Article Text

Abstract
Objective Accumulating evidence links the intestinal microbiota and colorectal carcinogenesis. Fusobacterium nucleatum may promote colorectal tumour growth and inhibit T cell-mediated immune responses against colorectal tumours. Thus, we hypothesised that the amount of F. nucleatum in colorectal carcinoma might be associated with worse clinical outcome.
Design We used molecular pathological epidemiology database of 1069 rectal and colon cancer cases in the Nurses’ Health Study and the Health Professionals Follow-up Study, and measured F. nucleatum DNA in carcinoma tissue. Cox proportional hazards model was used to compute hazard ratio (HR), controlling for potential confounders, including microsatellite instability (MSI, mismatch repair deficiency), CpG island methylator phenotype (CIMP), KRAS, BRAF, and PIK3CA mutations, and LINE-1 hypomethylation (low-level methylation).
Results Compared with F. nucleatum-negative cases, multivariable HRs (95% CI) for colorectal cancer-specific mortality in F. nucleatum-low cases and F. nucleatum-high cases were 1.25 (0.82 to 1.92) and 1.58 (1.04 to 2.39), respectively, (p for trend=0.020). The amount of F. nucleatum was associated with MSI-high (multivariable odd ratio (OR), 5.22; 95% CI 2.86 to 9.55) independent of CIMP and BRAF mutation status, whereas CIMP and BRAF mutation were associated with F. nucleatum only in univariate analyses (p<0.001) but not in multivariate analysis that adjusted for MSI status.
Conclusions The amount of F. nucleatum DNA in colorectal cancer tissue is associated with shorter survival, and may potentially serve as a prognostic biomarker. Our data may have implications in developing cancer prevention and treatment strategies through targeting GI microflora by diet, probiotics and antibiotics.
- CANCER EPIDEMIOLOGY
- COLORECTAL CANCER
- INTESTINAL BACTERIA
- COLONIC BACTERIA
- COLONIC MICROFLORA
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Microorganisms play an important role in health and disease conditions, including cancer.
Fusobacterium nucleatum has been shown to promote colorectal tumour growth and inhibit antitumour immune responses in animal models.
F. nucleatum DNA is detectable in a subset of human colorectal neoplasias.
What are the new findings?
The amount of F. nucleatum DNA in colorectal cancer tissue is positively associated with colorectal cancer-specific mortality, independent of clinical, pathological and major tumour molecular features.
The amount of F. nucleatum DNA in colorectal cancer tissue is positively associated with pT stage.
The amount of F. nucleatum in colorectal cancer tissue is associated with microsatellite instability (MSI)-high in univariable and multivariable analyses (independent of CpG island methylator phenotype (CIMP) and BRAF mutation status), whereas CIMP and BRAF mutation are associated with F. nucleatum only in univariate analyses but not after adjusting for MSI status.
How might it impact on clinical practice in the foreseeable future?
F. nucleatum DNA in colorectal carcinoma tissue may serve as a potential prognostic biomarker.
Our population-based data can provide insights for the development of new colorectal cancer prevention and treatment strategies through targeting the microbiota.
Introduction
More than 100 trillion (1014) microorganisms inhabit the human intestinal tract and play an important role in health and disease conditions, including cancer.1–4 A growing body of evidence suggests a potential link between the microbiota and colorectal carcinogenesis.5–13 Proportions of colorectal cancers with specific molecular features including microsatellite instability (MSI), CpG island methylator phenotype (CIMP)-high and BRAF mutation have been shown to decrease continuously from ascending colon to rectum, supporting a gradual change in pathogenic influence of intestinal microbiota and luminal contents along the proximal-distal axis.14
Studies have demonstrated an enrichment of Fusobacterium nucleatum in human colorectal adenomas and carcinomas compared with adjacent normal tissue.15–17 Experimental studies have shown that F. nucleatum activates the WNT signalling pathway in colorectal carcinoma cells and may promote colorectal tumour growth,18 and that F. nucleatum may inhibit T cell-mediated immune responses against colorectal tumours.16 ,19 Consistent with these lines of experimental evidence, a higher amount of tissue F. nucleatum DNA has been associated with advanced disease stage6 ,7 ,20 and a lower density of T cells in human colorectal carcinoma tissue.21 However, the prognostic significance of F. nucleatum DNA in colorectal cancer tissue, controlling for clinical, pathological and tumour molecular features, remains uncertain. We hypothesised that a higher amount of tissue F. nucleatum DNA might be associated with worse clinical outcome in colorectal cancer.
To test this hypothesis, we used over 1000 colorectal carcinoma cases in two US nationwide prospective cohort studies (the Nurses’ Health Study and the Health Professionals Follow-up Study), and examined the amount of tissue F. nucleatum DNA in relation to colorectal cancer mortality. Use of our comprehensive database enabled us to examine its prognostic role, while controlling for potential confounders including statuses of MSI, CIMP and BRAF mutation.
Methods
Study population
We used the database of two US nationwide prospective cohort studies, the Nurses’ Health Study (with 121 701 women enrolled in 1976) and the Health Professionals Follow-up Study (with 51 529 men enrolled in 1986).22 ,23 Every 2 years, participants were sent follow-up questionnaires to gather information on health and lifestyle factors, and asked whether they had received diagnoses of major disease including cancers. The National Death Index was used to ascertain deaths of study participants and identify fatal colorectal carcinoma cases. Follow-up has exceeded 90% for each 2-year questionnaire. Study physicians reviewed medical records for all colorectal cancer cases, and assigned the cause of death for all deceased cases. Formalin-fixed paraffin-embedded (FFPE) tissue blocks were collected from hospitals where participants with colorectal carcinoma had undergone tumour resection. We included colon and rectal carcinoma cases, considering the colorectal continuum model.24 A single pathologist (SO), who was unaware of other data, conducted a centralised review of H&E-stained tissue sections from all colorectal carcinoma cases, and recorded pathological features. Tumour differentiation was categorised as well to moderate or poor (>50% vs ≤50% glandular area). We analysed available data on tissue F. nucleatum DNA and patient survival in 1069 colorectal carcinoma cases diagnosed up to 2008. Written informed consent was obtained from all study participants.
Quantitative PCR for F. nucleatum
DNA was extracted from colorectal carcinoma tissue in whole-tissue sections of FFPE tissue blocks using QIAamp DNA FFPE Tissue Kit (Qiagen). We performed a quantitative PCR assay to measure the amount of tissue F. nucleatum DNA, after assay validation as previously described.21 Custom TaqMan primer/probe sets (Applied Biosystems) for the nusG gene of F. nucleatum and for the reference human gene, SLCO2A1 were used as previously described.7 Each reaction contained 80 ng of genomic DNA and was assayed in 20 μL reactions containing 1× final concentration TaqMan Environmental Master Mix 2.0 (Applied Biosystems) and each TaqMan Gene Expression Assay (Applied Biosystems), in a 96-well optical PCR plate. Amplification and detection of DNA was performed with the StepOnePlus real-time PCR Systems (Applied Biosystems) using the following reaction conditions: 10 min at 95°C and 45 cycles of 15 s at 95°C and 1 min at 60°C.
Our validation study has previously shown that in colorectal carcinoma cases with detectable F. nucleatum DNA, the cycle threshold (Ct) values in the quantitative PCR for F. nucleatum and SLCO2A1 decreased linearly with the log-transformed amount of input DNA from the same specimen (r2>0.99), and that the interassay coefficient of variation of Ct values from the same specimen in five different batches was 1% or less for all targets.21 Each specimen was analysed in duplicate for each target in a single batch, and we used the mean of the two Ct values for each target. The amount of tissue F. nucleatum DNA in each specimen was calculated as a relative unitless value normalised with SLCO2A1 using the 2−ΔCt method (where ΔCt=‘the mean Ct value of F. nucleatum’—‘the mean Ct value of SLCO2A1’).21
Analyses of MSI, DNA methylation, and KRAS, BRAF and PIK3CA mutations
DNA was extracted from colorectal carcinoma tissue in whole-tissue sections from FFPE tissue blocks. MSI status was analysed with the use of 10 microsatellite markers (D2S123, D5S346, D17S250, BAT25, BAT26, BAT40, D18S55, D18S56, D18S67 and D18S487) as previously described.25 We defined MSI-high as the presence of instability in ≥30% of the markers, and MSI-low/microsatellite stable (MSS) as instability in <30% of the markers. Methylation analyses of long interspersed nucleotide element-1 (LINE-1)26 ,27 and eight promoter CpG islands specific for CIMP (CACNA1G, CDKN2A, CRABP1, IGF2, MLH1, NEUROG1, RUNX3 and SOCS1)28 ,29 were performed. PCR reaction and pyrosequencing were performed for KRAS (codons 12, 13, 61 and 146),30 ,31 BRAF (codon 600)25 and PIK3CA (exons 9 and 20).32 ,33
Statistical analysis
All statistical analyses were conducted using SAS (V.9.3, SAS Institute, Cary, North Carolina, USA) and all p values were two-sided. Our primary hypothesis testing was a linear trend test in Cox proportional hazards regression model to assess an association of the amount of tissue F. nucleatum DNA with colorectal cancer-specific mortality. Overall mortality was a secondary outcome. Cases with detectable F. nucleatum DNA were categorised as low versus high based on the median cut point amount of F. nucleatum DNA, while cases without detectable F. nucleatum DNA were categorised as negative. Test for a linear trend was conducted across the ordinal categories (negative (0), low (1), and high (2)) of the amount of tissue F. nucleatum DNA as a continuous variable in the Cox proportional hazards regression model. A two-sided α level was set at 0.05 for our primary hypothesis testing.
For analyses of colorectal cancer-specific mortality, deaths as a result of other causes were censored. To control for confounders, we used multivariable Cox proportional hazards regression models. Multivariable models included disease stage as a stratifying variable using strata function in the SAS proc phreg command. In addition to the amount of tissue F. nucleatum DNA, the multivariable model initially included sex, age at diagnosis (continuous), year of diagnosis (continuous), family history of colorectal cancer in a first-degree relative (present vs absent), tumour location (proximal colon vs distal colon vs rectum), MSI (high vs low/MSS), CIMP (high vs low/negative), KRAS (mutant vs wild type), BRAF (mutant vs wild type), PIK3CA (mutant vs wild type) and tumour LINE-1 methylation level (continuous). A backward stepwise elimination with a threshold of p=0.05 was used to select variables in the final models. For cases with missing information on LINE-1 methylation level (5.1%), we assigned a separate indicator variable. For cases with missing information in any of the categorical covariates (family history of colorectal cancer in a first-degree relative (0.4%), tumour location (0.3%), MSI (4.3%), CIMP (8.5%), KRAS (7.5%), BRAF (3.6%) and PIK3CA (9.3%)), we included these cases in the majority category of a given covariate to minimise the number of variables in multivariable Cox models. We confirmed that excluding the cases with missing information in any of the covariates did not substantially alter results (data not shown). Previous experimental studies provide evidence for potentiating effects of F. nucleatum on colorectal tumour progression.16 ,18 If the hypothesis that tissue F. nucleatum is associated with shorter survival is true, high disease stage and poor tumour differentiation (both of which are associated with tissue F. nucleatum in the current study) are likely mediators on the causal pathway from the amount of tissue F. nucleatum DNA to shorter survival. Thus, we did not include disease stage or tumour differentiation in multivariable Cox proportional hazards regression models in our secondary analysis. The proportionality of hazards assumption was assessed by a time-varying covariate, using an interaction term of colorectal cancer-specific survival term and the amount of F. nucleatum DNA (p=0.45). The Kaplan-Meier method was used to describe the distribution of colorectal cancer-specific survival and overall survival, and the log-rank test for trend was performed to assess a linear trend in survival probability across the ordinal categories (negative (0), low (1) and high (2)) of the relative amount of tissue F. nucleatum DNA.
All cross-sectional univariable analyses for clinical, pathological and tumour molecular associations were secondary exploratory analyses, with an adjusted two-sided α level of 0.003 (=0.05/16) for multiple hypothesis testing. To assess associations between the ordinal categories of the amount of tissue F. nucleatum DNA and other categorical variables, Fisher's exact test was performed. To compare mean age and mean LINE-1 methylation levels, an analysis of variance assuming equal variances was performed.
We conducted logistic regression analyses to assess associations of the amount of tissue F. nucleatum DNA (an ordinal predictor variable (negative, low and high)) with each component of the American Joint Committee on Cancer staging system, including pT stage (an ordinal outcome variable (pT1 vs pT2 vs pT3 vs pT4)), pN stage (an ordinal outcome variable (pN0 vs pN1 vs pN2)), and M stage (a binary outcome variable (M0 vs M1)). Test for a linear trend was conducted across the ordinal categories (negative (0), low (1) and high (2)) of the amount of tissue F. nucleatum DNA as a continuous variable in logistic regression models. The multivariable logistic regression model initially included age (continuous), sex, year of diagnosis (continuous), family history of colorectal carcinoma in a first-degree relative (present vs absent), tumour location (proximal colon vs distal colon vs rectum), MSI (high vs low/MSS), CIMP (high vs low/negative), KRAS (mutant vs wild type), BRAF (mutant vs wild type), PIK3CA (mutant vs wild type) and LINE-1 methylation level (continuous). For cases with missing information in any of the covariates, we assigned a separate (‘missing’) indicator variable. A backward stepwise elimination with a threshold of p=0.05 was used to select variables in the final models. To assess independent associations of MSI, CIMP and BRAF mutation status (predictor variables) with the amount of tissue F. nucleatum DNA (an ordinal outcome variable (negative vs low vs high)), we performed multivariable ordinal logistic regression analysis. In addition to MSI, CIMP and BRAF mutation status, the multivariable ordinal logistic regression model initially included age (continuous), sex, year of diagnosis (continuous), family history of colorectal carcinoma in a first-degree relative (present vs absent), tumour location (proximal colon vs distal colon vs rectum), KRAS (mutant vs wild type), PIK3CA (mutant vs wild type) and LINE-1 methylation level (continuous). For cases with missing information in any of the covariates, we assigned a separate (‘missing’) indicator variable. A backward stepwise elimination was performed with a threshold of p=0.05 to select covariates in the final model. We assessed the proportional odds assumption in the ordinal logistic regression model, which was generally satisfied (p≥0.06).
Results
F. nucleatum in colorectal cancer tissue and patient mortality
We measured the relative amount of F. nucleatum DNA in tumour tissue of 1069 colorectal carcinoma cases within the Nurses’ Health Study and the Health Professionals Follow-up Study, using the quantitative PCR assay as previously described.21 Table 1 shows clinical, pathological and tumour molecular features of the 1069 cases.
Characteristics according to the amount of Fusobacterium nucleatum DNA in colorectal cancer tissue
F. nucleatum DNA was detected in colorectal carcinoma tissue in 134 (13%) of the 1069 cases. We equally dichotomised the cases with detectable F. nucleatum DNA into low versus high.
To test our primary hypothesis, we examined the relationship between the relative amount of tissue F. nucleatum DNA and patient mortality (table 2).
The amount of Fusobacterium nucleatum DNA in colorectal cancer tissue and patient mortality
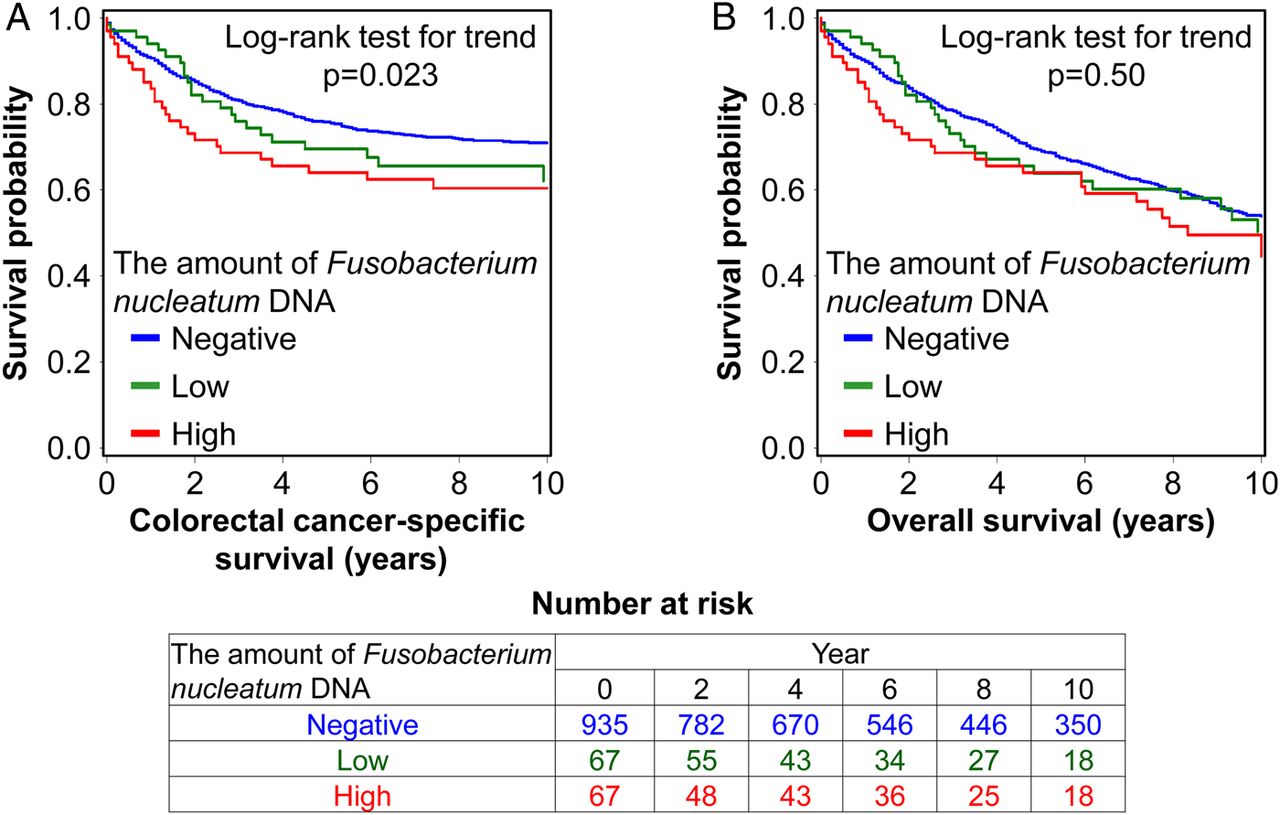
In the 1069 colorectal cancer cases, there were 578 deaths, including 315 colorectal cancer-specific deaths, during a median patient follow-up of 10.7 years (IQR: 7.0–15.8) for censored cases. The amount of tissue F. nucleatum DNA was associated with higher colorectal cancer-specific mortality in univariable (p for trend=0.023) and multivariable Cox regression analyses (p for trend=0.020). Compared with F. nucleatum-negative cases, multivariable HRs for colorectal cancer-specific mortality in F. nucleatum-low cases and F. nucleatum-high cases were 1.25 (95% CI 0.82 to 1.92) and 1.58 (95% CI 1.04 to 2.39), respectively. In Kaplan-Meier analysis, a higher amount of tissue F. nucleatum DNA was associated with shorter colorectal cancer-specific survival (p=0.023 by the log-rank test for trend; figure 1A).

{kind=link}
Kaplan-Meier curves for colorectal cancer-specific survival (A) and overall survival (B) according to the amount of Fusobacterium nucleatum DNA in colorectal cancer tissue. The p value was calculated by the log-rank test for trend (two-sided). The table (bottom) shows the number of patients who remained alive and at risk of death at each time point after the diagnosis of colorectal cancer.
In a secondary analysis of overall mortality as an outcome, the amount of tissue F. nucleatum DNA was not significantly associated with overall mortality (p for trend=0.99; table 2: p=0.50 by the log-rank test for trend; figure 1B).
Considering that disease stage and tumour differentiation may be on the causal pathway from the amount of tissue F. nucleatum DNA to shorter survival, we also used the multivariable Cox regression model that did not include disease stage or tumour differentiation in a further secondary analysis, and observed a significant association of the amount of tissue F. nucleatum DNA with higher colorectal cancer-specific mortality (p for trend=0.0001; see online supplementary table S1).
Tissue F. nucleatum in relation to other features in colorectal cancer
As shown in table 1, a higher amount of tissue F. nucleatum DNA was associated with proximal tumour location, higher pT stage, poor tumour differentiation, MSI-high, MLH1 hypermethylation, CIMP-high and BRAF mutation (p≤0.001 with the adjusted α level of 0.003 for multiple hypothesis testing).
As an exploratory analysis, we examined associations of tissue F. nucleatum DNA with pT stage, pN stage and M stage (table 3).
Association of the amount of Fusobacterium nucleatum DNA in colorectal cancer tissue with each component of the American Joint Committee on Cancer staging system
The amount of tissue F. nucleatum DNA was associated with higher pT stage in univariable (p for trend=0.0003) and multivariable ordinal logistic regression analyses (p for trend=0.0007). The association of tissue F. nucleatum DNA with pN or M stage was not statistically significant (p for trend ≥0.029 with the adjusted α level of 0.003; table 3).
Table 4 shows the distribution of colorectal cancer cases according to combined MSI/CIMP/BRAF status.
The amount of Fusobacterium nucleatum DNA in colorectal cancer tissue in relation to combined MSI/CIMP/BRAF status
As an exploratory analysis, we performed multivariable ordinal logistic regression analysis to assess independent associations of MSI, CIMP and BRAF mutation status with the amount of tissue F. nucleatum DNA (table 5).
Ordinal logistic regression analysis to assess independent associations of MSI, CIMP and BRAF mutation status with the amount of Fusobacterium nucleatum DNA in colorectal cancer tissue
The amount of tissue F. nucleatum DNA was associated with MSI-high (multivariable OR, 5.22; 95% CI 2.86 to 9.55), independent of CIMP and BRAF mutation status. In contrast, CIMP or BRAF mutation was not associated with F. nucleatum after adjusting for MSI status.
Discussion
We conducted this study to test the hypothesis that a higher amount of tissue F. nucleatum might be associated with worse clinical outcome in colorectal cancer. Using the database of the 1069 colorectal carcinoma cases in the two US nationwide prospective cohort studies, we observed the association between the amount of tissue F. nucleatum DNA and higher colorectal cancer-specific mortality.
Recent studies have provided mechanistic insights into the relationship between F. nucleatum and colorectal tumour progression. F. nucleatum expresses the virulence factor FadA on the bacterial cell surface, which has been shown to activate the WNT signalling pathway in colorectal carcinoma cells and promote colorectal tumour growth.18 F. nucleatum may inhibit T cell-mediated immune responses against colorectal tumours in the ApcMin/+ mouse model.16 ,19 Our recent study has shown an inverse association between the amount of tissue F. nucleatum DNA and CD3+ T cell density in colorectal cancer.21 In the present study, a higher amount of tissue F. nucleatum DNA was associated with a higher pT stage and worse clinical outcome. These lines of evidence together with the findings from our current study support the hypothesis that F. nucleatum-high colorectal cancers may represent a more biologically aggressive cancer subtype. In light of possible roles of F. nucleatum in downregulating T cell-mediated antitumour immune responses and in promoting colorectal tumour progression, future investigations may be warranted to explore potential influence of tissue F. nucleatum on efficacy of the T cell-based immunotherapies for colorectal cancer.
Colorectal cancers develop through the accumulation of genetic and epigenetic alterations, influenced by microbial and other environmental exposures and host responses to the exposures.34–38 In the current study, a higher amount of tissue F. nucleatum DNA was associated with key tumour molecular features of colorectal cancer, including MSI-high, CIMP-high, LINE-1 hypomethylation and BRAF mutation, which have been associated with clinical outcome in colorectal cancer.39–46 By using over 1000 human colorectal carcinoma cases, to our knowledge we provided the first evidence that supports the prognostic significance of the amount of F. nucleatum DNA in colorectal cancer tissue, independent of clinical, pathological and major tumour molecular features. In addition, our current study could demonstrate that tissue F. nucleatum was associated with MSI-high, but not with CIMP-high or BRAF mutation in multivariate analysis that adjusted for each other.
We acknowledge limitations of our study. First, the data on cancer recurrence were limited in the two cohorts. However, colorectal cancer-specific mortality is a reasonable cancer-specific outcome in the current study, which used the population-based data of long-term patient follow-up, since median survival for recurrent (local or metastatic) colorectal cancer was approximately 10–20 months during much of the time period of this study.47 Second, the data on cancer treatment were limited. However, it is unlikely that the distribution of chemotherapy use could substantially differ according to the amount of tissue F. nucleatum DNA, because the data on tissue F. nucleatum DNA were not available for treatment decisions.
Strengths of this study include the use of our molecular pathological epidemiology48–51 database (of over 1000 colorectal carcinoma cases in the two US nationwide, prospective cohort studies), which integrated epidemiological exposures, clinicopathological features, key tumour molecular features and tissue F. nucleatum DNA in colorectal carcinoma. Importantly, our colorectal cancer specimens were derived from a large number of hospitals in diverse settings across the US, which increases the generalisability of our findings. In addition, the sample size and comprehensiveness of the colorectal cancer database enabled us to assess the prognostic significance of tissue F. nucleatum DNA, controlling for potential confounders.
In conclusion, the amount of tissue F. nucleatum DNA was associated with higher colorectal cancer-specific mortality. These findings need to be validated in additional populations, as analytical and clinical validations are important to implement clinical use of tumour tissue biomarkers.52 Upon validation, F. nucleatum DNA in colorectal carcinoma tissue may serve as a prognostic biomarker. In addition, our population-based data may provide insights for future studies to develop strategies for colorectal cancer prevention and treatment through targeting the microbiota.
Acknowledgments
The authors thank the participants and staff of the Nurses’ Health Study and the Health Professionals Follow-up Study for their valuable contributions as well as the following state cancer registries for their help: AL, AZ, AR, CA, CO, CT, DE, FL, GA, ID, IL, IN, IA, KY, LA, ME, MD, MA, MI, NE, NH, NJ, NY, NC, ND, OH, OK, OR, PA, RI, SC, TN, TX, VA, WA, WY.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors KM, RN, ZRQ and YC contributed equally as co first authors. JAM, ATC, CSF and SO contributed equally as co last authors. All authors contributed to review and revision. DAM, ELG, LAG, GJF, GD, WSG, CH MM, JAM, ATC, CSF and SO developed the main concept and designed the study. ATC, CSF and SO wrote grant applications. KM, RN, ZRQ, YC, YS, JY, RD, YM, MS, JAM, ATC, CSF and SO were responsible for collection of tumour tissue, and acquisition of epidemiological, clinical and tumour tissue data, including histopathological and immunohistochemical characteristics. KM, YS, ADK, MG, SB, DAM, WSG, CH, MM, CSF and SO performed data analysis and interpretation. KM, RN and SO drafted the manuscript. JAN, MS, MG, HB, ELG, GJF, GD, WSG, MM, JAM, ATC, CSF and SO contributed to editing and critical revision for important intellectual contents.
Funding This work was supported by US National Institutes of Health (NIH) grants (P01 CA87969 to S E Hankinson; UM1 CA186107 to M J Stampfer; P01 CA55075 and UM1 CA167552 to W C Willett; P50 CA127003 to CSF; R01 CA137178 to ATC; R01 CA151993 and R35 CA197735 to SO; and K07 CA190673 to RN); and by grants from The Paula and Russell Agrusa Fund for Colorectal Cancer Research, The Friends of the Dana-Farber Cancer Institute, Bennett Family Fund, and the Entertainment Industry Foundation through National Colorectal Cancer Research Alliance. KM is supported by a fellowship grant from Uehara Memorial Foundation and a grant from Program for Advancing Strategic International Networks to Accelerate the Circulation of Talented Researchers from Japanese Society for the Promotion of Science.
Disclaimer The authors assume full responsibility for analyses and interpretation of these data. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests ATC previously served as a consultant for Bayer Healthcare, Millennium Pharmaceuticals, Pozen and Pfizer. This study was not funded by Bayer Healthcare, Millennium Pharmaceuticals, Pozen or Pfizer. MM applies a patent on Fusobacterium in colorectal cancer diagnosis, and has ownership interest in and is a consultant and advisory board member for Foundation Medicine.
Ethics approval The institutional review boards at the Harvard TH Chan School of Public Health and the Brigham and Women's Hospital (Boston, Massachusetts, USA).
Provenance and peer review Not commissioned; externally peer reviewed.
Use of standardised official symbols: We use HUGO (Human Genome Organisation)-approved official symbols for genes and gene products, including APC, BRAF, CACNA1G, CDKN2A, CRABP1, IGF2, KRAS, MLH1, NEUROG1, PIK3CA, RUNX3, SLCO2A1 and SOCS1; all of which are described at www.genenames.org.