Article Text

Abstract
Objective In the revised Atlanta classification of acute pancreatitis, the term necrotising pancreatitis also refers to patients with only extrapancreatic fat necrosis without pancreatic parenchymal necrosis (EXPN), as determined on contrast-enhanced CT (CECT). Patients with EXPN are thought to have a better clinical outcome, although robust data are lacking.
Methods A post hoc analysis was performed of a prospective multicentre database including 639 patients with necrotising pancreatitis on contrast-enhanced CT. All CECT scans were reviewed by a single radiologist blinded to the clinical outcome. Patients with EXPN were compared with patients with pancreatic parenchymal necrosis (with or without extrapancreatic necrosis). Outcomes were persistent organ failure, need for intervention and mortality. A predefined subgroup analysis was performed on patients who developed infected necrosis.
Results 315 patients with EXPN were compared with 324 patients with pancreatic parenchymal necrosis. Patients with EXPN less often suffered from complications: persistent organ failure (21% vs 45%, p<0.001), persistent multiple organ failure (15% vs 36%, p<0.001), infected necrosis (16% vs 47%, p<0.001), intervention (18% vs 57%, p<0.001) and mortality (9% vs 20%, p<0.001). When infection of extrapancreatic necrosis developed, outcomes between groups were equal (mortality with infected necrosis: EXPN 28% vs pancreatic necrosis 18%, p=0.16).
Conclusion EXPN causes fewer complications than pancreatic parenchymal necrosis. It should therefore be considered a separate entity in acute pancreatitis. Outcome in cases of infected necrosis is similar.
- Pancreas
- pancreatitis
- necrosis
- peripancreatic
- extrapancreatic
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Patients with acute pancreatitis can develop extensive extrapancreatic necrosis without developing necrosis of the pancreatic parenchyma as determined on contrast-enhanced CT.
What are the new findings?
-
Patients with extrapancreatic necrosis only have a better prognosis than patients with pancreatic parenchymal necrosis. Outcome in case of infected necrosis is similar.
How might it impact clinical practice in the foreseeable future?
-
The revised Atlanta classification of acute pancreatitis will distinguish necrotising pancreatitis into extrapancreatic necrosis only and pancreatic parenchymal necrosis.
-
To accurately compare outcomes, future studies in necrotising pancreatitis should report the number of patients with extrapancreatic necrosis only.
Introduction
In a disease as complex as acute pancreatitis, correct terminology and clear definitions are essential in interdisciplinary communication among treating physicians as well as in reports of clinical research. In the 1992 Atlanta classification, necrotising pancreatitis was defined as diffuse or focal area(s) of non-viable pancreatic parenchyma typically associated with extrapancreatic fat necrosis or non-enhanced pancreatic parenchyma >3 cm in length or involving >30% of the area of the pancreas.1 This definition did not include patients with extrapancreatic necrosis only (EXPN). Over the years a few small case series have described patients undergoing surgical removal of extensive extrapancreatic necrosis while the pancreatic parenchyma appeared to be viable.2–5 Since these first reports, no prospective study has compared the outcome of patients with EXPN with patients with pancreatic parenchymal necrosis (or, in short, pancreatic necrosis) in a large consecutive cohort.
The primary aim of this study was to investigate whether the rate of complications and mortality of patients with EXPN differs from that of patients with pancreatic necrosis with or without extrapancreatic necrosis. The second aim was to determine whether the rates of complications differ between patients with EXPN or pancreatic necrosis who develop infected necrosis.
Methods
Patients
This was a post hoc analysis of a database of a prospective multicentre cohort study.6 Patients with acute pancreatitis were included between March 2004 and November 2008 in all eight Dutch university medical centres and 13 large teaching hospitals of the Dutch Pancreatitis Study Group. During the study period, all patients admitted with acute pancreatitis were screened for eligibility for the Dutch PROPATRIA and PANTER trials.7 ,8 Regardless of eligibility for the randomised trials, patients were asked for informed consent for registration in the prospective database on admission.
Details on the general treatment protocol, data collection and definitions of outcomes (eg, definition of primary infected necrosis or organ failure) of this cohort have been described previously.6 Infected necrosis was defined as a positive culture of pancreatic or extrapancreatic necrosis obtained by means of fine needle aspiration or from the first drainage procedure or first necrosectomy, or the presence of gas in the peripancreatic collection on contrast-enhanced CT. In the current study, new analyses were performed specifically to compare patients with pancreatic necrosis (with or without extrapancreatic necrosis) with patients with EXPN as determined on CECT. Patients with interstitial pancreatitis were excluded. The following baseline parameters were assessed: age, aetiology, American Society of Anaesthesiologists (ASA) classification on admission, Acute Physiology, Age, and Chronic Health Evaluation (APACHE)-II score on admission, Imrie or Modified Glasgow score, C reactive protein (CRP) during the first 48 h of admission and number of transferred patients from other hospitals to one of the hospitals of the Dutch Pancreatitis Study Group. The following outcome parameters were assessed: organ failure, multiple organ failure, development of sterile or infected necrosis, conservative treatment or intervention and mortality.
The study was conducted in accordance with the principles of the Declaration of Helsinki and was investigator-initiated and investigator-driven. The ethics review board of each participating hospital approved the study. Patients or their legal representatives gave written informed consent. We adhered to the STROBE statement guidelines for reporting on observational cohort studies.9
Definitions of extrapancreatic necrosis and pancreatic necrosis
Pancreatic necrosis was defined as focal or diffuse non-enhancement of the pancreatic gland as determined on CECT. Extrapancreatic necrosis only without pancreatic necrosis (ie, EXPN; figure 1) was defined as extrapancreatic morphological changes exceeding fat stranding with complete enhancement of the pancreatic parenchyma without signs of focal or diffuse non-enhancement able to be determined on the final CECT of hospitalisation or before any intervention. Patients with both pancreatic and extrapancreatic necrosis were included in the pancreatic necrosis group (figure 2). Patients with pancreatic necrosis without extrapancreatic necrosis, which is very rare, were also included in the group of patients with pancreatic necrosis.
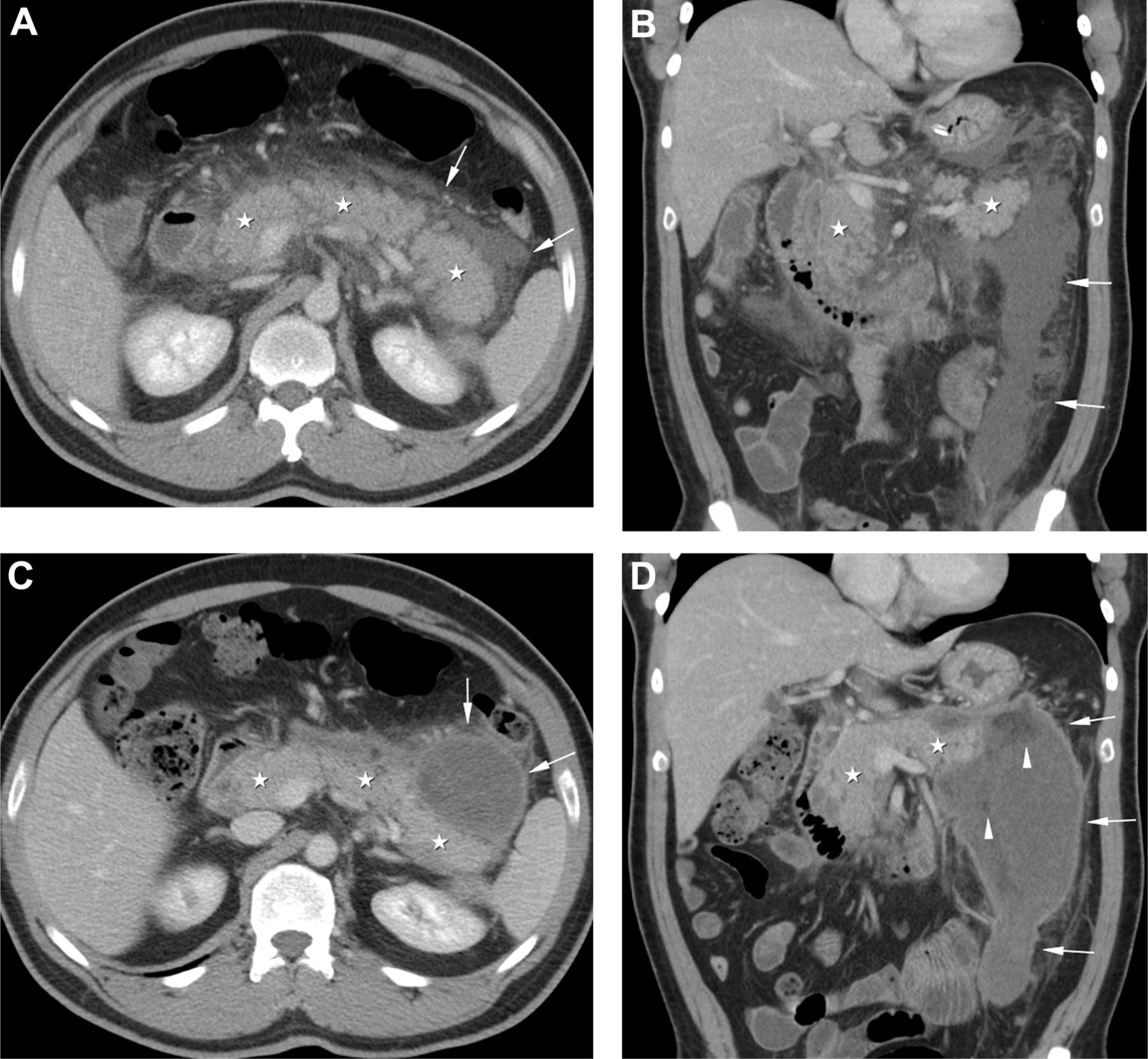
Extrapancreatic necrosis. (A, B) Axial and coronal reconstructed contrast-enhanced CT scans in a 37-year-old man with alcohol-induced pancreatitis 6 days after onset of symptoms. There is normal enhancement of the pancreatic parenchyma (white asterisks) with a poorly marginated peripancreatic collection (arrows) extending into the left anterior pararenal compartment. (C, D) Axial and coronal reconstructed contrast-enhanced CT scans 2 months later, again showing a normal enhancement of the pancreas surrounded by a well encapsulated heterogeneous peripancreatic collection (arrows) with areas of non-liquid (fat) densities (arrowheads) in the left anterior pararenal compartment. During surgery a large amount of necrotic material was debrided and pus was drained. The patient recovered uneventfully with preservation of normal pancreatic function.

Acute necrotising pancreatitis. Axial contrast-enhanced CT scan in a 45-year-old woman with acute biliary pancreatitis. There is non-enhancement of the neck and part of the body of the pancreas (white asterisk) indicative of parenchymal necrosis with normal enhancement of the tail of the pancreas (black asterisk).
Evaluation of imaging
CECT generally was performed approximately 7 days after admission. In patients with clinical deterioration or without clinical improvement, additional CECTs were performed. In patients participating in the PROPATRIA trial, a CECT after 7–10 days was part of the protocol. Radiologists in the participating centres assessed the CECT for the presence or absence of necrotising pancreatitis. Based on their evaluation, patients were included in the prospective database. After closure of the database following completion of the PANTER trial, all CECTs performed during and after hospitalisation were reviewed by a single experienced abdominal radiologist (TLB) who was unaware of the patients' clinical background, possible interventions and the initial radiology report. Because extrapancreatic or parenchymal necrosis can be missed on CECTs performed early in the disease course, all CECTs performed in each patient were reviewed. The final decision on the presence or absence of EXPN or pancreatic necrosis was based on the final CECT of hospitalisation or before any intervention.
Statistical analysis
Continuous data are presented as median with interquartile range (IQR). Differences were tested with the Mann–Whitney U test. Proportions were compared by the χ2 test, the Fisher exact or the linear-by-linear association test, as appropriate. To assess whether EXPN is an independent predictor of clinical outcome, multivariable regression analysis was performed adjusting for potential confounders (eg, prognostic variables on admission such as age). The following clinical outcomes were analysed: persistent organ failure, persistent multiple organ failure, infected necrosis, the need for intervention and mortality. EXPN was entered into the model as the main factor. As co-variables, all prognostic variables that were potentially different between patients with EXPN and those with pancreatic necrosis on admission in univariable analysis (p<0.2) were included. The results are reported as adjusted odd ratios (ORs) with 95% confidence intervals (CIs). A two-sided p<0.05 was considered statistically significant. Analyses were performed with SPSS V.15.0 (SPSS).
Results
Patients
Of the 639 patients included in the prospective database, 315 patients (49%) had EXPN (determined on CECT) and 324 patients (51%) had signs of pancreatic necrosis (with or without extrapancreatic necrosis) (figure 3). Only four of the 639 patients (0.6%) had pancreatic necrosis without any signs of peripancreatic necrosis and these patients were included in the pancreatic necrosis group. Patients with interstitial pancreatitis were excluded. Baseline characteristics are shown in table 1. No differences were seen in age, sex, aetiology, ASA classification and predicted severity based on APACHE-II scores and CRP levels. The median Imrie score at 48 h after admission was higher in patients with pancreatic necrosis (4 vs 3, p<0.001). The percentage of transferred patients was also higher in patients with pancreatic necrosis (36% vs 13%, p<0.001).

{kind=link}
{kind=link}
{kind=link}
Study population.
Admission characteristics of patients with extrapancreatic necrosis only (EXPN) compared with patients with pancreatic parenchymal necrosis
Use of CECT
A median number of 2 (IQR 4–7) CECTs were performed in each patient (table 1). Patients with EXPN were scanned less frequently than those with pancreatic necrosis (median 2 (IQR 1–4) vs 6 (IQR 3–10), p<0.001). The overall median time between onset of symptoms and the final CECT of hospitalisation or before any intervention was 14 days (IQR 7–46). Patients with EXPN had their final CECT earlier than patients with pancreatic necrosis (median 9 days (IQR 5–21) after admission vs 34 days (IQR 9–71), p<0.001).
Outcomes
The different outcomes of patients with pancreatic necrosis and EXPN are presented in table 2. All outcomes occurred less often in patients with EXPN. More specifically, patients with EXPN had a significantly lower risk of developing single or multiple organ failure. Twice as many patients with pancreatic necrosis developed persistent organ failure during admission (21% vs 45%, p<0.001). Persistent multiple organ failure was also seen in twice as many patients with pancreatic necrosis (15% vs 36%, p<0.001). Patients with EXPN had a lower risk of developing infected necrosis (16% vs 47%, p<0.001). The need for intervention was lower in patients with EXPN (18% vs 57%, p<0.001). Finally, the death rate in patients with EXPN was significantly lower (9% vs 20%, p<0.001).
Outcome of patients with extrapancreatic necrosis only (EXPN) compared with patients with pancreatic parenchymal necrosis
After adjustment for potential confounding factors with multivariable regression, patients with EXPN still had better clinical outcomes. After adjusting for male sex, Imrie score and transferred patients, EXPN was independently associated with a lower risk of organ failure (adjusted OR 0.53, CI 0.37 to 0.78, p<0.001), multiple organ failure (adjusted OR 0.48, CI 0.32 to 0.72, p<0.001), infected necrosis (adjusted OR 0.30, CI 0.20 to 0.45, p<0.001), any intervention (adjusted OR 0.25, CI 0.17 to 0.38, p<0.001) and mortality (adjusted OR 0.59, CI 0.35 to 0.97, p=0.04).
Subgroup analysis of primary infected necrosis
The subgroup of 202 patients who developed infected necrosis was separately analysed. There were no significant differences between patients with infected EXPN and patients with infected pancreatic necrosis regarding all the aforementioned clinical outcomes (table 3). The incidence of persistent organ failure (55% of EXPN vs 60% of pancreatic necrosis, p=0.62) and persistent multiple organ failure (41% of EXPN vs 46% of pancreatic necrosis, p=0.63) was similar. Almost all patients with infected necrosis required an intervention (92% vs 94%, p=0.74). The likelihood of recovery following percutaneous catheter drainage without the need for additional necrosectomy was 28% versus 23% (p=0.57). Mortality did not differ significantly between the two groups (28% vs 18%, p=0.16).
Outcome in subgroup of patients with primary infected extrapancreatic necrosis only (EXPN) or pancreatic parenchymal necrosis
Discussion
This study, evaluating the clinical outcome of a large prospective cohort of patients with necrotising pancreatitis, shows that patients with EXPN (as determined on CECT) have a better prognosis than patients with pancreatic necrosis. However, in case of infected necrosis, rates of complication and mortality are similar. To our knowledge, this is the first report on clinical outcomes of EXPN in a large unselected cohort of patients with acute necrotising pancreatitis.
The presence of extrapancreatic necrosis as a separate entity in the absence of pancreatic necrosis was first recognised by Howard and Wagner in 1989.2 In a group of 13 patients, pancreatography after debridement of necrosis showed an intact pancreatic duct in most patients. Subsequently, Madry and Fromm reported the results of 40 patients operated for infected necrosis.4 Patients were described as having necrotic retroperitoneal fat without overt pancreatic necrosis. Sakorafas and colleagues were the first to report a better outcome in patients with EXPN who underwent surgical debridement.5 Operative and CT findings of 12 patients operated for necrotising pancreatitis between 1983 and 1997 suggested that necrotising pancreatitis did not always involve the pancreatic parenchyma. In contrast to the current study, this retrospective study only reported the outcome of patients who underwent surgical debridement for necrotising pancreatitis and did not provide the clinical outcome of the total group of patients (with or without organ failure, sterile or infected, conservative treatment or after intervention). In their study, including 12 patients with EXPN, mortality was 8% which is comparable to the 9% death rate found in 315 patients with EXPN in this study. In both studies the death rate in patients with pancreatic necrosis was 20%. Accurate comparison of death rates between the two studies, however, is hampered by differences in patient characteristics, CECT assessment of EXPN, and study design (ie, experienced single-centre study vs multicentre study with academic and non-academic hospitals).
In the present study EXPN was diagnosed if CECT showed extrapancreatic fat with morphological changes that exceeded fat stranding and if the pancreatic parenchyma did not show any signs of necrosis as determined on the last CECT of hospitalisation or before any intervention. We cannot exclude, however, that small focal areas of parenchymal necrosis were overlooked on CT in patients with EXPN. Inversely, extrapancreatic morphological changes could also consist of fluid only instead of fat necrosis. Previous studies have indeed questioned the accuracy of CECT for diagnosing EXPN.10 ,11 Small extrapancreatic collections (eg, <2 cm in diameter) most likely contain fluid which can easily be absorbed while large extrapancreatic effusions (eg, >5 cm in diameter) are less easily absorbed.12 Collections that do not dissolve early in the course of the disease will most likely contain some degree of peripancreatic tissue necrosis and, hence, have a greater chance of being detected. If extrapancreatic changes have been overestimated and incorrectly scored as EXPN (while those patients actually had interstitial pancreatitis without necrosis), this could potentially question the validity of the differences found in this study. It is known that patients with interstitial pancreatitis have a better prognosis than patients with EXPN. A recent study from Boston compared the outcome of patients with interstitial pancreatitis with that of eight patients with EXPN.13 Patients with interstitial pancreatitis had a better outcome in terms of organ failure, length of hospital stay, need for interventions and mortality, but this study did not include patients with pancreatic necrosis.
However, we have several reasons to believe that the presence of EXPN has not been overestimated in this study. First, several studies have actually demonstrated a good accuracy of CECT for EXPN when CECT findings were compared with the presence of fat necrosis at operation or autopsy.14–16 Second, in patients with EXPN the median time between onset of symptoms and the last CECT before discharge was 9 days. Extrapancreatic collections that persist throughout the second week after onset of symptoms will, in the majority of cases, contain some amount of fat necrosis.17 ,18 Third, the APACHE-II scores on admission and CRP levels after 48 h did not differ between patients with EXPN and those with pancreatic necrosis. If patients with interstitial disease (with extrapancreatic fluid instead of extrapancreatic necrosis) had been incorrectly scored as EXPN and included in the study, one could speculate that the median severity scores on admission in the EXPN group would have been lower than the median severity scores of patients with pancreatic necrosis. However, as patients with interstitial disease (based on CECT) were not included in the study, we did not investigate whether the severity scores in this group of patients is actually lower than in patients with EXPN. In a previous multicentre study we found a death rate of 0.8% in patients with interstitial pancreatitis (the death rate in patients with EXPN in this study was 9%).19 Although the Imrie scores did differ significantly after 48 h, these scores reflect the ongoing inflammatory response and are likely to be more severe in patients with parenchymal necrosis. The same difference in ongoing inflammatory response between groups was seen in patients with organ failure during the first week.
The pathophysiological explanation for the better outcome of patients with EXPN remains speculative. It is generally believed that trypsin activation within pancreatic acinar cells leads to autodigestion and local inflammation.20 ,21 Following a cascade of intracellular events, the pancreatic acinar cells may become necrotic. In some patients, extensive local inflammation causes a severe systemic inflammatory response syndrome that may lead to organ failure.22 ,23 In EXPN, necrosis of the acinar cells does not seem to occur and the pancreatic parenchyma is preserved (at least on CECT). This might be indicative of a less severe local inflammatory response. Subsequently, a less severe local inflammatory response could explain the less severe systemic inflammatory response in patients with EXPN. Another potential explanation may be that the amount of released inflammatory mediators or cytokines in EXPN is lower. The concentration of inflammatory mediators might be higher in the pancreatic acinar cells than in the extrapancreatic fatty tissue. Parenchymal necrosis causes these mediators to be released into the systemic circulation. Conceivably, the higher the amount of mediators released, the more severe the systemic inflammatory response will be.24 Lastly, it might be possible that ductal disruption, which may occur with parenchymal necrosis, causes more complications. Ductal disruption could facilitate bacterial invasion of pancreatic tissue. In this study we found that patients with pancreatic necrosis developed infection significantly more often (47% vs 16%).
In patients with necrotising pancreatitis, pancreatic exocrine and endocrine insufficiencies and pancreatic fistulas following interventions are common long-term complications.8 ,25 ,26 In theory, EXPN will not cause these complications. None of the patients with EXPN in the study by Sakorafas developed endocrine or exocrine insufficiency during long-term follow-up. In a previous study, pancreatic fistulas were shown to cause considerable morbidity.27 For this cohort, however, our prospective database did not include data on exocrine and endocrine insufficiency or pancreatic fistulas.
This clinical study does not necessarily prove, in terms of biology, that EXPN is a separate entity. Based on the results of this study, however, EXPN should be recognised as a different clinical entity within necrotising pancreatitis (compared with parenchymal necrosis) because it heralds several significant clinical implications. First, in cases of EXPN determined on CECT, surgeons should refrain from debridement of the pancreas during necrosectomy (eg, in case of infected necrosis) to prevent iatrogenic pancreatic injury. This knowledge is crucial as during surgery the differentiation between necrotic pancreatic parenchyma and peripancreatic fat necrosis can be difficult. Second, to compare reports of clinical studies on new interventions in necrotising pancreatitis accurately, future studies should report the number of patients with EXPN. Third, the presence of EXPN is a favourable prognosticator compared with pancreatic necrosis. The presence of EXPN should not change overall management but does provide the clinician with information for risk stratification. Fourth, our finding that infected EXPN has a similar poor outcome to that of infected pancreatic necrosis underlines the importance of adequate monitoring and timely recognition and treatment of sepsis in all patients with necrotising pancreatitis.
In summary, this study provides necessary data on the outcome of patients with EXPN. The prognosis of patients with non-infected EXPN has been shown to be significantly better than that of patients with non-infected pancreatic necrosis and could be considered a different clinical entity in acute pancreatitis. In case of infection, however, the prognosis is similar among patients with EXPN and those with parenchymal necrosis.
References
Footnotes
-
Funding The study was supported by a research grant from the Dutch Organization for Health Research and Development (ZonMw, grant numbers 945-06-910). OJB is sponsored by The Netherlands Organization for Health Research and Development (ZonMw, grant number 17 099.2902) to perform clinical studies on necrotising pancreatitis. The sponsors had no involvement in any stage of the study design, data collection, data analysis and interpretation of the study results.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Institutional Review Board of Utrecht University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.