Article Text

Abstract
Objective Postpolypectomy surveillance guidelines for colorectal cancer introduced the concept of ‘risk stratification’; however, few studies have been conducted for validation of its usefulness. The aim of this study was to assess the 5-year incidence of advanced neoplasia recurrence based on the risk stratification scheme of the guidelines and to identify its risk factors.
Methods A prospective study of surveillance colonoscopy after screening colonoscopy was carried out at the Seoul National University Hospital Healthcare System Gangnam Center. 3803 asymptomatic Koreans aged 50–69 were enrolled prospectively and 5-year cumulative adenoma rates were analysed according to three risk groups: normal (no baseline adenoma), low-risk (1–2 adenomas <10 mm) and high-risk (an advanced adenoma or ≥3 adenomas) groups. The RR was computed by HR using Cox proportional regression after multivariate adjustments. The primary outcome was the 5-year cumulative rate of recurrent advanced adenoma in each risk category and the secondary outcome was its predictive factors.
Results Among 3803 subjects enrolled between 2003 and 2005, 2452 were followed-up within 5 years: 1242, 671 and 539 in the normal, low-risk and high-risk groups, respectively. Compared with the normal group, the low-risk group had a sufficiently low 5-year incidence and did not show an increased risk for subsequent advanced adenoma (2.4% vs 2.0%, HR=1.14, 95% CI 0.61 to 2.17). Conversely, a significantly higher 5-year rate (12.2%) and early recurrence (4.6, 7.4 and 9.6% at 1, 2 and 3 years) of advanced adenoma were revealed in the high-risk group. Among various patients and adenoma characteristics, only high-risk adenoma (HR=5.95, 95% CI 3.66 to 9.68) along with a number of ≥3 (HR=3.06, 95% CI 1.51 to 6.57) and size ≥10 mm (HR=3.02, 95% CI 1.80 to 5.06) were independent predictors.
Conclusions The surveillance interval for low-risk patients could be extended beyond 5 years. Colonoscopic surveillance should be targeted to high-risk patients, and 3-year follow-up after initial polypectomy may be appropriate.
- Colorectal neoplasia
- surveillance
- colonoscopy
- recurrence
- risk factor
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Surveillance for colorectal cancer is a large part of colonoscopic practice, draining resources from screening and diagnosis.
Postpolypectomy surveillance guidelines introduced the concept of ‘risk stratification’ on the basis of baseline adenoma characteristics.
Lack of confidence in the guidelines may be one of the reasons for low adherence among colonoscopists.
What are the new findings?
Compared with those with average risk, low-risk patients had very low 5-year incidence and did not show an increased risk for subsequent advanced adenoma.
High-risk patients showed a significantly higher 5-year rate and early recurrence of advanced adenoma.
Among various patients and adenoma characteristics, only high-risk adenoma along with a number of ≥3 and size ≥10 mm were independent predictors.
How might it impact clinical practice in the foreseeable future?
These findings support the risk stratification scheme of the current guidelines.
Low-risk patients may be followed-up as average-risk subjects. Colonoscopic surveillance would be targeted to high-risk patients, and 3-year follow-up after initial polypectomy may be appropriate.
Introduction
The first screening colonoscopy and polypectomy produce the most significant effects on reducing incidence and mortality of colorectal cancer (CRC).1 2 It is also evident that most patients with adenoma will not benefit from surveillance: up to half of all adults have adenomas during their lifetime and only 6% develop CRC.3 The fact that surveillance is now a large part of colonoscopic practice, draining resources from screening and diagnosis, has become increasingly obvious.4 To date, most studies have focused on the time interval from initial colonoscopy to the next examination, and the recommended interval has been lengthened.3 5–7 Besides, greater knowledge of risk factors for recurrence of advanced adenoma would allow their stratification; the frequency of follow-up can then be tailored, which would improve the overall efficiency and effectiveness of colonoscopic surveillance. Newly developed postpolypectomy surveillance guidelines have introduced the concept of ‘risk stratification’ on the basis of baseline adenoma characteristics.7 They call for repeated screening colonoscopy at 10 years for subjects with no adenoma, and surveillance at 5–10 years for patients with low-risk adenoma, defined as one or two small (<10 mm) adenomas, and at 3 years for those with high-risk adenoma, defined as an advanced adenoma or ≥3 synchronous adenomas. However, uncertainty remains with respect to policies for low-risk patients. Furthermore, due to insufficient empirical evidence and lack of confidence in the guidelines, most colonoscopists have erred on the side of repeating examinations earlier than the recommended interval.8–11 Only one surveillance study used the risk stratification scheme of the current guidelines and reported their limited predictive accuracy for advanced adenoma at 4 years.10 12 Few studies have included average-risk persons with a negative screening colonoscopy; even the largest of these studies had a rather small sample size for precise risk estimation (298 adenoma-free controls), and risk variables were not extensively assessed.13
The aim of this large-scale prospective study was to (1) estimate the 5-year cumulative incidence of advanced adenoma and compare differences among risk categories inherent to the guidelines and (2) determine whether purported risk factors for occurrence of colorectal neoplasia would also be predictive of its recurrence.
Methods
Study population
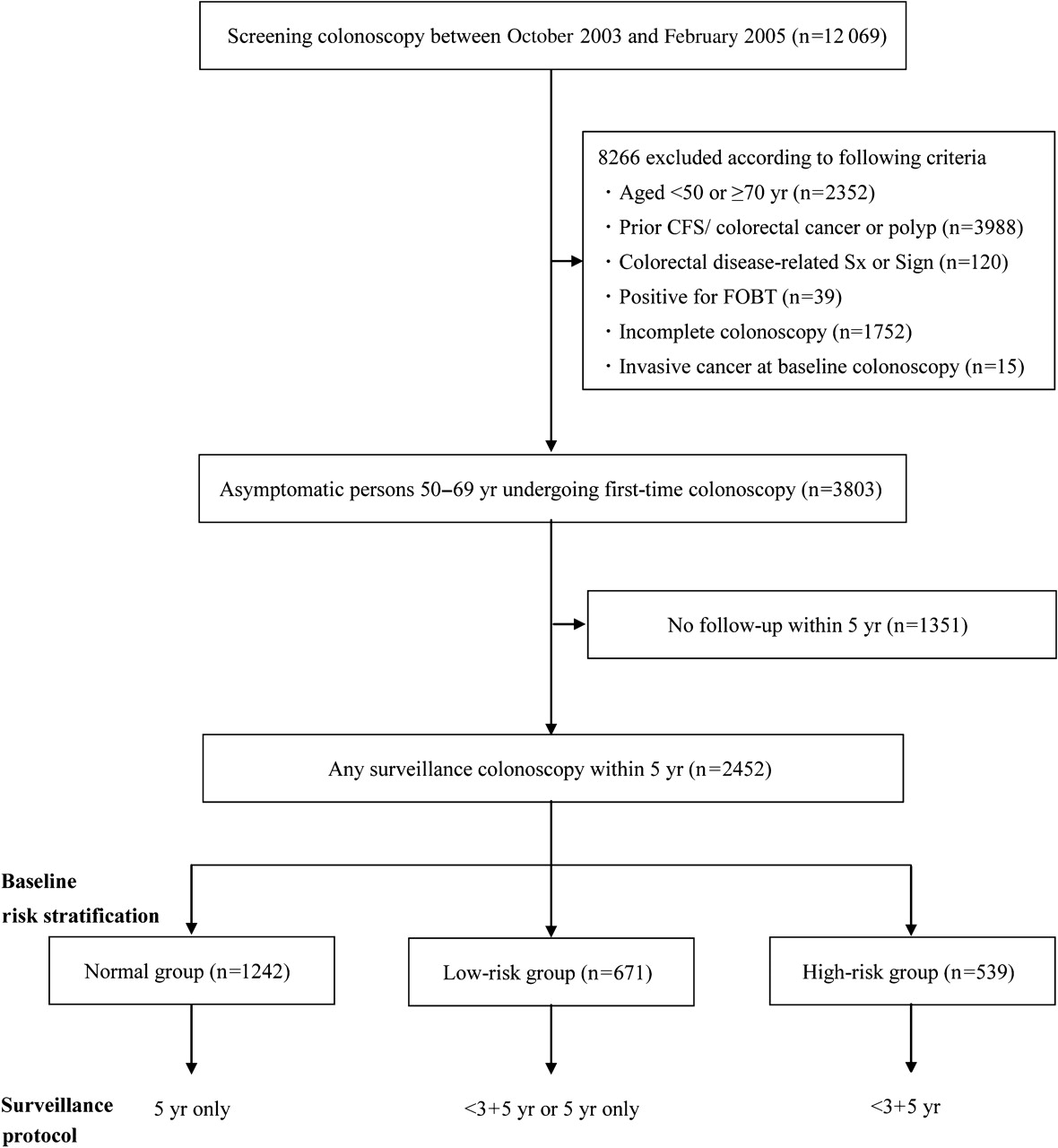
This is a prospective study conducted at the Seoul National University Hospital (SNUH) Healthcare System Gangnam Center. Our surveillance protocols were dependent on the risk stratification scheme of the current guidelines.7 The normal group (no adenoma detected at baseline) was rescreened at 5 years. In the case of the low-risk group (1 or 2 adenomas <10 mm), timing of the next examination was not determined by a rigid protocol and was left to the physician's discretion—that is, either within 3 years and 5 years or at 5 years only by taking into account age, family history, co-morbidities and patients’ preference. The high-risk group (an advanced adenoma or ≥3 adenomas) was assigned to follow-up within 3 years and then 5 years after baseline colonoscopy (figure 1). Each subject was informed of a scheduled surveillance programme. Follow-up clinic reminder calls were made 1 month before the expected date of colonoscopy. The study protocol was approved by the Institutional Review Board of SNUH. Written informed consent for participation was obtained from all subjects prior to the procedures.

Diagram of enrolment in study groups and surveillance protocol.
To be included in the study, subjects were required to meet the following criteria: (1) first-time screening colonoscopy between October 2003 and February 2005; (2) asymptomatic volunteers aged 50–69 at their initial examination; (3) complete clearing colonoscopy at every examination; and (4) at least one or more follow-ups within 5 years after baseline colonoscopy. We excluded the following cases: colorectal disease-related symptoms or signs (eg, recent bowel habit change, unexplained weight loss, anaemia, faecal occult blood test positivity or lower gastrointestinal tract bleeding not attributable to haemorrhoids), prior history of CRC or polyp, surgical resection of the colon or rectum, inflammatory bowel disease or intestinal tuberculosis, coagulopathy, and incomplete examination of the entire colon due to inadequate preparation or technical difficulties. Fifteen cases of invasive CRC at baseline colonoscopy were also excluded.
Colonoscopy and pathological review
All colonoscopic examinations had been equally allocated to a total of 15 board-certified endoscopists who experienced >3000 colonoscopies (at least 500 polypectomies) and achieved >25% of the adenoma detection rate in routine procedures.14 15 Conventional white light colonoscopes (CF-H260 series; Olympus, AIZU, Japan/EC-450HL5, EC-450WM5 or EC-590ZW series; Fujinon, Saitama, Japan) were used in performance of all procedures. During the study period, adenoma detection rates of the individual examiners ranged between 28% and 34% (mean 31%) with no significant differences among them (p >0.05). Since publication of the study by Barclay et al, we have attempted to adjust withdrawal times to a minimum of 6 min for each colonoscopy in order to allow for adequate inspection.16 Colonoscopy reports provided information on number, location and size (estimated with opened biopsy forceps or measured after resection) of polyps. All detected polyps were completely removed: diminutive polyps ≤5 mm by biopsy forceps and larger ones by en bloc endoscopic mucosal resection. Large sessile or flat adenomas and laterally spreading tumours (ie, tumours >10 mm in diameter with a low vertical axis, but extending laterally along the interior luminal wall)17 18 exceeding 20 mm in size were removed by piecemeal endoscopic mucosal resection or endoscopic submucosal dissection.19 20 All specimens were classified by expert gastrointestinal pathologists according to the WHO criteria.21 Only a minority (<2%) of polyps with metaplastic histological features were diagnosed as serrated adenoma. The quality of bowel preparation was rated as follows: (1) excellent (clean and empty); (2) good (clear fluid); (3) fair (brown fluid but no residue after aspiration); and (4) poor (semisolid or solid stool).22
Definitions and assessment of risk variables
Structured, self-administered questionnaires were reviewed on gastrointestinal symptoms and personal medical history, including current smoking (at least one cigarette per day for the previous 12 months), alcohol consumption (≥70 g/week) and regular use (ie, medication for ≥3 months during the preceding 12 months) of aspirin/non-steroidal anti-inflammatory drugs (NSAIDs) or 3-hydroxy-3-methylglutaryl CoA reductase inhibitors (statins). The questionnaires also asked about family history of CRC (at least one first-degree relative with CRC diagnosed at any age), educational attainment and monthly family income. Further information was ascertained by endoscopists regarding reasons for colonoscopy and prior diagnosis of CRC or polyps. Physical examinations for all subjects were performed on the day of colonoscopy by trained nurses using a written systematic protocol with standardised instruments. All colonoscopy and pathology reports, as well as medical records, were collected from our database (Healthwatch version 2.0).14 15
A complete clearing colonoscopy was considered to include the following: colonoscope insertion into the caecum, above fair grade preparation and removal of all detected polyps. In the case of a remnant adenomatous polyp or poor grade preparation, repeated endoscopy was conducted in order within 6 months to complete the previous endoscopic procedure. When residual lesions of previously treated polyps were observed at follow-up, they were counted as polyps detected during the same endoscopic examination. Any subsequent colonoscopy occurring within 6 months of the prior colonoscopy of an individual was judged to be a part of the same episode; additional adenomas were regarded as missed lesions and included as part of the prior colonoscopy findings. We defined an adenoma as recurrent if found during any colonoscopy performed at least 6 months after the baseline colonoscopy. Findings for each subject were stratified according to the most advanced lesion detected (ie, adenoma with the largest diameter or the most serious histology). Advanced adenoma was classified as ≥10 mm in diameter, containing >25% villous structure or high-grade dysplasia. Pathological interpretation of intramucosal carcinoma or carcinoma in situ was categorised as a high-grade dysplasia.
Statistical analysis
Data were stratified according to the three aforementioned baseline risk groups. In addition, we compared the baseline characteristics of subjects who underwent follow-up colonoscopy and those who did not in each risk group using the Student t test and χ2 test as appropriate for comparison of means and proportions. The Kaplan–Meier method was used for description of the cumulative rate of advanced adenoma. RR was estimated using the Cox proportional hazard regression model by computation of the HR and corresponding 95% CIs after multivariate adjustments (age, sex, family history, body mass index (BMI), waist circumference, smoking, alcohol, aspirin/NSAIDs, statins, education level, household income, baseline adenoma characteristics and risk categories according to the guidelines). We used absolute risk for calculation of the number needed to rescreen—that is, the number of persons who would need 5-year rescreening colonoscopy in order to detect one advanced adenoma. The Statistical Package for the Social Sciences version 17.0 (SPSS) was used for all analyses. A two-tailed p value of <0.05 was considered statistically significant.
Results
Baseline characteristics of the study population
The detailed enrolment process and rates of actual surveillance are shown in figure 1 and table 1. In brief, a total of 55 193 persons visited our centre for a routine check-up between October 2003 and February 2005. One-fifth of them (n=12 069) underwent colonoscopy (mean age 52.7±9.6 years, 63.5% male). Reasons for colonoscopy included a prior history of colorectal polyps/routine postpolypectomy surveillance (55.4%) and family history of CRC (7.0%). A small number of procedures were performed for diagnostic purposes, including faecal occult blood test positivity (0.3%), anaemia/lower gastrointestinal tract bleeding (0.7%) and change in bowel habits (1.1%). Following application of various exclusions or the initial enrolment criteria outlined above, the remaining 3803 asymptomatic persons aged 50–69 with first-time screening colonoscopy were eligible. Of those, 1351 did not have colonoscopic surveillance. Accordingly, 2452 (56.9% among persons with no baseline adenoma, 71.8% among those with low-risk adenoma and 78.6% among those with high-risk adenoma) underwent at least one follow-up colonoscopy within 5 years and comprised the study population. We also compared baseline characteristics of the surveillance group with those of the non-surveillance group (table 1); among subjects with a negative baseline colonoscopy, the former group was more likely to be older and to have higher proportions of males, family history, college graduates and high economic status. On the other hand, among those with baseline adenomas (both low-risk and high-risk categories), there were no intergroup differences in terms of sociodemographic features or purported CRC risk variables.
Comparison of baseline characteristics between subjects who underwent follow-up colonoscopy (n=2452) and those who did not (n=1351) in each risk group
Baseline characteristics of the study population are given in table 1. A total of 2452 subjects were classified as follows: 1242 in the normal group (50.7%), 671 in the low-risk group (27.4%) and 539 in the high-risk group (22.0%), including 27 cases with high-grade dysplasia. Subjects in the higher risk groups were more likely to be older, male and have greater exposure to putative risk factors, including obesity represented by BMI or waist circumference, smoking and alcohol, as well as possible chemopreventive agents, such as aspirin/NSAIDs and statins (for each variable, p<0.001). However, numerical differences in rates of family history, aspirin/NSAID or statin user and high socioeconomic status were not statistically significant among the three risk groups. Mean follow-up period and average frequency of surveillance colonoscopy were 4.7 years/1.1, 4.5 years/1.3 and 4.4 years/1.9 in the normal, low-risk and high-risk groups, respectively. Most episodes consisted of a single examination and ∼9% had more than two examinations within 6 months which was considered as part of the previous examination. Bowel preparation was graded as good to excellent in 82.0% and no major complications resulting in serious morbidity or death were documented at either baseline or follow-up examinations. Two cases of microperforation and five cases of minor bleeding were reported, all of which followed polypectomy and were treated medically.
Cumulative incidence of recurrent colorectal neoplasia
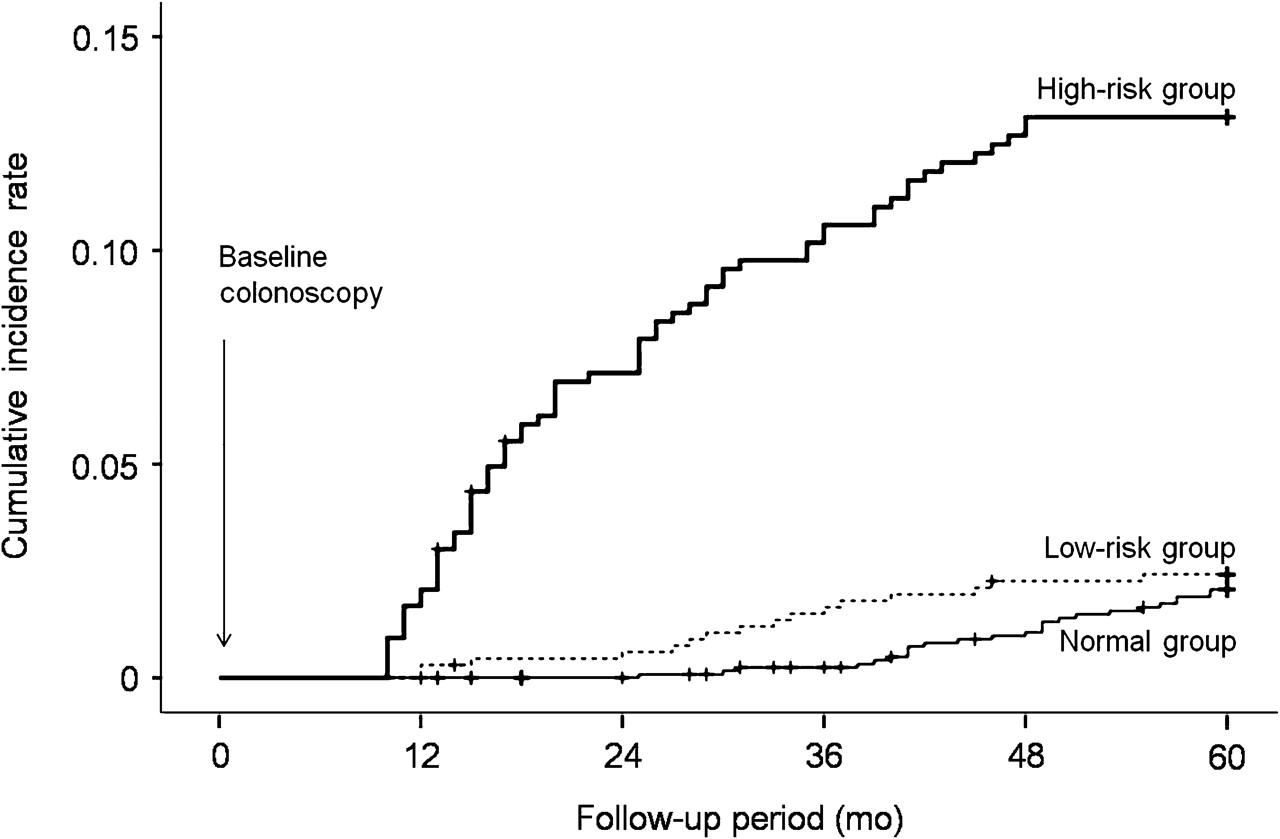
Cumulative results represent the most advanced lesion found in any colonoscopy performed during the follow-up period (table 2). Five-year cumulative rates of overall adenoma showed a progressive increase across the three risk groups (28.7, 45.8 and 57.3%, p<0.001). With respect to the 5-year incidence of advanced adenoma, the high-risk group exhibited a significantly higher rate of 12.2% as compared with rates of 2.0% for the normal group and 2.4% for the low-risk group. Surveillance results according to the timing of the first follow-up colonoscopy are summarised in table 2. Among subjects in the low-risk group, 355 (52.9%) underwent their first surveillance within <3 years. Rates of advanced adenoma were similar irrespective of the timing of the first surveillance (1.7% at <3 years vs 2.2% at 3–5 years, p=0.11). Almost all subjects in the high-risk group underwent their first surveillance within 3 years and the majority of them underwent repeat examinations. Notably, most advanced adenomas in the high-risk group were detected within <3 years, with 1-, 2- and 3-year cumulative rates of 4.6, 7.4 and 9.6%, respectively (figure 2). Numbers needed to rescreen were 49 (95% CI 15 to 88) for the normal group and 42 (95% CI 12 to 98) for the low-risk group, while the number for the high-risk group was 8 (95% CI 5 to 20). Among 138 newly observed advanced adenomas in 107 subjects, 91 (66%) were ≥10 mm and 73 (53%) had villous histology. No significant difference in the location of recurrent advanced adenomas was observed between the right-side (n=71) and the left-side colon (n=67). During the follow-up period, only four subjects were diagnosed with interval high-grade dysplasia or cancer; among three cases of high-grade dysplasia, two were from the high-risk group (at 18 and 28 months) and one was from the low-risk group (at 59 months). One case of invasive rectal cancer (T1N0) developed in a 64-year-old man in the high-risk group 23 months after baseline colonoscopy.
Occurrence of colorectal neoplasia based on timing of follow-up colonoscopy and their 5-year cumulative rates in different risk groups

{kind=link}
{kind=link}
Cumulative incidence of advanced adenoma according to the baseline risk categories.
Risk factors for recurrence of colorectal neoplasia
Table 3 presents the RR of various patient and adenoma characteristics for interval neoplasia after multivariate adjustments. Old age, male, alcohol, number of adenomas (≥3) and villous histology at baseline had a significant effect on overall adenoma recurrence. Meanwhile, the high-risk group (vs low-risk group, HR=5.95, 95% CI 3.66 to 9.68) along with a number of ≥3 (vs 1 or 2 adenomas, HR=3.06, 95% CI 1.51 to 6.57) and size ≥10 mm (vs <10 mm adenoma, HR=3.02, 95% CI 1.80 to 5.06) were the only independent predictors for advanced adenoma recurrence. Conversely, compared with the adenoma-free group, the low-risk group did not show an increase in the risk for subsequent advanced adenoma (HR=1.14, 95% CI 0.61 to 2.17). In addition, the HR for advanced adenoma did not differ significantly regardless of histology type or other covariates.
Multivariate analyses on RR of baseline characteristics for recurrent colorectal neoplasia
Discussion
To the best of our knowledge, this is the first large-scale study to prove the usefulness of current postpolypectomy surveillance guidelines. Low-risk patients developed advanced adenoma at the same low rate as average-risk persons, which suggests that the presence of one or two non-advanced adenomas may not increase the risk for subsequent advanced adenoma (2.4% vs 2.0%, HR=1.14, 95% CI 0.61 to 2.17). Our results were in accordance with a previous US report13—albeit their high point estimate for RR (1.92) and wide CI (0.83 to 4.42) due to possible type II error—and provide empirical support for recent revision of the surveillance interval for low-risk patients from 5 years to 5–10 years.7 We confirmed that high-risk patients have a significantly higher 5-year incidence of advanced adenoma (12.2%), which increased with time up to 3 years after initial examination, but was significantly lower for those re-examined after >3 years (figure 2). This finding may be representative of either incident cases since the prior colonoscopy or higher chances of missed lesions or incomplete removal at baseline, even though it was performed only by experts.13 24 25 Its implications for surveillance are important because achievement of a clean colon may reduce or even eradicate the need for follow-up in some subgroups.26–28 Our data reinforce the effectiveness of initial screening for reducing the incidence of serious outcome; the overall rate of interval high-grade dysplasia or cancer was remarkably low (0.4 per 1000 person-years), allowing for their prevalence at first-time colonoscopy (0.6% in 50–59 years).15
We also evaluated the predictive value of multivariable risk models, including patient and adenoma characteristics. Concurring with previous reports, we found a close relationship between baseline adenoma findings and advanced adenoma recurrence; number (≥3) and size (≥10 mm) independently increased the risk.6 13 29–31 Villous histology failed to reach statistical significance after adjusting for size, which is consistent with some,24 29 32 but not all,2 12 13 former studies. Considering a high correlation between the two variables, these results should be interpreted with caution and limited numbers of small (<10 mm) villous adenoma (35 cases) could make treating it as a separate risk factor difficult. Of particular importance, high-risk adenoma, by definition of the current guidelines, was the strongest predictor (vs low-risk adenoma, HR=5.95, 95% CI 3.66 to 9.68), indicating that the guidelines are effective in terms of risk stratification. This contrasts with the result from the Polyp Prevention Trial,12 which showed limited discrimination between low-risk and high-risk categories among the self-selected, above average-risk population. Furthermore, our study suggests that known risk or preventive factors for colorectal neoplasia do not necessarily translate into clinically useful predictive guidelines. Among a few prospective studies, contradictory evidence has been reported on age,30 31 gender,2 family history,29 33 obesity,34 35 smoking36 37 and aspirin/NSAID38 or statin use.39 40 In this study, none of these factors showed a significant effect on recurrence of advanced adenoma. Considering a rather short interval of 5 years, additional studies with sufficient duration of such exposure may be required for development of recurrent adenomas.
Major advantages of our prospective study include the large sample size and a comprehensive range of risk variables, resulting in well-powered evaluations on the rare incidence of recurrent advanced adenoma and more detailed risk analysis through multivariate adjustments. In addition, a unique aspect of the study was the inclusion of 1242 adenoma-free controls, which allowed comparison with different degrees of neoplasia or better discrimination between low-risk and high-risk categories. Unlike prior studies, which were conducted in a diagnostic rather than a screening setting, subjects were strictly limited to asymptomatic persons who underwent first lifetime colonoscopy for better assessment of the real-world impact of a surveillance approach for the mass population. An additional strength is high-quality data collection using our large database (Healthwatch version 2.0)14 15 and fully computerised electronic medical records, including accurate information on gastrointestinal symptoms and various risk variables.
The main shortcoming of the study is the single-centre study design, which may limit application of our results to general colonoscopy practice settings. Therefore, further multicentre studies are needed in order to confirm our findings. Another drawback is the possibility of selection bias from health-conscious and financially independent persons with more frequent family history at either enrolment or follow-up. However, this is a problem that is common to all surveillance studies, and family history and socioeconomic status did not appear to be major determinants of recurrent neoplasia (table 3). Other potential limitations are relevant to the fact that by examining colorectal adenomas detected at screening or surveillance colonoscopies, our results pertain to their prevalence rather than incidence. Finally, about half of the low-risk patients underwent repeat colonoscopies within less than 3 years. This might be useful for detection of interval neoplasia overlooked at baseline colonoscopy, but not sufficient for identification of de novo lesions.12 13 In addition, identification and removal of small adenomas during early examinations could have reduced the incidence of advanced adenoma during the subsequent follow-up period, and, thereby, the 5-year rate of advanced adenoma may have been underestimated in these patients.
In summary, our data provide support for a risk stratification scheme using current guidelines; compared with the adenoma-free group, the low-risk group had a very low 5-year incidence of advanced adenoma and did not show increased risk. Therefore, the surveillance interval for low-risk patients could be extended beyond 5 years. Future studies focusing on the safety and cost-effectiveness of a 10-year interval are mandatory. High-risk adenoma along with the number (≥3) and size (≥10 mm) of baseline adenoma were the only predictors for advanced adenoma recurrence, suggesting that colonoscopic surveillance should be targeted at high-risk patients. Considering the early recurrence of advanced adenoma in these patients, standard 3-year follow-up after initial clearing may be appropriate and necessary.
Acknowledgments
The authors gratefully acknowledge the invaluable assistance of the following endoscopists at SNUH Healthcare System Gangnam Center in application of the surveillance protocol as well as meticulous endoscopy procedures: Seon Hee Lim, Jeong Yoon Yim, Chung Hyun Kim, Kyung Ran Cho, Hansoo Kim, Jung Mook Kang and Jong In Yang.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Seoul National University College of Medicine/Seoul National University Hospital Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.