Article Text

Abstract
Research into Crohn’s disease has recently been focused on the genetics of the patient, the gastrointestinal flora, the gut epithelium and mucosal immune responses. For over 60 years pathologists have reported that the fundamental alteration in Crohn’s disease occurs in regional lymphatics of the intestine—the disease is a lymphocytic and granulomatous lymphangitis. At an earlier time, experimental sclerosis of regional intestinal lymphatics of the pig produced a chronic segmental enteritis with many features of Crohn’s disease, including lymphocytic and granulomatous lymphangitis of the bowel wall and enteroenteric and enterocutaneous fistulas. In Crohn’s disease, differences in the anatomic distribution of vasa recta appear to explain long-segment disease of the ileum and short-segment disease of the more proximal intestine. A variety of bacteria and viruses cause lymphangitis, suggesting that microorganisms may be at the centre of the basic changes in Crohn’s disease. Dietary antigens and lipids are worthy of consideration as well. Now that antibodies to label lymphatics are available, attention should be directed at defining the initial damage to lymphatic endothelium and agents that might be responsible.
Statistics from Altmetric.com
Currently there is widespread opinion within the gastrointestinal research community that Crohn’s disease is caused by genetic susceptibility, abnormal intestinal permeability, interactions between the bacterial flora and surface epithelial cells, and dysregulation of the host’s immune response.1–5 Genetic studies have driven the notion that hereditary factors render the mucosal surface susceptible, and rodent model studies have shown that ileitis and colitis do not occur in the absence of bacterial flora. Presently, technology is driving the hypothesis rather than the reverse. Attention has been directed at understanding the composition of the intestinal flora,6 the layering of the intestinal flora,7 its interaction with the mucous coating and bacterial receptors in the mucosa. One might surmise that the patient has had the misfortune of acquiring both genetic susceptibility and an intestinal flora that takes advantage of such susceptibility.
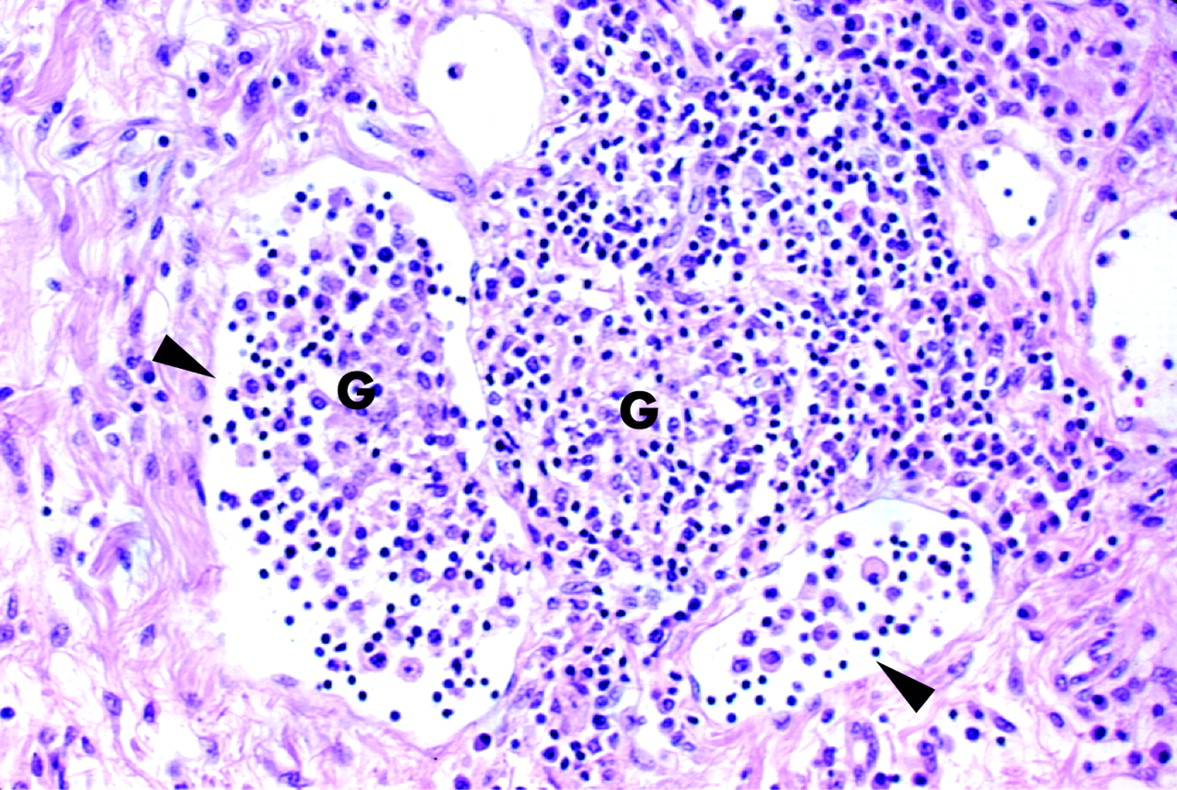
We write today to remind the scientific community of the works of eminent pathologists of an earlier time in the twentieth century. These include Blackburn, Hadfield and Hunt;8 Warren and Sommers;9 Van Patter;10 Meadows and Batsakis;11 Lockhart-Mummery and Morson;12 Mottet13 and Morson.14 These individuals had the opportunity to study numerous tissue specimens from patients with Crohn’s disease before the time when the lesions were distorted, reduced and in fact artifactually damaged by such treatments as the prolonged use of antibiotics, corticosteroids, immunomodulators and, more recently, biologics. These early investigators repeatedly pointed out that the gross segmental distribution of the lesions had to be accounted for; and that the microscopic appearance and distribution of the lesions—that is, beneath the lymphoid follicles of Peyer’s patches, in the basal portion of the lamina propria, in the superficial and deep submucosa, between the planes of smooth muscle of the muscularis and in the subserosa—suggested lymphatic disease (Table 1). These lesions are comprised of lymphocytic thrombi within lymphatics and multiple large aggregates of lymphocytes, often containing granulomas, with or without multi-nucleated giant cells; in other words, a lymphocytic and granulomatous response consistent with chronic lymphangitis (figs 1 and 2).

Attention has been directed at understanding the composition of the intestinal flora,6 the layering of the intestinal flora,7 its interaction with the mucous coating and bacterial receptors in the mucosa.
Wakefield et al, in 1989 and 1991, recognised that there was a pattern to the distribution; however, at the time they thought it represented granulomatous vasculitis.15 16 We could not confirm their results17 and nor could others.18 19 The granulomas of Crohn’s disease appear to be in and around the very thin walled lymphatics that are often found adjacent to small arterioles and venules.19 Also forgotten are the works of research investigators who, having regarded earlier pathological descriptions, attempted to re-create the lesions of Crohn’s disease. Especially noteworthy are the works of Kalima who obstructed short segments of the regional lymphatics of the small intestine with sclerosing agents, at first in the rat and later in the pig.20 21 Following such obstruction, these animals developed segmental intestinal disease characterised by many of the changes that occur in Crohn’s disease, including lymphocytic and granulomatous change in the lymphatics upstream of those obstructed, thickening of the bowel wall, aggregations of lymphocytes, a distribution similar to that described above, and enteroenteric and enterocutaneous fistulas. No animal model since that time has been able to achieve such resemblance to Crohn’s disease. Earlier on, in a similar attempt to reproduce the lesions of Crohn’s disease, Reichert and Mathes injected crystalline silica into lymphatics22 and Chess fed silica and talc to dogs.23 These latter workers are to be credited for their attempts; however, it was Kalima who achieved the greater result. Modern day rodent models of inflammatory bowel disease pale by comparison. Lymphocytic inflammation in the subserosa of the very thin walled intestine of the mouse or rat hardly approximates Crohn’s disease. We fail to see the resemblance between current rodent models and Crohn’s disease, and although one can certainly damage the mucosa of the intestine with 2,4,6-trinitrobenzene sulfonic acid or with dextran sodium sulfate, what results is mucosal damage and not the transmural regional enteritis of Crohn, Ginsburg and Oppenheimer.24
Especially noteworthy are the works of Kalima who obstructed short segments of the regional lymphatics of the small intestine with sclerosing agents, at first in the rat and later in the pig.
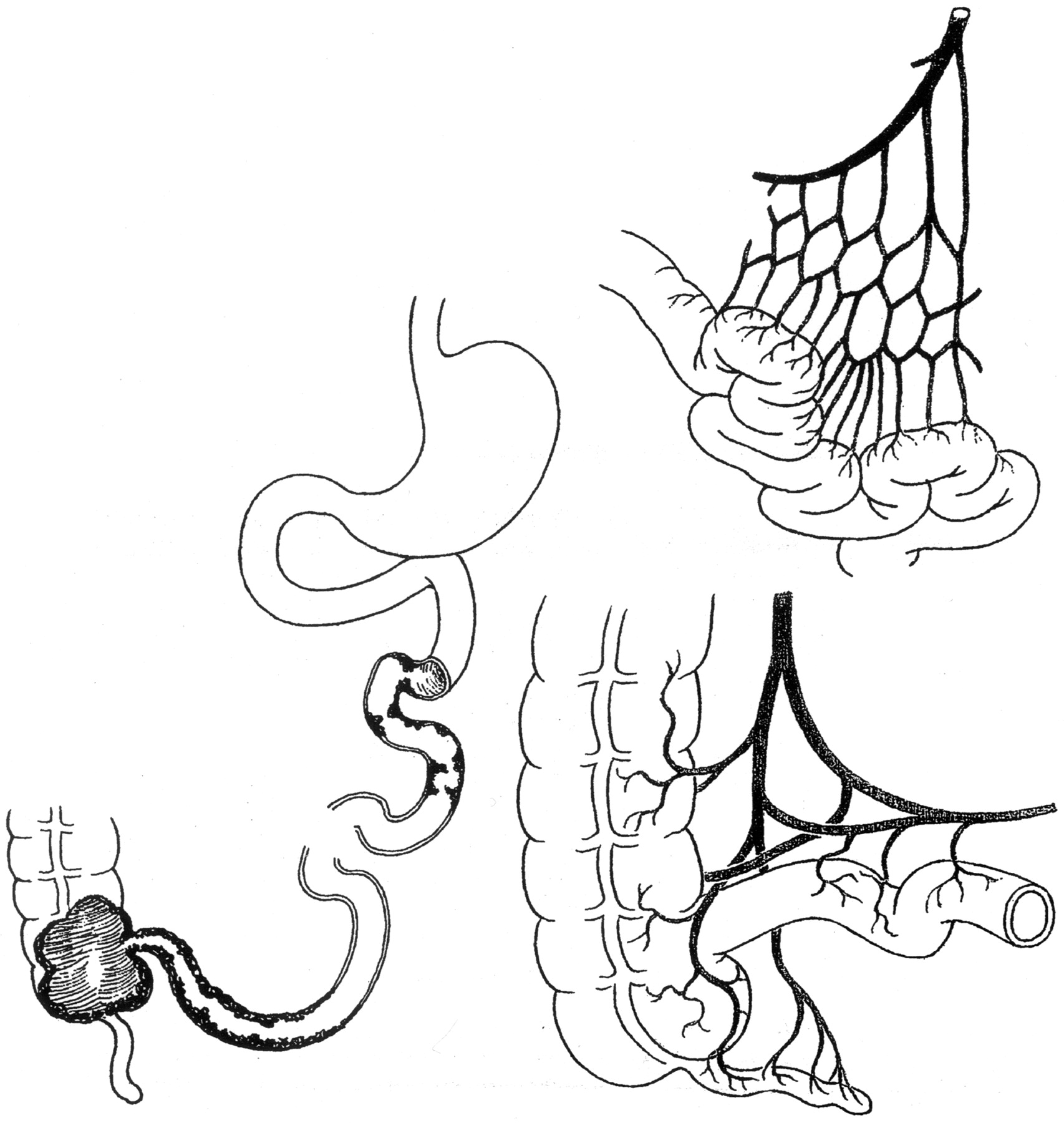
Tonelli et al have tried to make us aware that the distribution of lesions and the character of them represent an obstructive lymphocytic lymphangitis.25 26 Perhaps their work has not been widely appreciated. They have pointed out, for example, that the shorter segments of Crohn’s disease in the jejunum and the longer segments in the ileum are consistent with the shorter vasa recta of the jejunum and the longer lymphatic collecting ducts of the ileum (fig 3). 26 Another Italian surgeon, Del Gaudio, also proposed that the lymphatics were the root of Crohn’s disease. He went so far as to attempt to bring new lymphatic drainage to the resection anastomotic site by wrapping the junction with omentum.27 28 It is, however, questionable if the omentum has sufficient lymphatics to help the matter and if wrapping the site of an anastomosis represents a means of establishing increased lymphatic outflow.
{kind=link}
{kind=link}
{kind=link}
There are important reasons for re-emphasising the intestinal lymphangitis that occurs in Crohn’s disease. If intestinal lymphangitis is the root of the disease, then we need to focus on events that damage lymphatic endothelium. One may wish to recognise the lymphatic endothelium as putative target for whatever luminal agents or antigens are instigating the Crohn’s disease. Some bacteria are notable for producing lymphangitis, including streptococci,29 corynebacteria,30 pasteurellas31 and nocardia.32 33 Chlamydia suis when inoculated into weanling pigs produced a transmural enteritis with large lymphohistiocytic aggregates in the submucosa and lymphocytic aggregates that coursed through muscle coats and into the subserosa.34 Though not well appreciated, viruses can induce similar changes—for example, herpes viruses,35 adenoviruses36 and parvoviruses.37 In chronic hepatitis C, large aggregates of lymphocytes, often in a follicular pattern, occur in the portal tracks (lymphatics there)—a virus-induced lesion similar to those of the submucosa in Crohn’s disease.38 The Epstein-Barr virus induces large aggregates of lymphocytes, some of the time with follicular pattern,39 40 which begs the question, under what circumstances does Epstein-Barr virus target lymphatic endothelium. Are there other viruses that we need to seek?
If intestinal lymphangitis is the root of the disease, then we need to focus on events that damage lymphatic endothelium.
The idea that ingested microparticles may be responsible for Crohn’s disease fails to address the question of whether such particulate matter damage or have the potential to damage lymphatic endothelium.41 In 1985, Van Kruiningen et al described an intestinal lipogranulomatous lymphangitis of the dog: a disease that is characterised by segmental distribution and granulomas of the lymphatics, in this instance in response to retained dietary lipid material.42 It is not clear why this disease was not recognised prior to 1971, as the lesions are grossly evident where the mesentery attaches to the intestine and as the histopathology is unmistakable. No microorganisms have been identified in the intestinal lymphangitis of the dog, and in limited attempts the disease was not transmissible. Thus, we are inclined to attribute this new intestinal disorder to changes in the commercial diets fed to dogs: changes that have been significant since the end of World War II.
Appreciating that Crohn’s disease is a lymphocytic, granulomatous lymphangitis, aetiologists may choose to focus their attention on agents that target lymphatic endothelium.
What research does this call for? We believe that Kalima’s experimental pig model should be reproduced under modern day circumstances now that we have immunohistochemical reagents, such as antibodies to podoplanin,43 Prox-1,44 and LYVE-1,45 and monoclonal D2-4046 that will label lymphatics. There is also a need to re-examine lymphatic damage in early lesions and in resection specimens from patients with Crohn’s disease. Finally, appreciating that Crohn’s disease is a lymphocytic, granulomatous lymphangitis, aetiologists may choose to focus their attention on agents that target lymphatic endothelium.
REFERENCES
Footnotes
Competing interests: None.
Funding: HJ Van Kruiningen has been supported by the Broad Medical Research Program, and J-F Colombel by the Association F. Aupetit, Institut de Veille Sanitaire, INSERM and CH et U Lille.