Article Text

Abstract
BACKGROUND Platelet activating factor (PAF) is believed to amplify the activity of key mediators of the systemic inflammatory response syndrome (SIRS) in acute pancreatitis, resulting in multiorgan dysfunction syndrome. We tested the hypothesis that a potent PAF antagonist, lexipafant, could dampen SIRS and reduce organ failure in severe acute pancreatitis.
METHODS We conducted a randomised, double blind, placebo controlled, multicentre trial of lexipafant (100 mg/24 hours intravenously for seven days commenced within 72 hours of the onset of symptoms) involving 290 patients with an APACHE II score >6. Power calculations assumed that complications would be reduced from 40% to 24%. Secondary end points studied included severity of organ failure, markers of the inflammatory response, and mortality rate.
FINDINGS Overall, 80/138 (58%) patients in the placebo group and 85/148 (57%) in the lexipafant group developed one or more organ failures. The primary hypothesis was invalidated by the unexpected finding that 44% of patients had organ failure on entry into the study; only 39 (14%) developed new organ failure. Organ failure scores were reduced in the lexipafant group only on day 3: median change −1 (range −4 to +8) versus 0 (−4 to +10) in the placebo group (p=0.04). Systemic sepsis affected fewer patients in the lexipafant group (13/138v 4/148; p=0.023). Local complications occurred in 41/138 (30%) patients in the placebo group and in 30/148 (20%) in the lexipafant group (20%; p=0.065); pseudocysts developed in 19 (14%) and eight (5%) patients, respectively (p=0.025). Deaths attributable to acute pancreatitis were not significantly different. Interleukin 8, a marker of neutrophil activation, and E-selectin, a marker of endothelial damage, decreased more rapidly in the lexipafant group (both p<0.05); however, absolute values were not different between the two groups.
INTERPRETATION The high incidence of organ failure within 72 hours of the onset of symptoms undermined the primary hypothesis, and power calculations for future studies in severe acute pancreatitis will need to allow for this. Lexipafant had no effect on new organ failure during treatment. This adequately powered study has shown that antagonism of PAF activity on its own is not sufficient to ameliorate SIRS in severe acute pancreatitis
- platelet activating factor
- organ failure
- systemic inflammatory response syndrome
- lexipafant
- acute pancreatitis
Abbreviations used in this paper
- PAF
- platelet activating factor
- SIRS
- systemic inflammatory response syndrome
- IL
- interleukin
- MODS
- multiple organ dysfunction syndrome
- CRP
- C reactive protein
- PMN
- polymorphonuclear
- ERCP/ES
- endoscopic retrograde cholangiopancreatography/endoscopic sphincterotomy
- LREC
- local research ethics committee
- CT
- computerised tomography
- OFS
- organ failure score
- AUC
- area under the curve
Statistics from Altmetric.com
- platelet activating factor
- organ failure
- systemic inflammatory response syndrome
- lexipafant
- acute pancreatitis
Severe acute pancreatitis is characterised by systemic organ failure as well as local pancreatic complications1 and is still associated with a mortality rate of 15–30%, despite continuing improvements in critical care.2 Although the use of endoscopic sphincterotomy in patients with gall stones,3-5 selective gut decontamination,6and prophylactic antibiotics6 ,7 may be of benefit, specific medical therapy has not been successful.8 ,9
A change in the understanding of the pathophysiology of acute pancreatitis occurred with the suggestion that the initial phase of severe acute pancreatitis depends on neutrophil activation,10 accompanied by the systemic inflammatory response syndrome (SIRS).11 Organ failure is more important than pancreatic necrosis in the prediction of death in acute pancreatitis.12 Proinflammatory cytokines including interleukin (IL)-1β, IL-6., IL-8, tumour necrosis factor α, and platelet activating factor (PAF), and the anti-inflammatory cytokines IL-2 and IL-10, are implicated in the pathogenesis of SIRS in acute pancreatitis.13 This understanding has led to the development of an alternative treatment strategy aimed at interrupting the inflammatory response in an attempt to reduce the degree of SIRS and multiple organ dysfunction syndrome (MODS).2 ,14-18PAF may be induced from key cellular systems involved in SIRS, including endothelial cells, monocytes, neutrophils, and platelets, resulting in their activation with release of other proinflammatory cytokines.19 Moreover, PAF increases vascular permeability, induces leucocyte infiltration, oedema, and tissue injury, and has a negative inotropic effect.20 PAF is a particularly relevant target for therapy as its administration can induce experimental acute pancreatitis17 and because PAF antagonists ameliorate acute pancreatitis in other experimental models.17 ,20-23
Lexipafant is one of the most powerful PAF antagonists so far developed.24 Two phase II randomised trials involving a total of 133 patients with acute pancreatitis showed significant improvement in organ failure scores (OFSs).14 ,25 This report describes the results of a double blind, placebo controlled, randomised trial of lexipafant in consecutively screened patients with acute pancreatitis at high risk of a severe attack.
Methods
STUDY DESIGN
This was a multicentre, double blind, placebo controlled, randomised, parallel group, phase III study designed and conducted in accordance with the recommendations of the EEC Committee for Proprietary Medicinal Products.26 The primary objective was to determine if an infusion of lexipafant given within 72 hours of the onset of symptoms of predicted severe acute pancreatitis could reduce the frequency of systemic (organ failure) or local complications.1 The dose selected had been used in a phase II study25 (100 mg daily by infusion for seven days). This dose produced plasma concentrations of lexipafant of more than 10 times those needed to abolish the effects of PAF in ex vivo experiments. Selection of patients with an APACHE II score >6 was expected to produce a frequency of severe (that is, complicated) acute pancreatitis of 40%. To show a 40% reduction in the frequency of complications (from 40% to 24%) given α=0.05 with a power of 80%, each group required 150 patients. No interim analysis was carried out. Secondary objectives were assessment of the influence of lexipafant on measures of disease severity, as shown by OFS, incidence of sepsis, and plasma markers of the inflammatory response (IL-8, E-selectin, IL-6, C reactive protein (CRP), and polymorphonuclear (PMN) elastase), duration of hospital and intensive care unit (ICU) stay, and mortality rate. Patients were assessed daily for nine days and then weekly until discharge from hospital. All complications, adverse events, and any deaths, in hospital or after discharge, were recorded. The clinical care of the patients remained with the responsible clinician in each hospital. All patients underwent ultrasonography to detect gall stones. Computerised tomography (CT) was undertaken on clinical grounds at the request of the responsible clinician. Similarly, the use of antibiotics and endoscopic retrograde cholangiopancreatography and endoscopic sphincterotomy (ERCP/ES) was not specified, although recorded. As the study neared completion, a closure date was set to allow projected inclusion of 300 patients.
Study location
Eighteen centres (see appendix ) recruited patients from 78 hospitals in the UK between November 1994 and August 1996 (see appendix). Study personnel from each centre visited adjacent hospitals to recruit patients and to administer trial medication.
Inclusion and exclusion criteria
All of the following were required for inclusion: severe abdominal pain of <72 hours duration at initiation of study treatment; serum amylase level >3 times the upper limit of the normal range in the 72 hours before study entry; a clinical picture consistent with acute pancreatitis; and an APACHE II score27 >6 in the 24 hours before study entry. Patients were excluded for any one of the following reasons: age <18 or >80 years; premenopausal women in whom pregnancy could not be excluded; pancreatitis believed to be due to trauma, surgery, neoplasm, or ERCP/ES; patients unsuitable for ventilation because of pre-existing illness; patients who had received other investigational agents in the preceding three months; patients receiving oral anticoagulant therapy; and patients who had previously received lexipafant.
Assignment and drug administration
After enrolment, patients were randomly allocated to receive an intravenous infusion containing lexipafant (British Biotech Pharmaceuticals Ltd, Oxford, UK) or an identical placebo infusion. Lexipafant was presented in ampoules containing 5 mg/ml in aqueous solution buffered to pH 3.9–4.4. Placebo ampoules contained vehicle only. The medication was diluted in 0.9% NaCl or 5% dextrose solution and infused over 10 minutes to provide a 4 mg loading dose, followed by 4 mg in 20 ml/h for 168 hours.
Ethical considerations
The study was conducted in accordance with recommendations for good clinical practice.26 In each participating hospital the local research ethics committee (LREC) gave approval for the study before patient recruitment began and all amendments were submitted to the LREC. Informed consent was obtained from patients or, if they were unable because of severity of illness, from their next of kin.
ASSESSMENT OF OUTCOME
Organ failure
Organ failure was defined as follows:cardiovascular failure if systolic blood pressure was ⩽90 mm Hg despite fluid replacement;respiratory failure if the PaO2/FiO2 ratio was ⩽300 mm Hg;central nervous system failure if the Glasgow coma score was <13; coagulopathy if platelet count was ⩽80×109/l; andrenal failure if plasma creatinine was >170 μmol/l.
Local complications
Pancreatic necrosis was diagnosed by CT showing non-enhancing pancreatic parenchyma (tissue density <50 Hounsfield units after intravenous contrast) >3 cm in size, or >30% of the area of the pancreas. Pancreatic abscess was defined as a circumscribed intra-abdominal collection of pus in the proximity of the pancreas containing little or no necrotic material. Pseudocyst was defined as fluid collection rich in pancreatic enzymes, enclosed in a non-epithelial wall and present at least four weeks after the onset of acute pancreatitis. Acute fluid collections, which occurred within the first four weeks of acute pancreatitis located in or near the pancreas and lacking a wall of granulation and fibrous tissue, were not included as a complication.
Organ failure score (OFS)
OFS was calculated as suggested by Bernard and colleagues28 (table 1). Hepatic failure was not included in the calculation of OFS, in accordance with the Atlanta criteria, because in acute pancreatitis elevated bilirubin more commonly represents biliary obstruction than hepatocellular damage.
Organ failure scores. Each organ failure was scored 0–4 as defined by Bernard and colleagues.28 The score for each patient was the sum of the scores for each organ/system
Sepsis
Sepsis was defined as two or more signs indicative of SIRS, with simultaneous evidence of infection shown by positive bacterial or fungal cultures.29
Blood assays
Blood samples were obtained before study entry, at 12 and 24 hours after entry, and for up to nine days after admission to the study for estimation of IL-8, E-selectin, IL-6, CRP, and PMN elastase. Serum was stored at −20°C and the assays were performed at a central laboratory (Ravenscourt Laboratories). IL-8, E-selectin, and IL-6 were determined using Quantikine kits (Research and Diagnostic Systems, Minneapolis, USA). Detection limits were 18 pg/ml for IL-8, <0.1 ng/ml for E-selectin, and 0.35 pg/ml for IL-6. PMN elastase was assayed using either the IMAC technique or ecoline PMN elastase kits (both Merck Ltd, Lutterworth, Leics, UK); the lower limits of sensitivity of the assays were 8 μg/l and 4 μg/l, respectively. CRP was measured using TINA-QUANT kits (Boehringer-Mannheim, Germany). Routine haematology, biochemistry, coagulation, and urine analysis were performed at the participating hospitals.
Deaths
These were categorised as attributable to acute pancreatitis or otherwise by the principal investigators, before the randomisation code was broken. The protocol contained provision for subgroup analysis of deaths in patients treated within 48 hours of the onset of symptoms.
Serious adverse events
The principal investigator in each centre was asked to decide whether in their opinion any adverse advent was drug related. Lexipafant levels were determined in blood samples from patients with any adverse events.
STATISTICAL ANALYSIS
Data on the clinical record forms were entered into a Clintrial database on a VAX 4015A computer. All data entry was verified by an independent observer by means of blinded duplicated data entry. Data records were downloaded into ASCII files and converted into SAS version 6.11 data sets (SAS Ist, Cary, North Caroline, USA). Categorical data were analysed using the χ2 test and Fisher's exact probability test. Continuous variables were compared using the Wilcoxon rank sum test. The probability of death was modelled using a logistic regression analysis with duration of symptoms before treatment and baseline OFS as covariates together with an interaction of treatment by duration of symptoms. The estimated log odds ratio for death related to symptom duration was calculated by: log (odds: lexipafant group)−log (odds: placebo group).30 An algorithm was written to allow interpolation of missing data for calculation of OFSs (see appendix ). Changes from baseline values of inflammatory markers were calculated for each patient, median values were plotted, and the area under the curve (AUC) was used for comparison of treatment groups.
Results
A total of 2340 patients were screened of whom 379 (16.2%) were eligible for the study but 88 were not recruited because consent was withheld (n=80), study personnel were not available (n=4), or LREC approval had not been completed (n=4). Of the 291 (76.8%) patients randomised, one withdrew from the study before receiving any trial medication and was not considered in any subsequent analysis. Thus 139 were randomised to the placebo group and 151 to the lexipafant group.
Antibiotics were given to 75 (54%) patients in the placebo group on the first day versus 72 (49%) in the lexipafant group; in the first week these values were 100 (72%) and 97 (66%), respectively. Ten patients in the placebo group underwent ERCP/ES within 48 hours compared with 11 in the lexipafant group. Between three and seven days, the respective values were eight and six patients, and after this, nine and 17 patients, respectively.
There were 42 (14%) deaths, of which 35 were attributed to acute pancreatitis. In three cases death was not due to acute pancreatitis but to multiple thrombotic episodes (placebo), myocardial infarction, (lexipafant), and pulmonary emboli (lexipafant) (one patient each). Three patients died after having been discharged from hospital following complete recovery from acute pancreatitis: one each from myocardial infarction at 115 days (placebo), brain stem infarction at 168 days (lexipafant), and pneumonia complicating a second attack of acute pancreatitis at 63 days (placebo). One further patient (lexipafant) died from metastatic carcinoma and was not actively treated (major protocol violation). Analysis of deaths attributable to pancreatitis therefore was based on 136 patients in the placebo group and 147 in the lexipafant group (fig 1). Other outcome variables were analysed after excluding patients with an incorrect diagnosis or major protocol violation (138 in the placebo group and 148 in the lexipafant group). Patient characteristics (table 2) and aetiology were similar in the two groups.
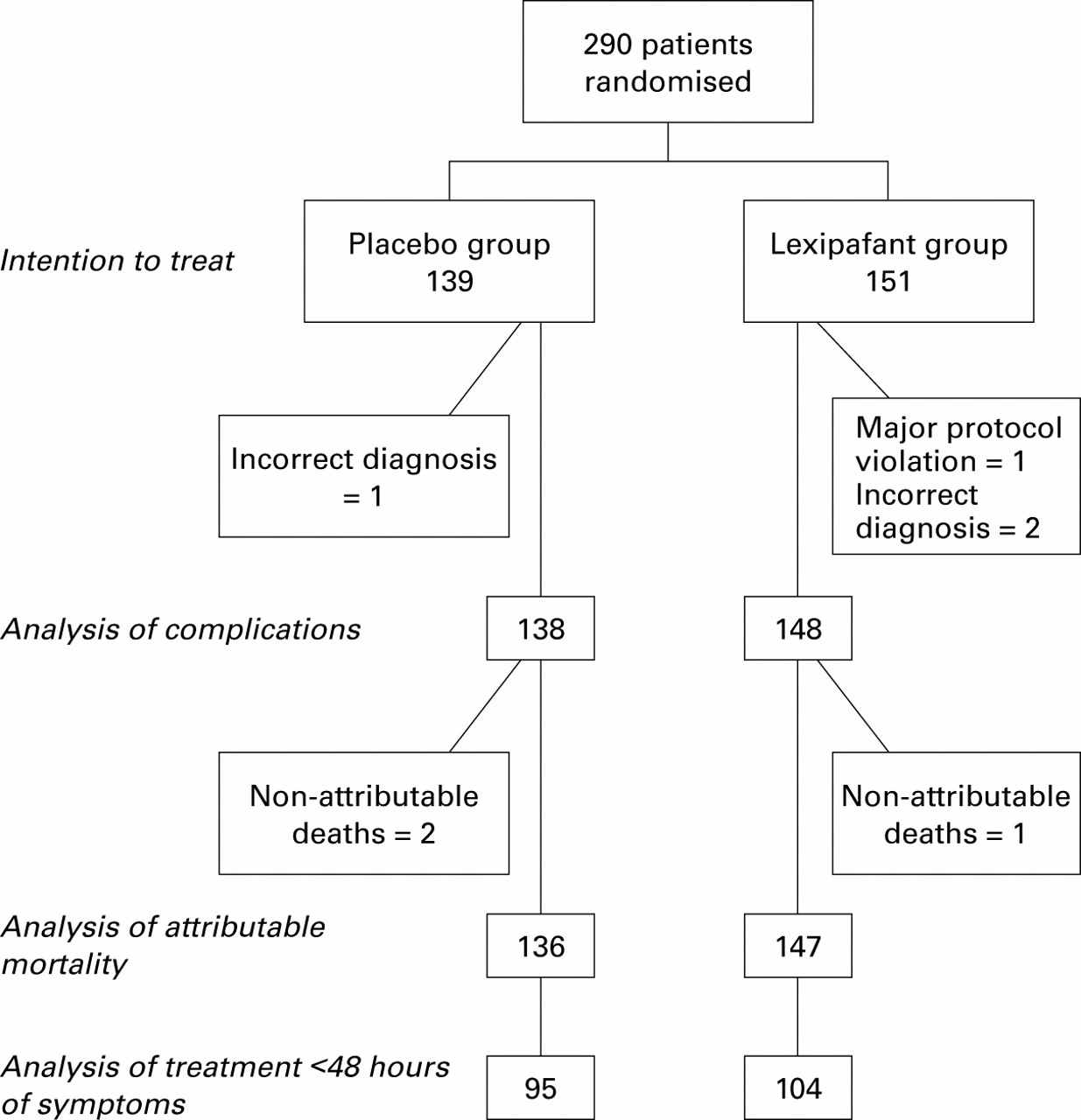
Summary of patients treated. A total of 2340 patients were screened; 379 were eligible and 291 were randomised. One patient withdrew after randomisation. Treatment allocations, exclusions, and non-attributable deaths showing the basis for analysis of outcome by intention to treat, complications, and attributable mortality.
Charactistics of all patients in the two treatment groups at the time of entry to the study
COMPLICATIONS
Incidence of organ failure
We found that 126 (44%) of the 286 patients already had organ failure on the day of admission and new organ failure developed in only 39 (14%) patients (table 3). The difference in total frequency of organ failure was 0.5% (95% confidence intervals (CI) −11 to +12%). New organ failure developed in 21 of 79 patients without organ failure who received placebo, and in 18 of 81 who received lexipafant, a difference of 4% (95% CI −9 to +17%). These differences between groups were not significant.
Incidence of organ failure, local complications, and deaths in the two groups
Incidence of local complications
CT was performed in 62 (45%) patients in the placebo group and in 56 (38%) in the lexipafant group. Significantly more patients developed a pseudocyst in the placebo group (p=0.025) but overall the number of patients who developed local complications in the two groups was not significantly different (table 3). Fifty nine (85%) of 71 patients with local complications also had early organ failure; of the 165 patients with organ failure, 36% developed local complications. Thirty six (45%) of 80 patients in the placebo group who had organ failure developed local complications compared with 23 (27%) of 85 patients in the lexipafant group (χ2=5.78, p=0.016).
CHANGES IN OFS
Mean OFS decreased consistently from the baseline score in the lexipafant group whereas in the placebo group there was an initial increase over days 1 and 2 (fig 2). The median change at day 3 was zero (range −4 to +10) in the placebo group and −1 (−4 to +8) in the lexipafant group (p=0.04). There was no significant difference in the change in OFS at day 7 between the two groups (−1 (−5 to + 15) and −1 (−6 to +9), respectively).

Mean organ failure scores (OFS) in the placebo and lexipafant groups (mean (SEM)). Values observed on day 3 were significantly different in the placebo and treatment groups (p=0.039).
SYSTEMIC SEPSIS
Thirteen (9%) patients in the placebo group developed sepsis compared with four (3%) in the lexipafant group (p=0.023).
INFLAMMATORY MARKERS
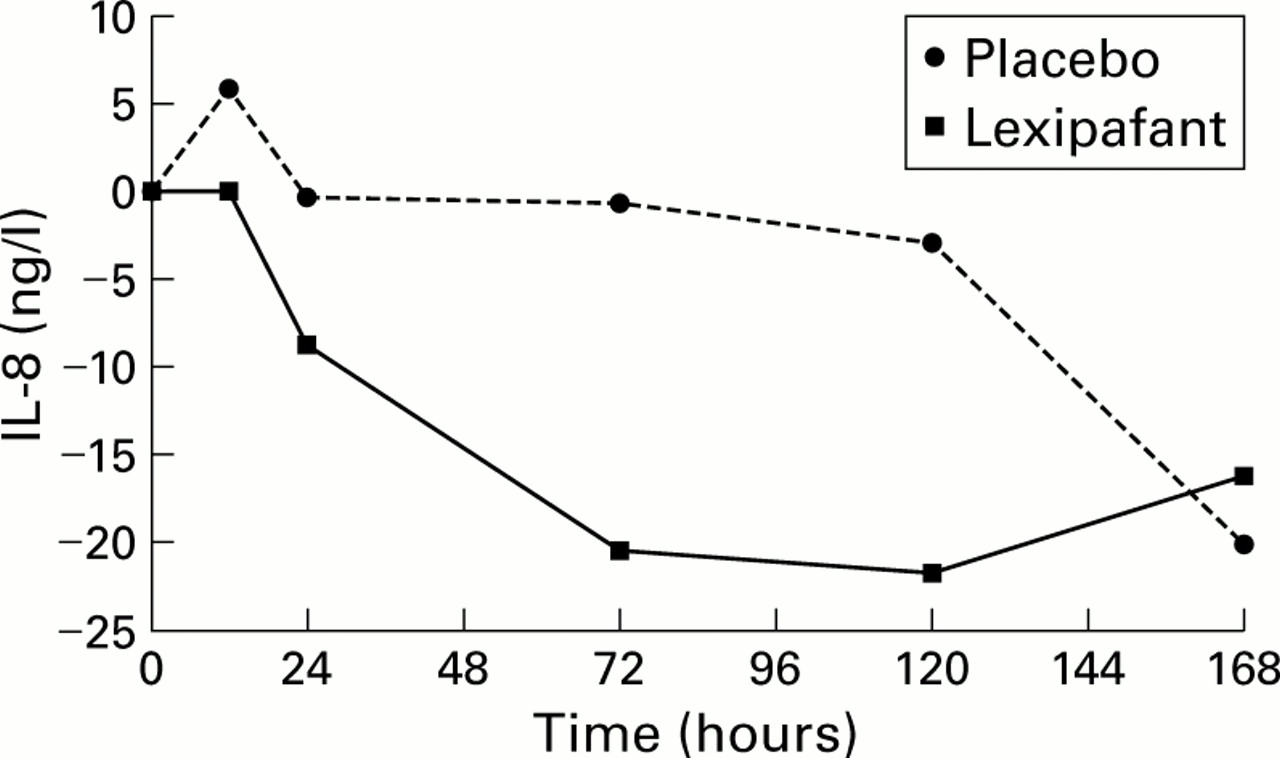
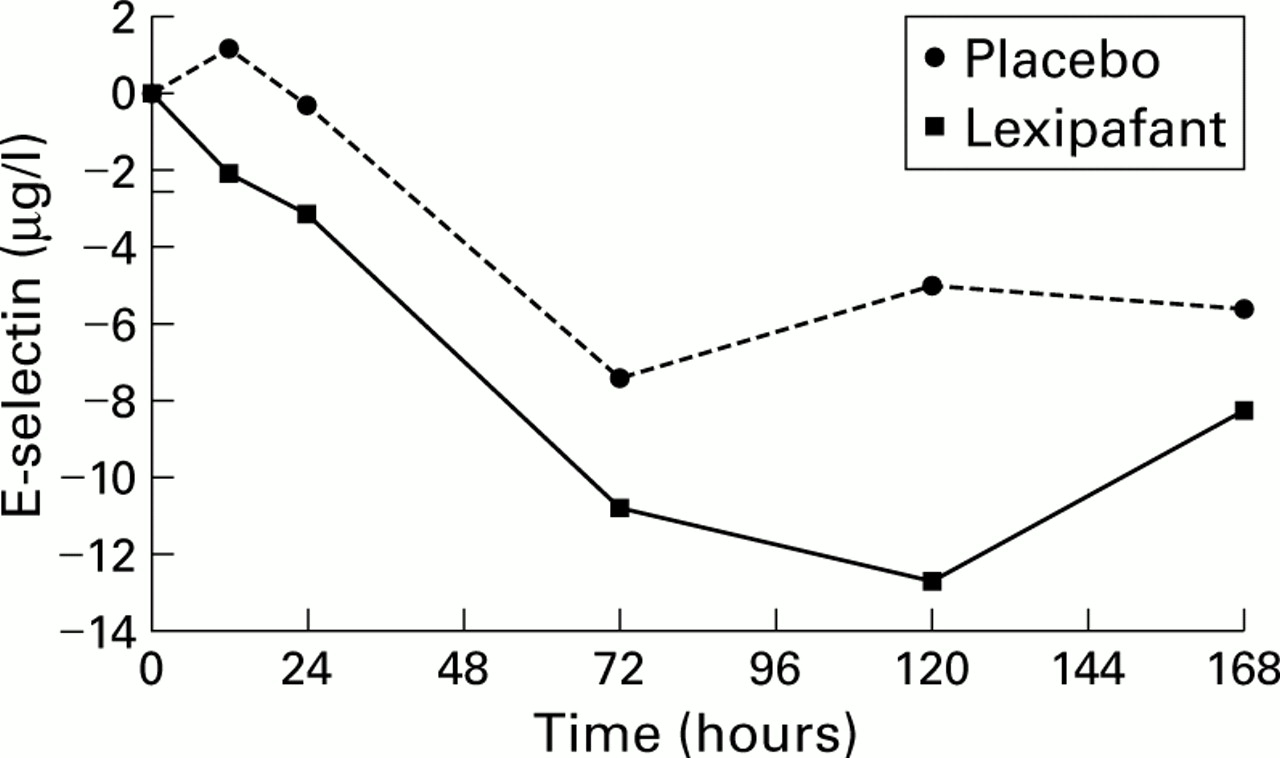
Median (interquartile range) baseline values of IL-8 were 31 (0–69) ng/l in the placebo group and 37 (0–80) ng/l in the lexipafant group; E-selectin values were 67 (51–100) μg/l and 70 (53–104) μg/l, respectively. IL-8 and E-selectin levels increased compared with baseline values at 12 hours in the placebo group but not in the lexipafant group (figs 3, 4). Overall, changes from baseline in IL-8 and E-selectin concentrations were significantly different, although there were no differences in absolute values at any time point. Values for IL-6, CRP, and PMN elastase were not significantly different between the two groups (data not shown).
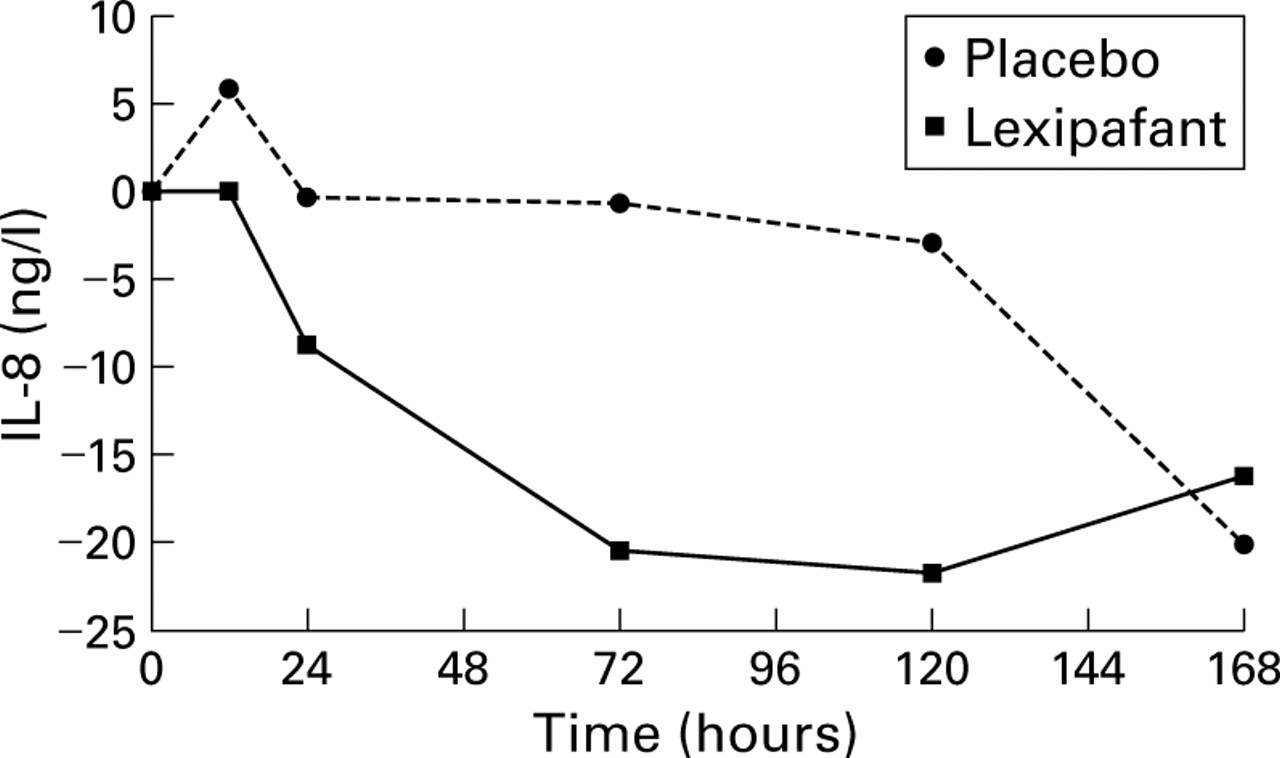
Median (interquartile range) changes in interleukin 8 (IL-8) levels from baseline values given in the text. Values observed 12 hours after the start of therapy were significantly different (p=0.006, Wilcoxon rank sum test). Median area under the curve (AUC) for placebo was 0 (−499 to 9820) and for lexipafant –1.53 (−3890 to 1190) (p=0.003).

Median (interquartile range) changes in E-selectin levels from the baseline values given in the text. Values observed 12 hours after the start of therapy were significantly different (p=0.005, Wilcoxon rank sum test). Median area under the curve (AUC) for placebo was −0.0 (−24 to 130) and for lexipafant −1.3 (−95 to 77) (p=0.03).
LENGTH OF HOSPITAL/ICU STAY
Median hospital stay for all patients was 10 (range 0–304) days in the placebo group and 9 (3–137) days in the lexipafant group. Hospital stay in surviving patients was 9 (1–304) days in the placebo group and 9 (3–137) days in the lexipafant group. Twenty four of the lexipafant treated patients and 25 of the placebo treated patients were admitted to the ICU. Median ICU stay was 11 (1–132) days in the placebo group and 9.5 (1–71) days in the lexipafant group. Of these, 12 in the placebo group and eight in the lexipafant group died. In survivors, median ICU stay was 12 (1–45) days in the placebo group and 14 (5–71) days in the lexipafant group. None of these observations was significantly different.
DEATHS
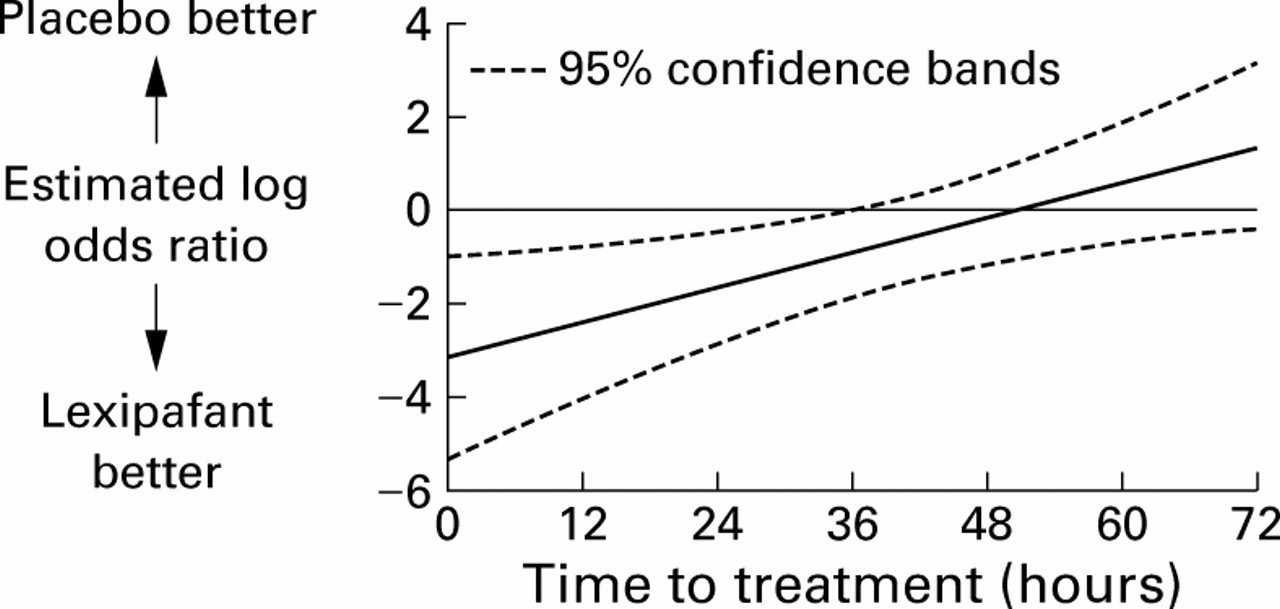
There were 21 (15%) attributable deaths in the placebo group and 14 (10%) in the lexipafant group (χ2=2.23, p=0.131). There were eight attributable deaths in the placebo group versus five in the lexipafant group during the first week and 13 versus nine deaths after the first week. Logistic regression analysis suggested that the probability of death was significantly reduced by early treatment with lexipafant (p<0.05) (fig 5). All patients who died in the first week had organ failure; all patients except one who died subsequently had experienced organ failure within the first week.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between duration of symptoms before treatment and risk of death, expressed as log odds ratio of death in the lexipafant group compared with the placebo group. Solid line, estimated ratio; broken lines, 95% confidence intervals.
ADVERSE EVENTS
There were no significant differences in overall or serious adverse events between the two groups.
Discussion
This is the largest systematic prospective study of severe acute pancreatitis ever undertaken and has revealed new insights into the natural history of the disease. Forty four per cent of patients with a predicted severe attack (APACHE II score >6 within 24 hours of admission) had organ failure within 72 hours of the onset of symptoms; new organ failure developed in only 14% of patients after entry to the study. Although the study design included patients with an admission APACHE II score >6, because previous reports indicated that the proportion of patients developing a severe complication (MODS and/or local pancreatic complications) would be 45%,31 ,32 the high incidence of organ failure at the time of entry to the study meant that we could not test the primary end point of reduced frequency of complications. The majority of organ failures had occurred before initiation of treatment, and the study lacked power to confirm an effect on the small numbers of new organ failure. This new observation has important implications for the design of future studies in patients with predicted severe acute pancreatitis
Eighty three per cent of patients who developed local pancreatic complications had early organ failure; conversely, 36% of patients with organ failure developed local pancreatic complications. Nearly all deaths (34/35 or 97%) occurred in patients who had early organ failure.
These findings are contrary to the view that death in the first week can be avoided by intensive care support and that subsequent deaths are due to local pancreatic complications which can be managed effectively by surgical intervention.33 This perception is derived from series with highly selected patient groups. In contrast, the present population based study showed that deaths occur both early and late, principally from MODS. This is consistent with the findings of a review of national figures from Scotland, which included nearly 14 000 cases of acute pancreatitis. Of the patients who died, 54% did so in the first seven days of admission.34 The cause of these early deaths was usually MODS.
A recent study has shown that pancreatic necrosis is only predictive of death if MODS is present as well.12 In the present studylate deaths also occurred, almost invariably in patients who had early MODS, which lends support to the two hit hypothesis of SIRS and MODS.35 The type of response of the immune system to the first hit (onset of acute pancreatitis and SIRS) determines the outcome during the recovery phase from a second hit (such as secondary sepsis, gall stone obstruction of the main pancreatic duct, bleeding, etc), resulting either in a muffled re-enaction of SIRS or fatal MODS.
The realisation that SIRS is an important component of the pathophysiology of severe acute pancreatitis,36 and that this might be susceptible to modification by antagonists of known mediators of the inflammatory response, provided reason to study lexipafant, a PAF antagonist which is more potent in ligand binding than PAF itself. The PAF molecule has a major role in promoting and amplifying white cell-endothelial interactions involving activation of various chemokines, cell adhesion molecules, and integrins, resulting in the ingress of highly active white cells into the parenchyma and consequent MODS.19 There was some evidence that lexipafant treated patients showed a more rapid reduction in plasma levels of the inflammatory markers IL-6 and E-selectin, although absolute values were not different. The only clinical correlate of this observation was reduction in OFS on day 3 in the lexipafant group, although there was no overall difference in the numbers of patients with organ failure. Interestingly, sepsis, a clinically important expression of severe organ failure, was less frequent in the lexipafant treated patients.
Two previous phase II randomised studies showed more rapid reduction in OFSs without the development of new organ failure in lexipafant treated groups.14 ,25 In the present study, with greater numbers of patients, there was no significant effect of lexipafant on the development of new organ failure. In addition, at the end of the treatment period there was no difference in OFSs between the two groups, in contrast with the findings in the smaller phase II studies.14 ,25
Detection of pancreatic necrosis is dependent on the rate of use of CT. As CT was performed in only 41% of patients, data on pancreatic necrosis need to be treated with circumspection. Nevertheless, the development of pseudocysts and local complications in patients with organ failure was also significantly reduced in the lexipafant group.
Post hoc logistic regression analysis showed that treatment with lexipafant and earlier institution of therapy were highly related to a lower mortality rate. However, the results of a much larger phase III study do not support the hypothesis that administration of lexipafant within 48 hours of the onset of symptoms reduces the mortality rate in severe acute pancreatitis (unpublished data).
In conclusion, the efficacy of lexipafant was rigorously tested (in a double blind manner) within the general service provision of 78 hospitals in the UK, principally district general hospitals. There was a high frequency of organ failure at study entry. Consequently, the study failed to demonstrate its primary end point of a reduction in the frequency of organ failure, and it is now clear that the total frequency of organ failure was not an appropriate end point for assessment of new therapies in predicted severe acute pancreatitis. There was no reduction in new organ failure with lexipafant treatment. Antagonism of PAF activity does not appear to influence the course of organ failure in severe acute pancreatitis.
Acknowledgments
The authors wish to thank all those who contributed patients, and all the co-investigators listed in appendix for their dedication to data collection. We are grateful to Professor Sir David Cox, Professor of Statistics, University of Oxford, UK, for advising on the statistical analysis. This study was funded by British Biotech Pharmaceuticals Ltd, Oxford, UK. Financial support to meet staff costs and other running costs was provided at each study centre (see appendix).
Appendix
Details of the study centres and participants are given in table TAI.
Study centres and participants
Appendix
Details of all participating hospitals are given in table TAII.
Full list of participating hospitals
Appendix
Algorithm for interpolation of missing data points to enable calculation of organ failure scores for each day during the study treatment period is described below. Where data were missing at day 0 or at hospital discharge, “normal” values were assigned, as shown in table TAIII.
Missing FiO2 values from day 0 to hospital discharge were set at 21% (room air).
If PaO2 was missing at all time points, it was set at 11.5 kPa at any time point for which FiO2 >21%.
For any group of three consecutive time points at which FiO2 was 21% or missing and PaO2 was missing, the middle value of PaO2 was set to 11.5 kPa (giving a PaO2/FiO2 ratio of 411.74—that is, 11.5 (0.21×0.133)).
Where raw data were missing for any of days 1–7, missing values were estimated by linear interpolation using available data from the nearest days before and after the time point. For example, the value of a parameter at day k between days m and n was estimated by: value at day k=value at day m+(k−m) (n−m)×value at day n−value at day m). (In the case of respiratory data, it is the PaO2/FiO2 ratio, rather than PaO2, that is interpolated).
The last recorded OFSs of patients who died were carried forward until the day of death. If death occurred before day 7, scores of 0 for any organ on the day of death were carried forward up to day 7. Scores of >0 on the day of death were replaced by 4 on the day of death and carried forward up to day 7.
“Normal” values assigned in the algorithm for interpolation of missing data points to enable calculation of organ failure scores for each day during the study period, where data were missing at day 0 or at hospital discharge
Abbreviations used in this paper
- PAF
- platelet activating factor
- SIRS
- systemic inflammatory response syndrome
- IL
- interleukin
- MODS
- multiple organ dysfunction syndrome
- CRP
- C reactive protein
- PMN
- polymorphonuclear
- ERCP/ES
- endoscopic retrograde cholangiopancreatography/endoscopic sphincterotomy
- LREC
- local research ethics committee
- CT
- computerised tomography
- OFS
- organ failure score
- AUC
- area under the curve