple linear regression was used to identify determinants of DSS and weight loss.
Results: Multiple linear regression identified the following determinants of DSS: gastric sensitivity (β = 0.77, p = 0.25), depression (β = 0.12, p = 0.06) and somatisation (β = 0.48, p<0.0001) (controlling for age and occupation, R2 = 0.29, p<0.0001). The effect of depression on DSS is partially mediated by somatisation. Gastric sensitivity (β = 2.87, p = 0.08), history of childhood sexual abuse (β = 9.37, p = 0.0006), depression (β = 0.19, p = 0.24) and somatisation (β = 0.67, p = 0.01) are independent determinants of weight loss (controlling for gender and occupation, R2 = 0.42, p<0.0001). The effect of depression on weight loss is fully mediated by somatisation.
Conclusion: Symptom severity and weight loss in FD are determined by psychosocial factors (depression, abuse history) and somatisation, and only to a lesser extent by gastric sensorimotor function. The importance of psychosocial factors and somatisation compared to gastric sensorimotor function is most pronounced in hypersensitive patients.
Statistics from Altmetric.com
Functional dyspepsia (FD) is a syndrome defined by the presence of symptoms originating from the gastroduodenal region, without identifiable cause by conventional diagnostic means.1 Its pathophysiology remains incompletely understood and is likely to be multifactorial.2 3 According to the biopsychosocial model, FD symptoms result from a complex reciprocal interaction between biological, psychological and social factors. The role of these factors in FD can be predisposing, precipitating or perpetuating.2–5
Evidence in the literature supports the relevance of the biopsychosocial model to FD. First, symptom generation/reporting in FD is associated with gastric sensorimotor dysfunction; different symptom clusters are associated with different gastric sensorimotor abnormalities.6–8
Second, there is growing evidence for an association between functional gastrointestinal disorders (FGIDs), including FD, and psychopathology, not only in treatment-seeking but also in community populations.9–12 In addition, psychopathological factors influence FD symptom generation/reporting.7 13–17 For example, FD symptoms correlate with anxiety, anger–hostility, depression and general psychological distress.15 18 Neuroticism and a history of psychological abuse are associated with an FD symptom cluster characterised by epigastric pain and burning.7 Finally, alexithymia, anxiety and depression correlate with gastrointestinal (GI) symptoms in a mixed FGID group.19
Third, somatisation is believed to play an important role in functional somatic syndromes (FSSs) (or somatoform disorders) in general20 and in FD in particular.21 In FD, somatisation correlates with epigastric pain, epigastric and retrosternal burning and total dyspeptic symptom scores.7 18 Somatisation can be defined in several ways, the common element being “... presence of somatic symptoms that cannot be (adequately) explained by organic findings.”20 22 However, this descriptive definition can be conceptualised in several ways, the most important distinction being between “presenting somatisation” (secondary to psychological distress) and “functional somatisation” (primary phenomenon).20 22–24
In summary, FD symptoms are associated with gastric sensorimotor dysfunction, with psychosocial factors and with somatisation. However, the available literature consists exclusively of studies investigating the role of each of these separately. Our aim was to establish the relative contribution of gastric sensorimotor dysfunction, psychosocial factors and somatisation to FD symptoms and weight loss. Given the previously published differences between hyper-sensitive and normosensitive patients,6 7 25 we analysed the whole patient sample as well as both subgroups separately.
MATERIALS AND METHODS
Patient sample
Consecutive Dutch-speaking patients recently diagnosed with FD (either at their visit to our clinic or at a recent visit to a secondary-care gastroenterologist which led to referral to our centre) were recruited between January 2002 and August 2007. The patient sample of the present study does not overlap with study populations from previous studies by our group,6–8 but it does overlap with the study population from our recent study on the relationship between anxiety and gastric sensorimotor function in FD.25 Further details about patient selection have been published recently.25
Gastric sensorimotor function testing
Details about gastric sensorimotor function testing have been published recently.25 Briefly, we used our standard barostat protocol. During isobaric stepwise distension, patients scored their perception of upper abdominal sensations at the end of every distending step using a graphic rating scale (0–6) with verbal descriptors. Perception, discomfort and pain thresholds were defined as the lowest pressure above minimal distending pressure (MDP) evoking a perception score of 1 or more, 5 or more, and 6 or more, respectively. The slope of the pressure–volume curve was used to quantify gastric compliance. Meal-induced gastric relaxation (accommodation) was quantified as the difference between the average volumes during 30 min before and 60 min after administration of the meal.
Dyspepsia symptom severity and measurement of weight loss
On the day of the study, the intensity of nine dyspeptic symptoms was scored on a Likert scale (range 0–3 (absent, mild, moderate, severe)), as previously reported.6–8 DSS is defined as the sum of all nine items.26 Body weight and weight loss since the onset of dyspepsia symptoms as well as duration of symptoms were determined previously at the outpatient clinic.
Measurements of psychosocial factors and psychiatric disorders
The following validated self-report questionnaires were completed on the day of the study.
Depression
The depression module of the Patient Health Questionnaire (PHQ-9) was used to screen for depressive co-morbidity.27 28 Depression score was used as a continuous variable.
Anxiety disorders
The anxiety disorder module of the PHQ was completed, allowing a diagnosis of the current Diagnostic and Statistical Manual IV (DSM-IV) panic disorder and other anxiety disorders in a categorical (yes/no) way using the algorithm described previously.28–30
Positive and negative affect
Positive and negative affect (PA and NA) are two independent, distinctive measures of mood.31 PA reflects enthusiasm, activity and energy, and alertness, whereas NA is a general dimension of subjective distress and unpleasurable engagement.31 NA has received considerable attention in the literature concerning FSS, but lack of PA may be equally important, although it is relatively neglected.17 32 Moreover, patients with FD may have lower PA but not higher NA compared to the general population.33 The Positive and Negative Affect Schedule (PANAS), consisting of two 10-item mood scales measuring PA and NA over the previous 2 weeks, was used in this study.31
Perceived stress
To measure perceived stress over the past month, the recent version of the 30-item Perceived Stress Questionnaire (PSQ) was used. This instrument has been shown to be reliable and valid in a population of patients with GI disorders.34
Alexithymia
Alexithymia is a psychological trait consisting of three dimensions: (1) difficulty identifying feelings and distinguishing between feelings and bodily sensations (DIF); (2) difficulty describing feelings (DDF); and (3) externally oriented thinking (EOT).35 36 Alexithymia, particularly its DIF dimension, may play an important role in FSSs, including FD.17 35 37 38 In this study, the well-validated, reliable and widely used 20-item Toronto Alexithymia Scale (TAS-20) was used to assess alexithymia.36
History of abuse
A history of childhood sexual, physical or psychological abuse plays an important role in the onset and course of psychiatric disorders, FSS and their complex interplay.39 This study used the sexual and physical abuse questionnaire developed by Leserman et al,39 and validated in a population with GI disorders. A screening question from a previously validated psychological abuse measure was added.7 40
Measurements of somatisation
Somatisation
The PHQ somatoform disorder module (PHQ-15) is a self-report questionnaire composed of 15 somatic symptoms, including 14 of the 15 most prevalent DSM-IV somatisation disorder criteria.41 42 All items are rated on a Likert scale (0 to 2). The PHQ-15 has high internal reliability and convergent and discriminant validity.41
To avoid overlap with other measures in this study, we did not take into account the two depressive items and the three GI symptoms included in the PHQ-15. Thus, the somatisation score we used is the sum of the remaining 10 items (PHQ-10). Current somatisation (past month) was measured. It should be noted, however, that this abbreviated version is not a validated instrument, which provides a limitation of the data on somatisation.
Moreover, a limitation of the PHQ-15 as a self-report measure (without interview) is that it cannot distinguish between “medically explained” and “unexplained” symptoms,41 which is an important feature of the somatisation concept.22 43 In this study, adequate clinical and technical investigations were performed to rule out a medical explanation of GI symptoms, but not systematically of other somatic symptoms as included in the PHQ-15, although major non-GI medical co-morbidity that may account for these somatic symptoms was ruled out on an “as needed” basis. Nevertheless, it should be emphasised that the PHQ symptom count in this study can only be characterised as indicative of somatisation. However, total self-reported PHQ somatic symptom counts are highly associated with physician-rated somatoform disorder symptom counts.41 44 Furthermore, the distinction between medically explained and unexplained symptoms may be problematic and less relevant than previously thought.23 45–49 Indeed, it may be important to take biological, psychological and social factors into account to adequately explain all bodily symptoms. Even when detailed medical records are available, deciding whether reported symptoms are adequately explained by medical findings has proven very difficult.23 49 Finally, the number of physical symptoms as such, whether medically explained or not, is associated with impairment, health care seeking and outcome, independent of psychiatric co-morbidity.46 48
Irritable bowel syndrome
Irritable bowel syndrome (IBS) was assessed with a previously used 10-item yes/no self-report questionnaire assessing the Rome II criteria for IBS.7
Statistical analysis
SAS 9.1.3 was used. Data are presented as median (interquartile range (IQR)) (most variables not normally distributed). If a certain variable(s) was (were) missing for a patient, this patient was excluded from all analyses in which the missing variable(s) was (were) used.
First, univariate association measures between DSS and weight loss on the one hand and gastric sensorimotor variables, psychosocial variables and somatisation variables on the other were calculated using Spearman’s correlation (ρ) and non-parametric one-way ANOVA.
Second, two different linear regression models were built with DSS and weight loss as the dependent variables. Gastric sensorimotor variables, psychosocial variables and somatisation variables that were univariately associated with the dependent variable (p<0.05) were entered into the regression model as independent variables in a hierarchical way. In step 0, sociodemographic variables (age, gender, marital status, education, occupation) were controlled for when appropriate. Gastric sensorimotor variables were entered in step 1, psychosocial variables in step 2 and somatisation variables in step 3, allowing detection of potential mediating effects. After entering the variables from one step together, backward elimination of nonsignificant variables that were entered in that step was performed. Tolerances were calculated for each independent variable to detect multicollinearity.
RESULTS
Patient characteristics
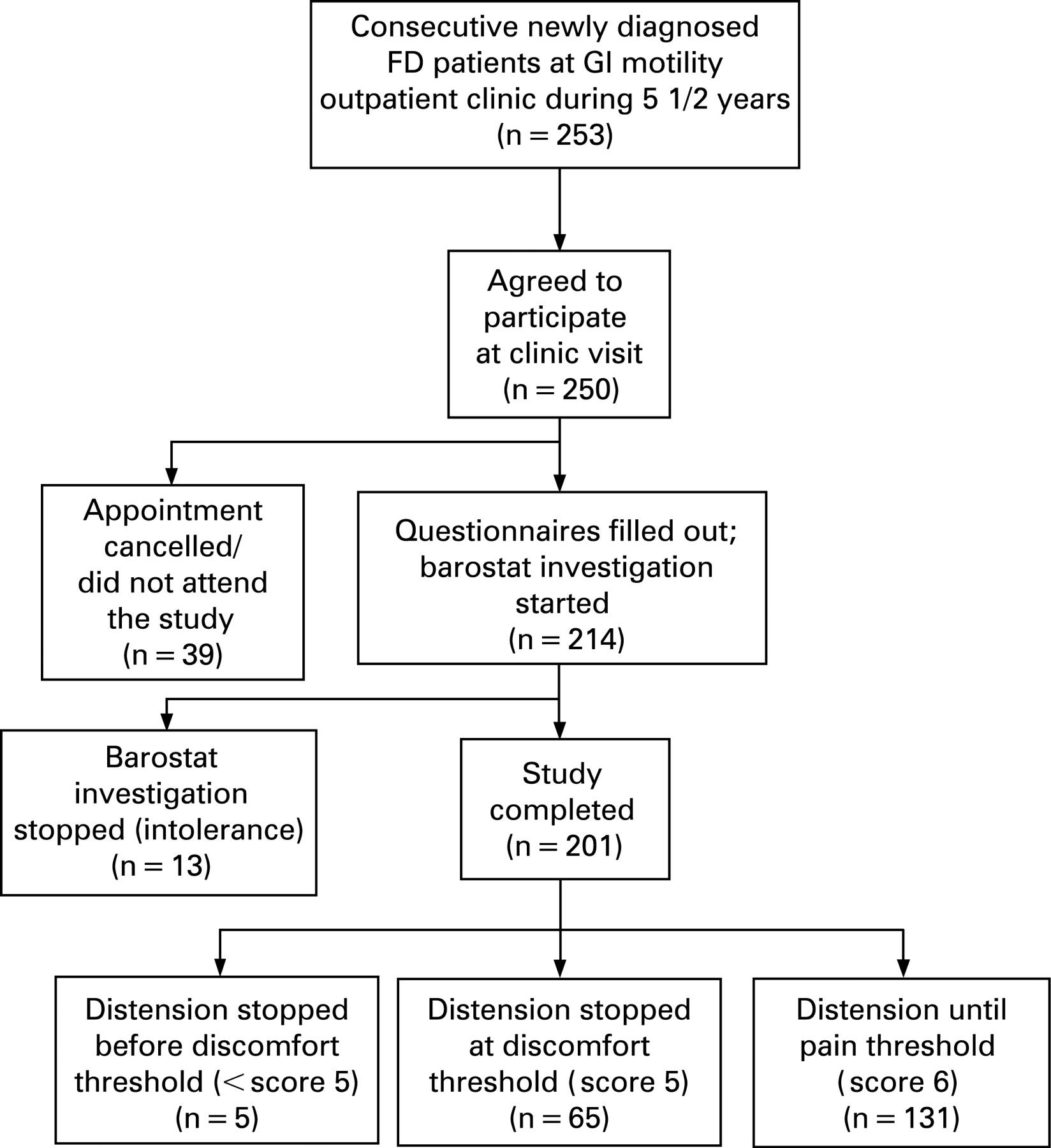
Two hundred and fifty-three patients with FD were asked to participate after being diagnosed with FD at the GI outpatient clinic. There were no refusals to participate at the clinic visit. Thirty-nine patients cancelled their study visit or did not attend, allowing 214 barostat investigations to be performed. In 13 patients, the procedure had to be stopped prematurely as they could not tolerate insertion of the tube or had severe discomfort once the tube was inserted. Two hundred and one patients completed the study (fig 1). One hundred and fifty patients (75%) were women. Table 1 shows relevant patient characteristics. Seventy-nine patients (39%) were hypersensitive to gastric distension. Seventy-one patients (35%) had depression scores ⩾10 (optimal cut-off).27
Univariate associations
Dyspepsia symptom severity
Whole patient group
Univariate correlates are shown in table 2. DSS is associated with several gastric sensorimotor function variables, but associations with depression, fatigue and somatisation are stronger.
Subgroup analyses
In normosensitive patients, DSS is significantly associated with age (ρ = −0.24, p = 0.008), occupation (F = 2.76, p = 0.008), gastric perception threshold (ρ = −0.19, p = 0.04), and with depression (ρ = 0.25, p = 0.007), positive affect (ρ = −0.19, p = 0.05) and somatisation (ρ = 0.32, p = 0.0005).
In hypersensitive patients, DSS is not significantly associated with sociodemographics or gastric sensorimotor function. Significant associations were found with depression (ρ = 0.25, p = 0.01) and somatisation (ρ = 0.48, p<0.0001).
Weight loss
Whole patient group
Univariate correlates are shown in table 3. Gastric sensitivity is the only sensorimotor function variable associated with weight loss. The associations with psychosocial factors (depression, PA, abuse history) and somatisation variables are stronger.
Subgroup analyses
In normosensitive patients, weight loss is significantly associated with gender (F = 5.81, p = 0.01), education (F = 2.1, p = 0.05), occupation (F = 2.5, p = 0.02), pain threshold (ρ = 0.25, p = 0.05), compliance (ρ = −0.21, p = 0.04) and accommodation (ρ = −0.20, p = 0.05), but more strongly with depression (ρ = 0.32, p = 0.001) and somatisation (ρ = 0.31, p = 0.002).
In hypersensitive patients, weight loss is significantly correlated with age (ρ = 0.25, p = 0.05), occupation (F = 4.35, p = 0.002) and compliance (ρ = 0.25, p = 0.05), but more strongly with overall/childhood sexual abuse history (F = 5.4, p = 0.02 and F = 10.4, p = 0.002, respectively), and somatisation (ρ = 0.47, p = 0.0001).
Multiple regression
Dyspepsia symptom severity
Whole patient group
The results are summarised in table 4. Somatisation and depression are the most important determinants of DSS (controlling for age and occupation). Gastric sensitivity is a significant independent determinant of DSS only before somatisation is entered into the model.
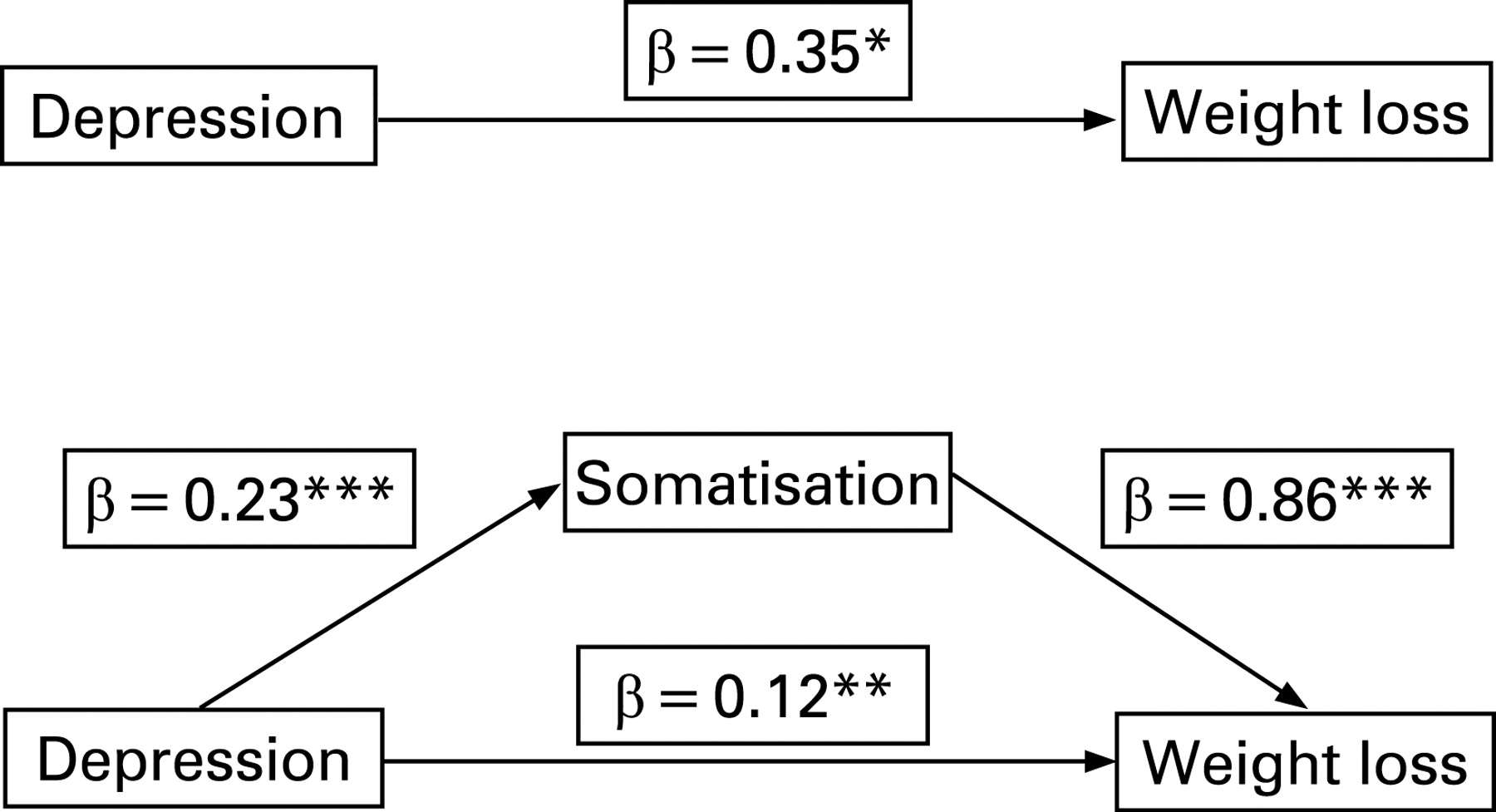
Entering somatisation reduced the regression coefficient for depression to borderline significance, indicating that somatisation may be a partial mediator of the effect of depression on DSS.50 To test this mediation hypothesis further, a regression model with somatisation as the dependent variable and depression as the independent variable was estimated.50 This showed that depression is a significant predictor of somatisation, confirming the mediation hypothesis (fig 2).

Subgroup analyses
In normosensitive patients, the final model (controlling for age and occupation, R2 = 0.26, p<0.0001) includes depression (β = 0.09 (SD 0.07), p = 0.22) and somatisation (β = 0.23 (SD 0.11), p = 0.05). The effect of depression is fully mediated by somatisation. No gastric sensorimotor function variable reached significance.
In hypersensitive patients, a similar model was obtained (controlling for occupation, R2 = 0.41, p<0.0001), including depression (β = 0.08 (SD 0.11), p = 0.47) and somatisation (β = 0.83 (SD 0.16), p<0.0001). The effect of depression is again fully mediated by somatisation. Compared to normosensitive patients, the effect of somatisation is more significant in hypersensitive patients, and the amount of variance explained is higher.
Weight loss
Whole patient group
The results are summarised in table 5. Sexual abuse in childhood and somatisation are the most important determinants of weight loss; the effects of gastric sensitivity and occupation are borderline significance in the full model. Entering somatisation reduced the regression coefficient for depression to non-significance, indicating that depression no longer has a significant direct effect on weight loss when somatisation is controlled for (full mediation) (fig 3).
{kind=link}
{kind=link}
{kind=link}
Subgroup analyses
In normosensitive patients, the final model (controlling for gender (p = 0.05) and education (p = 0.02), R2 = 0.33, p<0.0001) includes accommodation (β = −0.01 (SD 0.005), p = 0.01), depression (β = 0.25 (SD 0.14), p = 0.08) and somatisation (β = 0.44 (SD 0.22), p = 0.05). The effect of depression is partially mediated by somatisation.
In hypersensitive patients, the final model (controlling for age and occupation (p = 0.03), R2 = 0.54, p<0.0001) includes overall childhood abuse (β = 7.6 (SD 3.6), reference category = no abuse, p = 0.04) and somatisation (β = 1.05 (SD 0.47), p = 0.03).
DISCUSSION
To the best of our knowledge, the relative contribution of gastric sensorimotor function, psychosocial factors and somatisation to FD symptoms and weight loss has not been assessed in a single study before. In the whole patient group of the present study, gastric sensitivity, but no other gastric sensorimotor variable, is associated with FD symptoms and weight loss. Psychosocial factors (depression, PA) and somatisation are more strongly associated with DSS and weight loss. Using multiple regression, gastric sensitivity is no longer an independent determinant of DSS after somatisation is entered in the model. Somatisation is the most important determinant of symptom severity and weight loss in FD; the effect of depression is mediated by somatisation. Separate analyses of normosensitive and hypersensitive subgroups show that gastric sensorimotor function may be somewhat more important in normosensitive patients, although only the effect of accommodation on weight loss was significant in multiple regression. In hypersensitive patients, their effect is very limited, even in univariate analysis, whereas the effect of somatisation and history of abuse is stronger.
Several findings of this study are in line with previously published work. First, the previously reported association between hypersensitivity to gastric distension and FD symptoms6 7 was confirmed, although weaker compared to the association with depression and somatisation. Second, dyspeptic symptom scores were shown to correlate with general psychiatric distress as well as with somatisation and depression in two recently published studies.15 18 In a recent community-based study, dyspepsia symptoms were associated with general psychiatric distress and somatisation but not with gastric sensorimotor dysfunction (accommodation, emptying).12 However, in these studies, correlational analyses rather than multiple regression models were used. Third, the stronger association with psychosocial factors and somatisation in hypersensitive patients is in line with previous findings by our group.25
In the present study, somatisation was the most important determinant of FD symptoms and weight loss, even when sociodemographic, gastric sensorimotor and psychosocial variables were controlled for. Co-morbid IBS, however, was not associated with DSS or weight loss, in uni- or multivariate analysis. The concept of somatisation is, although clinically very important, problematic and ambiguous.22 It is important to note that, given the nature of the somatisation measure used in this study, the PHQ-10 somatisation scores can only be seen as indicative of functional somatisation. In other words, the somatisation scores in this study only provide a continuous measure of the number and severity of somatic symptoms reported by a patient, without firm implications for the possible biopsychosocial processes underlying this phenomenon.22 41 48
Determining the processes underlying somatisation falls beyond the scope of this study, but is an important question in FSS research. There is growing evidence for a multidimensional model of somatisation, in which all these dimensions interact in a complex reciprocal way.20 23 49 51 First, sociocultural reinforcement and modelling may be important, as well as maladaptive stress coping and illness cognition or symptom attribution.20 51 Second, several personality traits have been associated with somatisation, including alexithymia, especially its DIF dimension.35 Third, central pain amplification may play a key role in somatisation. There is growing evidence about the influence of cognition and emotion on central pain processing, and thus on reporting of painful physical symptoms.51–53 Arousal, anticipation, attention to bodily sensations and different forms of anxiety (including anxiety sensitivity, fear of pain and visceral-specific anxiety) may all highly interact with central pain processing systems in health and disease.14 53 54 Knowledge about putative neurobiological mechanisms underlying these processes is growing.51–53 55
Finally, it has long been hypothesised that depression and somatisation are closely related and frequently overlapping, but not identical, entities;43 56 recent epidemiological9 as well as neurobiological evidence supports this hypothesis. Both in a recent literature review, as in a recently published large epidemiological study, somatic pain symptoms were highly prevalent in depressive patients, independent of co-morbid “somatic” diagnosis.57 58 Conversely, co-morbidity with anxiety and depression in FSS/somatoform disorders is high.9 Moreover, depression as well as FSS/somatoform disorders have repeatedly been associated with a history of trauma or abuse as well as with other psychosocial stressors.39 59 Neurobiological support for the reported association between depression and somatisation is growing. Feedback from the body to the brain is believed to be important in mood regulation and brain regions processing bodily signals have been shown to play a key role in normal mood regulation as well as depression.60 61 This leads to the hypothesis that “alarm systems” for physical and psychological pain or stress are closely linked throughout evolution and share neurobiological mechanisms.62 Futhermore, neurotransmitters including serotonin and noradrenaline and dysfunction of the hypothalamic–pituitary–adrenal axis play an important role in depression as well as FSS/somatoform disorders.52 63 The finding in the present study that depression is a determinant of FD symptoms, but that its effect is partially mediated by somatisation, is in line with the evidence outlined above. However, clarifying the biopsychosocial mechanisms underlying these associations falls beyond the scope of this study.
There are several important limitations of this study that should be addressed. First, we only used self-report measures, which may be prone to certain forms of bias. For example, relating a history of abuse may be prone to recall bias and the results may be confounded by present depressive symptoms.64 However, the abuse measures we used are reliable and valid, specifically in populations with functional GI disorders65 and have been widely used. The specific problems regarding self-report measures of somatisation have already been adressed in the materials and methods section, as this is an important issue for understanding the concept of “somatisation” as used throughout this article. In general, although a structured clinical interview remains the “gold standard” that is clearly superior to self-report measures for diagnosing psychiatric co-morbidity, we carefully chose self-report measures, most of which have been validated with a structured interview as a comparison.
Second, this is a cross-sectional study, permitting conclusions about associations but not about causal or temporal relationships between the variables studied. For example, it cannot be determined whether the onset of depressive symptoms precedes the onset of somatic symptom reporting or vice versa. These results should therefore be interpreted with sufficient caution and require replication in longitudinal studies before any definite conclusions can be drawn. Given the lack of such studies at this moment, however, we feel that these results provide important, although limited evidence about the relative contribution of gastric sensorimotor function, psychosocial factors and somatisation in FD symptom generation.
Third, the patient population consists of tertiary care patients with FD, limiting generalisability of the results towards other populations of patients with FD. The gender distribution (75% women) is high compared to the lack of female predominance in FD,66 but in line with previous publications by our group.7 25 However, the ratio of women to men is typically higher in tertiary care patients.67 As patients were recruited consecutively, they reflect the average tertiary care patients with FD seen in our clinic and were therefore heterogeneous in terms of onset and course of illness, psychiatric co-morbidity, previous medication use, for example.
Fourth, some of the associations are relatively weak. For example, despite a quite extensive psychological and physiological characterisation of a large patient sample, the final model was only found to explain 29% of the variance in DSS. We therefore believe it is important to characterise patients with FD even more extensively in future, longitudinal studies. Autonomic nervous system68 and stress hormone measurements69 as well as psycho-physiological measures of arousal, hypervigilance or symptom-specific anxiety70 and behavioural measures of stress coping, illness cognition and symptom attribution could be potentially useful in this respect.
Finally, we believe it should be emphasised that the results of this study, in our opinion, do not necessarily imply that symptom generation/reporting in FD is mainly or purely psychological rather than somatic in origin, given the second limitation of the study stated above and the growing knowledge of neurobiological processes underlying psychological phenomena including depression. We believe, however, that this study provides another piece of evidence in favour of a biopsychosocial model of FSS in general and hypersensitive FD in particular.
REFERENCES
Footnotes
See Commentary, p 1642
Funding: LVO is a research fellow and JT is a clinical researcher of the Research Foundation–Flanders (FWO–Vlaanderen). This study was funded by a grant from the Research Foundation–Flanders to JT.
Competing interests: None.
Ethics approval: Approval for this study was given by the Medical Ethics Committee of the University Hospital Leuven, in 2001.