Article Text

Abstract
Background The long-term performance of colorectal cancer (CRC) screening programmes based on a 2-year faecal immunochemical test (FIT) is still unclear.
Methods In a sample of 50 to 69-year-olds repeatedly screened with the FIT (OC-Hemodia latex agglutination test; cut-off: 20 µg haemoglobin/g faeces), we examined: (1) the FIT positivity rate, the CRC and advanced adenoma detection rate and the FIT’s positive predictive value (PPV) for advanced neoplasia, at each round of screening and (2) the cumulative CRC and advanced adenoma detection rate after five rounds of FIT.
Results Over 12 years (2002–2014), 123 347 individuals were administered the FIT up to six times, and 781 CRCs and 4713 advanced adenomas were diagnosed. The CRC and advanced adenoma detection rates declined substantially from the first to the third (rate ratio (RR) 0.25, 95% CI 0.20 to 0.32) and second (RR 0.51, 95% CI 0.47 to 0.56) rounds, respectively, and then remained stable. The PPV for advanced neoplasia dropped by 18% in the second round (RR 0.82, 95% CI 0.77 to 0.89), with no further reduction thereafter due to a concomitant decline in the FIT positivity rate (RR first to sixth rounds: 0.56, 95% CI 0.53 to 0.60).
The cumulative CRC and advanced adenoma detection rates over five consecutive rounds were 8.5‰ (95% CI 7.8 to 9.2), and 58.9‰ (95% CI 56.9 to 61.0), respectively.
Conclusions Repeated FIT significantly reduces the burden of colorectal disease while facilitating an efficient use of colonoscopy resources. The cumulative detection rate after five rounds of FIT is similar to primary screening with colonoscopy, supporting the need to account for the cumulative sensitivity of repeated FITs when evaluating the test’s efficacy.
- colorectal cancer screening
- colorectal cancer
- colonic neoplasms
- colonic polyps
- colonoscopy
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Colorectal cancer (CRC) screening based on a faecal immunochemical test (FIT) reduces cancer-related mortality.
The rate of advanced neoplasia detection drops substantially between the first and second rounds of FIT programmes, but data on the long-term performance of FIT-based screening programmes are still lacking.
While population screening programmes have shown that FIT reduces the incidence of CRC, their value is still debated because FIT is less sensitive than colonoscopy in detecting advanced adenomas.
What are the new findings?
The CRC detection rate dropped by 75% from the first to the third screening rounds, and the advanced adenoma detection rate dropped by 49% from the first to the second rounds, remaining stable thereafter.
The positive predictive value of FIT for advanced neoplasia dropped by 18% in the second round, then remained stable.
For every 1000 persons screened biennially from ages 50 to 54 years over 10 years, an estimated four to seven colorectal cancers and 42 to 48 advanced adenomas are diagnosed, and 170 to 180 persons have at least one positive test result.
The cumulative CRC and advanced adenoma detection rates over five consecutive rounds of FIT were similar to those estimated after one-off primary screening with colonoscopy.
How might it impact on clinical practice in the foreseeable future?
Screening programmes based on multiple FITs enable an efficient use of colonoscopy resources.
The lower burden of disease among women and younger age groups may justify the adoption of differentiated screening protocols after the third FIT.
The cumulative CRC and advanced adenoma detection rates support the need to account for the overall sensitivity of repeated tests when assessing the efficacy of the FIT.
Introduction
The faecal immunochemical test (FIT) has been recommended for colorectal cancer (CRC) screening purposes in Europe1 because it is associated with higher participation rates and a greater sensitivity for CRC and advanced adenoma than other screening options, such as the guaiac faecal occult blood test.2–6
No randomised controlled trials have been conducted on CRC screening programmes based on the FIT, so the only available evidence of their impact comes from population screening programmes. Published data suggest that FIT-based screening reduces both CRC-related mortality,7–10 thanks to an earlier diagnosis and the incidence of CRC,7 11 12 because advanced adenomas are detected and removed at post-FIT colonoscopy.
The value of FIT-based screening programmes in reducing the incidence of CRC is still debatedm however, because the FIT is less sensitive than colonoscopy in detecting advanced adenoma.13 According to a recent systematic review for the US Preventive Services Task Force, the FIT’s sensitivity in detecting advanced adenoma ranged from 22.2% to 40.3%.13 Most of the available studies compared colonoscopy with a single FIT, whereas the latter’s efficacy derives from the cumulative sensitivity of repeated tests.14–16 Nonetheless, the long-term advanced adenoma and CRC detection rate achieved by a formally structured FIT-based screening programmes remains unclear, largely because previous studies were limited to a short-term horizon with few repeated rounds.14 17–19
As repeated tests account for the majority of FITs performed as part of established screening programmes (eg, 76.4% of all FITs performed as part of the Veneto Region’s programmes in 2013),20 screening protocols need to ensure the most efficient combined use of FITs and endoscopic resources. A substantial drop in the advanced neoplasia detection rate has been identified between the first and second rounds of FIT programmes and attributed mainly to prevalent lesions being excluded in the first round.15 16 The positive predictive value (PPV) of FIT positivity at colonoscopy likewise declines with subsequent repeated rounds, negatively affecting the efficient use of endoscopy as a result.
The aims of this study were: (1) to assess the performance of a screening programme based on a FIT every 2 years in a very large population-based cohort followed up for six test rounds and (2) to quantify the cumulative CRC and advanced adenoma detection rates.
Methods
Setting
The Veneto Region (north-eastern Italy; population 4 915 000) is covered by several local health authorities, which introduced CRC screening programmes between 2002 and 2009. For the present study, we selected five screening programmes (conducted in Belluno, Feltre, Alto Vicentino, Pieve di Soligo and Bussolengo) started in 2002–2004. Overall, the 50 to 69-year-old target population, as of 1 January 2002, included 215 235 residents. Over the whole study period (2002–2015), the participation rate was 69.3%. All these programmes applied the same protocol throughout the study period. Individuals aged 50–69 years were invited to take a FIT every 2 years. The OC-Hemodia latex agglutination test, developed with the OC-Sensor Micro instrument (Eiken, Tokyo, Japan), was used. Quantitative haemoglobin analysis was performed with automated instruments. The cut-off for test positivity was 20 µg Hb/g faeces (100 ng Hb/mL buffer). Colonoscopy was recommended for individuals testing positive on the FIT, after which they were referred for surgery, postcolonoscopy surveillance or further rounds of FIT, depending on its outcome. Subjects with a false-positive FIT result were invited back for screening with FIT after 5 years. All the data collected on each screening round (FIT plus any colonoscopy) were recorded using dedicated software and are available as individual records.
Dataset
The screening database was used to identify the cohort of subjects who had a FIT during the first round of the five study programmes. Then the records of all their subsequent screening FITs, performed up until 31 December 2015, were obtained and ordinally numbered for each subject. To ascertain the performance of the rounds of FIT repeated with the established frequency (ie, every 2 years), subjects were censored, and any subsequent tests were disregarded if they failed to comply with the 2-yearly schedule at any round (ie, subjects who attended the first and the second round, missed the third and attended the fourth were censored after the second round). Overall, 31 393 tests were rejected for this reason.
The result of each FIT was recorded, together with any colonoscopy performed. The outcome of colonoscopy could be: CRC; advanced adenoma (≥1 cm in diameter, of villous/tubulovillous type or with high-grade dysplasia); non-advanced adenoma or negative. Up to three lesions (the most severe) were recorded for each colonoscopy.
Outcome measures
The following indicators were calculated at each FIT round:
Participation rate;
FIT positivity rate;
FIT+subjects’ compliance with recommendation to undergo colonoscopy;
CRC, advanced adenoma and non-advanced adenoma detection rate (x1000 subjects screened);
PPV of FIT positivity for advanced neoplasia (CRC or advanced adenoma) at colonoscopy (%);
Number needed to screen (NNScreen) and number needed to scope (NNScope) to detect one case of advanced neoplasia;
Cumulative FIT positivity rate (%) and CRC and advanced adenoma detection rate (x1000 subjects screened) after five rounds of FIT (ie, 10 years of the programme).
Statistical analysis
Descriptive statistics, stratified by screening round, were used to summarise the results of the screening programme. The different rounds were compared using Pearson’s χ2 test and Snedecor’s F for homogeneity of proportions, as appropriate.
A multivariable analysis was run to examine the association of each indicator with gender, age (in 5-year brackets) and screening round. For each indicator, we computed the rate ratios (RR), with 95% Wald CI, estimated using Poisson’s regression and taking the 50 to 54-year-old group, male gender and the first screening round for reference.
The Kaplan-Meier method was used in the survival analysis to calculate the cumulative FIT positivity and the CRC and advanced adenoma detection rates (after five rounds). For this analysis, each subject contributed to the person-time with the interval between the dates of their first and last FIT or last colonoscopy (if their last FIT had been positive). The analysis was limited to subjects who were 50–64 years old at their first FIT. All statistical tests were two sided and statistical significance was set at 0.05. The SAS, V.9.4 (SAS Institute, Cary, NC) was used for all the statistical analyses.
Results
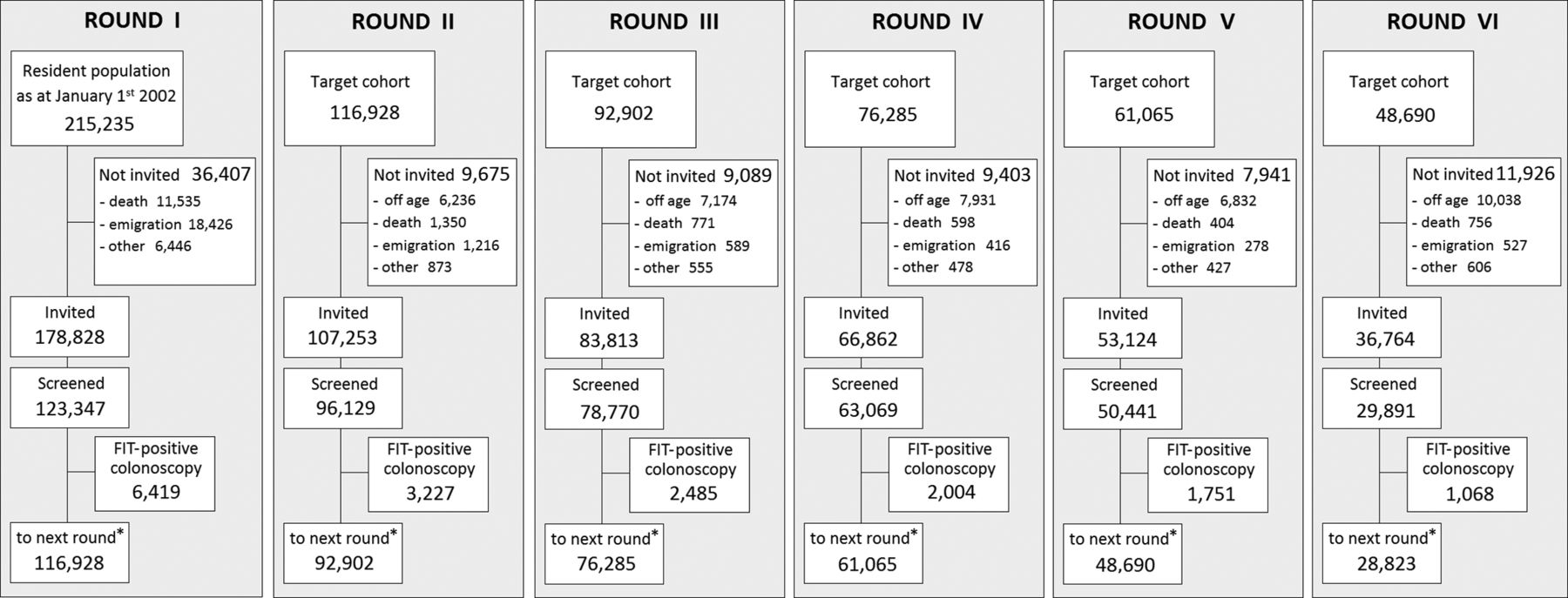
Figure 1 shows the flowchart of the study cohort. Overall, 178 828 individuals were invited for a first round of FIT and a cohort of 123 347 responded to the invitation (69%). The screening protocol established that FIT-negative subjects should be invited to repeat the test every 2 years. By the end of the study, data were available on 441 647 FITs. Table 1 shows the number of FITs performed at each round of screening: it ranged from 123 347 for the first round to 29 891 for the sixth. The mean age of the target population rose from 59.1 years at the time of the first round to 64.5 years at the sixth. Meanwhile, the proportion of males declined from 47.7% to 45.5%. The participation rate was lowest for the first round (69%), and exceeded 94% in the third, fourth and fifth rounds.

Flowchart of the study cohort by screening round. *Including FIT-negative subjects plus FIT-positive subjects who did not comply with colonoscopy. FIT, faecal immunochemical test.
Main characteristics of the screening results, overall and by screening round
FIT positivity rate
Considering all screening rounds, the FIT positivity rate was 4.1%. It dropped from the first (5.7%) to the second round (3.6%) and ranged from 3.3% to 3.8% in subsequent rounds. On multivariable analysis, it dropped by 39% at the second round compared with the first and by 43%–47% at subsequent rounds (table 2, figure 2A).

Rate ratios for FIT positivity (A), colorectal cancer detection rate (B), advanced adenoma detection rate (C) and PPV of FIT + for advanced neoplasia on colonoscopy (D) by screening round. Data were adjusted for gender and age. Vertical lines indicate 95% CIs. FIT, faecal immunochemical test; PPV, positive predictive value; RR, rate ratio.
Multivariable analysis to identify predictors of different performance indicators (RR (95% CIs))
FIT positivity was associated with age (RR by 5-year increase in age: 1.21, 95% CI 1.19 to 1.23) and gender (RR for women: 0.66, 95% CI 0.64 to 0.68).
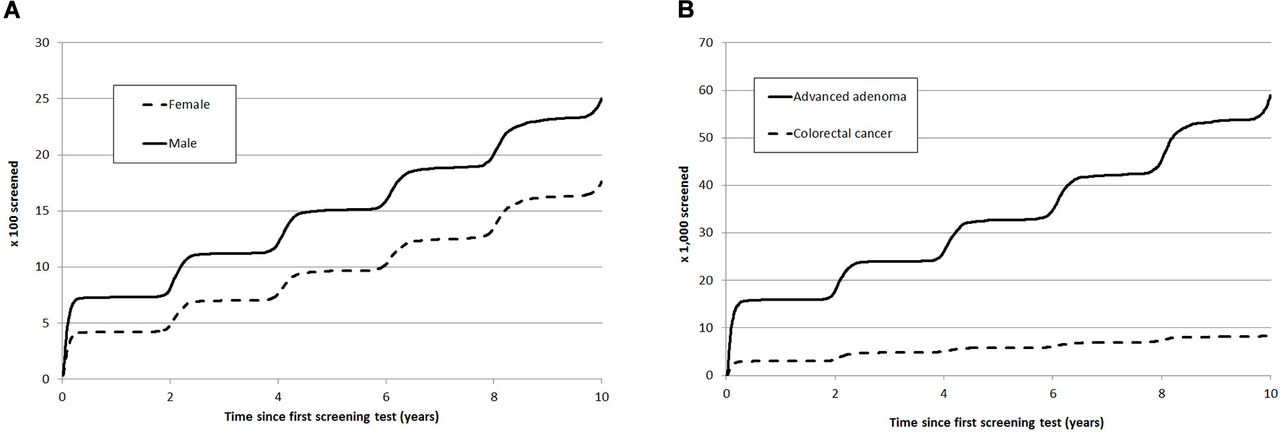
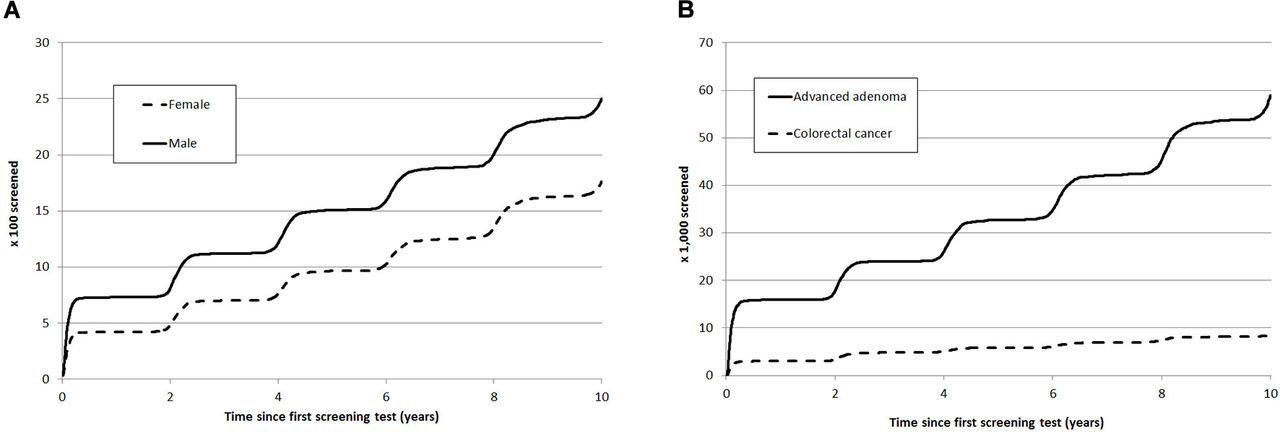
The cumulative FIT positivity rate over five consecutive rounds in the whole sample aged 50–64 years at the baseline was 17.6% for women (95% CI 17.2 to 18.1) and 25% for men (95% CI 24.5 to 25.5) (figure 3A). By baseline age and gender, the cumulative FIT positivity rate ranged from 14.5% (95% CI 13.9 to 15.1) in 50 to 54-year-old women to 43.4% (95% CI 39.0 to 48.1) in men aged 60–64 (table 3).
{kind=link}
{kind=link}
{kind=link}
Cumulative FIT positivity by gender (%) (A) and cumulative colorectal cancer and advanced adenoma detection rate (‰) (B) after five rounds of screening in subjects of both genders aged 50–64 years at first screening test (Kaplan-Meier estimates). FIT, faecal immunochemical test.
Cumulative FIT positivity (%) and colorectal cancer and advanced adenoma detection rate (‰) after five rounds of screening, by gender and age at first screening (Kaplan-Meier estimates)
Overall, 781 patients were diagnosed with CRC, 4713 with advanced adenoma and 2844 with non-advanced adenoma.
CRC detection rate
The CRC detection rate was 3.34‰ at the first round and 1.69‰ at the second, then lower than 1‰ at subsequent rounds (table 1). The reduction was substantial between the first and second rounds (RR 0.48, 95% CI 0.40 to 0.57) and between the first and third rounds (RR 0.25, 95% CI 0.20 to 0.32), while further decreases in subsequent rounds were negligible (table 2, figure 2B). A statistically significant association was apparent with both age (RR for 5-year increase 1.45, 95% CI 1.35 to 1.56) and gender (RR for women 0.51, 95% CI 0.44 to 0.59).
Adenoma detection rate
The advanced adenoma detection rate was 15.9‰ at the first round and 8.5‰ at the second (table 1). This reduction was significant (RR 0.51, 95% CI 0.47 to 0.56), while there were no relevant further reductions at subsequent rounds (table 2, figure 2C). A statistically significant association was apparent with both age (RR for 5-year increase 1.27, 95% CI 1.23 to 1.31) and gender (RR for women 0.45, 95% CI 0.42 to 0.48).
The non-advanced adenoma detection rate was 7.5‰ at the first round and less than 7.0‰ at subsequent rounds. On multivariable analysis, there was a reduction of about one in four between the first and second rounds (RR 0.76, 95% CI 0.68 to 0.84), and no further changes thereafter (table 2).
Cumulative CRC and advanced adenoma detection rate
After 5 rounds of screening in the whole sample of 50 to 64-year-olds, the cumulative CRC and advanced adenoma detection rates were 8.5‰ (95% CI 7.8 to 9.2) and 58.9‰ (95% CI 56.9 to 61.0), respectively (figure 3B). The cumulative CRC detection rate ranged from 4.3‰ (95% CI 3.4 to 5.6) in women aged 50–54 to 25.9‰ (95% CI 17.2 to 38.9) in men aged 60–64 (table 3). The cumulative advanced adenoma detection rate was associated with age and gender, too, ranging from 29.5‰ (95% CI 26.7 to 32.7) in women aged 50–54 to 144.1‰ (95% CI 111.9 to 184.6) in men aged 60–64.
PPV of FIT positivity for advanced neoplasia
The highest PPV of a FIT + result for advanced neoplasia at colonoscopy emerged for the first round (36.9%) and dropped by around 20% at all subsequent rounds (table 2, figure 2D).
NNScreen and NNScope to detect one case of advanced neoplasia
Overall, 52 individuals needed to be screened at the first round and around 100 at subsequent rounds to detect one case of advanced neoplasia. Compared with the first round, the NNScreen was 88% higher at the second round, and more than twice as high at subsequent rounds (table 2). Twice as many women as men had to be screened to detect one case of advanced neoplasia (RR 2.13, 95% CI 2.12 to 2.15), while the NNScreen dropped by 22% for every 5-year increase in age (RR 0.78, 95% CI 0.78 to 0.78).
The number of colonoscopies needed to detect one advanced neoplasia was 2.7 in the first round, then ranged from 3.3 to 3.5 (RR first to sixth round 1.27, 95% CI 1.19 to 1.36) in subsequent rounds.
Discussion
In a FIT-based CRC screening programme, the main performance parameters—FIT positivity and advanced neoplasia detection rates—reach a steady state already in the second round, with the notable exception of the CRC detection rate, which continues to decrease with subsequent rounds. Although fewer lesions are detected over time, colonoscopy resources are used efficiently throughout the programme, as indicated by the relatively high PPV for advanced neoplasia at subsequent rounds.
CRC and adenoma detection rates
Unlike the case in previous studies,14 15 18 the large size of our study population enabled us to distinguish between the long-term CRC and advanced adenoma detection rates. This analysis newly revealed that the CRC detection rate continued to drop over several screening rounds, with a nearly twofold difference compared with advanced adenoma, that is, (RR first to sixth round: 0.18 vs 0.52). This particular trend may theoretically stem from a combination of at least three factors: (1) precancerous lesions occur more frequently and before any invasive neoplastic growth; (2) FIT is more sensitive for CRC than for advanced adenoma and (3) some cancers are prevented thanks to the removal of precancerous lesions (ie, advanced adenomas). This interpretation is in keeping with the finding that the non-advanced adenoma detection rate dropped by one in four from the first to the second round and then exhibited no further decline.
One relevant consequence of the very low CRC detection rate seen after the third round lies in that FIT for repeatedly screened individuals is effective primarily in the detection of advanced adenoma, differing from the first two rounds, where the much higher rate of invasive CRC detection somewhat marginalises the concomitant detection of precancerous lesions.
A strong association was seen consistently across FIT rounds between age and/or gender and the rates of detection of both CRC and advanced adenoma. Previous studies were either insufficiently powered to reveal this association or their analysis only considered the PPV of post-FIT colonoscopy.14 16–19 This evidence of a multidimensional association between FIT round, age and sex on the one hand and advanced neoplasia detection rate on the other suggests that different FIT-based screening policies could be considered for different groups in the target population, as some carry a lower risk of disease due to their age or gender or FIT screening history. The cut-off for positivity could be raised, for instance, or the interval between screenings could be extended for women and younger individuals after their third FIT, provided sensitivity for CRC does not drop below reference standards (ie, proportional incidence <20% for the first interval/year, <40% for the second).21 This may be particularly important when coping with limited resources and the need to prioritise people at higher risk for screening.
PPV of FIT positivity for advanced neoplasia
Although the rate of detection of clinically relevant lesions decreases significantly over time in repeatedly screened populations, the PPV for our sample dropped by only one-fifth after the first round. This effect is due to the concomitant reduction in FIT positivity and consequently in the number of post-FIT colonoscopies. The PPV observed at subsequent rounds remains steady at around 30%, which represents the standard considered desirable by the GISCoR (Italian Group for Colorectal Screening).22 Similar figures were recently reported in a study based on annual FIT screening.19
Cumulative FIT positivity and CRC and advanced adenoma detection rates
We computed the cumulative performance of FIT over five consecutive screening rounds and compared it with the performance of one-off primary screening colonoscopies (given the recommended 10-year interval between the latter procedures).23
In the present FIT-based screening programme for 50 to 64-year-olds, the cumulative detection rates for CRC (0.85%) and advanced adenoma (5.9%) were similar with those reported for both an Italian primary colonoscopy screening (in subjects 50–69 years old: CRC 0.8%; advanced adenoma 6.0%)24 and in a US trial (subjects 50–84 years old: CRC 0.7%; advanced adenomas or sessile serrated polyps measuring ≥1 cm 7.6%).25 These figures do not allow for any direct comparison to be drawn on the efficacy of the two screening strategies (ie, primary endoscopy vs repeated FIT over a decade) in reducing the incidence and mortality of CRC. Our results nonetheless confirm that the efficacy of FIT screening depends on the cumulative sensitivity of repeated tests, so any comparison between FIT and other screening strategies (especially those based on one-off tests like endoscopy) should not consider only a single FIT because it would underestimate the test’s efficacy.
Finally, the PPV of repeated FITs for advanced neoplasia was higher than that of primary colonoscopy,24 which would suggest that FIT-based screening programmes perform better than one-off primary screening colonoscopies.
These data may be useful when preparing material to support informed decision-making, which should also include a quantification of one of the harmful effects of screening, that is, false-positive tests. The message for 50 to 54-year-olds could be: “For every 1000 persons in this age bracket screened biennially over 10 years, an estimated four to seven colorectal cancers and 42 to 48 advanced adenomas are diagnosed, 170 to 180 persons have at least one positive test result and 91 to 98 are recalled at least once for a colonoscopy that yields a negative result" (these last data are not shown here).
Study limitations
The present study has some limitations. First, we only considered FITs performed in subjects who had repeated the tests as scheduled. A sensitivity analysis showed that including the 31 393 tests that we had rejected (9% of all FITs performed after the first round) would have raised the FIT positivity rate in subsequent rounds by 6.8%, and the CRC and advanced adenoma detection rates by 6.9% and 6.0%, respectively. This is hardly surprising because the prevalence of lesions among individuals failing to take one or more scheduled FITs tends to increase, gradually returning to prescreening levels. The net result of our selection was thus a slightly lower estimate of some study parameters. Having said that, our cohort’s generally excellent compliance with the scheduled rounds of FIT would minimise any other risk of selection bias.20
A second limitation of our work lies in that some aspects of our screening protocol (such as our chosen cut-off for test positivity and 2-year test interval) may prevent our results from being generalised to all FIT-based programmes.
Third, the CRC and advanced adenoma detection rates were used as surrogates for cancer prevention because it would be impractical to measure the additional value of each subsequent round for the purposes of the long-term reduction in the incidence of CRC and the related mortality. This is widely accepted in the CRC screening literature, as all the available tests are compared in terms of the relative rates of detection of clinically relevant lesions.26–31 This approach has already been widely used in the CRC screening literature.26–31
Finally, the cumulative figures reported for the 60 to 64-year-old group slightly underestimate the results after five rounds because persons 62–63 and 64 years of age were only eligible for four and three FITs, respectively. We chose to report this realistic value rather than theoretically approximate this age group to the cumulative detection rate after five rounds completed by the 60 to 61-year-olds.
In conclusion, in a population repeatedly screened with FIT, we observed a significant reduction in the burden of colorectal disease, associated with an efficient use of colonoscopy resources throughout the programme. In such a scenario, the lower risk of disease among women and younger age groups warrants differentiated screening protocols beyond the third FIT.
After five rounds of FIT, the cumulative detection rates in our sample were similar to those achievable with a primary endoscopy strategy. The cumulative sensitivity of repeated FITs needs to be taken into account when evaluating the test’s efficacy.
Acknowledgments
The authors thank the staff members of the Veneto Tumour Registry, actively involved in both data collection and validation: Maddalena Baracco, Emanuela Bovo, Eva Carpin, Antonella Dal Cin, Annarita Fiore, Alessandra Greco, Stefano Guzzinati, Giancarla Martin, Laura Memo, Silvia Rizzato and Sandro Tognazzo.
References
Footnotes
Contributors MZ, MR: study concept and design; MZ, GC: analysis of data; MZ, CH: drafting of the manuscript; all authors: critical revision of the manuscript for content.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.