Article Text

Abstract
Background Previous studies have shown that aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) lower colorectal cancer (CRC) risk. However, the lowest effective NSAID dose, treatment duration, and effects on survival are not defined. In a large population-based case–control study, we have explored the relationship between NSAID dose and duration, CRC risk and overall CRC-specific survival.
Methods The relationship between NSAID use and CRC risk was examined in 2279 cases and 2907 controls. Subjects completed food-frequency and lifestyle questionnaires. NSAID categories were low-dose aspirin (75 mg), non-aspirin NSAIDs (NA-NSAIDs) and any NSAID. Users were defined as taking >4 tablets/week for >1 month. ORs were calculated by logistic regression models and adjusted for potential confounding factors. Effect of NSAID use on all-cause and CRC-specific mortality was estimated using Logrank tests and Cox's hazard models.
Results In all, 354 cases (15.5%) were taking low-dose aspirin compared to 526 controls (18.1%). Low-dose aspirin use was associated with decreased CRC risk (OR 0.78 95% CI 0.65 to 0.92, p=0.004), evident after 1 year and increasing with duration of use (ptrend=0.004). NA-NSAID and any NSAID use were also inversely associated with CRC. There was no demonstrable effect of NSAIDS on all-cause (HR 1.11, p=0.22, 0.94–1.33) or CRC-specific survival (HR 1.01, p=0.93, 0.83–1.23).
Conclusion This is the first study to demonstrate a protective effect against CRC associated with the lowest dose of aspirin (75 mg per day) after only 5 years use in the general population. NSAID use prior to CRC diagnosis does not influence survival from the disease.
- Colorectal cancer
- aspirin
- NSAIDs
- chemoprevention
- cancer prevention
- non-steroidal anti-inflammatory drugs
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Epidemiological studies show aspirin and other NSAIDs reduce colorectal cancer incidence by ∼40%
Four randomised controlled trials demonstrate aspirin decreases incidence of colorectal cancer pre-cursor lesions, adenomas
The dose and duration of aspirin /other NSAID intake remains undefined
What are the new findings?
The lowest daily dose of aspirin, 75 mg, reduces the incidence of colorectal cancer
The reduction in colorectal cancer incidence is evident after only 5 years' use
The protective effect is apparent in the general population and not just in high-risk groups
How might it impact on clinical practice in the foreseeable future?
These findings will aid design of future large scale chemoprevention trials
Introduction
Colorectal cancer (CRC) is ranked second as a cause of cancer mortality with 492 000 deaths per annum worldwide. Scotland is a high-incidence country, with an average of 3465 registrations annually (2001–2005), while CRC is the second commonest fatal cancer.1 Complementary approaches are required to improve survival, including early detection and incidence reduction through population and high-risk group screening. However, screening programmes are costly which may limit implementation in all healthcare systems.2 3 Survival could also be improved indirectly by preventive interventions, such as chemoprevention. This is particularly relevant to high-risk groups, such as those with genetic predisposition and with previous CRC. Chemoprevention, as an adjunct to colonoscopy surveillance in post-polypectomy patients, may be more cost-effective than surveillance alone.4
Evidence from epidemiological studies, clinical trials, and experimental studies suggests that NSAIDs protect against CRC. Observational studies have shown aspirin and other NSAID intake is associated with a reduction in risk of both colorectal adenomas and carcinomas.5 6 Although considerable heterogeneity exists within and between studies, the magnitude of the effect is remarkably consistent, despite differing NSAIDs, dosing regimens, duration of use, study populations and geographical locations.
These observational studies are further supported by four randomised controlled trials (RCTs) demonstrating that aspirin reduces colorectal adenoma risk in both average and high-risk populations.7–10 One trial was terminated early due to the magnitude of aspirin's protective effect compared to placebo.9 RCT meta-analysis confirms the striking protective effect against adenomas with low daily doses of aspirin (81 mg to 325 mg), which are similar to those used for cardiovascular protection.11 However, the majority of adenomas do not progress to cancer, and hence these data may not reflect NSAID activity against CRC.
Two RCTs, the Physicians' Health Study and the Women's Health Study, did not show a reduction in CRC incidence in average-risk individuals.12 13 However, these studies were conducted in healthcare professionals and are not representative of the population. The Physicians' Health Study also had a lower than average CRC incidence compared to the general population and subjects were not known to be free of colorectal neoplasia at enrolment. Furthermore, a recent RCT in high-risk individuals did not detect a protective effect of aspirin (27 months use) after 2.2 years follow-up.14 However, duration of aspirin use or follow-up may be insufficient to detect differences in colorectal neoplasia development. Further trial data with longer follow-up are awaited. Indeed, Flossman examined two aspirin RCTs with cardiovascular primary endpoints and found that aspirin did reduce CRC incidence after 5 years use and with a latency of 10 years.6
Despite considerable evidence of a protective effect of NSAIDs in colorectal neoplasia, the US Preventive Services Task Force (USPTF) has not recommended aspirin for primary chemoprevention.5 The USPTF concluded that questions remain regarding the most effective dose, duration of intake and start age. Indeed, the minimal dose to prevent adenomas and CRC is yet to be established. Data have been limited on whether NSAID use reduces CRC mortality. One large cohort study suggested a reduction in mortality when aspirin was used for more than 15 years.15 16
A recent international consensus statement has called for studies to define the lowest effective dose of NSAID, treatment duration, age to commencement and identification of population subgroups where the risk/benefit ratio is optimised.17 Here, we present the results of a large population-based case–control study in which we have conducted a detailed exploration of these issues. We aimed to investigate the primary hypothesis that aspirin and other NSAIDs reduce the incidence of CRC and to determine whether NSAID use prior to diagnosis of CRC influences survival.
Methods
Design and participants
The study included 2254 cases and 2907 controls from a population-based case–control study of CRC (Study of Colorectal Cancer in Scotland, SOCCS). SOCCS aimed to recruit prospectively all incident CRC cases aged 16–79 presenting to surgical units in Scotland. Exclusion criteria were death prior to ascertainment, inability to consent or complete questionnaires. Ascertainment bias was minimised by research staff maintaining contact with CRC nurse specialists in Scotland-wide surgical centres. Recruitment was completed within 2–3 months of diagnosis to limit survival bias. We recruited ∼45% of all incident cases in Scotland over the study period. During the same period controls were randomly drawn from a population-based register. Cases and controls were matched on age (±1 years), gender and residential area. Participation rates were 52% for cases and 39% for controls and questionnaires were completed sufficiently to permit analysis by 82% of cases and 97% of controls. Approval was granted by the Multicentre Research Ethics Committee, 18 Local Research Ethics committees, 18 Caldicott guardians and 16 NHS trust management committees. All participants provided written informed consent.
Assessment of lifestyle and NSAID data
Subjects completed a lifestyle and cancer information questionnaire reporting their status 1 year prior to diagnosis (for cases) or recruitment (for controls). Medical history, physical activity, smoking status, height, weight and waist circumference were recorded. Participants reported demographic, socioeconomic and ethnicity data. Women stated menstrual and reproductive history, hormone replacement and contraception use.
Subjects reported intake of aspirin, other NSAIDs and analgesics. Specific indication(s) for NSAID use were not recorded. Individuals reporting regular drug use stated the date of drug commencement, number of months and number of days per week ingested. We did not have information on aspirin or other NSAID intake after cases were diagnosed with CRC.
Dietary assessment
A semi-quantitative food frequency questionnaire was administered (Scottish Collaborative Group FFQ, Version 6.41. http://www.foodfrequency.org). The validity for ranking nutrients has been described.18 Consumption frequency of specified food measures was converted into nutrients using a programme based on weight and nutrient composition of representative foods derived from the UK food composition tables (McCance and Widdowson's The Composition of Foods, 6th summary edition). Supplement nutrient information was collected from manufacturers' information. Quality of questionnaire completion was checked weekly. Inadequately completed forms were not analysed.
Tumour staging data
A total of 3334 of the 3476 (95.9%) tumours were assigned an AJCC stage derived from a synthesis of clinical, pathological and imaging information. Staging involved contact with individual patient general practitioners and surgeons, radiology and pathology departments, as well as each of the managed clinical networks throughout Scotland.
Data used for survival analysis
Up to the censoring date (30 April 2008), there were 1170 deaths in the 3417 recruited cases. Cause of death was determined by examining all death certificates in blinded manner with respect to NSAID use. There were 1023 deaths of the 1170 due to CRC (84% of all deaths). Data on the initial date of diagnosis termed incidence date was available for 3399 cases. Information regarding NSAID intake was completed to an appropriate level for analysis in 676 of the cases that died out of the 1170 (57.8%).
Statistical analysis
The statistical package used was Intercooled STATA version 10.0 (Stata Corp). The Pearson χ2 test was used to test the difference between cases and controls in terms of gender, smoking, NSAIDs intake, physical activity and Carstairs Deprivation Index. The t-test was used to test differences in mean age, body mass index (BMI), total energy, fibre and alcohol intake. Logistic regression models were used to estimate the strength of association between NSAID categories and CRC risk. Logrank tests and Cox's hazard models estimated NSAID effects on all-cause and CRC-specific mortality.
Meta-analysis
A systematic review was performed to identify case–control and cohort studies that reported the relationship between low doses of aspirin and CRC. Medline and ISI Web of Knowledge databases were searched using the keywords colorectal cancer and aspirin, with limits set to English articles from 1980 to 2010. In addition, relevant studies were identified by searching the references of selected studies. ‘Low dose’ of aspirin was defined as less than or equal to 165 mg of aspirin taken daily. Eligible studies were selected according to pre-determined inclusion criteria. In particular, criteria to be fulfilled were (1) studies that measured CRC incidence; (2) the strength of association had to be stated in the form of RR or OR; and (3) the study population had to be comparable with the general population. The title and abstract of studies identified were scanned to exclude any that were irrelevant. Each article was then systematically reviewed against inclusion criteria.
Meta-analysis of the cohort and case–control studies was conducted and pooled estimates with corresponding 95% CI were reported using the fixed effect model (Mantel–Haenszel method). In case of heterogeneity (p Value<0.1) the random effect model (DerSimonian–Laird method) was applied. Meta-analysis was conducted using STATA 10.0 statistical software.
Results
Demographic data of study population and drug categories
The cases were matched to controls for age, gender and area of residence. There were no differences in baseline characteristics such as gender, deprivation category, smoking, alcohol and fibre intake (table 1). As expected more cases had positive family history of CRC. Cases engaged in less physical activity and had a higher dietary energy intake compared to controls. There was no significant difference in BMI.
Summary statistics of potential confounding factors
NSAID ingestion and colorectal cancer risk
There was a lower risk of CRC in users of any NSAID compared to non-users (table 2). The risk reduction remained significant after adjusting for confounding factors, including age, energy intake, physical activity, smoking, total fibre, alcohol intake, gender, BMI and deprivation index. The effect was then examined in the different drug categories. CRC risk was reduced in subjects on 75 mg aspirin, non-aspirin (NA) NSAIDs and those ingesting both 75 mg aspirin and NA-NSAIDs (table 2). The overall reduction in risk for any NSAID was similar for colon and rectal cancer (colon OR 0.72, p=0.00006, 95% CI 0.62 to 0.85; rectal OR 0.73, p=0.0001, 95% CI 0.61 to 0.88).
Non-steroidal anti-inflammatory drug (NSAID) intake variables and the risk of colorectal cancer: crude and adjusted ORs (95% CI) in the whole sample from logistic regression models
We examined the reduction in CRC risk stratified by AJCC disease stage (supplementary table 1). To summarise, the reduction in CRC risk was similar between early (AJCC 1 and 2) and later stage (AJCC 3 and 4) disease. In addition, the association between duration of NSAID use and CRC risk was considered. There was a reduction in AJCC 1 and 2 after 1–3 years' ingestion and in AJCC stage 3 and 4 after 5–10 years' intake.
Effect of dose on CRC risk
There was evidence of a dose-dependent effect of aspirin on CRC risk with the greatest risk reduction in those consuming >525 mg aspirin per week (equivalent to more than 75 mg of aspirin/day) (OR 0.66, 95% CI 0.41 to 1.05) (table 2). However, the protective effect was present even for the lowest daily dose (75 mg) of aspirin (OR 0.79, 95% CI 0.66 to 0.95). Indeed, doubling the aspirin dose did not lead to proportionate reduction in CRC risk. This might suggest that the lowest dose of aspirin is effective. However, the dose-dependency is difficult to interpret, since the participant number taking two or more 75 mg tablets daily is small. Regular users of NA-NSAIDs had a lower risk of CRC (OR 0.74, 95% CI 0.6 to 0.9). This risk reduction was even greater in patients who were on both 75 mg aspirin and NA-NSAIDs (OR 0.47, 95% CI 0.31 to 0.7).
Effect of duration of NSAID intake on CRC risk
There was an inverse association between CRC and duration of use, which increased with duration of use, up to 10 years with low-dose aspirin, NA-NSAIDs and the ‘any NSAID’ categories (table 2). However, there was a modest risk reduction in users of both 75 mg aspirin and NA-NSAIDs even after 1 year of use (OR 0.87, 95% CI 0.59 to 1.28; OR 0.79, 95% CI 0.6 to 1.03). The cumulative dose, accounting for both dose (75 mg aspirin) and duration of intake, is calculated in tablet-years. One-tablet year is defined as one 75 mg aspirin tablet per day for 1 year. Cumulative dose analysis confirmed a reduction in CRC risk after 5 years of consistent use (table 2). We also considered whether the protective effect of NSAIDs may be related to analgesic effects and found no CRC risk reduction in users of other analgesics (supplementary table 2).
The association between NSAIDS and CRC was examined after gender stratification (supplementary table 3). The inverse association between 75 mg aspirin and CRC, including the duration of intake and cumulative dose effects, were observed in both genders but was statistically significant only in males. This may be a reflection of more men being on 75 mg aspirin for cardiovascular protection.19 There was evidence of a dose-dependent reduction in CRC risk with aspirin in both genders. The inverse association between NA-NSAIDs and CRC was statistically significant only in females. There was a greater reduction in OR in those on both 75 mg aspirin and NA-NSAIDs.
Summary statistics of the confounding factors in survivors and non-survivors (n=2259, excluding 16 cases with no incidence date and four cases with incidence dates before 1 January 1998)
Meta-analysis of low-dose aspirin studies
We systematically reviewed published cohort and case–control studies specifically reporting the relationship between low dose aspirin and CRC (figure 1). We identified 548 titles from the search conducted. After elimination of studies with alternative end-points, and studies which did not fit the inclusion criteria, six cohort and three case–control studies were identified (supplementary figure 1).20–28 The pooled risk ratios for the cohort studies based on a fixed effects model (p for heterogeneity p=0.44) showed a modest reduction in CRC incidence (RR (95% CI): 0.9 (0.9, 1.09)) (figure 1). Meta-analysis, based on a random effects model (p for heterogeneity 0.06), of data from the case–control studies and our data confirmed that low dose aspirin reduces CRC incidence (OR (95% CI): 0.81 (0.63, 1.04)) (figure 1).

Metanalysis of cohort studies (A) and case–control studies (B) examining effect of low doses of aspirin on colorectal cancer incidence.
NSAIDs, survival and death from colorectal cancer
Next, we investigated whether NSAID use prior to diagnosis was associated with a difference in survival in cases. There were a total of 2259 cases for analysis after the exclusion of 20 cases (incidence date issues), which had food, drug and lifestyle information available. There were 676 deaths within this group. We compared confounding factors between the deceased and survivors (table 3). There were no differences between gender, family history, physical activity, dietary energy, fibre and alcohol intake. As anticipated there were more deaths in the older age group, more deprived (deprivation categories 4–7), those with a greater BMI and smokers (table 3).
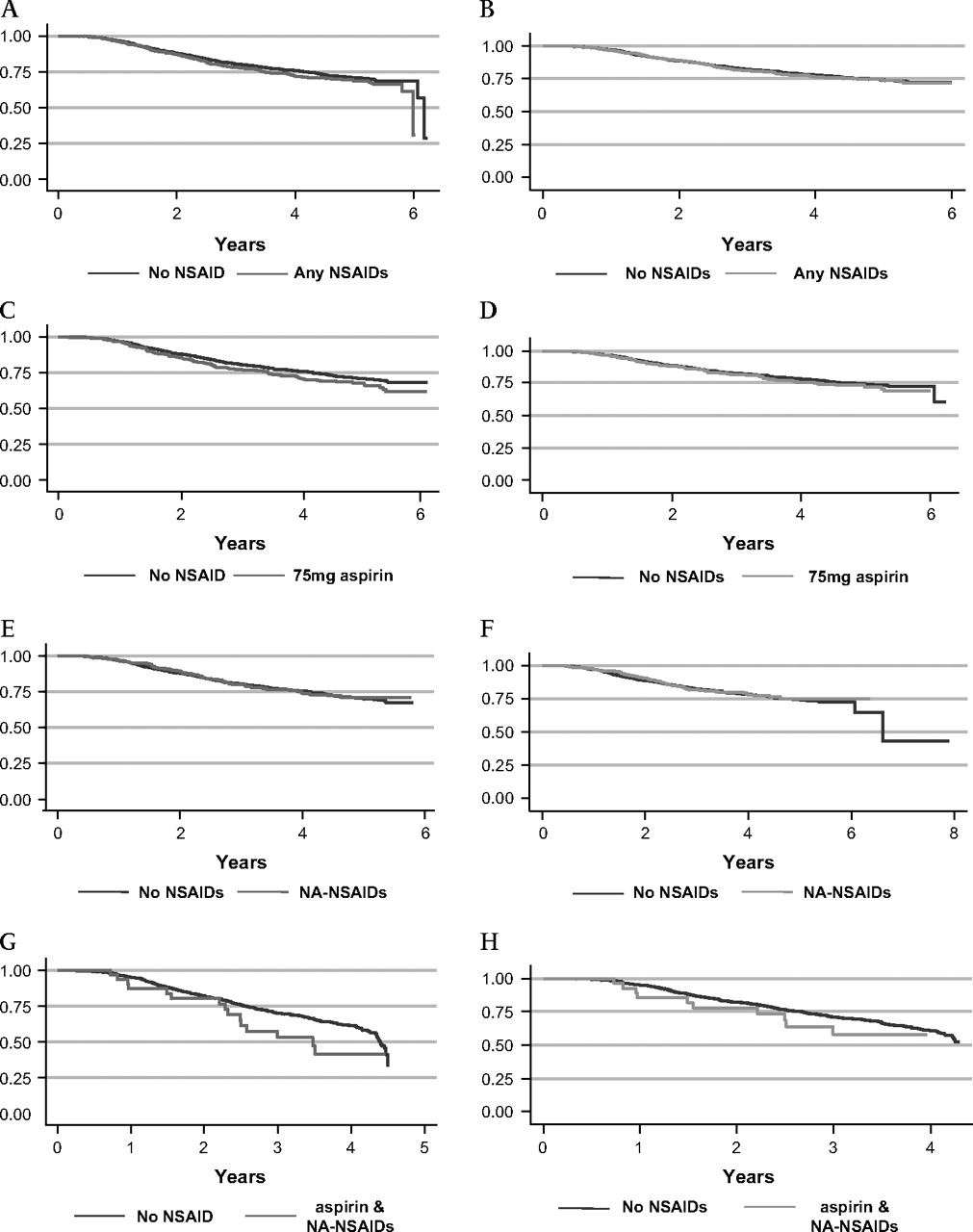
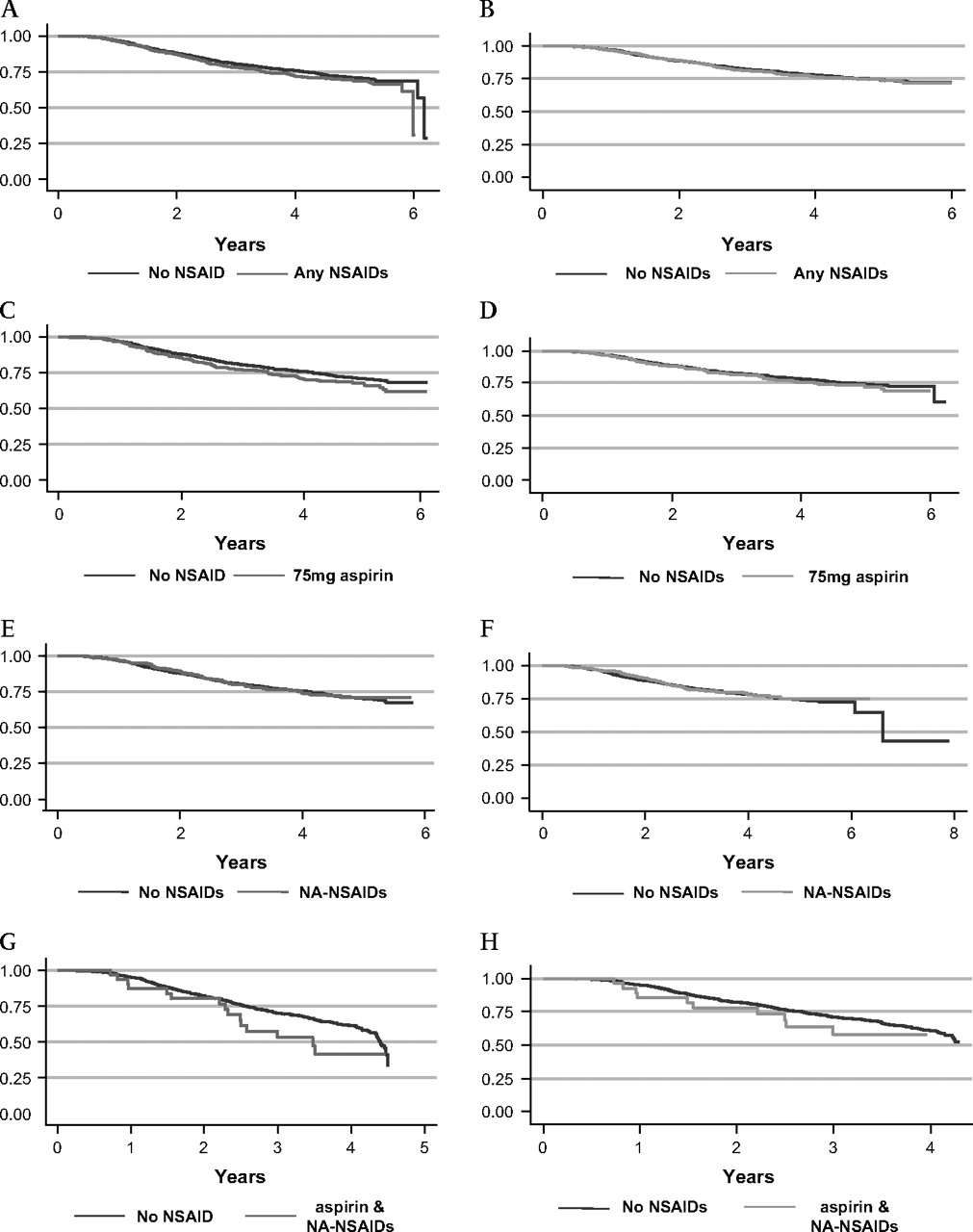
We found that there were no significant differences in all-cause and CRC-specific mortality in any drug categories when adjusted for age, gender, family history and AJCC stage (table 4, figure 2). We next examined the number of deaths that may have been due to NSAID-related complications. In the cases taking NSAIDs there were 224 deaths of which six may have related to NSAIDs; one bleed and five cerebrovascular accidents (CVAs). In the cases not taking NSAIDs, there were 486 deaths of which three deaths were due to bleeding and three due to CVAs. There was no difference between deaths due to bleeding (OR=0.36, 0.04–2.9, p=0.44) or CVAs (OR=3.68, 0.87 to 15.5, p=0.12) between NSAID users and non-users in CRC cases.
Survival analysis for all cause and colorectal cancer mortality by non-steroidal anti-inflammatory drug (NSAID) intake
{kind=link}
{kind=link}
Effect of non-steroidal anti-inflammatory drugs (NSAIDs) and overall and colorectal cancer (CRC)-specific mortality. Kaplan–Meier survival estimates of overall mortality (red line) and CRC-specific mortality (green line) for any NSAID (A,B), 75 mg aspirin (C,D), non-aspirin NSAIDs (E,F) and both aspirin and NA-NSAIDs (G,H).
Discussion
We show that aspirin and other NSAIDs are associated with a reduction in risk of CRC in the Scottish population of ∼30%. Furthermore, this study is the first to show that the effect is apparent after 5 years' use of daily low dose 75 mg aspirin, commonly used for cardiovascular protection. The magnitude of the protective effect increases with duration of use up to 10 years. Although we had a large, well-characterised incident case series with detailed staging information and 4.70 (IQR: 2.97, 5.74) years of actual follow-up, we did not detect any effect of aspirin or NSAIDs on CRC survival.
Our results showing decreased CRC incidence are consistent with previous studies examining NSAIDs and CRC incidence. The USPTF concluded that there was a 22% reduction in incidence in cohort studies and that three case–control studies showed a significant decrease in CRC risk (OR 0.3–0.7), while four case–control studies identified a trend that favoured aspirin-mediated reduction in CRC incidence.5 A meta-analysis of 19 case–control studies indicates that aspirin or NSAID use is associated with a reduced CRC risk (pooled HR 0.8, 95% CI 0.73 to 0.87).6 Flossman also concluded that there was a reduction in CRC incidence (pooled HR 0.74, 95% CI 0.56 to 0.97) in two large cardiovascular prevention RCTs. This contrasted previous RCT results from the Physicians' Health Study and the Women's Health Study and has been partially attributed to the higher aspirin doses used in the cardiovascular protection trials.12 13 29 Nonetheless, the available RCT data have not established the lowest effective dose imparting a significant protective effect. The key finding of our case–control study is that the daily 75 mg dose of aspirin is associated with a lower incidence of CRC in the general population. It is noteworthy that our results differ from the two RCTs which failed to show a reduction in CRC incidence.12 13 However, these studies had selected populations of healthcare professionals whereas our study reflects the population at large. Furthermore, it was not known at the time of enrolment whether the participants already had colorectal adenomas or cancer. Our data not only reflect the results from previous observational studies suggesting a protective effect but show that this can be achieved with low-dose aspirin.
Experimental and epidemiological data have suggested a dose-dependent effect with respect to NSAIDs and prevention of colorectal carcinogenesis. The adenoma RCTs with multiple aspirin doses failed to identify any dose-related effect as the higher aspirin dose did not appear to be protective.7 8 However, secondary analysis of the Baron study suggests that the higher aspirin dose is protective.30 In any case, it is not clear whether doses sufficient to prevent adenomas would prevent CRC. Two studies that examined specifically the dose relationship with CRC incidence did not find a significant association with 75 mg aspirin daily dose.26 27 Another recent cohort study suggested that 6–14 aspirin tablets per week (equivalent of 278–650 mg aspirin daily) were required to reduce CRC incidence.24 In contrast, we show that 75 mg aspirin (≤7.75 mg tablets/week) reduces CRC incidence. Although there is a trend towards a dose-dependent association with aspirin, it is not directly proportional to the dose. Indeed, the UK-TIA trial did not show evidence of a dose-dependent protective gradient against CRC, even comparing 1200 mg/day, with 300 mg/day and 75 mg/day.6 Although the meta-analysis result is not significant, given the CIs, it provides a useful review of the studies that have specifically examined low doses of aspirin and presents our results within the context of previous findings. Our data provide reassurance that lower doses of aspirin do provide worthwhile risk reduction effects.
There has been considerable debate regarding the optimum duration of NSAID use. Our results show that the risk reduction with the lowest dose of aspirin (75 mg daily) is evident as early as after 1 year of ingestion with the results becoming significant after 5 years' use. This is in contrast to previous data which suggested that a low dose (50-162 mg/day) for 5–10 years was inadequate for CRC prevention.24
Previous data suggested that a longer duration of intake was required for the risk reduction in later stage disease, perhaps indicating a greater effect at cancer initiation rather than progression.24 We found no significant difference in aspirin use from the group as a whole compared to each AJCC stage. However, we found that a longer duration of intake (AJCC 3 & 4; 5–≤10 years) of any NSAID was required for the risk reduction to be significant in the later stage disease compared to earlier stage disease (AJCC 1 & 2; 1–≤ 3 years). The adenoma RCT meta-analysis reported that aspirin's protective effects are present for advanced adenomas, more likely to progress to cancer, strengthening its chemopreventive role.11
There is differential gene expression between the colon and rectum.31 32 One study suggested that COX-2 expression is greater in the rectum compared to the colon.33 Combined data analysis from the Nurses' Health Study and the Health Professionals Follow-up Study (HPFS) suggests that aspirin reduces CRC incidence and increases survival in cancers over-expressing COX-2.34 35 Further analysis from the same group (HPFS only) alluded to a stronger effect of aspirin in the rectum compared to the colon but cautioned that the numbers were low.34 We found no differences between risk reductions dependent on CRC site. It has been reported BMI influences the protective effect of NSAIDs, with higher BMI groups displaying a greater risk reduction.36 We found no differences in CRC risk reduction when stratified by BMI or gender.
NSAIDs fulfil several criteria required of the ideal chemopreventive agent: effectiveness, convenient and inexpensive dosing schedule and ease of ingestion.37 However, NSAIDs are associated with an increase in haemorrhagic strokes and gastrointestinal complications such as peptic ulcers and bleeding. Hence, the risks of chemoprevention with NSAIDs outweigh benefits in low to moderate risk populations given the high dose and duration of intake required.5 The adenoma RCT meta-analysis found that there was no difference in the rates of death, myocardial infarction or major bleeding but that there was a significant increase in stroke rate.11 We examined the rate of fatal complications in CRC cases taking NSAIDs compared to cases not taking NSAIDs. We found no difference between the rates of fatal stroke and bleeding in the two groups although power to detect an effect may have been limited.
Few studies have examined the effect of NSAIDs on CRC mortality. Early epidemiological studies did show decreased CRC-specific mortality in NSAID users.15 16 The Women's Health Study showed no reduction in overall or cancer-specific mortality but this study did not identify a protective effect either.13 Another study showed an increase in all-cause mortality and no change in CRC-specific mortality.38 However, these studies did not examine overall and cancer-specific survival specifically once CRC has developed. We attempted to examine whether aspirin and other NSAID use influences survival after CRC diagnosis. We found no significant difference in all-cause or CRC-specific mortality. The lack of effect on survival may reflect sample size issues and the limited duration of intake. In particular, the Nurses' Health Study showed that decreases in CRC mortality became significant after 11–20 years of aspirin use.39 This study showed a non-statistically significant decrease in CRC mortality at doses equivalent to 75 mg aspirin/day. Interestingly, a non-linear U-shaped relationship between CRC death and aspirin dose was observed; the benefit associated with low-moderate doses (139–650 mg/day) was statistically significantly greater than higher doses (>650 mg/day). Recently, Chan and colleagues have addressed this question by examining the Nurses' Health Study and the HPFS cohorts. Their study shows that both cancer-specific and overall survival is increased in those who start taking aspirin after the diagnosis of CRC, but that aspirin taken before diagnosis does not affect survival.35 Another current study has shown that aspirin use prior to diagnosis decreases overall and cancer-specific mortality from CRC.40
A key strength of our study is the prospective nature of the CRC dataset, along with stringently matched controls. The cases were consecutively recruited across all the main surgical centres in Scotland and therefore represent the population. The controls were population-based matched for age, gender and area of residence with the cases, and hence the results are relevant to the general population rather than just high-risk groups. Although a recall-based questionnaire may be considered as a potential bias, it has the advantage that subjects have not introduced dietary and lifestyle changes since being diagnosed with cancer. The results of this study are further strengthened by the fact that detailed data were collected on potential confounding factors. The main shortcoming of this study is that we do not know if cases continued to take NSAIDs after diagnosis, which clearly may limit the conclusions drawn from the survival data presented. A recent study found if CRC cases were taking NSAIDs prior to diagnosis, 82% continued post-diagnosis40 A further limitation of this study, and others of similar design, is that there is no outcome measure which reflects plasma levels of NSAIDs ingested. Hence, there may be variation in exposure due to individual pharmacokinetics but one assumes such variation would be evenly distributed between cases and controls.
In summary, the key findings of our study are that high aspirin doses are not required for protection against CRC and that, while protection increases with duration of use, there are effects apparent within 5 years. Our results show that the lowest daily dose of aspirin used clinically (75 mg) is associated with reduced risk of CRC. This effect is apparent as early as 1 year but increases with time up to 10 years. Moreover, our results are applicable to the general population and not just high-risk groups. We found no demonstrable effect of NSAIDs on survival and so well-powered RCTs of incident CRC cases are required to address this issue.
Acknowledgments
We are grateful to Ruth Wilson and all those who contributed to recruitment, data collection and data curation for the COGS and SOCCS studies. In addition to all consultant colorectal surgeons who provided stage and other data on their patients, we are also indebted to Bob Diament (Chair), Farley Weir and Kevin Campbell of WoSCAN; Terry O'Kelly (Chair), Paulette McCouaig and Nicola Smith of NoSCAN for staging data.
References
Footnotes
FVND & ET are joint first authors and contributed equally to this study.
Funding The work was funded by grants from Cancer Research UK C348/A3758, C348/A8896), Scottish government Chief Scientist Office (K/OPR/2/2/D333, CZB/4/94); Medical Research Council (G0000657-53203); Centre Grant from CORE as part of the Digestive Cancer Campaign (http://www.corecharity.org.uk). ET is funded by Cancer Research UK Fellowship C31250/A10107. FVND is funded by Cancer Research UK Clinician Scientist Fellowship C26031/A11378.
Competing interests None.
Ethics approval This study was conducted with the approval of the Multicentre Research Ethics Committee, UK.
Provenance and peer review Not commissioned; externally peer reviewed.