Article Text

Abstract
Gastroparesis is defined by delayed gastric emptying (GE) and symptoms of nausea, vomiting, bloating, postprandial fullness, early satiety and abdominal pain. Most common aetiologies include diabetes, postsurgical and postinfectious, but in many cases it is idiopathic. Clinical presentation and natural history vary by the aetiology. There is significant morbidity and healthcare utilisation associated with gastroparesis. Mechanistic studies from diabetic animal models of delayed GE as well as human full-thickness biopsies have significantly advanced our understanding of this disorder. An innate immune dysregulation and injury to the interstitial cells of Cajal and other components of the enteric nervous system through paracrine and oxidative stress mediators is likely central to the pathogenesis of gastroparesis. Scintigraphy and 13C breath testing provide the most validated assessment of GE. The stagnant gastroparesis therapeutic landscape is likely to soon see significant changes. Relatively newer treatment strategies include antiemetics (aprepitant), prokinetics (prucalopride, relamorelin) and fundic relaxants (acotiamide, buspirone). Endoscopic pyloromyotomy appears promising over the short term, especially for symptoms of nausea and vomiting. Further controlled trials and identification of the appropriate subgroup with pyloric dysfunction and assessment of long-term outcomes are essential. This review highlights the clinical presentation, diagnosis, mechanisms and treatment advancements for gastroparesis.
- GASTROPARESIS
- GASTRIC EMPTYING
- INTERSTITIAL CELLS OF CAJAL
- MACROPHAGES
- PROKINETIC AGENT
Statistics from Altmetric.com
Key messages
Gastroparesis is a morbid disease associated with diabetes, postsurgical, postinfectious or idiopathic in aetiology.
Nausea, vomiting, bloating, postprandial fullness and early satiety are cardinal features of gastroparesis. Upper abdominal pain is highly prevalent.
Diabetic gastroparesis and idiopathic gastroparesis have varied clinical features. Idiopathic gastroparesis likely constitutes as the larger subset of patients with gastroparesis.
Two-thirds of patients do not improve over 1 year of follow-up.
Small bowel motor abnormalities may also be found in patients with gastroparesis.
Assessment of regional abnormalities in gastric function will likely provide a better correlation with symptoms and targeting therapy.
Loss or injury to interstitial cells of Cajal (ICC) plays a central role in animal models of delayed gastric emptying (GE) and in humans with gastroparesis.
Macrophage-based immune dysregulation mediates development of delayed GE by injuring ICC and other components of the enteric nervous system.
Pharmacological (neurokinin 1 (NK1) antagonistic antiemetics, serotonergic prokinetics and fundic relaxants) and surgical/endoscopic (pyloromyotomy) treatments expand our treatment options.
Understanding the clinical presentation, natural history, pathophysiology and new treatment options for gastroparesis will allow advancements in diagnosis, prevention and treatment of this disorder.
Introduction
Gastroparesis is defined by a delay in gastric emptying (GE) in the absence of mechanical obstruction of the gastric outlet.1 Cardinal symptoms include postprandial fullness/early satiety, nausea/vomiting and bloating. Abdominal pain is increasingly recognised to be one of the most common symptoms in this disease.2 Over the last decade, there has been a paradigm shift in our understanding of the clinical presentation, physiological and molecular alterations in gastroparesis.
Clinically, traditionally, diabetes has been seen as the prototypical cause of gastroparesis. However, diabetic gastroparesis (DG) constituted only about a third of patients with gastroparesis in one tertiary-care study3 and population-based studies show that only 1%–5% of patients with diabetes develop gastroparesis.4 5 In contrast, idiopathic gastroparesis (IG) constituted the most common aetiology accounting for over 50% of the patients with gastroparesis enrolled in the National Institutes of Health (NIH Gastroparesis Clinical Research Consortium (GpCRC).6 A more recent US population-based cross-sectional study showed that IG constituted 28% of the overall patients with gastroparesis identified, while the remaining associated with diabetes. However, diagnostic code-based determination may have resulted in greater association of gastroparesis with diabetes in this study.5 Another unexpected clinical observation has been the association of an overweight/obese status with gastroparesis7 which contrasts with the older observations of weight loss and malnutrition. This finding raises a potential link with the proinflammatory state and oxidative stress associated with obesity. Although not included in the three cardinal symptoms in the Gastroparesis Cardinal Symptom Index (GCSI), abdominal pain is observed in >80% patients with gastroparesis, particularly in those with associated bowel disturbances.2 More recently, opioid use was found to be common in patients with gastroparesis, which can further exacerbate the symptoms and complicate the clinical presentation.8
From a physiological standpoint, a singular end point on the GE scintigraphy to define gastroparesis has allowed diffusion of the technique but has also been criticised because of a lack of correlation with symptoms in many but not all studies.9 10 However, measurement of GE is important as patients with slow and rapid GE can have indistinguishable symptoms11 yet require different treatment approaches. Additionally, GE provides a tangible end point in animal studies and in human clinical trials. The lack of a strong correlation may reflect dissociation between physiology and symptoms once the disease has established, or the fact that the gut can only express a disease process with a limited set of symptoms which can be overlapping. It may also reflect a continuum between symptoms associated with mild/moderate GE delay to severe and ingrained symptoms with overlap from spinal and supra spinal mechanisms. A balanced appreciation of both physiology and clinical symptoms is necessary along with mechanistic studies to understand and clinical trials to address symptoms. Furthermore, refinement and development of new techniques for studying the different aspects of gastric function is likely to provide better understanding of the clinical symptoms and develop targeted therapies.12
The molecular understanding of gastroparesis has significantly evolved over the last decade. We have gone from a disorder of unknown aetiology to enteric neuropathy to myopathy to an established role for the loss or dysfunction of the interstitial cells of Cajal (ICC).13 The emerging animal model and human work suggest a role of an innate immune dysregulation in gastroparesis and putative immune interactions that may be driving the injury to the enteric nervous system (ENS) and ICC.14 15 This has energised a new paradigm for targeting cellular and molecular dysfunction seen in gastroparesis. In this review, we will summarise recent literature on clinical presentation, epidemiology, natural history, pathophysiology, diagnosis and treatment considerations for gastroparesis. Additionally, we will provide future directions for research and discuss the evolving landscape of therapeutic strategies for gastroparesis.
Clinical presentation, epidemiology and natural history
The term gastroparesis encompasses any clinical condition characterised by symptoms suggestive of a deranged digestive function of the proximal GI tract that is associated with objective evidence of an abnormally prolonged retention of gastric contents in the absence of demonstrable mechanical obstruction. No stringent consensus exists on the symptoms that should be included in the definition of gastroparesis.10 Postprandial fullness, early satiety, nausea, vomiting and bloating are the cardinal symptoms originally proposed.1 Symptom profiling from patients enrolled in GpCRC showed that severe early satiety and postprandial fullness was reported by 50%–60% of patients with gastroparesis and DG and IG had similar severity scores.16 Nausea was reported by 95% of the patients (predominant symptom in 29%). It was related to the meals in three quarters of the patients and lasted most of the day in over 40% of the patients. Patients with DG scored higher on the nausea/vomiting subscore of Patients Assessment of Upper GI Disorders-Symptoms (PAGI-SYM), with vomiting lasting several hours or most of the day in over 50% of patients with DG compared with 24% in IG. Patients with DG also reported vomiting in the morning before eating.17 Severe bloating (GCSI ≥4 of 5) was reported by ~40% of gastroparetics and was associated with female gender, overweight status, altered bowel function and probiotic use.18 Bloating was not associated with disease aetiology, smoking status or GE. In a large observational registry study, symptoms that prompted evaluation more often included vomiting for DG and abdominal pain for IG. DG had more severe retching and vomiting than those with IG, whereas, IG had more severe early satiety and postprandial fullness. Additionally, gastric retention was greater in patients with type 1 DG compared with IG.6 Upper abdominal pain of moderate–severe intensity was reported by two-thirds of patients with gastroparesis. It was more prevalent in patients with non-acute onset of gastroparesis, those with bowel disturbances, and opiate and antiemetic use. However, it was not associated with degree of GE delay or with presence of diabetic neuropathy in DG. Compared with nausea/vomiting predominant gastroparesis, pain predominant gastroparesis was associated with greater impairment in quality of life (QoL).2 Additionally, higher depression and anxiety scores were associated with gastroparesis severity on both investigator-reported and patient-reported assessments. Notably, psychological dysfunction did not vary by the aetiology or degree of GE delay.19 Another important aspect of gastroparesis that clinicians need to take into consideration is the presence of overlapping symptoms suggestive of involvement of other regions of the GI tract including the small bowel and the colon.
Only limited information exists on the epidemiology and natural history of gastroparesis. In a population-based study in Minnesota20 epidemiological data were calculated by identifying: (A) ‘true gastroparesis’ defined as typical symptoms and scintigraphically proved delayed GE. (B) ‘probable gastroparesis’ defined as typical symptoms and food retention in the stomach at endoscopy. (C) ‘possible gastroparesis’ defined as either asymptomatic delayed GE or typical symptoms alone. Although as yet the best available study on gastroparesis, it was based on data collected by a symptom questionnaire that did not include postprandial fullness, one of the most frequent symptoms of gastroparesis among patients seen both in Europe21 and in USA.22 The age-adjusted incidence of gastroparesis in the period 1996–2006 was 6.3 per 100 000 person-years, ranging between 2.4 for men and 9.8 for women, with these figures increasing with advancing age with a peak incidence of 10.5 per 100 000 in patients 60 years of age or older. The age-adjusted prevalence of definite gastroparesis per 100 000 persons in 2007 was 24.2, ranging between 37.8 for women and 9.6 for men, with a female-to-male ratio of 3.9:1. The vast majority of subjects with typical symptoms would never undergo GE tests, so it was estimated that the actual prevalence of gastroparesis in the general population could approach 2%, but only 1 out of 10 of these individuals is likely to be diagnosed.23 A different approach to estimating the prevalence of gastroparesis is by calculating the prevalence of dyspepsia in the general population and the relative proportion of postprandial distress syndrome and mixed dyspepsia; that is around 5%–7% of the general population.24 Since GE is delayed in approximately 25%–35% of these patients, one could predict a prevalence of gastroparesis ranging between 1.3% and 1.4% of the general population.
In a recent study looking at sex and ethnic distribution in a cohort of patients with gastroparesis, a higher proportion of blacks presented with diabetes as the aetiology, had more severe retching, vomiting, and hospitalisation rates in the past year compared with whites. Hispanics had less severe nausea, less early satiety, and a lower proportion was using prokinetics than non-Hispanics.25 Another study also showed that non-white patients had worse symptoms, poorer QoL and healthcare utilisation as compared with whites.26 In a study from the Type I Diabetes Exchange Clinic Registry, women are more likely to have gastroparesis than men27 but this was not found to be the case in the Olmsted County Study.4 A greater proportion of women with gastroparesis was noted in the recent populated-based study5 and also in a tertiary-care experience of patients with upper GI disorders.28 In the GpCRC registry, women were more likely to have IG, more severe symptoms of postprandial fullness, early satiety, bloating and upper abdominal pain.25 They were also less likely to improve over 48 weeks of follow-up29 as compared with men.
A prospective follow-up of a large cohort of patients showed that two-thirds of patients with gastroparesis did not improve over 1 year. Predictors of improvement (decrease in GCSI ≥1) over 48 weeks included age ≥50 years, moderate/severe gastroparesis (>20% gastric retention at 4 hours) and onset of gastroparesis following an infectious prodrome. Overweight/obese status, presence of severe abdominal pain, concomitant GORD and depression were associated with lower odds of improvement on GCSI over-time.29 Over the 48 weeks of follow-up, prokinetic, proton pump inhibitor, anxiolytic use and gastric stimulator implantation rates increased in patients with type 1 diabetes, whereas, opiate use increased in patients with type 2 diabetes.30 Additionally, patients with type 1 diabetes had higher haemoglobin A1c, longer symptom duration, longer diabetes duration, greater gastric retention and more hospitalisations. Patients with type 2 diabetes were older, heavier, had more comorbidities, more bloating and fullness. Opioid use in gastroparesis, especially potent opioids (morphine, hydrocodone, oxycodone, methadone, hydromorphone, etc) is associated with worse symptoms, greater gastric retention, and poorer QoL and healthcare utilisation.8 Opioid users also had lower employment rates than non-users.31
As to the impact of gastroparesis on the general health status, the few data that are available suggest gastroparesis is a serious clinical condition. Patients with definite, probable and possible gastroparesis in Olmsted County were followed up for a median of 5 years and, compared with the general population, had increased rates of hospitalisations as well as a decreased life expectancy.20 On the contrary, delayed GE was not found to be associated with increased mortality rates in patients with diabetes followed up for 25 years.32 Hospitalisation rates may increase in the future, since they are related to poor glycaemic control and infection rates in both type 1 and type 2 diabetes, two conditions that are rapidly increasing in industrialised countries.33 This may be balanced by and the trend even reversed by improved therapeutic approaches that have become available to larger proportions of affected individuals. Cardinal gastroparesis symptoms are reported by about 10% of patients with type 1 diabetes,34 but the majority never undergoes a GE test. When GE was evaluated, it was found to be delayed in over 40% of patients with insulin-dependent diabetes,35 but generally normal in uncomplicated type 2 diabetes.36 In fact, DG seems to be associated with both poor glycaemic control and vascular and neurogenic complications that are more likely to occur in type 1 diabetes.34 Box 1 summarises clinical features of gastroparesis using the GpCRC studies.
Clinical features of diabetic gastroparesis (DG) and idiopathic gastroparesis (IG) from gastroparesis registries in the Gastroparesis Clinical Research Consortium
50%–60% of patients with DG and IG report early satiety and postprandial fullness.
Patients with DG have greater nausea and longer periods of vomiting than IG.
Bloating in both DG and IG is higher in women, overweight, those with altered bowel function and those using probiotics.
Vomiting is often the presenting symptom in DG. Abdominal pain is often the presenting symptom in IG.
Abdominal pain associates with non-acute onset of gastroparesis, bowel disturbances, and opiate and antiemetic use. Pain-predominant patients have greater impairment in quality of life than nausea/vomiting-predominant patients.
Physiology and pathophysiology of GE
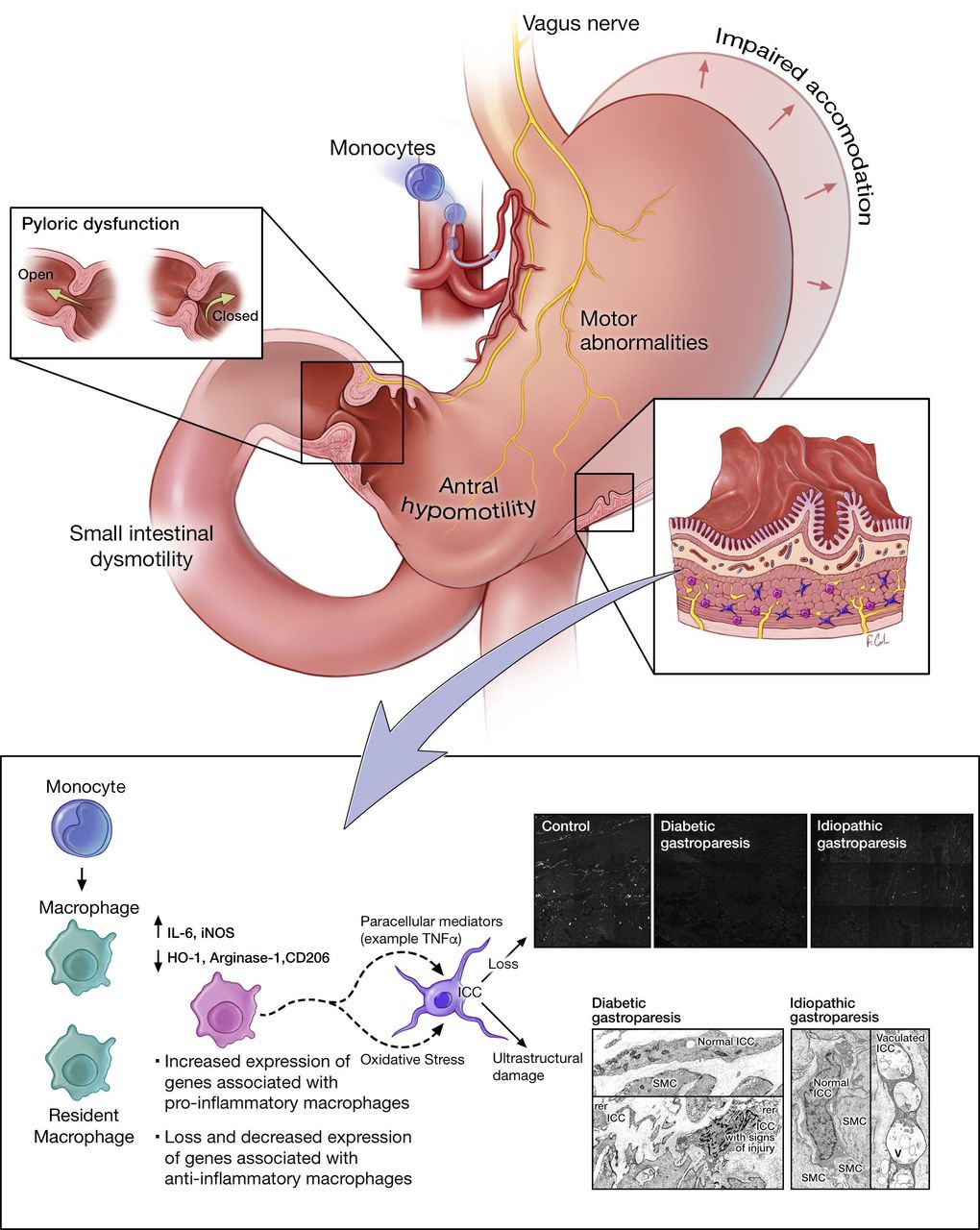
Emptying of a meal from the stomach into the small bowel is the final result of a number of complex and highly coordinated motor and secretory events.37–39 Ingestion of a meal in humans of at least 250 Kcal converts fasting into fed motor and secretory activities. From a neuromuscular standpoint three separate areas are involved in GE: fundus, antrum and pylorus. Swallowing triggers active relaxation of the gastric fundus so that it can accept large volumes of ingesta without detectable increases of intragastric pressure. Subsequently, a steady increase in fundic tone pushes gastric contents that are captured by phasic contractions and pushed towards a rapidly closing pylorus so that digestible solids are ground together with gastric secretions and bounced backwards into the proximal part of the stomach. The maximal frequency of antral contractions is set by the ICC located at the upper part of the greater curvature generating a slow-wave basal electrical rhythm (pace-setter potential) with a frequency of three depolarisations per minute. This process continues until all digestible solids are reduced to particles of 2 mm or less and leave the stomach in small volumes of liquid and homogenised food (chyme) just before pyloric contractions. GE also requires normal small bowel function because antro-pyloro coordination is necessary to empty the stomach, and because neuroendocrine inhibitory signals arise from both the proximal and distal small bowel, based on the composition of the chyme, to modulate emptying rates, so that delivery to the absorbent mucosa matches liver and pancreas secretory activities.39–41 Recent data indicate that enteric dysmotility is more frequent than delayed GE in patients with symptoms suggestive of gastroparesis, and correlates with the severity of clinical manifestations42 suggesting the small bowel should be kept in mind when a patient presents with symptoms suggestive of gastroparesis. Once the caloric content of the meal has been completely emptied from the stomach, secretomotor activities switch back to the fasting state and the three phases of the interdigestive migrating motor complex (IDMMC) return.43 Gastric, biliary and pancreatic secretions also fluctuate during fasting with their peaks coincident with the late phase II preceding phase III which aborally sweeps GI contents including the indigestible solid components of the meal (vegetable fibres) that had been left in the stomach. Unlike what happens in the postprandial state, the pylorus does not close on an oncoming phase III antral contraction. Since the frequency of IDMMCs varies extensively even in healthy individuals and not all phase IIIs start from the stomach,44 emptying of indigestible solids is highly unpredictable, particularly in the disease state, since antral contractility has been found to be decreased in gastroparesis.45 Figure 1 provides an overview of physiological and molecular abnormalities in gastroparesis. Another entity to consider is rapid GE which can be due to increased amplitude of gastric contractions,46 and symptoms of which can be identical to those with gastroparesis, especially in the setting of diabetes.11 A study showed that patients with delayed GE had less frequent bloating than those with normal and accelerated GE.47

GI pathophysiological changes in human gastroparesis. Physiological changes such as impaired accommodation of the gastric fundus/body, motor abnormalities including antral hypomotility, impaired pyloric relaxation and small intestinal dysmotility can result in impaired gastric emptying and clinical manifestations of gastroparesis. At a cellular level, loss of interstitial cells of Cajal (ICC) has been reported in over half of the patients with gastroparesis and nearly all of the patients had signs of injury to ICC on ultrastructural studies. The loss of ICC correlated with delayed gastric emptying in diabetic gastroparesis. Ultrastructural studies also showed changes in nerves and smooth muscle cells which were less appreciable on immunohistochemistry. More recently, human studies have shown loss of macrophages with anti-inflammatory phenotype (CD206-positive, M2 or alternatively activated macrophages) and increased expression of genes associated with proinflammatory macrophages on transcriptomic analysis of full thickness biopsies. This is complemented by animal model studies of diabetic gastroparesis where an altered macrophage activation was shown to mediate injury to ICC likely through paracrine mediators. Additionally, CSF1 op/op mice lacking macrophages were protected from development of gastroparesis in spite of having diabetes suggesting an essential role for immune cells in development of delayed gastric emptying. Immune-mediated mechanisms likely play a critical role in pathogenesis of gastroparesis.
Pathogenesis
Normal gastric function relies on neuromuscular coordination by the extrinsic innervation, inhibitory and excitatory components of the ENS, ICC, fibroblast-like cells and gastric smooth muscle. Regional abnormalities in motility patterns of the gastric fundus, body, antrum, pylorus and proximal small bowel can result in delayed GE as this is measured as a composite end point. Vagal innervation to the stomach is important for accommodation and possibly mediating pyloric relaxation. Early observations in DG showed blunted pancreatic polypeptide response and gastric secretion on sham feeding suggesting vagal dysfunction.48 Histological changes in myelinated and unmyelinated vagal nerve fibres have been reported in patients with DG.49 The sympathetic component of the autonomic nervous system has also been shown to be affected in DG with axon-dendritic histological and prevertebral ganglionic gene expression changes.50 51 Abnormalities in both inhibitory (neuronal nitric oxide synthase, nNOS; vasoactive intestinal peptide, VIP) and excitatory (acetylcholine; substance P) components of the ENS have been described in humans with gastroparesis and in animal models of delayed GE although the findings are not always apparent on histology and may require electron microscopy. Indeed, in humans it appears that enteric neurons are preserved in gastroparesis with potential functional changes only seen on electron microscopy.52 53 Streptozotocin-induced diabetic rats demonstrated an increase in VIP immunoreactivity which was reversible with insulin administration.54 A non-insulin-dependent diabetic rat model showed attenuation of non-adrenergic, non-cholinergic inhibitory neurotransmission and reduced sensitivity of adrenoceptors to norepinephrine in the colon.55 Nitric oxide (NO) is a key physiological mediator of non-adrenergic non-cholinergic relaxation in the GI smooth muscle. Sildenafil, an inhibitor of phosphodiesterase type 5 (PDE 5) was shown to inhibit gastric and intestinal transit in high doses, an effect that was blocked by N(gamma)-nitro-L-arginine methyl ester (L-NAME), a non-selective NOS inhibitor and methylene blue, a guanylate cyclase inhibitor.56 Reduced NOS activity was seen in streptozotocin-induced diabetic rats and diabetic mice. One study has shown that dimerised nNOS expression correlates better with gastric relaxation suggesting that post-translational modifications may be important in mediation of inhibitory neurotransmission.57 Diabetes-related advanced glycation products can bind and inhibit nNOS in myenteric neurons,58 however, other factors like glucose, insulin, insulin-like growth factor,59 lipoproteins and oxidative stress60 61 molecules also play a role in nNOS regulation. In a study on nNOS−/ − mice, a model of delayed GE,62 neural stem cell transplantation into the pylorus increased the smooth muscle relaxation and restored GE.63 Myenteric nitrergic neuropathy has been found in the jejunum of spontaneously diabetic BB rats.64 Differences in nNOS signalling may explain increased predisposition for gastroparesis in women. In the gastric antrum of streptozotocin-induced Sprague-Dawley rats, female rats had greater impairment in nNOS dimerisation, nitrergic relaxation, increase in intragastric pressure and worse GE than male rats.57 Additionally, a diminished intracellular tetrahydrobiopterin:total biopterin ratio was shown to impair nNOS activity in diabetic female rats.65 Tetrahydrobiopterin supplementation has been proposed to be potentially effective in accelerating GE.66 The contribution of loss of nNOS expression towards GE delay in humans is unclear. In humans with DG and IG, only a small subset shows decrease in nNOS expression52 and efforts to increase NO using nitroglycerine and sildenafil did not result in clinical benefits.67 68 Additionally, although nNOS expression was decreased in response to hyperglycaemia in the non-obese diabetic (NOD) mice, it did not predict development of delayed GE.69 This suggests that nNOS may act as a cofactor or a post-translational protein may be involved in mediating its role. Considering the increasing overlap between gastroparesis and obesity, animal models have also examined the effects of a high-fat diet on ENS. Duodenal myenteric density of neurons expressing VIP and nNOS was found to be decreased and ultrastructural studies showed axonal swelling and loss of neurofilaments.70 In an ob/ob mouse model of obesity, lower inhibition of myosin light chain phosphatase genes was seen, but no clear effects on gastric antral smooth muscle contractility were noted.71 Although ob/ob mice are used as a model of delayed GE,72 the precise cellular injury in this model is not well established.
In addition to slow wave generation and setting of the smooth muscle membrane potential, ICC are also involved in cholinergic and nitrergic neurotransmission and mechanotransduction.73 Loss of ICC is one of the the most common cellular abnormalities reported in animal models of delayed GE as well as in humans. Full-thickness gastric body52 and antrum74 biopsies from both DG and IG have demonstrated a loss of ICC, with changes being more prominent in the gastric antrum than the body. Other human studies have also shown a loss of ICC in patients with DG.75 76 On ultrastructural examination, almost all patients with DG and IG had changes in ICC such as intracytoplasmic vacuoles, mitochondria with clear matrix, extended rough endoplasmic reticulum and apoptotic features (figure 1).53 Two major animal models of DG (streptozotocin rats77 and NOD mice69) have shown a decrease in the number of ICC. In streptozotocin-induced diabetic rats, antral ICC were depleted at 12 weeks of diabetes. NOD mice with delayed GE also showed loss of ICC networks in the gastric corpus and antrum as demonstrated by c-Kit (receptor tyrosine kinase) expression. Ano-1, a calcium-activated chloride channel protein is expressed in ICC and is important for the electrical activity of the ICC.78 Patients with DG have altered Ano-1 expression and different proportions of Ano-1 variants as compared with diabetic controls which affect the electrical activity of the ICC.79 Loss of ICC has been associated with gastric dysrhythmias in patients with DG. Animal studies have shown that even patchy loss of ICC can result in re-entrant tachycardias and loss of slow waves resulting in bradycardias. A subset of patients with DG with severe ICC loss was found to have tachygastria patterns on the electrogastrogram.80
The key points in molecular pathogenesis of gastroparesis are summarised in box 2. In DG, ICC loss correlates with the delay in GE.81 The underlying mechanisms for ICC loss were, until recently, unclear. Smooth muscle atrophy/degeneration and fibrosis has been observed in severe diabetes. This can result in depletion of smooth muscle produced stem cell factor which plays a role in ICC survival.82 A recent human transcriptomic study showed changes in various smooth muscle genes in IG.83 Data obtained from the NOD type 1 diabetes model suggest a role of uncountered oxidative stress to play a role in ICC loss and development of delayed GE.69 One mechanism for the control of oxidative stress is expression of haemoxygenase-1 (HO-1). HO-1 is produced by CD206-positive anti-inflammatory macrophages. Mice that develop delayed GE failed to upregulate HO-1 expression while upregulation of HO-1 by haemin increases expression of Kit and nNOS and reverses the delay in GE.84
Key points in molecular pathogenesis of gastroparesis
Loss or injury to ICC, the gastric pacemaker cells, is required for delayed gastric emptying to develop.
Smaller subsets of patients may have loss of enteric nerves and fibrosis in muscle layers.
Traditional neutrophilic immune infiltration is not common in patients with gastroparesis.
Macrophage-driven immune dysregulation and oxidative stress appear to be driving injury to ICC. Interactions between the immune and enteric nervous systems need to be further studied.
In the NOD mice, the development of delayed GE was associated with an increase in inducible nitric oxide synthase (iNOS) expression, a marker for macrophages with an ‘M1’ phenotype (classically activated or proinflammatory).69 Macrophage-deficient colony stimulating factor 1 (CSF1)op/op mice did not develop delayed GE despite the presence of severe hyperglycaemia.85 Administration of CSF1 resulted in replenishment of macrophages and development of delayed GE and ICC damage in >75% of the mice. Conditioned media from macrophages exposed to oxidative stress resulted in damage to cultured ICC which could be prevented by neutralising antibodies against interleukin 6R and tumour necrosis factor (TNF).86 Decreased CD206+ (alternatively activated, anti-inflammatory M2 macrophages) has also been reported in the gastric antrum of patients with DG and IG which correlated with the loss of ICC.74 Additionally, patients with DG had long GT alleles in the HMOX1 gene and these associated with worse nausea symptoms.87 Recent transcriptomic analysis of full thickness (excluding mucosa) gastric body biopsies from DG and IG reveal macrophage-driven immune dysregulation as the primary pathways affected. Additionally, genes associated with M1 (proinflammatory) macrophages were enriched in tissues from IG compared with controls.88 These data taken together suggest a new paradigm for the development of gastroparesis with macrophage-driven immune dysregulation and oxidative stress being central to driving injury to the ICC and subsequent delayed GE. Figure 2 provides a summary of cellular and molecular changes in human gastroparesis.

{kind=link}
{kind=link}
Summary of human studies highlighting cellular and molecular changes in gastroparesis. Ach, acetylcholine; Ano-1, anoctamin-1; DG, diabetic gastroparesis; ENS, enteric nervous system; ICC, interstitial cells of Cajal; IG, idiopathic gastroparesis; nNOS, neuronal nitric oxide synthase; SP, substance P; VIP, vasoactive intestinal peptide.
Diagnostic considerations
Patients with cardinal gastroparesis symptoms and normal upper endoscopy in the absence of alarm features may be candidates for a short-term treatment with prokinetics. Non-responders and early relapsers could also try short-term treatment with antisecretory drugs and antidepressants alone or in various combinations. If consistent response is not achieved or if country or state practice guidelines suggest ruling out mechanical obstruction first before targeting with prokinetics, patients should undergo traditional diagnostic testing to exclude mechanical obstruction or any organic disease. In case of negative findings patients should be referred to centres with specific interest in the field in order to undergo physiological testing of GE.24 Therefore, the diagnosis of gastroparesis is based on both recognition of cardinal symptoms and identification of delayed GE by appropriate instruments.
Symptom evaluation
Cardinal gastroparesis symptoms include postprandial fullness, early satiety, nausea, vomiting and bloating. Validated questionnaires such as the GCSI based on the PAGI-SYM89 and the more recently revised GCSI-Daily Diary score90 have been developed to quantitate the severity of these and other digestive symptoms, but their use is mostly restricted to clinical trials. Self-administered questionnaires with simple descriptive definitions of individual symptoms enriched by explanatory cryptograms have been demonstrated to decrease patient-doctor misunderstanding91 and similar questionnaires validated in different languages might help clinical practice in the near future.
GE measurement
Numerous techniques are available for measuring GE, but scintigraphy is the gold standard. Stable isotope breath testing as well as wireless motility capsule (WMC) provide reasonable alternatives.9 Scintigraphic GE is the current gold standard.92 An anteroposterior γ-camera recording of the gastric area for 4 hours after ingestion of a Tc-99m-labelled low-fat Egg Beaters (chicken egg white) meal is the standardised procedure that was internationally validated to obtain well-established normal values.93 The technique, however, has several limitations: (A) Caloric (255 KCal) and fat contents (2%) are low and do not mimic a normal meal even for symptomatic individuals, so that it probably underestimates the actual prevalence of gastroparesis, although, on the other hand, it has the advantage of reducing false-positive cases. (B) Due to radiation exposure, it should not be used in women of childbearing potential which represent a large group of patients seeking medical help for symptoms suggestive of gastroparesis and, for the same reason, it is not an ideal technique for repeated measurements that would be necessary, to investigate changes in clinical manifestations over time and/or need of monitoring the effects of treatment. (C) Nuclear medicine departments are rare globally and certainly insufficient to evaluate all potential patients with gastroparesis. (D) Even if a nuclear medicine department is available, γ-camera time is expensive and devoting it for diagnosing gastroparesis is not always possible, although this issue has been partly addressed by standardising delayed GE as >10% at 4 hours,93 thus limiting the use of the dedicated equipment to a minimum and/or allowing investigating numerous patients in the same session.
Some, but not all of the above limitations have been overcome by the validation of GE breath tests. Different substrates including octanoic acid, a medium-chain fatty acid,94 and Spirulina platensis, an edible algae,95 can be tagged with a stable (non-radioactive) carbon isotope (13C) and thereafter incorporated into the solid component of low caloric meals. After being emptied from the stomach, the organic substrates are digested and absorbed in the proximal small intestine and metabolised by the liver so that 13C is excreted by the lungs, and its rise over the baseline in breath samples can be measured by mass spectrometry. The rate-limiting step is GE and therefore appearance in the breath correlates with GE. 13C breath-testing GE shows a strong correlation with simultaneously obtained scintigraphy96 and the 13C spirulina technique has been approved by the US Food and Drug Administration (FDA).97 The technique is non-invasive and therefore suitable for repeated testing, simple to perform at the point of care and relatively cheap, since it does not require any special equipment onsite, since breath samples remain stable for long periods of time and can be centralised. Its main limitations are artefacts that can be encountered in patients with intestinal malabsorption and liver or lung diseases. One study has shown that up to 39% of patients with gastroparesis can have a positive lactulose breath test.98 Although, this represents an accelerated orocaecal transit, small intestinal bacterial overgrowth can affect interpretation of breath testing for GE, especially in the setting of diabetes and scleroderma which have been associated with small intestinal bacterial overgrowth. Furthermore, 13C spirulina is not available in Europe and has not been approved by European health authorities.
Similarly to scintigraphy and breath testing, WMC has been approved by FDA for measuring GE.97 WMC, also known as SmartPill, is a non-invasive technique to indirectly measure GE and intestinal transit times, by an ingested capsule recording pH, pressure and temperature signals that are analysed by an external receiver.99 As previously described, a large indigestible solid like the SmartPill, even if ingested with a test meal, does not reflect emptying of its caloric digestible components, since it is emptied separately during the fasting state. A study done to assess performance of WMC compared with 99mTc-based scintigraphy showed a correlation of 0.73 between 4 hours GE on scintigraphy and breath testing-based GE time. A 300 min cut-off for GE time provided a sensitivity of 65% and specificity of 87% for diagnosis of gastroparesis compared with a sensitivity of 44% and specificity of 93% for 4 hours GE scintigraphy.100 WMC provided new diagnosis in >50% of patients with suspected gastroparesis or slow intestinal transit.101 This was again shown in a recent study where WMC detected delayed GE in 10% more individuals than scintigraphy and in almost twice as many patients with diabetes got diagnosed with delayed GE than scintigraphy. As somewhat expected, diagnosis of rapid GE was made less often with WMC.102 It remains unclear if higher sensitivity of detecting delayed GE which is likely driven by the emptying delay due to non-physiological nature of pill emptying is clinically meaningful. A clear advantage of WMC, however, is that it allows assessment of global transit abnormalities which can be helpful in evaluation and management of comorbidities like constipation that associate with gastroparesis.103
Other techniques for measuring GE are MRI and ultrasonography, but they have been generally only used for research purposes. MRI can measure GE, and gastric accommodation to meal ingestion and wall motion. It requires expensive equipment use and investigated patients must remain still in the supine position, thus limiting the clinical applicability of the technique.104 Ultrasound equipment is readily available and the technique can be used to measure GE of liquids105 106 in non-obese individuals, but its use has also been restricted to research settings. Both GE and transpyloric liquid flow can be measured by transabdominal duplex ultrasonography, while three-dimensional ultrasonography can also measure intragastric volumes.107 Identification of intragastric bezoars or food residues at endoscopy or radiology, after an overnight fast also represents indirect confirmation of abnormal gastric motility.
Treatment—medical therapy
It remains reasonable to recommend to patients with gastroparesis to avoid large, high-caloric, fatty meals, as well as dietary fibres and any food that is recognised by the individual patient to aggravate postprandial symptoms. Although these suggestions are based on pathophysiological considerations or good common sense they have never been validated in appropriate studies. A randomised, controlled study in patients with DG reported improvement of reflux symptoms, fullness, nausea, vomiting and bloating on a diet consisting of small particle sized solids.108 In one study, only a third of patients with gastroparesis had nutritional counselling and only 2% were following any dietary suggestions. Despite the increasing percentage of patients with gastroparesis who are obese, over 60% of patients reported caloric-deficient diets (defined as <60% of estimated daily total energy requirement) and had deficiencies in several vitamins and minerals.109 Thus, a dedicated history for caloric intake and nutritional counselling is important for these patients.
The ideal therapy for gastroparesis should reverse the cellular defects, accelerate GE and improve cardinal symptoms. However, as previously discussed, the delay in GE is only partially related to the clinical manifestations of gastroparesis and other mechanisms are likely involved after the initial onset of the disease, including decreased gastric accommodation, small bowel motor abnormalities, visceral hypersensitivity, and so on.10 Thus, current treatments are evaluated primarily based on their efficacy on symptoms.92 Since different pathogenic mechanisms may be concomitantly present in the same subject, combination therapies would be theoretically appropriate, but they have never been tested. Co-prescription of prokinetics, antiemetics and neuromodulators may be necessary to control symptoms in severe cases, but it may lead to drug-drug interactions, due to concomitant metabolism by liver cytochrome P-450 enzymes,110 thus increasing potential hazards typical of these pharmacological classes (see below).
Prokinetics
A recent meta-analysis confirmed efficacy of prokinetics on clinical symptoms suggestive of gastroparesis, but most studies are old and their quality does not match the current requirements of American and European health authorities.111 They are classified into different pharmacological classes, including dopamine (D2) receptor antagonists, serotonin (5-HT4) receptor agonists, cholinesterase inhibitors, motilin-like agents, ghrelin-like agents, although many drugs have multiple mechanisms of action.
Metoclopramide is a D2-receptor antagonist with some 5-HT4 receptor agonism that exerts both prokinetic and antiemetic effects. It is the only medication available for the treatment of gastroparesis in USA, but, despite the chronicity of the condition, its use is restricted by the FDA to 12 weeks. It is available worldwide, unlike other compounds such as clebopride and cinitapride with similar modes of action and clinical effects that can be prescribed only in selected countries. Since they can cross the blood-brain barrier, they can exert central effects such as anxiety, depression, tremors and other more severe extrapyramidal side effects including, in rare cases, tardive dyskinesia. For this reason, metoclopramide received a black box warning from FDA.112
Domperidone does not cross the blood-brain barrier enough to cause similar neurological side effects, but it still can exert the antiemetic effects typical of benzamide derivatives, since the vomiting centre is located in the floor of the fourth ventricle in the brainstem, outside the blood-brain barrier. Its use is under regulatory scrutiny in some of the countries where it is commercially available, since it bears a potential risk of cardiac arrhythmias and even sudden death, due to inhibition of human ether-à-go-go-related gene (hERG) channel activity and relative prolongation of the QTc interval, typical of other pharmacological agents with 5-HT4 receptor agonistic activity.113 However, in other countries this can be obtained over the counter.
Prucalopride is a 5-HT4 receptor agonist devoid of adverse cardiac effects that exerts an enterokinetic effect and is approved for the treatment of chronic constipation in several countries including USA. It has been recently shown to exert a gastrokinetic effect also and to improve symptoms in a relatively small number of patients with IG.114 Velusetrag is another selective 5-HT4 receptor agonist with GI prokinetic effects that was shown to induce both symptom relief and GE acceleration in a dose-finding, placebo-controlled study in patients with DG or IG.115
Cholinesterase inhibitors exert a prokinetic activity throughout the alimentary canal and are effective in treating diffuse intestinal motor disorders including postoperative ileus, constipation and chronic intestinal pseudo-obstruction.116 Acotiamide is a recently developed cholinesterase inhibitor that also exerts a presynaptic muscarinic autoreceptor inhibitory activity. It was shown to enhance both contractile and accommodation activities of the stomach and, interestingly, to improve dyspeptic symptoms suggestive of gastroparesis, but not epigastric pain and burning symptoms.117 118
Motilin and ghrelin are hormones secreted by the proximal portions of the alimentary canal that accelerate GE. Pharmacological analogues of these hormones are being investigated for the treatment of gastroparesis. Macrolide antibiotics are agonists at motilin receptors that induce a marked acceleration of GE. Both erythromycin and azithromycin are used in clinical practice, based on the results of small studies,111 but their use is limited by side effects including abdominal cramps, nausea, diarrhoea, QT prolongation, as well as by tachyphylaxis.119 Furthermore, when a large study was conducted with a motilin-like agent devoid of antibiotic effect, no clinical benefit was obtained in patients with functional dyspepsia with or without gastroparesis.120 This negative result may be explained by the non-physiological effects of motilin analogues in the postprandial state, since motilin is a typical interdigestive hormone that activates phase III-like activity with a gastric component, thus emptying large undigested particles, unprepared to undergo digestion in the proximal small bowel. Since some patients with gastroparesis also present with impaired gastric accommodation, erythromycin should not be prescribed, as it increases fundic tone.121 The increase in fundic tone may have also contributed to the negative study result of the motilin-like agent. Relamorelin is a synthetic pentapeptide ghrelin receptor agonist that stimulates gastric contractions and has been shown to accelerate GE of solids and improve nausea, fullness, bloating and pain in patients with gastroparesis and type 2 diabetes.122 Two additional trials showed acceleration of GE, but mixed results on improvement in clinical symptoms.123 124
Antiemetics
As previously mentioned benzamide derivatives are prokinetics that exert an antiemetic effect by inhibiting D2 receptors in the brainstem. 5HT‐3 receptor antagonists such as granisetron and ondansetron are effective in controlling chemotherapy‐induced nausea and vomiting125 and can be prescribed in patients with dysmotility whose clinical picture is dominated by nausea and vomiting but where prokinetics increase the cardiac risks. 5HT‐3 receptor antagonists may also be administered via a patch reducing the variability in drug absorption in patients with frequent vomiting. Also, neurokinin antagonists are approved for the treatment of chemotherapy-induced emesis.126 Among these drugs, aprepitant, increases gastric accommodation127 and improves some digestive symptoms in patients with gastroparesis,128 but does not affect GE.127 Although the APRON Trial failed to show positive results on the primary end point of nausea, several other secondary end points showed improvement with aprepitant.128 More recently, tradipitant has been shown to meet the primary end point of improvement in nausea scores as well as nausea-free days and other secondary end points on GCSI and PAGI-SYM in a female-predominant population of patients with gastroparesis (60% IG, 40% DG) with moderate-to-severe nausea.129
Neuromodulators
Levosulpiride is an antipsychotic agent which accelerates GE by exerting both antidopaminergic and 5-HT4 agonistic activities.130 It has been shown to improve symptoms in patients with both DG131 and IG,132 but this did not correlate with the acceleration of GE. The anxiolytic 5-HT1A agonist buspirone enhances gastric accommodation and improves postprandial symptoms independently from its anxiolytic effect.133 Contradictory results are reported for antidepressants. In a large, well-designed study, patients with functional dyspepsia were randomised to amitriptyline or escitalopram. The former improved symptoms exclusively in patients with normal GE and predominant epigastric pain or burning, while the latter did not show any clinical effect.134 Nortriptyline also failed to prove superiority compared with placebo in another randomised controlled trial of patients with gastroparesis.135 On the contrary, mirtazapine, an antidepressant with central adrenergic and serotonergic activity, improved nausea, vomiting and loss of appetite in an open-label study of patients with gastroparesis.136 If these results are confirmed, mirtazapine would find an indication in patients with weight and appetite loss. In severely ill patients with gastroparesis seen in the emergency department, intravenous haloperidol decreased abdominal pain and nausea.137
Treatment—endoscopic and surgical
Gastric electrical stimulation
The precise mechanisms of action of gastric electrical stimulation (GES) are not known. Current stimulation settings do not alter GE. One study showed that loss of gastric ICC predicted poor response to GES.138 Another study showed better efficacy in patients with DG, men and those with shorter duration of gastroparesis.139 The GES assembly consists of two leads that are placed in the muscularis propria of greater curvature of the stomach about 10 cm proximal to the pylorus and a subcutaneously placed pulse generator. A temporary GES may be tried to determine response before a permanent device is placed. In the first double-blind randomised control trial (RCT) of 33 patients (17 DG, 16 IG), vomiting frequency decreased during the ON period. However, patients could not separate the ON and OFF periods over the course of the study.140 In a retrospective study of 48 patients, using high-frequency GES and longer follow-up, upper GI symptoms, glycaemic control and QoL improved with the use of GES.141 In another trial of patients with diabetes with gastroparesis, 6 weeks of GES reduced vomiting and other symptoms as well as improved QoL.142 A trial by the same group in patients with IG showed improvement in vomiting during the ON period. However, no significant reduction during the ON versus OFF periods was noted which was the primary end point.143 Another study also documented improvement in abdominal pain as well as decreased use of prokinetics and antiemetic following GES.144 Patients with malignancy- or drug-associated gastroparesis or severe comorbidities may benefit from temporary GES. However, only three of all the published studies were controlled and of these, only one (see above) showed partially positive results.145 Thus, the evidence from controlled trials is not supportive of the use in the broader population of patients with gastroparesis.
Botulinum toxin injections
Mearin et al made initial observations of pyloric dysfunction in a subset of patients with DG.146 Injection of botulinum toxin was first used for achalasia and subsequently extended to gastroparesis in open-labelled studies. In spite of a widespread clinical use for this strategy, only two small randomised controlled trials have assessed efficacy.147 148 Although underpowered, both of these showed no difference in improvement of symptoms between the placebo and active treatment arms. However, a larger open-labelled study of ~180 patients has suggested greater clinical response to 200 U as compared with 100 U and in female patients, patients with IG and those younger than 50 years of age.149 A more recent study in patients who have three cycles per minute rhythm on electrogastrogram (EGG) (thus suggestive of normal gastric body function), both Botox injections or pyloric balloon dilations resulted in 78% symptom improvement at 4 weeks.150 The conclusion in general is that there is no clinical evidence to support widespread use of Botox injections. However, resurgence of interest in assessment of pyloric function and therapies may better educate us on whether a specific subset of patients with gastroparesis may respond to Botox injections.
Pyloromyotomy
Although poor, the data from Botox studies together with the prior manometry studies and advances in endoscopic techniques have led to a resurgence of pyloromyotomy as a treatment for gastroparesis. One study showed that ~70% of patients with gastroparesis have loss of pyloric ICC and fibrosis.151 Another case series of four patients with type 1 DG showed atrophy of smooth muscle fibres and collagenous thickening between bundles of muscle fibres. These changes were more prominent in the pylorus than in the gastric body from the same subjects. Additionally, there was presence of eosinophilic inclusion bodies in the muscularis propria.152 The exact role of ICC in pylorus is not defined. Loss of inhibitory nitrergic neurotransmission may result in impaired pyloric relaxation.153 Most studies with gastric peroral endoscopic pyloromyotomy (G-POEM) have presented 3–6 months follow-up data with some studies documenting 12–18 months follow-up.154 The clinical response rate has been reported to be between 70% and 80% with GE improvement ranging from 4% to 64%. Almost all studies showed improvement in nausea and vomiting. Improvement in abdominal pain has been reported in three studies, however, effects disappeared by 6 months. Gastric ulcer and related bleeding were the most commonly reported complications followed by tension capnoperitoneum. Most of the reported studies originate from tertiary-care centres with endoscopic expertise and demonstrate 100% technical success. A recent study showed decline in ER visits and hospitalisation following G-POEM.155 The available data allow assessment of short-term efficacy. The long-term effects include possibility of pyloric scarring. Controlled studies are needed both to assess outcomes as well as help predict potential response to pyloromyotomy. Attempts to identify pylorospasm have been made using impedance planimetry (endoscopic functional luminal imaging probe, EndoFlip). In one study, early satiety and postprandial fullness correlated inversely with pyloric diameter and cross-sectional area.156 Another approach used is response to intrapyloric Botox injection to triage patients for pyloromyotomy.157 Some groups have proposed use of GES along with pyloroplasty in those with refractory symptoms of DG.158 There is also no standardised technique currently for performing the G-POEM. Hook knife is favoured by several endoscopists. Additionally, most studies have favoured posterior gastric antral wall or greater curvature instead of anterior wall for submucosal tunnelling.159 Correct identification of pyloric muscle ring and hence the extent of submucosal tunnelling required is often technically challenging. Finally, there is a variability in the approach with some performing circular muscle whereas others full-thickness myotomy. Generally, a 2.5–3 cm long muscle incision is considered optimal. Further controlled clinical trials with patient selection using high-resolution antroduodenal manometry or EndoFlip assessment of pyloric function in combination with long-term follow-up are awaited. Box 3 highlights the key points in treatment advancements for gastroparesis.
Key points in treatment advances for gastroparesis
Tricyclic antidepressants like nortriptyline and amitriptyline are ineffective for gastroparesis.
Antiemetic NK1 receptor antagonists like aprepitant and a newer agent tradipitant appear to be effective for at least some of the cardinal symptoms of gastroparesis.
Prokinetic serotonergic agents like prucalopride might be effective for gastroparesis.
Fundic relaxants like buspirone and acotiamide are under further investigation for patients with gastroparesis.
No current controlled evidence for immune-based therapies in gastroparesis exists and is needed.
Pyloric therapies may be effective for a subset of patients. However, more work needs to be done to select the patient subgroup with pyloric dysfunction and determine long-term efficacy in controlled studies.
Conclusions and future directions
The last decade has been a turning point in our clinical and molecular understanding of gastroparesis. We now have a good understanding of the cellular events that occur in the stomach of patients with gastroparesis and the central role of macrophages in the disease. The clinical features of once a poorly defined and elusive disease are now much better understood. Variations in clinical presentation by aetiology as well as evolution of symptoms and GE over time have been described. From a diagnostic standpoint, 13C breath test and WMC have been developed as non-invasive strategies for assessment of GE. Controlled clinical trials have helped evolve the treatment landscape of gastroparesis as well. For example, in a clinical trial of gastroparesis and another trial of patients with functional dyspepsia some of whom had delayed GE, tricyclic antidepressants were not useful. Positive results on several parameters obtained with aprepitant and relamorelin have helped identify newer classes of antiemetics with potential for treatment of gastroparesis. Gastroenterokinetics have also been shown to exert positive effects in these patients. There is also an emerging interest in assessing and targeting regional motility disturbances of the stomach. For example, pharmacological fundic relaxants like acotiamide and buspirone and surgical or endoscopic pyloric relaxation using pyloromyotomy are now being investigated in gastroparesis.
However, the challenges still exist in expanding the molecular understanding and establishing approved treatment options. From a diagnostic standpoint and for targeting, future investigations will have to provide regional assessments of GI functions and allow investigation of the pyloric anatomy and function. The mechanisms behind fundic and pyloric dysfunction in gastroparesis and their contribution towards GE and clinical symptoms associated with this disorder are still to be determined. Additionally, the role of duodenal and distal gut mechanisms in gastroparesis warrants further investigation. It is possible that a combination of symptoms, and molecular and physiological testing may help us identify subsets of patients with gastroparesis which can be then targeted using specific treatments. Additional work also needs to be done to understand the spinal and supraspinal mechanisms in the severe and refractory end of the disease spectrum. Pain in gastroparesis is still poorly understood and one of the hardest symptoms to treat often driving these patients towards opioids. Appropriate paradigms need to be developed for managing diabetes in patients with DG and for maintaining hydration and nutritional requirements. Lastly, identification of genetic, microbial and environmental triggers will help advance understanding of onset of gastroparesis and other associated upper GI disorders. In summary, the progress made over the last decade has resulted in a better understanding of gastroparesis and a promising outlook for management of this morbid disease. Future strategies will hopefully continue to build on this progress and help us reach a stage where gastroparesis can be prevented, assessed and treated with greater precision and success.
Acknowledgments
The authors thank Mr Frank Corl for help with the illustration and Ms Kristy Zodrow and Ms Lori Anderson for administrative assistance.
References
Footnotes
Contributors All authors contributed equally to this manuscript.
Funding MG and GF are supported by NIH DK068055 and DK74008. MG is also supported by NIH K23 DK 103911 and R03 DK 120745. GF is also supported by NIH DK057061.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.