Article Text

Abstract
The British Society of Gastroenterology guidelines on the management of cholangiocarcinoma were originally published in 2002. This is the first update since then and is based on a comprehensive review of the recent literature, including data from randomised controlled trials, systematic reviews, meta-analyses, cohort, prospective and retrospective studies.
- Cholangiocarcinoma guidelines
- cholangiocarcinoma
- hepatocellular carcinoma
- endoscopic retrograde pancreatography
- pancreatic cancer
- gall bladder cancer
- hepatic encephalopathy
- liver imaging
- brain imaging
- MRI
- nuclear magnetic resonance
Statistics from Altmetric.com
- Cholangiocarcinoma guidelines
- cholangiocarcinoma
- hepatocellular carcinoma
- endoscopic retrograde pancreatography
- pancreatic cancer
- gall bladder cancer
- hepatic encephalopathy
- liver imaging
- brain imaging
- MRI
- nuclear magnetic resonance
Background
Development of guidelines
These guidelines on the management of cholangiocarcinoma (CC) were originally published in 2002.1 This is the first update since and is based on a comprehensive review of the recent literature. The recent European HepatoPancreatoBiliary Association Consensus Conference on Cholangiocarcinoma guidelines have also been used as a source.2 Specific recommendations have been graded based on the quality of evidence available. In the absence of significant data, evidence was based on expert opinion. This manuscript has been developed with the support of The British Liver Trust and the UK cholangiocarcinoma charity, the Alan Morement Memorial Fund.
Intent
These guidelines are intended to bring consistency and improvement in the management from first suspicion of CC through to diagnosis and subsequent treatment. As stated in other British Society of Gastroenterology guidelines, patient preferences must be sought and decisions made jointly by the patient and health professional, based on the risks and benefits of any intervention. A multidisciplinary team approach is recommended, and these often complex cases should be managed in specialist centres with the relevant experience. The guidelines should not necessarily be regarded as the standard of care for all patients. Each case must be managed on the basis of individual clinical data.
Levels of evidence
Studies used as a basis for these guidelines are graded according to the quality of evidence using the Oxford Centre for Evidence-based Medicine levels of evidence (table 1).3 Grading of recommendations is as follows:
-
A: consistent level 1 studies.
-
B: consistent level 2 or 3 studies or extrapolations from level 1 studies.
-
C: level 4 studies or extrapolations from level 2 or 3 studies.
-
D: level 5 evidence or inconsistent or inconclusive studies of any level.
Levels of evidence
Epidemiology
CC is the second commonest primary liver tumour worldwide, after hepatocellular carcinoma (HCC).1 ,2 ,4 ,5 Incidence and mortality rates for intrahepatic CC have risen steeply and steadily across the world over the past few decades with concomitant falls in extrahepatic CC rates.4–14 Since the mid-1990s, more deaths have been coded in England and Wales due to CC than to HCC.4 ,5 CC kills approximately 1500 people annually in the UK, with approximately equal numbers of men and women.12 The cause of the rise in CC is unknown and is not explained by improvements in diagnosis.6 ,12–15 There is debate as to whether the rise in intrahepatic CC represents a genuine increase in true parenchymal primary CC. Recent evidence from USA and UK data suggest that rising intrahepatic CC rates partly reflects misclassification of perihilar (‘Klatskin’) tumours being incorrectly coded as intrahepatic instead of extrahepatic.12 The overall incidence and mortality from all CC, however, does appear to be increasing.12
Risk factors
Established risk factors
There are several established risk factors for CC, but these account for <30% of all cases.15–19 Most cases of CC are sporadic. Primary sclerosing cholangitis (PSC), with or without ulcerative colitis, is the commonest known predisposing factor for CC in the Western world (lifetime risk 5–35%).18 In a study of 211 patients with PSC of whom 60% had inflammatory bowel disease (IBD), malignancies were the most frequent cause of death (44%);18 41% of patients developed colorectal cancer (CRC) and 15 (39%) developed CC. Other malignancies included gall bladder cancer (GBC, n=2), pancreatic cancer (n=1), lymphoma (n=3), melanoma (n=1) and gastric cancer (n=1). Median interval between PSC diagnosis and CC was 2.5 years (range 0–9.8 years). The estimated risk of CC after 10 years was 9% with no significant differences in patients with and without IBD.18 In patients with IBD the 10- and 20-year risks for CRC were 14% and 31%, respectively, significantly higher than for non-IBD patients (2% and 2%). CC, cholangitis and age at entry were independent risk factors for the combined endpoint of death or liver transplantation.18
Other established risk factors for CC are summarised in table 2.13–19
Established risk factors for cholangiocarcinoma (CC)
Likely risk factors
Less established but likely risk factors for CC include cirrhosis of any cause and chronic viral hepatitis B or C.19 A combination of recent cohort, population-based, case-control and observational studies from around the world suggest that obesity, diabetes, fatty liver disease, alcohol, smoking, IBD without PSC and polymorphisms of genes coding for carcinogen metabolism, DNA repair, inflammation and biliary transporters may also be risk factors.15–19 Toxins other than Thorotrast have been linked to CC, including dioxins, nitrosamines and vinyl chloride.16
Anatomical classification
The term ‘cholangiocarcinoma’ includes all bile duct cancers (intrahepatic, perihilar and distal extrahepatic).12 ,20 ,21 Up to 20% of all CC are intrahepatic, according to published series, whereas 50–60% are perihilar, involving the bifurcation of the ducts. Perihilar CC are a subset of extrahepatic CC.12 Up to 20% of CC are distal extrahepatic tumours and 5% of tumours are multifocal. Given the differences in their frequency, pathobiology and management, intrahepatic, perihilar and distal extrahepatic CC should be viewed as separate entities.12 ,17
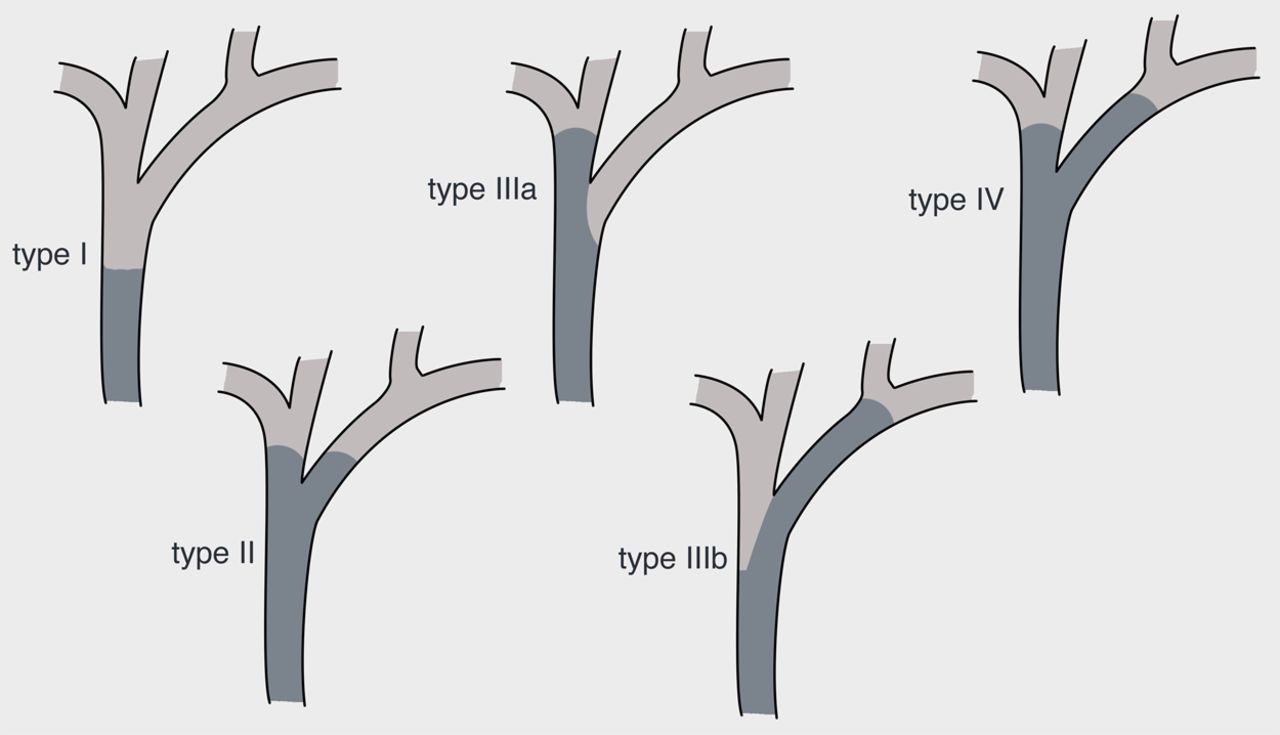
The extent of perihilar CC may be described by the Bismuth–Corlette classification (figure 1)20:
-
Type I: below confluence of left and right hepatic ducts.
-
Type II: reaching confluence but not involving left or right hepatic ducts.
-
Type III: occluding common hepatic duct and either right (IIIa) or left (IIIb) hepatic duct.
-
Type IV: multicentric or bilateral intrahepatic segmental involvement; or involving confluence and both right and left hepatic ducts.

Bismuth–Corlette classification of biliary strictures.
This classification is commonly used but has limitations. It does not take into account vascular encasement and distant metastases. A novel system for reporting perihilar CC was recently proposed based on tumour size, extent of disease in the main bile ducts, involvement of the hepatic artery and/or portal vein, lymph node involvement, distant metastases, volume of the putative remnant liver after resection and underlying liver disease.21 Although more complex than the Bismuth–Corlette classification, the important aim of this system is to standardise the prospective reporting of perihilar CC and help identify factors relevant to the outcome across multiple centres.
Pathology
Histological classifications
There are separate histological classifications of intrahepatic and extrahepatic CC.22–26 The WHO classifications are given in table 3.
WHO classification of biliary malignancies22–26
Macroscopic features of intrahepatic CC
Intrahepatic CCs are whiter and firmer than HCCs as they contain more desmoplastic stroma. They occur more commonly in non-cirrhotic livers than HCCs and are divided into four macroscopic types (table 4). The intraductal type carries the best prognosis and the periductal type carries the worst.
Main macroscopic types of cholangiocarcinoma (CC)
Histological grade
Over 90% of CCs are adenocarcinomas and are classified (1–4) according to the percentage of tumour composed of glandular tissue. Some types of adenocarcinoma are not graded (eg, carcinoma in situ, clear cell adenocarcinoma and papillary adenocarcinoma). Signet ring cell carcinoma is graded as 3 and small cell carcinoma as 4. Although histological grade correlates with postoperative outcome, stage is more important.23–26
Molecular diagnosis
CC is often associated with inactivation of tumour suppressor genes, for example, p53, Smad-4, bcl-2 and p16.15 ,27–33 Mutations in oncogenes have also been described including K-ras, p53, c-erbB-2 and c-neu. Chromosomal aneuploidy has been reported in over 80% of PSC-associated CC. Although mutations can lead to detectable phenotypic changes, molecular profiling in biliary cytology does not currently have an established diagnostic or prognostic role.15 ,27–33
Combined hepatocellular–cholangiocarcinomas
This entity should be distinguished from ‘collision’ tumours in which separate CCs and HCCs are present in the same liver. Combined hepatocellular–CCs are uncommon primary liver tumours accounting for 1–15% of all CCs. These are divided into classical and stem cell types. The latter is divided into the typical subtype in which there are nests of mature-appearing hepatocytes with peripheral clusters of small cells with the immunohistochemical profile of stem/progenitor cells; the intermediate cell subtype with tumour cells intermediate between hepatocytes and cholangiocytes; and the cholangiocellular type with tumour cells growing in an anastomosing pattern. In one series, 28% of HCCs contained cells expressing biliary/progenitor cell markers cytokeratin (CK) 7 and/or CK19.34 ‘Non-classical’ intrahepatic CCs are usually smaller and often arise in chronic liver disease, mostly HCV infection, and/or with significant fibrosis.35
Distinction from other tumours
Distinguishing intrahepatic CC from metastatic adenocarcinoma and other primary liver tumours can be difficult. Accurate differentiation, particularly from foregut metastases (lung, oesophagus, stomach, pancreas), often cannot be made histologically. Other modalities, especially imaging, are essential. Immunohistochemistry panels including CK7, CK19, CK20, CDX-2, TTF-1, oestrogen/progesterone receptors and PSA, depending on clinical context, can be helpful.35 CCs are usually CK7 positive and CK20 negative. In distinguishing HCC from CC, lack of mucin production and expression of HepPar-1, CD10 and glypican-3 by HCC are useful.35
Diagnosis
Clinical features
Perihilar or extrahepatic CCs typically present with features of biliary obstruction (jaundice, pale stool, dark urine and pruritus).1 Cholangitis is unusual without prior biliary instrumentation. CC is usually advanced at presentation, particularly with more proximal intrahepatic and perihilar tumours obstructing one duct. These often present with systemic manifestations of malignancy including malaise, fatigue and weight loss.15 ,36 Some cases are detected incidentally as a result of scans performed for other indications.
Blood tests
No blood tests are diagnostic for CC. Liver function tests often show an obstructive picture.1 Aminotransferases are frequently normal but may be markedly raised in acute obstruction or cholangitis. Prolonged biliary obstruction can cause a reduction in fat soluble vitamins and an increase in prothrombin time. In advanced disease, non-specific markers of malignancy such as albumin, erythrocyte sedimentation rate, C-reactive protein and haemoglobin may be altered.15 ,36
Serum tumour markers
Carbohydrate antigen (CA) 19-9 and CA-125 are the most used serum tumour markers.15 ,36–40 Overall, their sensitivity and specificity are low and they are not helpful for monitoring disease progression.37–40 They may be useful in conjunction with other diagnostic modalities.
CA19-9 is elevated in up to 85% of patients with CC with a sensitivity of 40–70%, specificity of 50–80% and positive predictive value (PPV) of 16–40%, depending on cut-off values.36–38 CA19-9 elevation frequently occurs in PSC and other causes of non-malignant obstructive jaundice, but persistently raised levels of CA19-9 after decompression suggest malignancy.37–40 CA19-9 does not discriminate between CC, pancreatic or gastric malignancy and may also be elevated in severe hepatic injury from any cause. Furthermore, 10% of individuals lack Lewis antigen and cannot produce CA19-9.36–38 ,40
CA-125 is detectable in up to 65% of patients with CC.38 ,40 In a chemotherapy trial setting, a raised baseline CA-125 was found to be prognostic for survival.37 CA-125 is often raised in parenchymal liver disease and may not be helpful in this context.
Novel potential tumour markers linked to CC include Mac-2BP, matrix metalloproteinase-7, insulin-like growth factor 1, interleukin 6, trypsinogen and MUCIN-5AC. None has yet been validated in large clinical studies.
Immunoglobulin G4 (IgG4) cholangiopathy
Immunoglobulin (Ig) G4-associated cholangiopathy, the biliary presentation of a multisystem inflammatory disorder in which affected organs have a lymphoplasmacytic infiltrate rich in IgG4-positive cells, can mimic CC.41 A review of 53 such cases reported that most were men (85%), presented with obstructive jaundice (77%), were associated with autoimmune pancreatitis (92%), increased serum IgG4 levels (74%) and abundant IgG4-positive cells in bile duct biopsy specimens (88%).41 Strictures were confined to intrapancreatic bile ducts in 51% of cases, and proximal extrahepatic/intrahepatic ducts were involved in 49%. Following successful steroid therapy, relapse occurred in 53% of cases after steroid withdrawal. The presence of proximal extrahepatic/intrahepatic strictures was predictive of relapse. Steroid therapy normalised liver biochemistry in 61% and biliary stents were safely removed in 17 of 18 patients.41 IgG4 cholangiopathy should be excluded in suspected cases of CC by testing for increased IgG4 in serum and biliary samples.
Recommendations
-
Diagnosis of CC should not rely solely on serum tumour marker measurements (Grade B).
-
CA 19-9 remains the most widely used serum tumour marker for suspected CC, but does not exhibit high accuracy. It should be measured after biliary obstruction has been relieved (Grade B).
-
IgG4 cholangiopathy should be excluded in suspected cases of CC (Grade B).
Imaging
Imaging is the main diagnostic modality for CC.42–55 Appearances include an intrahepatic mass lesion with characteristics of a metastasis, a hilar stricture or distal bile duct obstruction, with or without a discernible mass. Differentiating between benign and malignant biliary strictures is challenging.
Ultrasonography
CC should be suspected when there is biliary ductal dilation, particularly with a related mass lesion and consistent clinical history. In suspected biliary obstruction, ultrasonography (US) is reliable for excluding gallstones but is operator-dependent and is insufficient alone for investigating suspected CC. For detecting advanced CC in patients with PSC, US offers specificity and negative predictive value of 90%, but sensitivity and PPV are only 50%.42–44 US may miss small tumours and cannot accurately define tumour extent.42–45 Colour-Doppler US may also detect tumour-induced compression or vascular thrombosis.
High resolution/spiral CT
Contrast CT has higher sensitivity for CC detection than US (up to 80%), providing good views of intrahepatic mass lesions, dilated intrahepatic ducts, localised lymphadenopathy and extrahepatic metastases. However, the extent of CC is often not well-defined.42–45 Abdominal lymphadenopathy is common in PSC and does not necessarily indicate metastatic disease.
MRI
Contrast MRI is the optimal imaging investigation for suspected CC.45–48 In addition to avoiding radiation, MRI delineates hepatobiliary anatomy, local extent of duct involvement by MR cholangiopancreatography (MRCP), parenchymal abnormalities including the presence of liver metastases and hilar vascular involvement (MR angiography). However, MRI is inferior to CT for detecting distant metastases, particularly in the lungs and bone.45 ,46
Cholangiography (MRCP, ERCP, PTC)
Cholangiography is essential for assessing the extent of bile duct involvement and resectability.1 ,47 ,49 MRCP is non-invasive, thus avoiding risks of endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic cholangiography (PTC) and avoiding radiation.46–48 In a retrospective study, MRCP had superior sensitivity (96%), specificity (85%) and accuracy (91%) compared with ERCP (80%, 75% and 78%, respectively) for differentiating between CC and benign strictures.47 A UK study comparing MRCP with ERCP in biliary obstruction predominantly relating to gallstone disease found in favour of MRCP with respect to cost-saving and quality of life.48 Similar studies on malignant biliary disease are lacking. ERCP and PTC allow bile sampling for cytology and stent insertion for relief of biliary obstruction. There is no clear evidence that PTC should generally be favoured over ERCP on the basis of the level of obstruction. Although ERCP is usually preferred above PTC, experience of and facilities for PTC should be available in treating centres for cases where ERCP has failed.
Histology and cytology
Although positive histology and/or cytology findings are often difficult to obtain, they are essential for confirming a diagnosis of CC, particularly in patients not proceeding to resection, and for clinical trials. Tumours are usually adenocarcinomas and have prominent desmoplastic stroma. However, except in cases where there is co-existing biliary dysplasia, it may not be possible, even with immunohistochemistry, to differentiate between CC and metastatic tumour. Examples of this include intraductal papillary neoplasm with associated invasive neoplasia, and mucinous cystic neoplasm with associated invasive neoplasia.50 ,51
Standard cytology from brushings at ERCP/PTC is positive in <50% of CC cases, hence negative cytology findings do not exclude malignancy.2 ,15 Combining cytology with biopsy increases the positive yield to 40–70%. Applying fluorescence in situ hybridisation (FISH), which uses fluorescently-labelled DNA probes to detect aneuploidy in cells, reportedly confirmed cancer in 60% of patients in whom standard brush cytology was negative.50 A subsequent study confirmed the ability of FISH to improve the diagnostic accuracy in indeterminate biliary strictures, increasing the sensitivity of brush cytology from 21% to 58%.56 Including the presence of 9p21 deletion increased the sensitivity to 89%. The specificity of FISH was 97% compared with 100% for cytology.56
Endoscopic ultrasound
Endoscopic ultrasound (EUS) allows good views of the distal extrahepatic biliary tree, hilar lesions, gall bladder, regional lymph nodes and vasculature. EUS facilitates fine needle aspiration of distal lesions and nodes which can enhance the sensitivity and PPV of CC detection to nearly 100%. However, the negative predictive value is low, which does not permit exclusion of malignancy following a negative biopsy.52 ,53 The potential risk of tumour seeding has led some centres around the world to advise against EUS fine needle aspiration in potentially resectable tumours. However, this is not the case in most centres. Rates of tumour seeding are unclear, being reported as between 1:10 000 and 1:40 000, although this may be an underestimate.
Positron emission tomography (PET) and PET-CT
In a study comparing CT plus MR versus positron emission tomography (PET)-CT, PET-CT exhibited no advantage for CC diagnosis but did have higher accuracy for detecting regional lymph node and distant metastases.54 PET-CT may have a potential role in preoperative staging, but this needs validating.54 ,55
Cholangioscopy
Given the disappointing accuracy of current diagnostic techniques, interest in cholangioscopy has renewed following technical improvements in endoscopes.57 In a prospective multicentre study, transpapillary cholangioscopy increased the ability to distinguish benign from malignant strictures compared with ERCP alone, and facilitated targeted biopsy.58 Cholangioscopy may be useful in experienced centres and further data are awaited.
Recommendations
-
Patients with suspected CC should have:
-
Combined MRI and MRCP (Grade B)
-
Contrast enhanced high resolution CT (Grade B).
-
-
Invasive cholangiography should be reserved for histological diagnosis, or therapeutic decompression where there is cholangitis, or stent insertion in irresectable cases (Grade B).
-
The above techniques are complementary and may all be necessary as part of a surgical assessment (Grade B).
-
FISH may enhance the diagnostic sensitivity of cytology samples (Grade B).
Staging
CC staging is based on the tumour-node-metastasis (TNM) system. The 7th edition of the TNM classification introduced a specific staging system for intrahepatic CC, separate from HCC, providing better prognostic information.22 ,23 The T category is based on the number of tumour nodules, vascular invasion and direct extension into extrahepatic tissues. Unlike HCC, tumour size is not considered important. A positive resection margin (non-R0 resection) is a very poor prognostic factor.
Although distant spread is late and uncommon in CC, comprehensive staging must be carried out to screen for metastatic disease. CT provides more accurate information for this purpose than MRI. At presentation, up to 50% of patients are lymph node-positive and 10–20% have peritoneal involvement. Most centres consider a staging laparoscopy to exclude local metastatic disease in those considered resectable on imaging. Only approximately 50% of patients with perihilar CC who undergo laparotomy are ultimately suitable for curative resection. In a study of 175 patients with suspected perihilar CC who underwent staging laparoscopy during the past decade, the overall yield and accuracy of staging laparoscopy decreased compared with earlier reports, possibly due to improved imaging techniques during this time period.59 Further studies on the benefit of staging laparoscopy in suspected CC are warranted.
Metastatic adenocarcinoma mimicking CC may arise from several organs, particularly the pancreas, stomach, breast, lung and colon. CC is difficult to differentiate from metastatic adenocarcinoma, particularly if the pathological sample is obtained from outside the biliary tree. Thorough clinical assessment and other investigations are necessary to exclude a primary from elsewhere.1 The extent to which this is pursued will depend on the individual case.60
Recommendations
-
Studies obtained for the initial diagnosis may also provide staging information. However, to rule out metastatic disease, contrast CT of the abdomen, chest and pelvis should be carried out on all patients, particularly if resection is being considered (Grade B).
Recommendations
-
Confirmatory histology and/or cytology at ERCP, laparoscopy or laparotomy should be obtained if at all possible (Grade C).
-
However, due to the risk of tumour seeding, surgical assessment of resectability should be established prior to EUS-guided or percutaneous biopsy attempted (Recommendation Grade B).
-
Laparoscopy may be considered to detect occult metastatic disease (Grade B).
Screening for CC in PSC
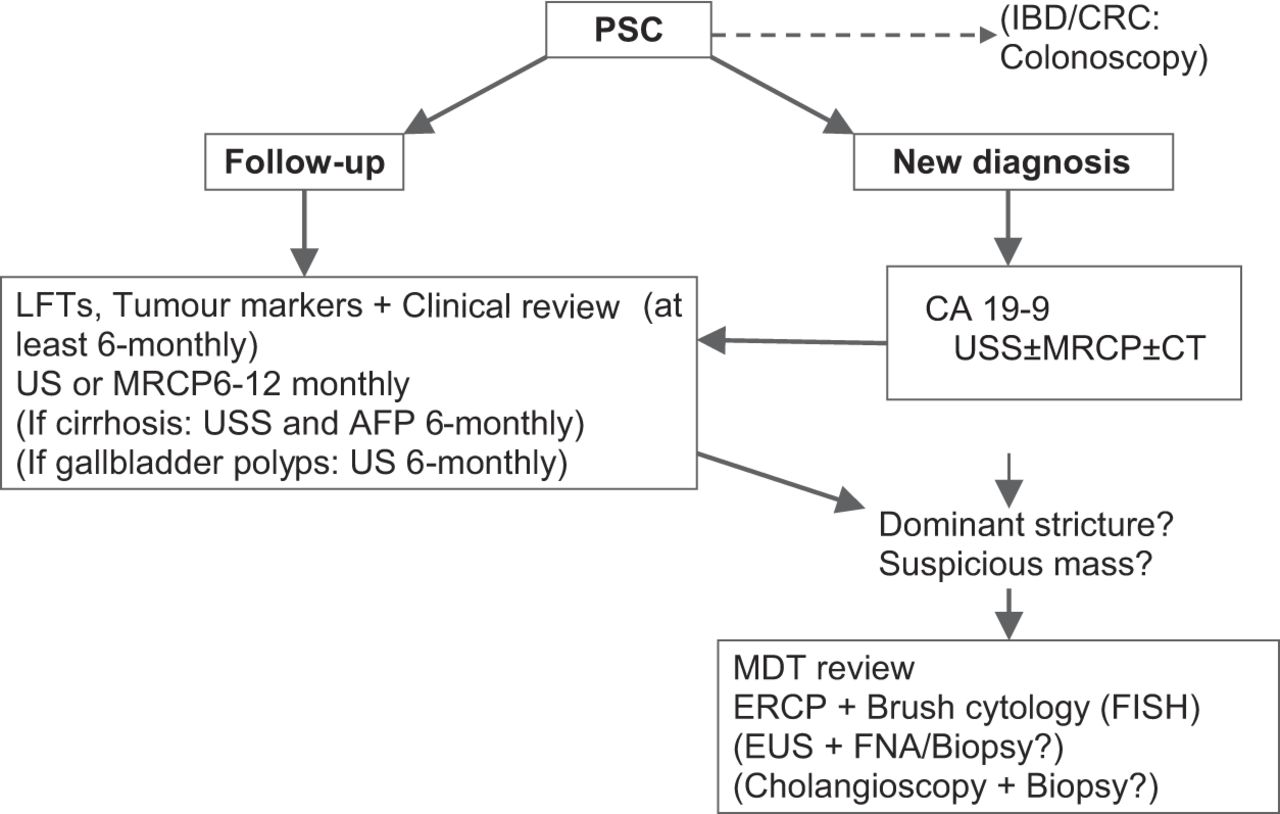
No benefit in screening for CC in PSC has been proven and there is no robust screening test. Nevertheless, most experts agree that early detection of CC in PSC is important to identify cases amenable to curative surgery and to avoid inappropriate liver transplantation.61–66 As well as an increased risk of CC, patients with PSC are also at increased risk of HCC; colorectal, gastric and pancreatic cancers; and malignant gall bladder polyps.62 ,64 ,66 Up to 50% of CCs are diagnosed within 2 years of PSC diagnosis and the subsequent risk of CC is approximately 1% per year.64–66 The severity of liver disease (Child–Pugh or Mayo score) does not appear to be a significant risk factor. Smoking, alcohol, duration of IBD if present, previous CRC/dysplasia and the HLA-DR4, DQ8 haplotype are reported risk factors for malignancy in PSC, but none has been validated as a predictive factor. A suggested algorithm for CC screening in PSC is given in figure 2. This is unproven and based on expert opinion. Regular investigations, including surveillance colonoscopies in patients with PSC and IBD and US for gall bladder lesions, are recommended in both the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD) guidelines.
{kind=link}
{kind=link}
Suggested algorithm for cholangiocarcinoma screening in primary sclerosing cholangitis (Recommendation Grade D). AFP, alpha-fetoprotein; CC, cholangiocarcinoma; CRC, colorectal carcinoma; ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasound; FISH, fluorescence in situ hybridisation; FNA, fine-needle aspiration; IBD, inflammatory bowel disease; MDT, multidisciplinary team; MRCP, magnetic resonance cholangiopancreatography; PSC, primary sclerosing cholangitis; US, ultrasonography.
Role of ursodeoxycholic acid (UDCA)
Small retrospective studies have suggested that ursodeoxycholic acid (UDCA) may reduce the risk of colonic dysplasia and CRC in patients with PSC. No significant protective effect of UDCA on the risk of CC has been demonstrated. Recent guidelines from both EASL and AASLD have concluded that the role of UDCA in PSC is currently unclear and that high-dose UDCA may even be harmful.64–66
Treatment
Surgery
Surgery is the only curative treatment for patients with CC; however, fewer than one-third of patients are resectable at diagnosis.67–73 Five-year survival rates following resection of intrahepatic CC, distal extrahepatic CC and hilar tumours are 22–44%, 27–37% and 11–41%, respectively.67 ,68 ,71–73 Survival depends on local clearance (R0 or R1 status), vascular invasion and lymph node metastases. R0 resection and well-differentiated tumour grading are independently associated with improved survival and lymph node involvement (occurring in 50% at presentation) is associated with reduced long-term survival.67 ,68 ,72 ,73 Peritoneal and distant metastases (10–20% at presentation) are contraindications to surgical resection. In a multivariate analysis, post-resection prognosis correlated most strongly with clinical stage and multiplicity of lesions.73
Resectable tumours
Resection, which should be guided by medical risk rather than age, involves a major operative procedure and requires appropriate surgical and anaesthetic experience. Surgical treatment depends on the site and extent of bile duct involvement by tumour. Intrahepatic CCs are usually treated by resection of the involved segments or lobe of the liver. Distal CCs are managed by pancreatoduodenectomy, as with ampullary or pancreatic head cancers. Major hepatectomy for hilar CCs carries a considerable risk of hepatic insufficiency if there is a small future liver remnant. Portal vein embolisation of the liver lobe to be removed is a safe method for increasing the future liver remnant and permits potentially curative hepatic resection to be carried out.74–76
Liver transplantation for CC
Historically, liver transplantation for CC was associated with rapid recurrence of disease and poor survival rates: around 10% for intrahepatic CC and 25% for extrahepatic CC.77 ,78 Recent studies, however, have reported 5-year survivals of over 70% in patients carefully selected by their response to pre-transplant chemoradiation.79 ,80 This applies to a minority of patients with CC and most of the published data so far have been from a single centre in the USA. However, a recent study analysed data from 12 transplant centres in the USA. Each had treated at least three patients with perihilar CC using varying protocols of neoadjuvant chemoradiation followed by liver transplantation between 1993 and 2010. Two hundred and eighty-seven patients were treated and 71 dropped out before transplantation. The overall intent-to-treat survival rate was 53% 5 years after treatment and the post-transplant recurrence-free survival rate was 65%. Patients with tumour mass >3 cm, transperitoneal tumour biopsy, metastatic disease or with a prior malignancy had significantly shorter survival times. Although most patients (n=193) came from one centre, the other 11 centres had similar survival times.81
Recommendations
-
For perihilar CC, the Bismuth classification is a guide to the extent of surgery required (aim is tumour-free margin of >5 mm). Surgical treatment is principally as follows (Grade B):
-
For types I and II: en bloc resection of the extrahepatic bile ducts and gall bladder, regional lymphadenectomy and Roux-en-Y hepaticojejunostomy.
-
For type III: as above plus right or left hepatectomy.
-
For type IV: not usually resectable but extended right or left hepatectomy may be feasible, dependent on biliary anatomy.
-
-
Segment 1 of the liver may preferentially harbour metastatic disease from hilar CC and removal should be considered with stages II–IV.
-
Intrahepatic CCs are managed by segmental or lobe resection.
-
Distal CCs are treated by pancreato-duodenectomy.
-
Increasing data suggest that liver transplantation for CC can be successful in rigorously selected patients undergoing neoadjuvant therapy in highly specialised centres.
Adjuvant therapy for resectable tumours
There is no current evidence to support the use of adjuvant chemotherapy or radiotherapy. Appropriate trials are needed to address this issue. The largest trial currently accruing is the BILCAP trial.82
Palliative procedures
Surgical resection with palliative rather than curative intent is unproven. Symptoms from biliary obstruction in irresectable disease may be palliated by biliary stenting rather than a surgical bypass. Stent placement resulting in adequate biliary drainage improves survival. Surgical bypass has not been demonstrated to be superior to stenting. Close liaison between oncological, palliative care and surgical teams is essential.
Reporting surgical specimens
Surgical resection specimens should be reported systematically, for example, according to Royal College of Pathologists’ guidelines.26 The final report should include the following information:
Tumour
-
Histological type
-
Histological grade
-
Extent of invasion (according to the TNM system)
-
Blood/lymphatic vessel invasion
-
Perineural invasion: this is common and has prognostic significance.
Margins
These must be adequately sampled because local recurrence is related to involvement of the margins. This is particularly important because extrahepatic CC may be multifocal in up to 5% of cases.
Regional lymph nodes
To stage lymph nodes accurately, the node groups must be specifically identified. Peripancreatic nodes located along the body and tail of the pancreas are considered sites of distant metastasis.
Additional pathological findings
These must be noted if present (eg, carcinoma in situ, sclerosing cholangitis).
Metastases
Metastases to other organs or structures should be reported.
Biliary decompression and stents
Stenting prior to surgery
Preoperative biliary drainage is controversial. It has been associated with bacteriobilia and fungal colonisation, higher rates of postoperative sepsis, wound infection, longer hospital stay and increased cost.83–90 A meta-analysis of preoperative biliary drainage for obstructive jaundice included four trials (n=235) comparing PTC-biliary drainage with direct surgery and one trial (n=85) comparing preoperative endoscopic drainage with direct surgery.91 Overall, there were no significant differences in mortality, morbidity or complications between the preoperative biliary drainage and the direct surgery groups. One of the included studies found that preoperative endoscopic biliary drainage prolonged hospital stay and increased cost. However, the overall strength of evidence was deemed low due to the poor quality of the included trials.91 A multicentre randomised trial comparing preoperative biliary drainage with surgery alone for patients with pancreatic cancer and obstructive jaundice included 206 patients; 106 were randomly assigned to undergo preoperative biliary drainage for 4–6 weeks (primarily by ERCP) followed by surgery, and 96 to surgery alone within 1 week of diagnosis.92 The rates of serious complications were 39% in the early surgery group and 74% in the biliary drainage group (RR in the early surgery group 0.54, p<0.001). Mortality and the length of hospital stay did not differ between the groups.92 Although most of the data relate to obstructive jaundice from cancers other than CC, on current evidence the routine use of preoperative biliary drainage cannot be recommended. In patients who are severely malnourished or have acute suppurative cholangitis and in those in whom major hepatic resection is planned, preoperative drainage may be beneficial.93 Rigorously designed randomised controlled trials (RCTs) with appropriate sample sizes are required with respect to CC.
Recommendation
-
Routine biliary drainage before assessing resectability or preoperatively should be avoided except for certain situations such as acute cholangitis, with modification of antibiotic prophylaxis according to patient characteristics and local microbiological specialist advice (Grade B).
Stents for palliation of jaundice
Most patients with CC have unresectable disease. In such patients, a study from the USA found that endoscopic stenting cost significantly less and was associated with longer survival than surgical treatment (19 vs 16.5 months), suggesting that endoscopic stenting is the procedure of choice for palliative biliary drainage.94 Most initially inserted stents are plastic. Stents of diameter ≥10Fr usually remain patent for approximately 3 months. Narrower stents have lower patency rates and should not be used routinely. Covered removable self-expanding metal stents (SEMS) may also be used and some specialists prefer SEMS in patients who are candidates for neoadjuvant therapies.95
Biliary drainage by the percutaneous route can be effective, particularly for high strictures involving segmental ducts. A multicentre retrospective Korean study of 85 patients with newly diagnosed advanced hilar CC who did not undergo surgery, chemotherapy or radiotherapy compared percutaneous versus endoscopic SEMS insertion.96 Successful biliary decompression was significantly higher in the percutaneous group than in the endoscopic group (93% vs 77%, p=0.049). Procedure-related complications, median survival and stent patency duration were similar in both groups.96
Bilateral versus unilateral stents in hilar CC/advanced malignant biliary strictures
Bilateral versus unilateral stent insertion for hilar strictures is controversial. Early small studies reported that 30-day mortality and cholangitis were lower in patients who underwent bilateral compared with unilateral drainage for hilar strictures.88 ,89 ,93 ,97 Failure to drain opacified lobes is associated with a poorer outcome. Post-stent cholangitis can be reduced by minimising the amount of contrast injected. Careful imaging with MRCP to plan endoscopic stent placement in complex hilar tumours may guide optimum stent placement. In particular, non-atrophic areas of the liver with a likelihood of providing viable bile production should be considered for drainage.93 Bilateral stent insertion is technically challenging and should not be carried out routinely. If contemplated, it should be performed in expert centres.
Metal versus plastic stents
Most patients with malignant biliary obstruction treated by plastic stents will require at least one stent change. Metal stents have several advantages over plastic stents.98–102 They have a relatively narrow delivery system (8Fr) with a wider diameter on deployment (10 mm). SEMS are also available that are 8 mm on deployment, which may help in stent selection, depending on the patient's anatomy. The patency rates of metal stents are significantly greater than those of plastic stents (up to 12 months vs 3 months). Metal stents are associated with fewer ERCPs, a shorter hospital stay and fewer complications than plastic stents in patients who survive more than 6 months. A retrospective study of unresectable hilar CC in the USA found that SEMS were more cost-effective than plastic stents for palliative drainage.102 Other studies have also found that metal stents are more cost-effective in patients surviving more than 4 months. Plastic stents may be satisfactory for patients surviving less time than this.
Disadvantages of uncovered metal stents include being difficult to remove endoscopically and potentially making surgery more technically challenging. Metal stents should not be deployed for biliary strictures prior to a multidisciplinary team decision on resectability. Tumour growth through the mesh of metal stents may lead to further problems with biliary obstruction and sepsis. This may be overcome by inserting plastic stents through the lumen of the metal stent, or placement of a further mesh metal stent where technically possible.
Covered versus uncovered stents
Covered biliary metal stents have recently been developed to prevent tumour ingrowth.103–106 A prospective RCT comparing covered and uncovered stents in irresectable malignant distal biliary obstruction found no difference in survival but a longer time to obstruction in the group with covered stents, who overall had fewer interventions and lower costs. Patency was higher in pancreatic cancer and in lymphadenopathy-associated obstruction compared with biliary malignancy, but numbers of the latter were small.103 Another RCT demonstrated improved survival in patients with extrahepatic CC who percutaneously received a covered (243 days) compared with an uncovered stent (180 days), with comparable cost and complication rates.105 The incidence of stent dysfunction was significantly lower in the covered stent group.105 The largest study so far in this area was a multicentre unblinded RCT of 400 patients with irresectable distal malignant biliary obstruction. Patients were randomised to ERCP with insertion of a covered or uncovered metal (nitinol) stent.106 There were no significant differences in stent patency time, patient survival time or complication rates between covered and uncovered metal stents. However, covered stents migrated significantly more often than uncovered stents and tumour ingrowth was more frequent with uncovered stents.106
Complications of stenting
Complications of stents include complications of endoscopy and sedation. Following palliative stenting, patients can die from recurrent sepsis, biliary obstruction and stent occlusion, as well as disease progression. Acute cholecystitis from covered stents is another recognised complication.
Photodynamic therapy
In an early prospective open-label trial, 39 patients with unresectable CC were randomised to stenting alone or stenting and photodynamic therapy (PDT).107 The PDT group had a significantly higher median survival (493 days vs 98 days).107 PDT was further evaluated in the larger UK Photostent-02 trial in which 92 patients with histologically or cytologically confirmed biliary tract cancer (BTC) were randomised to receive either PDT plus stenting or stenting alone.108 Overall survival was 5.6 months for PDT plus stenting and 8.5 months for stenting alone (HR 1.8, p=0.027). Nine patients (20%) in the PDT/stenting arm and 19 (41%) in the stenting alone arm received subsequent chemotherapy. Although overall survival was significantly improved among those who had chemotherapy compared with those who did not (11.1 vs 4.8 months, p=0.001), adjusting for this only reduced the PDT/stenting HR from 1.8 to 1.6, suggesting that failure to receive subsequent chemotherapy did not completely explain the excess risk from PDT.108
Recommendations
-
Initial stent insertion for biliary obstruction should be plastic or covered SEMS, particularly if the diagnosis and resectability are undecided (Grade C).
-
If the initial plastic stent becomes blocked, replacement with a metal stent is favoured if the estimated survival is expected to be >4 months (Grade B).
-
Covered stents cannot be recommended for routine use based on current evidence (Grade B).
-
Surgical bypass should be reconsidered in patients with a good estimated life expectancy where stenting has failed (Grade C).
-
Photodynamic therapy cannot be recommended for routine use based on the most recent data (Grade A).
Oncological approaches
Given that most patients present with unresectable disease and at least half have lymph node metastases, oncological approaches could potentially have a beneficial impact on many patients.109–116 As a general guide from trial data, patients who are relatively fit and are not deteriorating rapidly should be treated early in the course of their disease rather than waiting for clinical progression. The performance status (PS) is a major prognostic factor. Patients should have a WHO or ECOG PS of 0 or 1 after optimisation of biliary drainage. Even achieving stable disease in patients on therapy correlates with length and quality of life. This is particularly important because of the frequent difficulty in confirming objective radiological responses, particularly in the perihilar area. Good symptom control is paramount and requires multidisciplinary team input and, for many patients, palliative care is immediately appropriate.
Chemotherapy
Locally advanced or metastatic inoperable CC and GBC (Evidence level 1a)
Until recently, chemotherapy for CC had poor results and studies were small and disparate. In 2010, a new standard of care in unresectable BTC was established with the reporting of the UK NCRI ABC-01 and ABC-02 trials.39 ,113 ,114 ABC-02 is the largest randomised phase III study reported in BTC to date. Four hundred and ten patients with locally advanced or metastatic CC, or gall bladder or ampullary cancer were randomised to receive 24 weeks of either cisplatin plus gemcitabine (CisGem) or gemcitabine (Gem) alone.39 After a median follow-up of 8.2 months, the median overall survival was 11.7 months for the CisGem group (n=204) and 8.1 months for the Gem group (n=206), HR 0.64 (95% CI 0.52 to 0.80, p<0.001). The median progression-free survival was 8.0 months for the CisGem group versus 5.0 months for the Gem group (p<0.001). Patients in the CisGem group also had a significantly improved tumour control rate (81.4% vs 71.8%, p=0.049). Overall toxicity was similar between the arms, with a slight excess in clinically non-significant haematological toxicities for the CisGem group.39 The small proportion of patients with PS 2 in this study did not gain a survival advantage. Similarly, there was no clear advantage for the small subset of patients with ampullary cancer. However, patients with GBC (about 30% of the total cohort and well-balanced between the arms) derived as much benefit as the patients with CC. The efficacy of CisGem has been validated in the Japanese equivalent of the ABC-02 study, which reported similar outcomes.114 An investigation in the USA comparing direct medical costs, patient time costs and quality-adjusted life years in BTC found CisGem treatment to be cost-effective compared with Gem monotherapy.115
There are encouraging reports of several patients being successfully downstaged with neoadjuvant chemotherapy and converted to operability in phase II studies, with occasional long-term survivors. Regimens combining chemotherapy with newer targeted biological agents are now being tested.
Adjuvant therapy
There is currently no evidence to support postoperative adjuvant therapy for CC outside a trial setting. A phase III RCT evaluated postoperative adjuvant therapy with mitomycin C and 5-fluorouracil versus surgery alone in resected pancreatobiliary carcinoma.116 A significant survival benefit for patients with GBC was found. However, the trial was underpowered to show a survival advantage in CC and there was no significant survival advantage for patients with BTC overall. The UK NCRI BILCAP study is currently accruing and compares postoperative capecitabine monotherapy with observation alone. The trial is expected to report in 2014.82
Radiotherapy
External beam radiotherapy and chemoradiation
There is currently no evidence to support the routine use of radiotherapy postoperatively or for unresectable disease. Radiotherapy may have important palliative value—for example, for localised metastases or uncontrolled bleeding.109–112 The role of chemoradiation remains to be established in RCTs.
Local radiation techniques: intraoperative or intraductal brachytherapy
A small non-randomised retrospective study of metal stent insertion combined with external beam radiotherapy versus stent insertion alone showed a longer survival in the combination group (10.6 vs 6.4 months) and also longer stent patency (9.8 vs 3.7 months).109 However, overall patency rates were shorter than previously reported for metal stents. A large epidemiological retrospective study of 17% of 3839 patients with intrahepatic CC (on the USA SEER database) demonstrated a small survival benefit for radiotherapy plus surgery compared with radiotherapy alone (11 vs 7 months).110 A similar study in 4758 patients with extrahepatic CC suggested that palliative radiotherapy prolonged survival; however, the benefit associated with surgery and/or radiotherapy was not significant after controlling for potential confounders.111 In a small prospective randomised study of perihilar CC, 21 patients with percutaneous stenting followed by intraluminal Ir-192 brachytherapy and external radiotherapy were compared with 21 patients with stenting only. The combination group had a significantly improved mean survival compared with the group with stenting alone (388 vs 298 days).112 The value of intraoperative radiotherapy or brachytherapy is unproven and has not been shown to be superior to standard chemotherapy, chemoradiation or stenting alone.
Recurrent bile duct cancer
The prognosis for any treated patient with progressing, recurring or relapsing bile duct cancer is poor. Further treatment depends on several factors including prior treatment, site of recurrence, specific symptoms and PS. Relief of recurrent jaundice usually improves quality of life. Clinical trials should be considered if appropriate.
Locoregional therapies
Recent literature suggests an emerging role for locoregional therapies in intrahepatic CC, including transcatheter arterial chemoembolisation, radiofrequency ablation and transarterial hepatic yttrium-90 ((90)Y) radioembolisation, which have previously been successfully used for the treatment of HCC and colorectal liver metastases.117–125
Transcatheter arterial chemoembolisation (TACE)
In a retrospective matched series of transcatheter arterial chemoembolization (TACE, n=72) versus supportive therapy alone (n=83) for unresectable intrahepatic CC, survival was significantly improved in the TACE group (median 12.2 vs 3.3 months, p<0.001). Toxicities were significantly higher in the TACE group but no patients died within 30 days following TACE.117 In another retrospective analysis of 114 patients with intrahepatic CC who underwent curative resection, adjuvant TACE was given in 57 cases. In patients with poor prognostic factors (tumour size >5 cm, TNM stage III/IV), 3- and 5-year survival rates were 34% and 14% in the adjuvant TACE group compared with 0% and 0% in the non-TACE group, respectively (p<0.001). TACE had no effect on survival in patients without poor prognostic factors.118
Radiofrequency ablation
Several recent small studies have suggested that percutaneous US-guided thermal ablation for unresectable intrahepatic CC is safe and potentially effective, particularly for primary and relatively smaller tumours.120–124 In a Chinese study, 18 patients (8 primary and 10 recurrent cases after resection) with 25 intrahepatic CC nodules underwent US-guided thermal ablation with curative intention.120 Complete ablation was achieved in 23 (92%) nodules (diameter 0.7–4.3 cm) and incomplete ablation was found in the remaining two tumours which were larger (6–7 cm). There were no treatment-associated deaths. Overall survival rates at 36 and 60 months were 30% and 30%, respectively. The patient source (primary or recurrent case, p=0.001) and the number of nodules (p=0.038) were significant prognostic factors for recurrence-free survival. Survival rates for primary intrahepatic CC at 36 and 60 months were 63% and 63%, respectively.120
Radioembolisation
Radioembolisation using (90)Y microspheres was assessed in 33 patients with unresectable intrahepatic CC and appeared safe.125 Median overall survival was 22 months and time-to-progression (TTP) was 9.8 months. Survival and TTP were significantly prolonged in patients with ECOG 0 versus ECOG 1 or 2 (median overall survival 29.4, 10 and 5.1 months, respectively; TTP 17.5, 6.9 and 2.4 months, respectively). Tumour burden and tumour response were other predictors of survival (p<0.001).125
The emerging data for locoregional therapies in unresectable CC are encouraging, but larger studies are required to determine their efficacy.
Recommendations
-
Gemcitabine and Cisplatin combination chemotherapy is recommended for locally advanced or metastatic unresectable CC (Grade A).
-
Further data on specific disease subsets such as perihilar CC are warranted to identify the best treatment combination options for different subcategories of CC (Grade B).
-
All operable patients should be offered adjuvant treatment trials. Similarly, all patients who have inoperable tumours or who are operable but have not been rendered disease-free, or those patients with recurrences should be actively encouraged to participate in chemotherapy and/or radiotherapy clinical trials (Grade B).
-
Patients with PS ≥2 after adequate drainage and appropriate treatment of intercurrent sepsis should be considered for palliative care (Grade B).
-
Locoregional therapies such as radioembolisation and TACE need prospective randomised data to assess their true value.
Revision of guidelines
We recommend that these guidelines are regularly audited and we request feedback from all users. These guidelines should be revised in the light of new evidence that is likely to improve management.
Acknowledgments
We are grateful for input and support from The British Liver Trust and the Alan Morement Memorial Fund.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.