Article Text

Abstract
Background Oral administration of the omega-3 fatty acid eicosapentaenoic acid (EPA), as the free fatty acid (FFA), leads to EPA incorporation into, and reduced growth of, experimental colorectal cancer liver metastases (CRCLM).
Design: We performed a Phase II double-blind, randomised, placebo-controlled trial of EPA-FFA 2 g daily in patients undergoing liver resection surgery for CRCLM. The patients took EPA-FFA (n=43) or placebo (n=45) prior to surgery. The primary end-point was the CRCLM Ki67 proliferation index (PI). Secondary end-points included safety and tolerability of EPA-FFA, tumour fatty acid content and CD31-positive vascularity. We also analysed overall survival (OS) and disease-free survival (DFS).
Results The median (range) duration of EPA-FFA treatment was 30 (12–65) days. Treatment groups were well matched with no significant difference in disease burden at surgery or preoperative chemotherapy. EPA-FFA treatment was well tolerated with no excess of postoperative complications. Tumour tissue from EPA-FFA-treated patients demonstrated a 40% increase in EPA content (p=0.0008), no difference in Ki67 PI, but reduced vascularity in ‘EPA-naïve’ individuals (p=0.075). EPA-FFA also demonstrated antiangiogenic activity in vitro. In the first 18 months after CRCLM resection, EPA-FFA-treated individuals obtained OS benefit compared with placebo, although early CRC recurrence rates were similar.
Conclusions EPA-FFA therapy is safe and well tolerated in patients with advanced CRC undergoing liver surgery. EPA-FFA may have antiangiogenic properties. Remarkably, limited preoperative treatment may provide postoperative OS benefit. Phase III clinical evaluation of prolonged EPA-FFA treatment in CRCLM patients is warranted.
Trial Identifier: ClinicalTrials.gov NCT01070355.
- Angiogenesis
- Colorectal Cancer
- Fatty Acid Supplementation
- Lipid Mediators
- Liver Metastases
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
-
The omega-3 polyunsaturated fatty acid, eicosapentaenoic acid (EPA), has anticolorectal cancer (CRC) activity in preclinical rodent models.
-
EPA in the free fatty acid (FFA) form (EPA-FFA) has chemopreventative efficacy in familial adenomatous polyposis patients.
What are the new findings?
-
EPA-FFA, 2 g daily, is safe and well tolerated in patients undergoing liver resection surgery for CRC liver metastasis.
-
Oral EPA incorporates into CRC liver metastasis tissue.
-
EPA-FFA treatment is associated with reduced vascularity of liver metastases in ω-3 PUFA-naïve patients.
-
Preoperative (median 30 days) EPA-FFA treatment may have prolonged benefit on postoperative overall and disease-free survival.
How might it impact on clinical practice in the foreseeable future?
-
EPA-FFA has considerable potential as adjuvant therapy for secondary prevention of metastatic CRC.
-
Prolonged EPA-FFA use should be evaluated in patients at risk of CRC recurrence.
Introduction
Omega (ω)-3 polyunsaturated fatty acids (PUFA), including eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are found predominantly in oily fish, such as mackerel and sardines.1 Humans have limited ability to synthesise these long-chain PUFAs from α-linolenic acid, which is found in seed oils.2 The modern ‘western’ diet has a large preponderance of ω-6 PUFAs (found in vegetable oils), which is reflected by the large excess of ω-6 PUFAs, such as arachidonic acid (AA), over ω-3 PUFAs in humans.3
There is no convincing evidence from epidemiological studies that dietary fish intake reduces colorectal cancer (CRC) risk.4 However, there is considerable support from preclinical studies that individual ω-3 PUFAs, or fish oil mixtures, have chemopreventative efficacy against CRC.5 We have previously reported that EPA in the free fatty acid (FFA) form (EPA-FFA) 2 g daily for 6 months reduced rectal adenoma number and size in a randomised, placebo-controlled trial (RCT) in familial adenomatous polyposis (FAP) patients.6
There is also evidence from rodent CRC models that ω-3 PUFAs have direct anti-CRC activity.5 Dietary fish oil has been demonstrated to reduce CRC cell tumour growth.5 We recently tested the effect of EPA-FFA on MC-26 mouse CRC cell liver metastasis (CRCLM) in BALB/c mice.7 We demonstrated that EPA-FFA treatment was associated with reduced liver tumour burden.7
The mechanism(s) of the anti-CRC activity of ω-3 PUFAs has not been delineated. Several putative antineoplastic activities have been proposed, including modulation of cyclooxygenase (COX) function.2 ,5 In the BALB/c mouse model of CRCLM, we observed that dietary EPA was incorporated into CRCLMs, which was accompanied by a reduction in prostaglandin (PG) E2 content and appearance of PGE3.7 These changes in lipid biomarkers were associated with a decrease in the proliferation index (PI) of CRCLMs.7
Building on our promising preclinical data7 and those of others,5 demonstrating anti-CRC activity of EPA, we performed a Phase II RCT of EPA-FFA 2 g daily in patients awaiting liver resection for CRCLM (which we termed the EPA for Metastasis Trial (EMT) study).
Methods
EMT study design
Approval was obtained from Leeds (West) Research Ethics Committee (09/H1307/94) and the MHRA (16767/0240/001–0001). All participants provided written informed consent.
Patients older than 18 years of age, of either sex, with CRCLM, for whom liver resection surgery was considered appropriate (either first or second liver resection) were eligible. Subjects were excluded if neoadjuvant chemotherapy was planned or they had received any chemotherapy in the previous 3 months. Other exclusion criteria were known bleeding diathesis or anticoagulant therapy, unwillingness to stop existing fish oil supplement use, fish/seafood allergy, use of non-aspirin, non-steroidal anti-inflammatory drugs (NSAIDs) or corticosteroids, pregnancy, renal impairment (serum creatinine (Cr) >150 μmol/L) and active systemic inflammatory disease.
After written informed consent was obtained (visit 1), a blood and urine sample was collected. Participants completed a food frequency questionnaire (FFQ) in order to determine baseline ω-3 PUFA intake (see online supplementary methods). Participants were randomised 1:1 in a random permutated block of four using random number tables to either two enteric-coated, soft-gel capsules, each containing 500 mg 99% pure EPA-FFA (ALFA (SLA Pharma AG, Liestal, Switzerland)), twice daily with food, or two identical placebo capsules containing 500 mg mixed capric and caprylic acid medium-chain triglycerides (Sasol, Witten, Germany), twice-daily.6 Participants and investigators were blinded to treatment allocation until all participants finished the trial and all laboratory analyses had been completed. Capsules were taken from randomisation until the day before surgery. Existing fish oil supplement use was stopped at randomisation. Participants were contacted every 2 weeks to enquire about adverse events (AE). Patients were allowed to decrease the dose to one capsule twice daily with food in response to a perceived treatment-related AE, with a subsequent attempt to reinstitute the full dose.
On the day before surgery (visit 2), further blood and urine samples were collected and a second FFQ was completed. Trial medication was returned and counted. Liver resection surgery and postoperative care were performed as per local protocols. Blood and urine were collected, and a third FFQ completed at routine postoperative review approximately 6 weeks after discharge (visit 3).
Sample size calculation and statistical analysis
We previously reported that treatment with EPA-FFA was associated with a reduction in PI of mouse CRCLMs.7 Moreover, the Ki67 PI of CRCLMs has been demonstrated to predict disease-free survival (DFS) and overall survival (OS) after surgical resection or adjuvant chemotherapy.8 ,9 Therefore, we chose the CRCLM PI as the primary end-point. In our previous RCT of rofecoxib in CRCLM patients, the mean Ki-67 PI in the placebo arm was 50 (SD 22).10 The only study of the effect of an anti-CRC agent on the CRCLM PI revealed a 30% reduction in 5-fluorouracil-treated CRCLM tissue compared with control tumours.11 In order to detect a minimum 30% difference in PI between EPA-FFA and placebo groups with 80% power and a 5% two-sided significance level, we calculated that 35 patients were required in each arm. We assumed 20% drop-out before surgery,10 thus making the recruitment target 88 patients.
Secondary end-points included safety and tolerability of EPA-FFA, CRC cell apoptosis, tumour vascularity, tumour PUFA incorporation and PG levels.
The χ2 test, Student t test, Mann–Whitney U test or Wilcoxon rank sum test were used to evaluate differences between treatment groups. Skewed tumour vascularity and urinary PG metabolite data were logarithmically transformed prior to parametric tests on normally distributed data.
Exploratory end-points were OS and DFS after the intervention phase of the trial. Survival data were collected prospectively through the Leeds Hepatobiliary Surgery database,12 ,13 in which CRC recurrence (defined as radiological evidence of metastatic CRC) and mortality is recorded during six-monthly clinical and thoraco-abdominal CT scan follow-up, unless interval assessment is indicated. The censor date was 20 June 2013. Investigators were unblinded before analysis of long-term survival data. However, all participants remained blind to treatment allocation. The two treatment groups were compared by Kaplan–Meier survival analysis and the Cox proportional hazards model, which included factors with a p value <0.2 by univariate analysis. Data are presented as the HR and 95% CI.
Blood, urine and CRCLM tissue collection
Biological sample collection and storage is described in online supplementary methods.
Platelet aggregation studies
Whole blood platelet aggregation was measured using a Dynabyte (Munich, Germany) Multiplate platelet aggregometer, using AA (0.5 mM), ADP (6.5 μM) or collagen (0.64 (termed low concentration) or 3.2 μg/mL) as the agonist.
Assay of nuclear factor (NF) κB DNA binding activity
See online supplementary methods for details of peripheral blood mononuclear cell (PBMC) culture and the NFκB DNA binding assay.
Immunohistochemistry
Immunohistochemistry for Ki67 and neocytokeratin (CK)18 on formalin-fixed paraffin-embedded 4 μm CRCLM sections was performed using mouse antihuman Ki67 (MIB1 clone) antibody (Dako, Ely, UK), and mouse antihuman neo-CK18 antibody M30 (Roche, Mannheim, Germany), respectively (both 1:50 dilution), as described,10 with modifications described in online supplementary methods.
The percentage number of CRC cells with a Ki67-positive nucleus (the PI) was determined in predetermined high-power fields (×200) of each CRCLM adjacent to the tumour–liver interface (see online supplementary methods). Images were analysed using ImageJ with the cell counter plugin (http://rsbweb.nih.gov/ij/). A minimum 500 malignant epithelial cells were counted.
Quantification of neo-CK18-positive apoptotic epithelial cells using a colour deconvolution programme is described in online supplementary methods.
Immunohistochemistry for CD31 was performed using mouse antihuman CD31 antibody JC/70A (Dako), which was incubated with sections overnight at 4°C at a 1:40 dilution. Tumour vessel density and vascular area were measured at Genentech (San Francisco, CA) by in-house image analysis of Aperio ScanScope-scanned tumour sections (see online supplementary methods).14
All immunohistochemical analyses were performed blind to treatment allocation.
Measurement of tissue E-type PGs and urinary PGE-M by liquid chromatography-tandem mass spectrometry
Levels of PGE2 and PGE3 in tumour tissue were measured by liquid chromatography-tandem mass spectrometry (LC-MS/MS) as described and quoted as pg PG per mg wet weight tissue.7
Levels of 11α-hydroxy-9, 15-dioxo-2, 3, 4, 5-tetranor-prostane-1, 20-dioic acid (PGE-M) in urine were measured by LC-MS/MS.15 The limit of detection was 1.5 ng/mL. The urinary Cr concentration in mg/mL was measured using an ADVIA 1800 analyser (Siemens). The urinary PGE-M concentration is presented as ng PGE-M/mg Cr.
Measurement of tissue PUFA content
The relative PUFA content of tumour tissue was measured by gas chromatography-mass spectrometry as previously described.6 ,7
Endothelial cell culture and angiogenesis assays
Human umbilical vein endothelial cells (HUVECs) were cultured in endothelial cell culture medium supplemented with 10% (v/v) endothelial cell growth supplement (TCS Cellworks, Buckingham, UK). HUVECs were treated with EPA-FFA by dilution of a stock solution of fresh EPA-FFA in absolute ethanol, as described.16
Details of the three HUVEC angiogenesis assays are in online supplementary methods.
Results
Patient characteristics and clinical outcomes
Between April 2010 and July 2011, there were 203 consecutive patients who were screened in the outpatient clinic (figure 1). One hundred and two patients had one or more exclusion criteria, with the majority excluded because of adjuvant chemotherapy in the previous 3 months (figure 1).
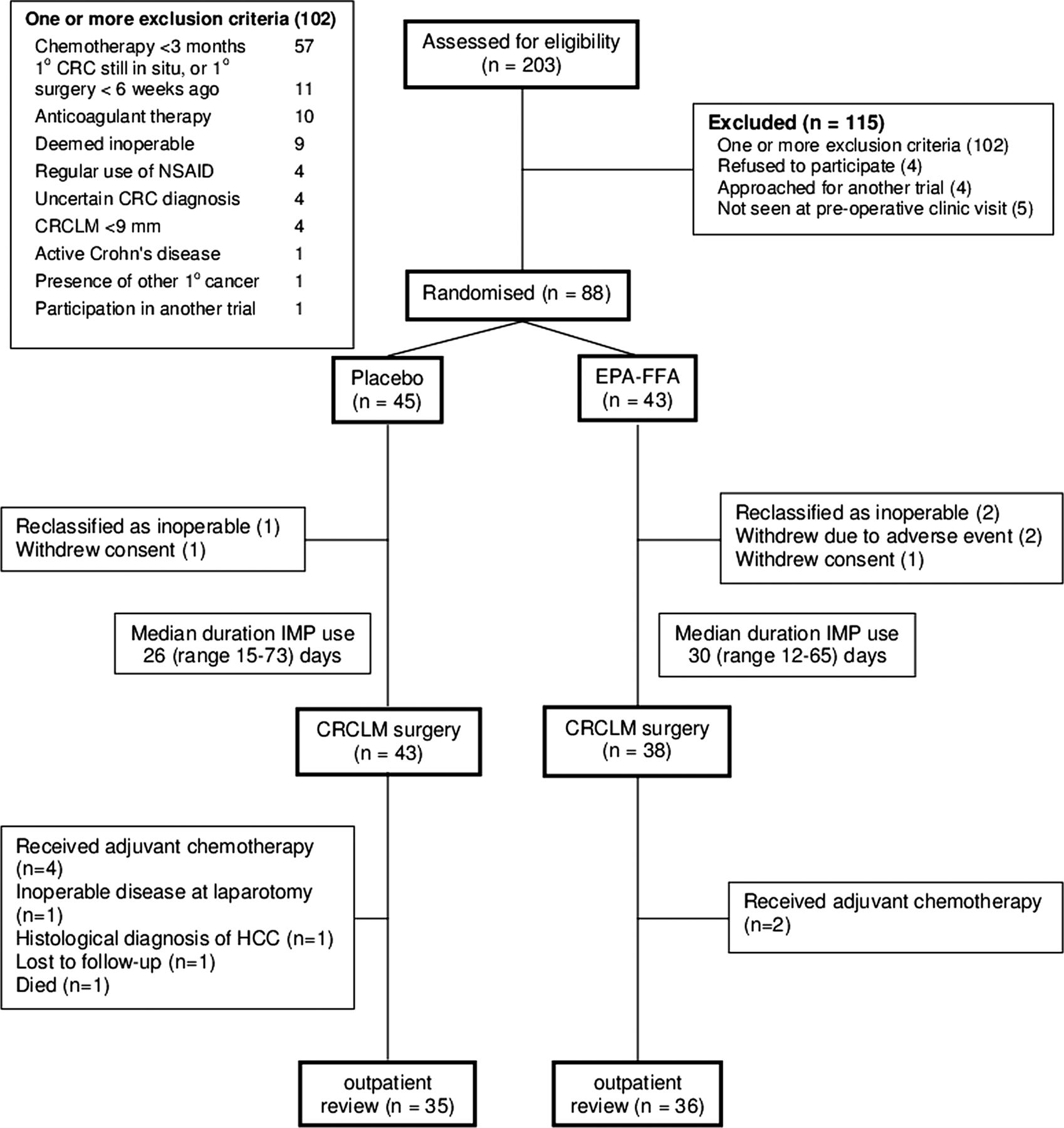
CONSORT diagram.
Eighty-eight patients were randomised to receive either EPA-FFA 2 g daily (n=43) or placebo (n=45), prior to liver surgery. The treatment groups were well matched (table 1). There was no significant difference between the two Trial arms regarding CRCLM characteristics (table 1), although patients in the placebo group had a greater proportion of synchronous metastatic disease and a shorter interval between primary CRC surgery and clinical presentation with CRCLM compared with the EPA-FFA group (table 1).
Baseline characteristics of randomised patients
Three participants were reclassified as inoperable and two patients withdrew consent (figure 1). Two patients in the EPA-FFA group were withdrawn due to diarrhoea. Therefore, 81 patients underwent CRCLM surgery in the Trial (figure 1). Investigational medicinal product (IMP) was taken for a variable period between randomisation and surgery, reflecting routine clinical practice. The median duration (range) of EPA-FFA use was 30 (12–65) days compared with 26 (15–73) days of placebo administration (p=0.62).
Compliance with EPA-FFA was excellent, confirmed by mean pill counts of 91% (EPA-FFA) and 94% (placebo). EPA-FFA was well tolerated in patients with CRCLMs with AEs limited to mild or moderate upper gastrointestinal symptoms, and diarrhoea in 12% and 19% of patients taking EPA-FFA, respectively (table 2).
Safety and tolerability of EPA-FFA in CRCLM patients
The extent of liver resection was similar in both treatment arms (see online supplementary table 1). There was no significant difference in postoperative AEs, blood transfusion requirement or length of hospital stay between the two treatment groups (table 2 and online supplementary table 1). Consistent with this, there was no significant effect of EPA-FFA on ex vivo platelet aggregation at the end of the treatment period (see online supplementary figure S1A), although aspirin use was associated with impaired platelet aggregation, as expected (see online supplementary figure S1B). There was no evidence of any additive or synergistic effect of EPA-FFA with aspirin (see online supplementary figure S1B).
We assessed dietary oily fish intake in order to exclude changes in ω-3 PUFA intake that might confound tissue PUFA data. The highest oily fish intake category was 2–4 portions per week (equivalent to daily intake of approximately 400–500 mg ω-3 PUFA per day assuming a portion size of 85 g).3 This level of oily fish intake was reported by four participants in the placebo group and two patients in the EPA-FFA group. There was no significant change in oily fish intake during the Trial (see online supplementary methods).
EPA-FFA treatment is associated with increased levels of EPA in CRCLM tissue
Liver tumours from patients who received EPA-FFA prior to surgery contained 40% more EPA than control CRCLMs (table 3 and figure 2A). There was a similar excess of docosapentaenoic acid (DPA) in CRCLMs from the EPA-FFA group (table 3 and figure 2B). However, there was a small, but statistically significant, decrease in tumour DHA content (table 3 and figure 2C). There was no overall difference in the AA content of CRCLMs from the two treatment arms (table 3 and figure 2D). The erythrocyte AA:EPA ratio is commonly quoted as a biomarker of ω-3 PUFA content.3 Comparison of individual tumour AA:EPA ratios demonstrated a significantly lower ratio in EPA-FFA-treated tumours than CRCLMs from the placebo group (table 3). Patients in the placebo group who previously took a fish oil supplement or who ate 2–4 portions of oily fish per week had a significantly higher EPA content in CRCLMs than ‘EPA naïve’ participants (figure 2A; p=0.037; Student unpaired t test). There was no correlation between the duration of EPA-FFA treatment and the relative tumour content of any PUFA (data not shown).
PUFA content of CRCLMs
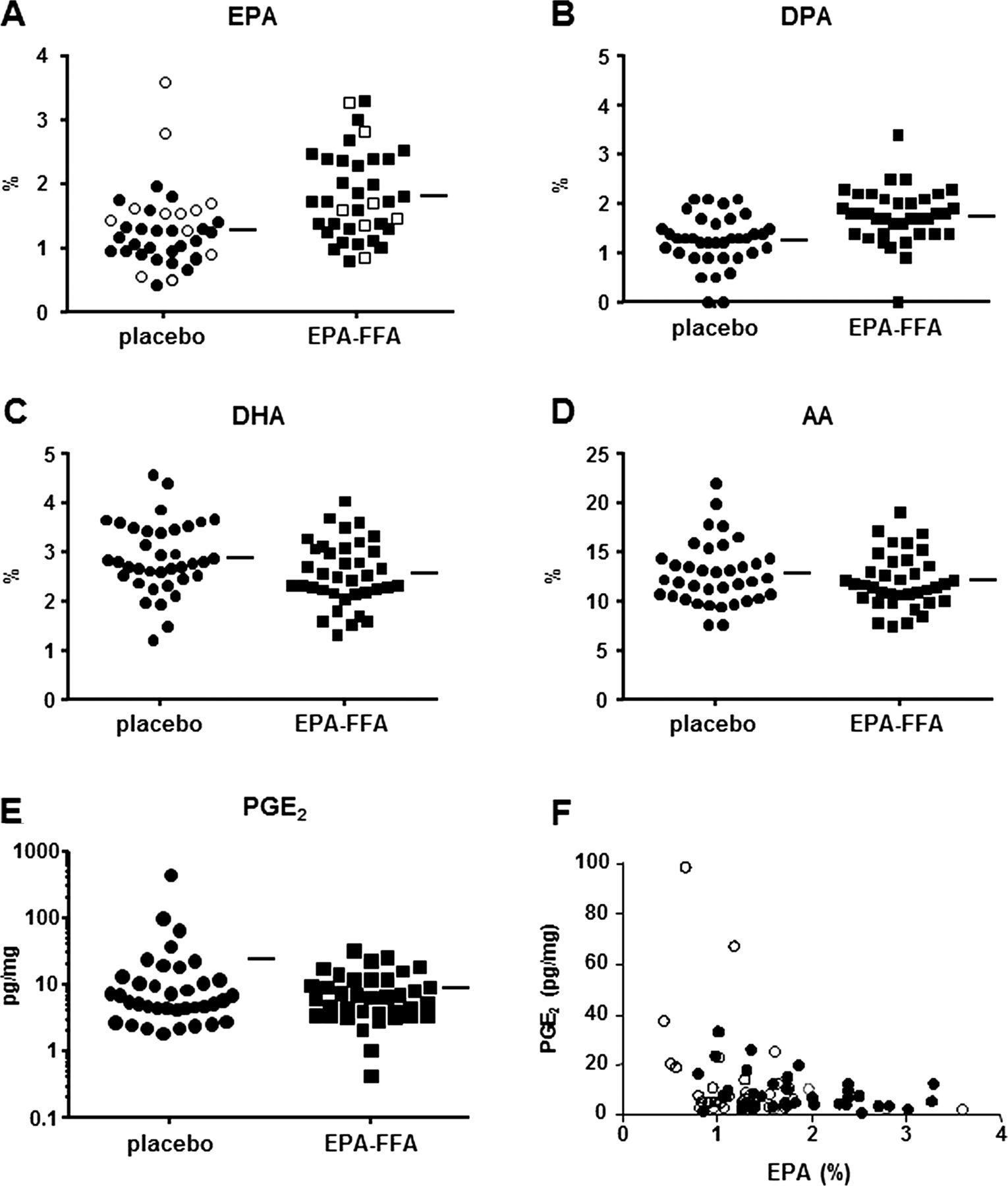
Levels of PUFAs and PGE2 in CRCLMs. A-D) Individual data points denote the CRCLM PUFA level (n=37 each group), expressed as the % fatty acid content. Bars represent the mean value. Unfilled data points in (A) denote tumours from patients who took fish oil supplements or who ate 2–4 portions of oily fish per week (placebo, n=12 (fresh frozen tissue was not available from one tumour); EPA-FFA, n=7). (E) The PGE2 level in CRCLMs (n=37 each group). Bars represent the mean value. (F) The relationship between the EPA content and PGE2 level in individual tumours. Unfilled circles represent tumours from placebo-treated patients (n=37) and filled circles represent tumours from EPA-FFA-treated patients (n=37).
E-type prostaglandin levels in CRC tissue
Prostaglandin E2 was detected in all tumour samples, but levels spanned several orders of magnitude (figure 2E). The mean (range) PGE2 level in tumours from EPA-FFA-treated patients was 8.8 (0.4–33.4) pg/mg compared with 24.5 (1.9–447) pg/mg in CRCLMs from patients who received placebo (p=0.68; Mann–Whitney U test). PGE3 was detected above the limit of detection (10 pg/mg) in only one tumour (21.1 pg/mg), which was the CRCLM specimen from the EPA-FFA arm with the highest PGE2 level. There was a weak inverse relationship between the EPA content and PGE2 level of individual CRCLMs (r=−0.30, p=0.009) figure 2F). However, there was no significant correlation between the tumour AA content and the corresponding PGE2 level (r=−0.11, p=0.36).
The effect of EPA-FFA on urinary PGE-M levels
Levels of the stable urinary metabolite PGE-M are believed to reflect systemic PGE2 production.17 There was no significant difference in the geometric mean urinary PGE-M level between the two groups at baseline (see online supplementary figure S2A). However, the post-treatment PGE-M level was 51.8% lower in the EPA-FFA group compared with placebo (p<0.001). This represented a 27.6% reduction in urinary PGE-M in the EPA-FFA group, compared with a 27.9% increase in urinary PGE-M in the placebo group related to baseline. Urinary PGE-M levels rose again by 52.2% at the postoperative follow-up in the EPA-FFA group (p=0.016). There was no significant difference in PGE-M levels postoperatively. There was no correlation between post-treatment urinary PGE-M values and the duration of EPA-FFA treatment (Pearson correlation coefficient 0.06, p=0.73). Subanalysis excluding those patients who were previous fish oil users or in the highest category of oily fish intake did not alter the overall findings (data not shown).
We also measured DNA binding of NFκB in PBMCs in order to test the hypothesis that EPA-FFA has systemic anti-inflammatory properties. A reversible reduction in NFκB binding in PBMCs from participants in the EPA-FFA group was observed, similar to the effect on urinary PGE-M levels (see online supplementary figure S2B).
EPA-FFA treatment is associated with reduced vascularity but no difference in CRC cell proliferation or apoptosis index
There was no significant difference in the CRCLM PI between the treatment groups (see online supplementary figure S3A). The mean (±SEM) PI of CRCLMs from the placebo group (n=41) was 73.0±2.4% compared with 70.7±2.7% in 37 EPA-FFA-treated tumours (p=0.68). There was no significant correlation between the PI and the PUFA content of, or PGE2 level in, individual CRCLMs (data not shown). There was also no significant difference in neo-CK18 CRC cell apoptosis between EPA-FFA- and placebo-treated CRCLMs (see online supplementary figure S3B). Similar results were obtained if the analysis was restricted to ‘EPA-naïve’ individuals (data not shown).
A secondary end-point of the Trial was the CD31-positive vascularity of CRCLMs. Vascularity scores of individual CRCLMs were highly variable in both treatment groups (figure 3A), consistent with data from our previous CRCLM trial.10 Analysis of evaluable CRCLM sections from the entire treatment population (placebo, n=39; EPA-FFA, n=36) did not reveal any difference in either of the two vascularity measures (p=0.87 and 0.74 for % vascular area and vessel density, respectively). However, if previous fish oil supplement users or those in the highest category of oily fish intake were excluded, we observed a trend towards reduced tumour vascularity in EPA-FFA-treated CRCLMs (figure 3A). The geometric mean tumour vascular area in EPA-FFA-treated CRCLMs (n=29) was 48% lower than in 26 placebo-treated tumours (0.027% vs 0.052%; p=0.075). The geometric mean tumour vessel density was 43% lower in EPA-FFA-treated CRCLMs compared with placebo-treated tumours (16.9 vs 29.6 vessels/106 μm2; p=0.09).

Antiangiogenic activity of EPA-FFA. (A) Vascularity of CRCLMs in placebo- and EPA-FFA-treated groups, excluding previous fish oil users and those in the highest category of oily fish intake (placebo, n=13; EPA-FFA, n=7). Bars represent the mean value. (B) The effect of EPA-FFA on (i) proliferation, (ii) motility and (iii) tube formation of HUVECs. (i) Data are the fold increase in optical density (OD) at 570 nm compared with time zero (mean and SEM of 12 replicate wells from two independent experiments). (ii) The mean and SEM % wound closure (n=6). *p<0.05 compared with control. (iii) The mean and SEM number of complete HUVEC loops (n=8). *p=0.06 compared with control.
Antiangiogenic activity of EPA-FFA in vitro
Given the finding of reduced vascularity of CRCLMs and existing in vitro evidence that EPA may have antiangiogenic activity,18 we tested whether EPA-FFA exhibited antiangiogenic activity against HUVECs. Acute exposure to EPA-FFA inhibited HUVEC proliferation in a concentration-dependent manner with an IC50 of approximately 15 μM (figure 3B(i)). EPA-FFA also reduced HUVEC cell motility as part of a wound closure response (figure 3B(ii)). Finally, acute exposure to EPA-FFA was associated with reduced tubule formation by HUVECs on basement membrane matrix (figure 3B(iii)). Taken together, these in vitro data are consistent with antiangiogenic activity of EPA-FFA.
EPA-FFA treatment prior to CRCLM surgery provides long-term OS and DFS benefit
Although the Trial was not powered to detect a difference in postoperative survival, we took the opportunity to address the hypothesis that incorporation of lipophilic EPA into cell plasma membranes may provide prolonged anti-CRC benefit after cessation of short-term, preoperative EPA-FFA treatment.
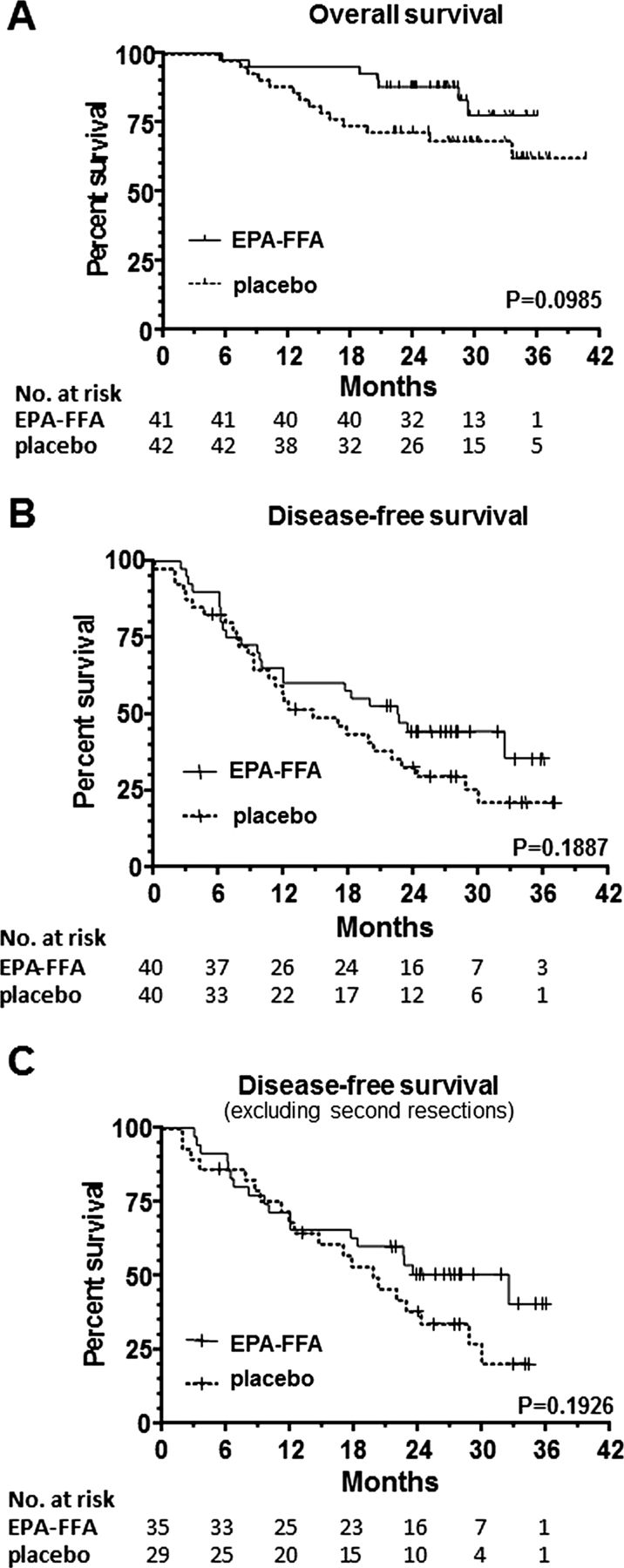
Overall survival (OS) up to 40 months after surgery was increased in patients allocated EPA-FFA (LogRank p=0.0985), which was explained by reduced mortality in the EPA-FFA group in the first 18 months after surgery (figure 4A). There were seven deaths in 41 evaluable CRCLM patients who received EPA-FFA compared with 14 deaths in the placebo group (n=42). There were two non-CRC-related deaths in the placebo group (liver failure and a cerebrovascular event). Univariate analysis of OS related to patient and CRC characteristics, as well as duration of IMP use, tumour EPA content and tumour AA/EPA ratio, demonstrated that only IMP allocation and the presence of synchronous disease yielded a p value less than 0.2. A multivariate Cox proportional hazards model revealed that only EPA-FFA treatment (HR 0.40 (CI 0.16 to 1.0); p=0.05) was retained in the model as a significant independent predictor of OS after CRCLM surgery. The presence of synchronous disease had a HR of 0.38 (0.14 to 1.1), which just failed to reach statistical significance (p=0.06).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
EPA-FFA confers OS and DFS benefit after surgery for CRCLM. (A) Overall survival. All randomised patients (including 3 patients, who did not undergo CRCLM resection at laparotomy) were entered into the survival analysis except one patient who was found to have HCC and 3 patients who withdrew prior to surgery. B) Disease-free survival. Three patients who did not undergo CRCLM resection at laparotomy, one patient with HCC and three patients who withdrew prior to surgery were excluded from the DFS analysis. C) Disease-free survival excluding individuals who underwent a second liver resection. In each case, the LogRank value is noted above and the number of evaluable cases is recorded below the X axis.
CRC recurred in 23 of 40 patients who received EPA-FFA prior to CRCLM surgery (median DFS 22.6 months) compared with 29 of 40 patients who were allocated to placebo (median DFS 14.7 months; LogRank p=0.1887). Any DFS benefit in the EPA-FFA group was explained by a reduction in CRC recurrence from 12 months after surgery onwards (figure 4B). Univariate analysis identified age, IMP allocation, second liver resection, the interval between primary CRC surgery and CRCLM, and previous chemotherapy as factors predicting recurrence. A Cox proportional hazards model revealed that second liver resection (HR 3.41 (1.63 to 7.13), p=0.001), and interval between primary CRC surgery and CRCLM (HR 0.98 (0.96 to 0.99), p=0.019), were retained as independent predictors of CRC recurrence. As second liver resection was a strong predictor of CRC recurrence, we excluded cases that underwent a second liver resection (placebo 11, EPA-FFA 6), on the basis that these patients have significantly more aggressive disease (figure 4C). Cox multivariate analysis now retained treatment allocation as a significant covariate (HR 0.35 (0.15 to 0.79); p=0.011) predicting DFS. Previous chemotherapy was identified as a negative predictive factor for DFS (HR 2.03 (0.90 to 4.59)) that failed to reach statistical significance (p=0.09).
Discussion
EPA-FFA is safe and well-tolerated in patients with metastatic CRC, who are scheduled for liver resection. EPA-FFA use did not affect postoperative bleeding or infective complications, consistent with a lack of ex vivo antiplatelet activity. Symptoms of mild-to-moderate gastrointestinal disturbance occurred in a small, but significant, proportion of patients taking EPA-FFA, similar to previous studies of EPA-FFA and other ω-3 PUFA preparations.5 ,6
This is the first report that oral intake of EPA leads to incorporation into secondary CRC tissue. Consistent with previous human and murine studies of normal and malignant colorectal tissue,5 ,7 there was elongation of EPA to DPA in CRCLMs. However, no desaturation of DPA to DHA was observed. There was only a modest reduction in relative tumour AA content in the EPA-FFA arm compared with placebo, consistent with a recent report of a small, but statistically significant, decrease in blood granulocyte AA levels in CRC patients after 7 days of oral ω-3 PUFA supplementation.19 Previous clinical studies of mixed ω-3 PUFAs have demonstrated that maximal incorporation into colorectal mucosa and circulating immune cells occurs within 3 weeks, with a reduction in AA content only becoming apparent from 6 weeks onwards.20 ,21
Stephenson et al did not observe an increase in CRCLM EPA content between 4 and 12 days after parenteral administration of mixed ω-3 and ω-6 PUFAs.22 Our data highlight the importance of the chemical form and formulation of ω-3 PUFAs for maximal bioavailability in cancer tissue.23
Intratumoral PGE2 levels varied widely in both treatment groups. A previous study of 21 CRCs described PGE2 levels one-to-two orders of magnitude lower than we report.24 Unlike mouse MC-26 CRCLM tissue,7 we did not detect PGE3, except in one (EPA-FFA treated) patient. One explanation is that tissue PGE3 levels were below the sensitivity (10 ng/mg) of our LC-MS/MS technique.
Urinary PGE-M values observed in the EMT study were elevated compared with healthy individuals,17 and were similar to those reported in studies of CRC and non-small cell lung cancer.17 ,25 One striking observation from the longitudinal analysis of urinary PGE-M levels is that PGE-M levels were not reduced after CRCLM resection. This suggests that CRCLM-derived PGE2 does not contribute significantly to generation of urinary PGE-M. Consistent with this notion, urinary PGE-M levels were similar in CRC patients who did or did not respond to therapy with cetuximab and celecoxib.25 EPA-FFA therapy was associated with a small, but statistically significant, reduction in urinary PGE-M level consistent with COX inhibition by EPA.5 The return of urinary PGE-M levels (and NFκB DNA binding in PBMCs) to baseline values, several weeks after treatment cessation, indicates reversible systemic anti-inflammatory activity of EPA-FFA. In future studies, it will be important to further delineate intratumoral and systemic anti-inflammatory activity of oral EPA therapy.
We report reduced tumour vascularity in EPA-FFA-treated CRCLMs from ‘ω-3 PUFA-naïve’ patients. Consistent with antiangiogenic activity of EPA-FFA in vivo, we confirmed that EPA-FFA had direct antiangiogenic activity against HUVECs.18 There is also evidence that ω-3 PUFAs may have antiangiogenic activity via reduced synthesis of proangiogenic factors.26 Future Phase III studies should evaluate antiangiogenic activity of ω-3 PUFAs stratified for basal ω-3 PUFA levels.
Possible OS and DFS benefit following short-term preoperative EPA-FFA is a fascinating preliminary observation. We acknowledge that the study was not powered to assess long-term clinical outcomes. However, we did prespecify OS and DFS analysis in our Cancer Research UK-approved protocol and a methodological strength was use of a prospective clinical database.12 ,13
Overall survival benefit from EPA-FFA was evident in the first 18 months after surgery, even though early CRC recurrence was similar in both treatment groups. Of note, the two study arms were well matched for factors that are known to impact on prognosis following CRCLM surgery.27
There was a suggestion of DFS benefit in the EPA-FFA group from approximately 12 months onwards. The strongest prognostic factor predicting CRC recurrence was whether second CRCLM surgery had taken place. This group of patients is likely to have more aggressive disease. Exclusion of this distinct subset of patients then revealed EPA-FFA allocation as predictive of improved DFS. By contrast, preoperative chemotherapy predicted CRC recurrence, albeit with a wide CI, consistent with previous data.12 Tumour progression during preoperative chemotherapy has been associated with poor outcomes after CRCLM surgery.13 Unfortunately, retrospective data on preoperative chemotherapy response were not available in order to explore this relationship further. Recently, preoperative chemotherapy has been identified as a significant predictor of CRC recurrence after CRCLM resection.12
We believe that prolonged survival benefit after limited preoperative EPA-FFA therapy is plausible. By contrast with tissue incorporation kinetics during oral ω-3 PUFA administration,20 ,21 disappearance of ω-3 PUFAs following cessation of therapy is believed to be much slower and occurs over a period of months, presumably related to the lipophilic nature of ω-3 PUFAs.2 ,28 ,29
Improved OS in the first 18 months after CRCLM surgery in patients randomised to EPA-FFA treatment, despite similar rates of CRC recurrence, suggests that EPA-FFA could reduce growth of established tumours consistent with efficacy in preclinical models and antiangiogenic activity.5 ,7 ,18 Alternatively, improved OS despite similar rates of CRC recurrence may be a manifestation of a beneficial effect of EPA-FFA on CRC-induced cachexia. Although a recent systematic review of fish oil for the treatment of cancer cachexia concluded that there was insufficient evidence to support benefit from ω-3 PUFAs,30 longer-duration studies hint that the combination of ω-3 PUFAs and chemo-radiotherapy may provide survival benefit.31
In summary, we have demonstrated that oral EPA-FFA is safe and well tolerated in patients with advanced CRC. Oral EPA treatment leads to incorporation of EPA into CRCLM tissue, is associated with possible reduced tumour vascularity, and has systemic anti-inflammatory activity. Remarkably, limited preoperative EPA-FFA exposure may prolong OS and DFS.
Acknowledgments
We thank all the patients who participated in the Trial. The Authors also wish to thank the external members of the Trial Steering Committee and Data Monitoring Committee (Professor Chris Twelves (Chair), Mr Richard Maltby, Mr Paxton Dewar). Mr Alex Wright and Dr Darren Treanor (Leeds Institute of Cancer Studies & Pathology) developed the image analysis algorithm for measuring apoptosis. The important contribution of Dr Adrian Jubb (Genentech Inc) to the analysis of tumour vascularity is acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figure 1
- Data supplement 3 - Online figure 2
- Data supplement 4 - Online figure 3
- Data supplement 5 - Online table
Footnotes
-
Contributors Study concept and design AJC, GJT, MAH; acquisition of data AJC, MV, ADR, AM, CF, PML, GJT; analysis and interpretation of data AJC, MV, AB, PML, GJT, MAH; drafting and critical revision of the manuscript AJC, AB, MAH.
-
Funding The Cancer Research UK Clinical Trials Awards and Advisory Committee approved the Trial. PML and ADR were supported by Department of Health/Cancer Research UK Yorkshire Experimental Cancer Medicine Centre funding. The Trial was adopted by the UKCRN Clinical Trials Portfolio (UKCRN ID 8946) allowing West Yorkshire Comprehensive Local Research Network funding of Pharmacy costs. SLA Pharma AG funded some of the experimental work and provided EPA-FFA and placebo. SLA Pharma AG played no role in the design or execution of the Trial. Laboratory costs were also supported by the Leeds Teaching Hospitals Charitable Foundation (Rays of Hope).
-
Competing interests MAH and AB have received unrestricted scientific grant funding and meeting expenses from SLA Pharma AG. MAH is listed as an inventor on a composition and use patent, which includes EPA-FFA (US Provisional Patent Application No. 60/411,067). He receives no royalties from this Patent.
-
Ethics approval Leeds (West) REC.
-
Provenance and peer review Not commissioned; externally peer reviewed.