Article Text

Abstract
Introduction Unexplained chest pain is potentially attributable to gastro-oesophageal reflux disease (GORD) or oesophageal motility disorders. Reflux chest pain may occur without heartburn. We explored the response of unexplained chest pain to proton pump inhibitor (PPI) therapy in randomised clinical trials (RCTs), differentiating patients with and without objective evidence of GORD.
Methods PubMed and Embase were systematically searched for RCTs that reported chest pain response to PPIs in patients who had had pH-monitoring and/or endoscopy to differentiate GORD-positive from GORD-negative subpopulations. Heterogeneity among studies was assessed using the Cochran Q and I2 statistics, and a fixed effect model was applied. Possible publication bias was assessed by Egger's test.
Results Six RCTs met the inclusion criteria. All used 24 h pH monitoring and/or endoscopy to define GORD-positive patients and improvement in chest pain to define response (five used ≥50%; one used ≥20%). The therapeutic gain of >50% improvement with PPIs relative to placebo was 56–85% in GORD-positive and 0–17% in GORD-negative patients. The RR of >50% improvement in chest pain with PPI versus placebo was 4.3 (95% CI 2.8 to 6.7; p<0.0001) for GORD-positive and 0.4 (95% CI 0.3 to 0.7; p=0.0004) for GORD-negative patients. Concomitant heartburn varied among trials from being an exclusion criterion to being essentially concordant with GORD-positive status.
Conclusions Unexplained chest pain in patients with endoscopic or pH-monitoring evidence of GORD tends to improve, but not resolve, with PPI therapy, whereas GORD-negative patients have little or no response. Heartburn was a poor predictor of whether patients with chest pain were GORD-positive or GORD-negative by objective testing.
- Chest pain
- Gastroeso phageal reflux
- proton pump inhibitors
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Possible oesophageal causes of chronic chest pain include gastro-oesophageal reflux disease (GORD) and oesophageal dysmotility.
Reflux-related chest pain may occur with or without concomitant typical symptoms of GORD.
Response of chest pain to empiric treatment with a proton pump inhibitor (PPI) has been suggested as a diagnostic tool to identify GORD as the cause of chest pain.
What are the new findings?
Systematic review of six randomised, placebo-controlled trials indicates that:
Chest pain in patients with abnormal oesophageal acid exposure and/or reflux oesophagitis tends to respond to PPI treatment, whereas patients without objective evidence of GORD have little or no response.
The therapeutic gain of >50% improvement with PPIs relative to placebo was 56–85% in GORD-positive and 0–17% in GORD-negative patients.
The presence of concomitant heartburn was a poor predictor of whether patients with chest pain responded to PPI therapy or not.
How might it impact on clinical practice in the foreseeable future?
The studies examined support the use of endoscopy and ambulatory pH monitoring in a management algorithm for patients with unexplained chest pain who either fail to respond or are unsatisfied with a trial of PPI therapy.
Introduction
Patients with chest pain for which no cardiac aetiology is demonstrable are often evaluated for an oesophageal aetiology. Possible oesophageal causes of chronic chest pain include gastro-oesophageal reflux disease (GORD) and oesophageal dysmotility.1 2 Recent evidence using impedance–pH reflux monitoring suggests that abnormal gastro-oesophageal reflux is more common than motor disorders in patients with chest pain, indicating that reflux is likely to have a major role in provoking chest pain in these patients.3 A further confounder in the management of patients with chest pain of non-cardiac origin is its long-recognised association with psychological comorbidity.4
Management strategies for non-cardiac chest pain of suspected oesophageal aetiology include both diagnostic testing and empiric therapy. Ambulatory pH-monitoring or, more recently, combined impedance/pH-monitoring can be used to demonstrate pathological reflux and/or to establish the degree of correlation between acid reflux events and chest pain.5 Alternatively, owing to the practicality of the approach, response of chest pain to empiric treatment with a proton pump inhibitor (PPI) has been suggested as a diagnostic tool to identify GORD as the cause of chest pain.6 However, for the empiric PPI therapy approach to be valid in this context, there is a presumption that chest pain is as responsive to acid suppressive therapy as is heartburn, a symptom widely managed with this strategy.7 Otherwise, diagnostic uncertainty persists since it is plausible either that the therapy is insufficient or that GORD is not the cause of the chest pain.
The Montreal definition and classification of GORD includes reflux-induced chest pain as a distinct oesophageal syndrome.8 Furthermore, the expert panel uniformly agreed that oesophageal and cardiac pain may be clinically indistinguishable (100% agreement) and that reflux-induced chest pain syndrome can occur without coexisting heartburn and/or regurgitation (98% agreement). However, while the former statement was based on evidence graded as ‘high’ quality, the latter was based only on ‘moderate’ quality data. Using the GRADE system9 for evaluating evidence, ‘moderate’ quality data implies that ‘Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.’9 In essence, the panel acknowledged the uncertainty of that statement. Consequently, the management of chest pain plausibly related to GORD is plagued by two uncertainties: first, whether or not response to empiric PPI therapy is a definitive diagnostic tool; and second, whether or not coexisting GORD symptoms (or test findings) are common. Hence, we aimed to address these questions through a systematic review of placebo-controlled trials of PPI therapy for chest pain of suspected oesophageal aetiology that had distinguished patients with and without objective evidence of GORD. We also sought to estimate the therapeutic gain of PPI therapy over placebo for the treatment of unexplained chest pain among patients with or without objective evidence of GORD.
Methods
We performed a systematic search of PubMed and Embase from 1966 to 4 March 2010 (figure 1). The search strategy and search terms used were: ‘Gastro-oesophageal Reflux’ (Mesh, PubMed only) OR GERD OR GORD OR reflux OR gastro-oesophageal reflux disease OR reflux oesophagitis OR non-erosive reflux disease OR NERD) AND (‘Proton Pump Inhibitors’ (Mesh, PubMed only) OR PPI OR omeprazole OR lansoprazole OR pantoprazole OR rabeprazole OR esomeprazole OR tenatoprazole) AND chest pain. This was supplemented by a search of abstracts from Digestive Disease Week and United European Gastroenterology Week 2007–2010. Recent reviews were also examined for references of relevant primary data.
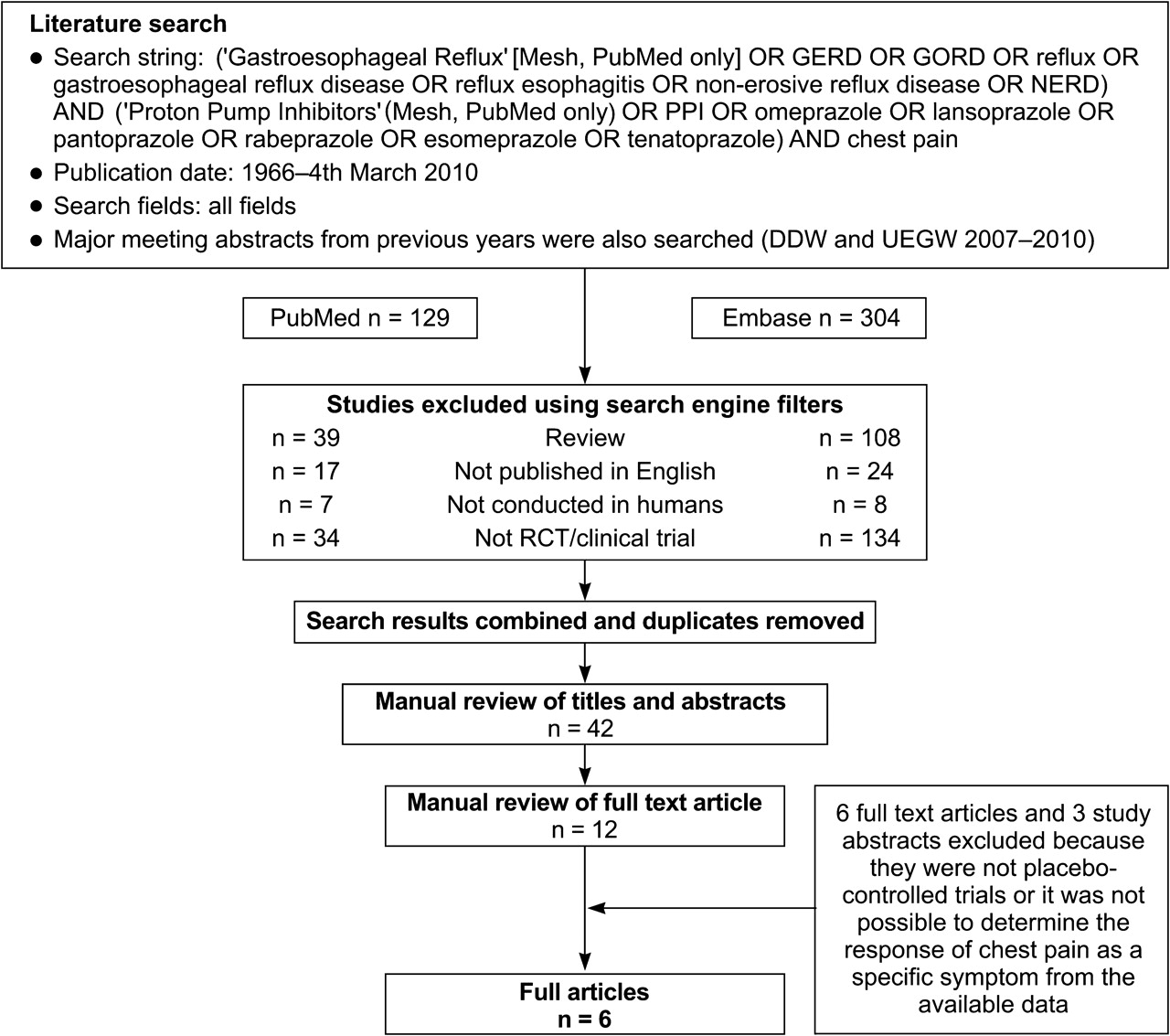
Flow diagram of search results. RCT, randomised controlled trial.
We selected publications that reported the change in chest pain as an individual symptom following PPI or placebo treatment in patients with unexplained chest pain. We excluded reviews, studies that had not been conducted in adults and studies that had not been published in English. We also excluded open-label or other studies that were not randomised controlled trials (RCTs). Studies were initially screened on the basis of titles and abstracts. The full article was reviewed when its relevance to this review was not clear from the abstract. All three authors independently reviewed the search results to ascertain their suitability for inclusion with disagreements resolved by consensus.
We examined the response of chest pain to PPI treatment in ‘GORD-positive’ and ‘GORD-negative’ patients separately. We considered objective evidence of GORD to be either a positive pH-monitoring test (abnormal oesophageal acid exposure) or endoscopic evidence of reflux oesophagitis. Although combined impedance/pH-monitoring would have been an additional criterion, we found no relevant RCTs that used this test. Within each study, GORD-negative patients were defined as the residual patient population not meeting the criteria for GORD. We calculated the therapeutic gain for PPI over placebo treatment (the proportion of patients who responded to placebo was subtracted from the proportion who responded to treatment) for both GORD-positive and GORD-negative patients.
Statistical analysis
Where appropriate, we performed meta-analysis of RCTs using StatsDirect version 2.7.8 (StatsDirect Ltd, Altrincham, Cheshire, UK). We assessed heterogeneity among included studies using the Cochran Q and I2 statistics. Statistically significant heterogeneity was defined as a p value of <0.10 on the Cochran Q test. If significant heterogeneity was found, we planned to use a random effects model for subsequent meta-analysis; otherwise, we planned on using a fixed effect model. We assessed possible publication bias by visual examination of funnel plots and the use of Egger's test for bias, with p values of <0.10 considered significant.
Results
Figure 1 summarises the search results. After eliminating duplicate hits, review articles and clinical studies that were not RCTs, 42 potentially relevant publications were identified. Review of the abstracts of these publications reduced the pool further to 12 articles, which were reviewed in full. Of these 12 articles, six were excluded after reviewing the full text because they were not randomised, placebo-controlled trials, did not adequately define GORD or did not adequately specify a means for defining response of chest pain to treatment.10–15 A further three studies identified by the search of recent major congress abstracts were excluded: the first was not placebo-controlled,16 it was not possible to determine the response of chest pain as a specific symptom in the second,17 and we were unable to extract the relevant information from the data available to us in the third.18
Hence, six RCTs were included in our analysis.6 19–23 All reported the response of chest pain to treatment with a PPI and with placebo in patients that could be designated as GORD-positive or GORD-negative. All of the included trials except one21 had a cross-over design. The primary endpoint in all the trials was to determine the clinical value of PPIs in detecting and/or treating patients with unexplained chest pain.
Assessment of chest pain
All patients in the trials had chest pain with a negative cardiac evaluation. Typically, this included a normal coronary angiogram. Beyond that, little detail is provided as to how closely the chest pain mimicked that of cardiac ischaemia. Table 16 19–23 details the methodology for assessing chest pain among studies, the instruments used to grade its severity and responsiveness to therapy, and the magnitude of response that was considered a therapeutic success. The main consistency among the six trials stems from the fact that three of them emanated from the same centre.6 22 23 Also notable (and distinct from GORD trials targeting heartburn) is the acceptance of partial response as constituting successful treatment; as little as 20% improvement could be construed as a therapeutic success in one trial.19
Chest pain assessment tools
Chest pain responsiveness to PPI therapy
Table 26 19–23 details the patient inclusion characteristics, PPI regimen and treatment response for the six RCTs. Although three studies used reflux oesophagitis as a diagnostic criterion for GORD,6 20 22 one specifically excluded patients with reflux oesophagitis.21 All trials except one21 used twice-daily PPI regimens, resulting in doses that were higher than those approved for the treatment of GORD. In every trial that a statistical evaluation was reported, PPI therapy was more effective than placebo in GORD-positive patients, whereas this was never the case in the GORD-negative subgroups. This difference is further accentuated in figure 2 for the five RCTs in which both GORD-positive and GORD-negative groups were tested; in one trial, only GERD-positive patients were studied.19 Assessed in terms of therapeutic gain relative to placebo, PPI therapy was associated with a mean therapeutic gain of 62% (range 56–85%) for GORD-positive patients and 5% (range 0–17%) for GORD-negative patients.
Responsiveness of chest pain to proton pump inhibitor therapy among the six clinical trials with patients with chest pain subgrouped into those with and without objective evidence of gastro-oesophageal reflux disease
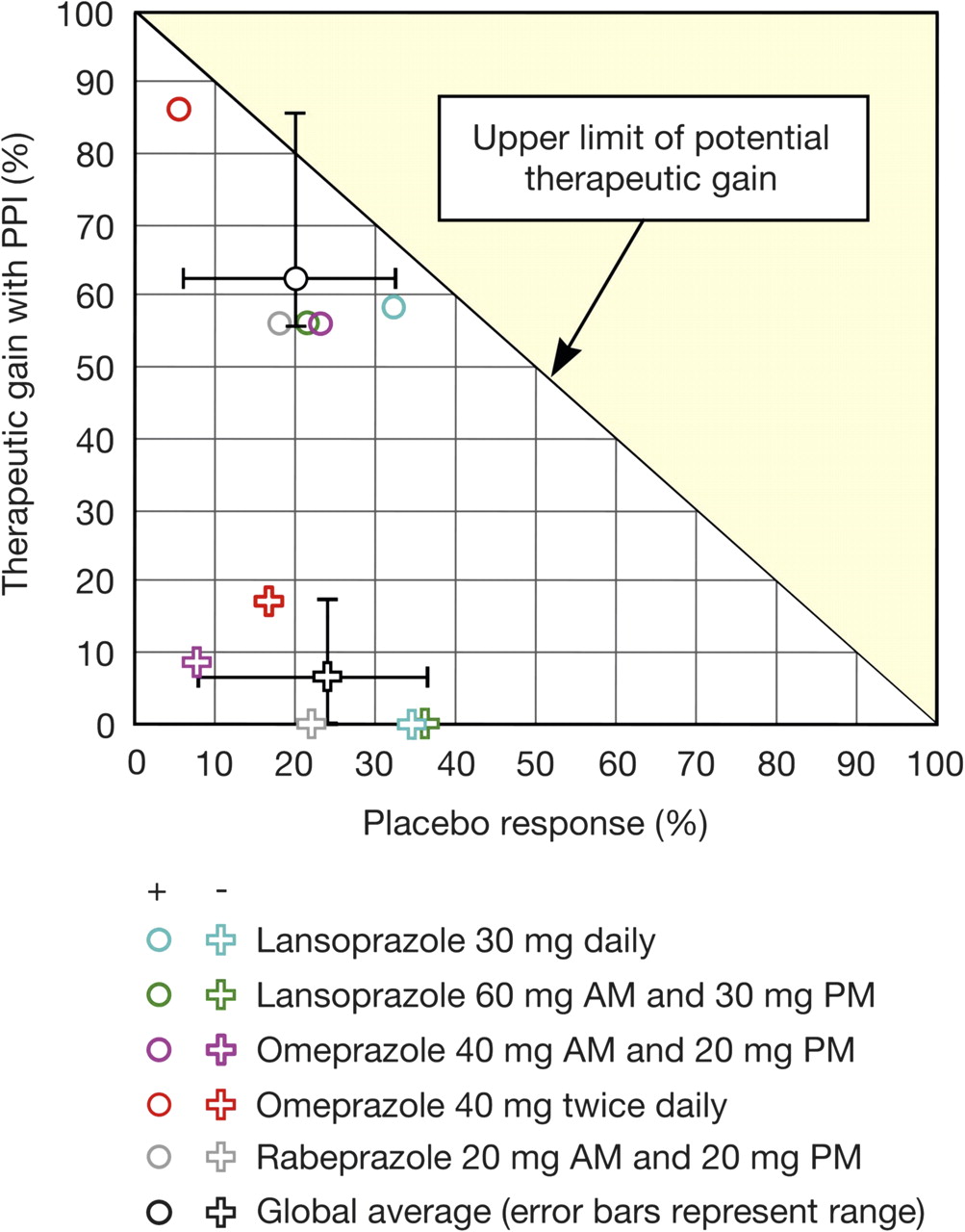
Therapeutic gain in randomised placebo-controlled trials of proton pump inhibitor treatment for unexplained chest pain. All five clinical trials used a threshold of >50% improvement in chest pain to define a positive treatment response.6 20–23 (+) indicates GORD-positive patients (abnormal oesophageal acid exposure and/or reflux oesophagitis); (−) indicates GORD-negative patients (no objective evidence of GORD); PPI, proton pump inhibitor. The upper limit of potential therapeutic gain (diagonal line) is 100 minus the placebo response rate.
Statistical analysis
The five RCTs included in figure 2 were sufficiently similar to be suitable for meta-analysis; they used the same threshold for a treatment response.6 20–23 Among GORD-positive patients in these five RCTs, the pooled RR for at least a 50% improvement in chest pain with PPI therapy compared with placebo was 4.3 (95% CI 2.6 to 6.7; p<0.0001). Since there was no statistically significant heterogeneity among these RCTs (Cochran Q=3.69; degrees of freedom (df)=4; p=0.45; I2=0%), a fixed effect model was applied (figure 3A). However, we found statistical evidence of publication bias (Egger's bias=2.97; 95% CI 1.19 to 4.75; p=0.013). Visual inspection of the funnel plot showed possible lack of small studies reporting a low magnitude of effect. For GORD-negative patients, the pooled RR for at least a 50% improvement in chest pain with PPI therapy over placebo was 0.44 (95% CI 0.28 to 0.69; p=0.0004). Again, there was no significant heterogeneity among the studies (Cochran Q=6.25; df=4; p=0.18; I2=36%) so a fixed effect model was applied (figure 3B). There was no evidence of significant publication bias (Egger's bias=−2.20; 96% CI −7.50 to 3.10; p=0.278).

{kind=link}
{kind=link}
{kind=link}
Gastro-oesophageal reflux disease symptoms other than chest pain
Throughout the studies, symptoms and symptom response were usually assessed by means of patient diaries (table 1). However, not all studies reported the presence of concomitant GORD symptoms (table 3). Symptoms were also recorded in symptom diaries during 24 h ambulatory intra-oesophageal pH monitoring to diagnose GORD in all studies (table 3), but the degree of correlation between oesophageal acid exposure and symptoms was not a specific inclusion criterion in any case. Not surprisingly, given the variable handling of GORD symptoms and reflux oesophagitis in patient screening for inclusion, there was marked variation in the prevalence of heartburn, regurgitation and dysphagia among studies reporting these data (table 3). One interesting association was the relatively high prevalence of dysphagia in some of the GORD-negative subgroups, suggesting altered oesophageal motility as a potentially relevant factor.
Oesophageal symptom profile in patients with chest pain categorised as gastro-oesophageal reflux disease-positive or-negative
Discussion
Chest pain can be a major symptom of oesophageal disease in general and of GORD in particular. This systematic review and meta-analysis examined the responsiveness of unexplained chest pain to PPI therapy where it had been established that the chest pain was ‘non-cardiac’ in aetiology. The major finding of this systematic review was that the coexistence of objective measures of GORD, specifically a positive pH-monitoring study or reflux oesophagitis, was strongly predictive of a positive response to PPI therapy, whereas the absence of such evidence was predictive of a poor treatment response. In contrast, the coexistence of heartburn and/or regurgitation in the clinical presentation was not a consistent predictor of PPI response (figures 2 and 3).
The implications of a likely GORD aetiology for unexplained chest pain would be straightforward if responsiveness to PPI therapy were complete and dichotomous, as is often the case with heartburn. However, this was far from the case. Rather, the threshold for a ‘positive’ chest pain response in these trials was typically a reduction in chest pain intensity of 50% or more, with one study accepting a threshold improvement of as little as 20%.19 That degree of responsiveness could just as easily be termed ‘PPI failure’ as a positive treatment effect and argues more for taking these findings as a proof-of-concept that PPI therapy can be beneficial in patients with objective evidence of GORD than for utilising a PPI trial as a diagnostic test. There is also the issue of PPI dose; with one exception21 all of the RCTs included in this analysis used twice-daily PPI dosing, which is higher than the doses typically approved for the treatment of GORD. However, the same magnitude of response was reported in the only trial that used standard dosing.21 Consequently, while the opinion that the treatment of chest pain requires a higher than standard dose of PPI may or may not be correct it is not based on clinical trial evidence demonstrating a dose–response relationship.
The panel of experts who formulated the Montreal definition and classification of GORD uniformly agreed that the experience of chest pain caused by acid reflux can be indistinguishable from ischaemic cardiac pain.8 Certainly, the heart and oesophagus share common elements of sensory innervation offering some physiological basis for symptom overlap.24 25 In GORD, the most typical symptom is heartburn. However, some patients may perceive ‘heartburn’ as chest pain. The experts participating in the Montreal consensus agreed that this distinction may be virtually impossible for some patients. A similar conclusion during the validation work for the Reflux Disease Questionnaire (RDQ) resulted in dimensionalising ‘heartburn’ into items measuring frequency and severity of both ‘burning’ and ‘pain’ behind the breastbone.26 Stemming from the RDQ development project and also reflecting the input of patient focus groups, the Diamond study of upper gastrointestinal symptoms in primary care included chest pain under the symptom descriptor of heartburn.27 Thus, although the studies included in this review focused on chest pain as a distinct symptom independent of heartburn, it remains unclear how often this is the case among the GORD-positive subgroups. Alternatively, in some instances, chest pain may be indicative of an altered subjective perception of reflux-induced sensation.
Although reflux was a likely trigger of chest pain in the GORD-positive subgroups in these RCTs, we found little evidence to support that contention among the GORD-negative subgroups. Patients who lacked definite evidence of GORD were, if anything, more likely to respond to a placebo than to a PPI (figures 2 and 3). These patients were also more likely to have concomitant dysphagia in some of the trials (table 3). Furthermore, other investigations have established that patients with unexplained chest pain, but without objective evidence of GORD, frequently have psychological comorbidity.4 28 29 Taken together, these observations suggest that a management algorithm for unexplained chest pain should use endoscopy and reflux testing as a branch point for selecting which patients might benefit from further testing with the intent of identifying non-GORD aetiologies. Although not a comprehensive list of possibilities, oesophageal motility disorders, anxiety, depression, somatisation and microvascular angina would be important considerations.30–32
Among the strengths of this systematic review was the extensive literature search used to identify potentially relevant studies, and our focus on high quality trials that clearly defined chest pain, characterised GORD, and evaluated the chest pain response to PPI or placebo treatment. A potential weakness, as with any systematic review and meta-analysis, is the possibility that some studies that failed to demonstrate a significant symptom improvement with a PPI may not have been published in the peer-reviewed literature, thereby leading us to overestimate the effectiveness of PPI treatment. However, we found no conclusive evidence of major publication bias.
In summary, patients with unexplained chest pain after cardiac evaluation with objective evidence of GORD (endoscopy, pH-monitoring) were likely to respond favourably to PPI treatment, whereas those without objective evidence of GORD were not likely to respond to treatment. The magnitude of response was only partial despite using PPI regimens in excess of those approved for the treatment of GORD. Coexistent typical GORD symptoms were not reliably related to PPI treatment response in the RCTs we reviewed. These observations support the observation that chest pain can be a major symptom of GORD with or without concomitant heartburn. How often this represents a ‘heartburn equivalent’, as opposed to pain closely mimicking cardiac ischaemia remains unresolved. The studies examined support the use of endoscopy and ambulatory pH monitoring in a management algorithm for patients with unexplained chest pain who either fail to respond or are unsatisfied with a trial of PPI therapy. Future studies may be improved by standardising pH (or pH/impedance) monitoring methodology, establishing the lowest effective dose of PPI, defining a clinically meaningful response to PPI treatment, developing suitable patient-reported outcome assessment tools for gauging the response of chest pain to therapy and assessing the impact of chest pain on patient health-related quality of life.
References
Footnotes
Funding NH was supported by an unrestricted educational grant from AstraZeneca R&D Mölndal, Sweden. Data from this study was accepted as a poster presentation at Digestive Disease Week 2011.
Competing interests PJK has acted as a consultant for AstraZeneca, Eisai, EndoGastric Solutions, Ironwood, Novartis, Movetis, Revalesio and XenoPort. NH is an employee of Oxford PharmaGenesis™ Ltd. CWH has acted as a consultant for Takeda, XenoPort, Santarus, Procter & Gamble, Merck/Schering-Plough Healthcare, Boehringer Ingelheim, Novartis Consumer Health, Novartis Oncology, Otsuka and KV Pharmaceuticals, and as a speaker for Takeda, Novartis and Otsuka.
Provenance and peer review Not commissioned; externally peer reviewed.