Article Text

Abstract
BACKGROUND Activated T cells are more susceptible to apoptosis than resting T cells. As intestinal T cells normally exhibit a higher state of activation, increased apoptosis may be necessary to maintain immune homeostasis in the specialised microenvironment of the mucosa. On the other hand, in Crohn's disease (CD) mucosal T cells are resistant to apoptosis, suggesting abnormal regulation of cell death mechanisms.
AIMS To investigate differences in expression of anti- and proapoptotic Bcl-2 family proteins, key regulators of apoptosis, between circulating and mucosal T cells, and possible alterations in CD.
PATIENTS AND METHODS Lamina propria T cells (LPT) were isolated from 10 control, seven CD, and eight ulcerative colitis (UC) patients, and peripheral blood T cells (PBT) from healthy volunteers. Purified T cells were stained intracellularly for Bcl-2, Bcl-xL, and Bax, and mean fluorescence intensity measured by flow cytometry.
RESULTS Compared with PBT, the expression level of Bcl-2 and Bax, but not Bcl-xL, was significantly greater in LPT, resulting in lower Bcl-xL/Bax ratios. In PBT, Bax expression was highly and significantly correlated with both Bcl-2 and Bcl-xL, but correlation with Bcl-2 was absent in LPT. Bax expression in CD, but not UC, LPT was significantly lower than in control LPT, resulting in a significantly higher Bcl-xL/Bax ratio. The significant correlation of Bcl-xL to Bax was preserved in CD, but not UC, LPT.
CONCLUSIONS Regulation of Bcl-2 family protein expression differs between circulating and mucosal T cells, probably underlying diverse survival potentials. In CD LPT, a low Bax expression and a high Bcl-xL/Bax ratio favour resistance to apoptosis and may contribute to the chronicity of inflammation.
- Bcl-2 family proteins
- apoptosis
- inflammatory bowel disease
- T cells
- Crohn's disease
- ulcerative colitis
Abbreviations used in this paper
- CD
- Crohn's disease
- IBD
- inflammatory bowel disease
- LPT
- lamina propria T cells
- PBT
- peripheral blood T cells
- UC
- ulcerative colitis
Statistics from Altmetric.com
Apoptosis is a physiological process of programmed cell death that is critical for organ development, tissue homeostasis, and elimination of abnormal or dangerous cells.1 Within the lymphoid system, apoptosis is fundamental to maintain immune homeostasis2 through a variety of regulatory mechanisms, including growth factor deprivation, oxidative stress, and triggering of death receptors.3 ,4 Prominent among the latter is the Fas receptor which is fundamental to T cell apoptosis,5yet susceptibility to cell death varies considerably among T cells. Naive T cells are largely Fas negative and thus resistant to Fas mediated apoptosis, unlike memory T cells which are mostly Fas positive.3 The normal intestinal mucosa is populated almost exclusively by Fas positive memory T cells and on Fas ligation the majority of lamina propria T cells (LPT) undergo apoptosis, in contrast with naive peripheral blood T cells (PBT) which are far less susceptible to death by the Fas pathway.6 Gut LPT are believed to be long lived to afford protection when eventually challenged by the original sensitising antigens. This implies that several mechanisms or factors must act to enable them to survive in the mucosal microenvironment in spite of their high susceptibility to cell death.7 Therefore, intrinsic differences must exist in regulatory mechanisms of T cell apoptosis between the circulation and the gut.
Abnormal regulation of apoptosis results in disease, including cancer, viral infections, neurodegenerative disorders, and acquired immunodeficiency syndrome.1 In particular, the development of autoimmunity is thought to be caused by defective T cell apoptosis,8 a phenomenon reported in several immune mediated diseases such as chronic atopic dermatitis, congenital lymphoproliferative syndrome with autoimmunity, rheumatoid arthritis, and asthma.9-12 Abnormal T cell apoptosis also appears to be involved in chronic inflammatory diseases of uncertain aetiology such as inflammatory bowel disease (IBD). Mucosal T cells derived from inflamed bowel segments display diminished susceptibility to apoptosis compared with T cells from normal mucosa.13 ,14 Boirivantet al have reported that LPT from Crohn's disease (CD), ulcerative colitis (UC), and diverticulitis are resistant to CD2 mediated apoptosis.13 We have reported that T cells derived from CD but not UC mucosa are resistant to a variety of apoptosis inducing signals, including growth factor deprivation, Fas ligation, and nitric oxide.14
Among the various factors responsible for regulation of T cell apoptosis, the family of Bcl-2 related proteins plays a pivotal role. This family contains several proteins with opposing activity, such as Bcl-2 and Bcl-xL which protect from apoptosis, and Bax which promotes apoptosis. What dictates the relative sensitivity or resistance to cell suicide is not their absolute level but the relative balance between the concentration of these antagonist and agonist proteins.15 ,16 Differences in susceptibility to death among T cells from different organs, or T cells from normal and disease tissues, are associated with altered ratios of Bcl-2 family proteins, as observed in aging, infectious, neoplastic, and autoimmune disease.11 ,17-20 Therefore, this study was designed to assess and compare expression of Bcl-2 family proteins in PBT and LPT, as well as T cells from normal, CD, and UC mucosa, and determine whether altered protein ratios could explain resistance of CD mucosal T cells to apoptosis.
Methods
PATIENT POPULATION
Surgical specimens from patients undergoing bowel resection at the University Hospitals of Cleveland and the Cleveland Clinic Foundation were used as a source of LPT. In IBD patients, LPT were isolated from macroscopically involved, dysplasia free segments of the bowel. In patients operated on because of colon cancer, LPT were derived from histologically normal areas of the mucosa at least 10 cm from the lesion. All diagnoses were confirmed by clinical, radiological, endoscopic, and histological criteria.
Crohn's disease
Seven patients with CD were studied. The group included three women and four men, aged 15–61 years. According to criteria established by De Dombal and colleagues,21 disease activity was classified as moderate in five and severe in two patients. The disease had been present from three months to 11 years. One patient had pure ileal involvement, three had ileocolic, and three had colonic involvement. Five patients were operated on for failure of medical therapy, one for bowel obstruction, and one for intractable pain. At the time of resection, one patient was receiving only corticosteroids, one was receiving corticosteroids and aminosalicylates, three were receiving corticosteroids and 6-mercaptopurine, one was on steroids and metronidazole, and one was on no specific therapy.
Ulcerative colitis
Eight patients with UC undergoing colectomy were evaluated; one woman and seven men, aged 28–77 years. Based on the criteria of Truelove and Witts,22 three patients had mild, two moderate, and three severe disease activity. The disease had been present for 1–30 years as partial or total colitis. Two patients were operated on for persistent bleeding, three for failure of medical therapy, one for benign colonic stricture, and two for dysplasia. Two patients were receiving corticosteroids and aminosalicylates, one aminosalicylates only, two corticosteroids, aminosalicylates, and 6-mercaptopurine, one aminosalicylates and folic acid, one corticosteroids, aminosalicylates, and 6-mercaptopurine, and one no specific treatment.
Controls
Ten surgical control patients admitted for bowel resection for malignant and non-malignant conditions were studied. Nine had adenocarcinoma of the large bowel, anywhere from the caecum to the rectum. Four patients were women and five were men, aged 37–80 years. One patient (a 64 year old woman) had colonic resection because of diverticular disease. Healthy volunteers served as the source of PBT. This study was approved by institutional review boards of the University Hospitals of Cleveland and the Cleveland Clinic Foundation.
ISOLATION OF LPT AND PBT
Lamina propria mononuclear cells were isolated as previously described,23 and macrophages were depleted by plastic adherence. For LPT purification, macrophage depleted lamina propria mononuclear cells were incubated for 30 minutes at 4°C with magnetically labelled anti-CD19, anti-CD14, and anti-CD16 antibodies directed against B lymphocytes, monocytes, and neutrophils, respectively (Miltenyi Biotec Inc., Auburn, California, USA). T cells were then isolated by negative selection using magnetic cell sorting (MACS; Miltenyi Biotec Inc.). PBT were isolated from heparinised venous blood using a Ficoll-Hypaque density gradient, and after monocyte depletion PBT were isolated by the same process of negative selection. In some experiments, PBT were enriched for CD45RO+ memory T cells by negative selection using a magnetically labelled CD45RA antibody. Resulting cell populations averaged 95% viability and exceeded 94% purity.
FLOW CYTOMETRIC ANALYSIS
Before intracellular staining, LPT and PBT were permeabilised using Permeafix (Ortho Diagnostic System Inc., Raritan, New Jersey) according to the manufacturer's instructions. Permeabilised cells were then stained with rabbit antihuman Bcl-2, Bcl-xS/L, or Bax (Santa Cruz Biotechnology Inc., Santa Cruz, California, USA) as primary antibodies for 20 minutes at room temperature. After washing, cells were stained with a secondary fluorescein labelled antirabbit IgG for 20 minutes at room temperature, after which cells were washed and analysed by a FACScan flow cytometer (Becton Dickinson, San Jose, California, USA).
STATISTICAL ANALYSIS
Data are expressed as mean (SEM). StatView software (Abacus Concepts, Inc., Berkeley, California, USA) was used to perform the Mann-Whitney U (unpaired) test for non parametric data analysis, and to calculate the regression coefficient (r) from correlations between two groups of data; p<0.05 was considered significant.
Results
DIFFERENTIAL EXPRESSION OF Bcl-2 FAMILY PROTEIN IN PBT AND LPT
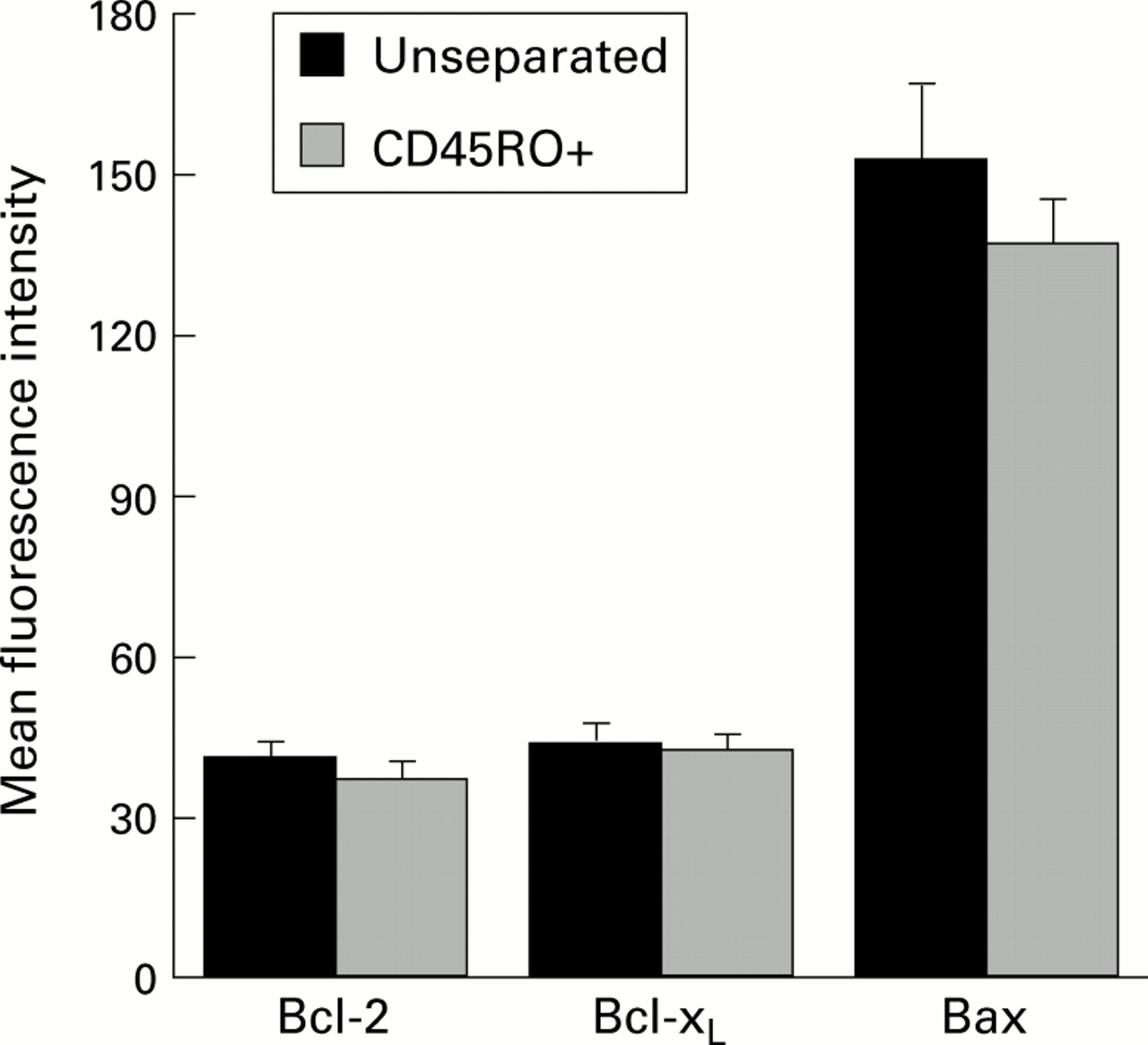
Initially we investigated whether normal T cells from the peripheral circulation and the intestinal mucosa, respectively less and more susceptible to apoptosis, were associated with differential expression of Bcl-2 family proteins. Flow cytometric analysis of PBT and LPT disclosed significant differences in expression levels of Bcl-2 and Bax but not Bcl-xL (fig 1). Levels of Bcl-2 and Bax were significantly higher in control LPT (p<0.001 and p<0.002, respectively) than those found in normal PBT (fig 2). When PBT memory cells (CD45RO+) were compared with autologous unseparated PBT, no differences were observed in levels of Bcl-2 and Bax expression between the two cell populations (fig3).
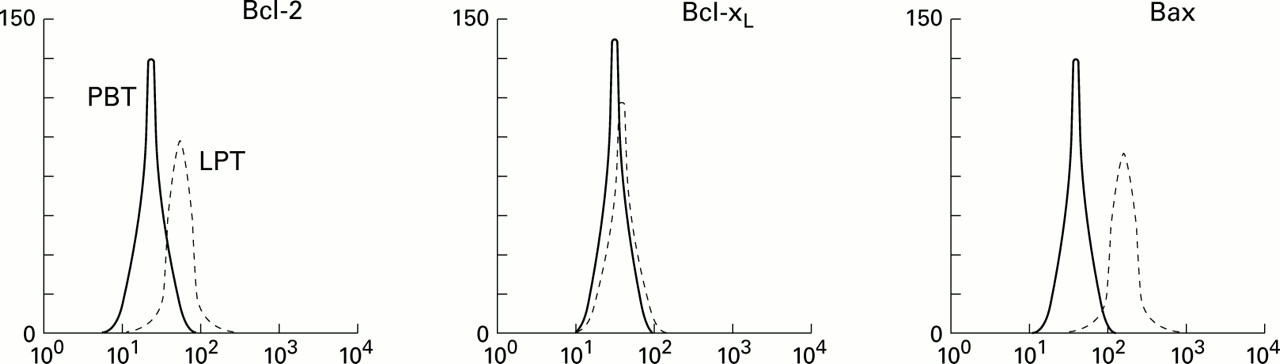
Representative flow cytometric analysis of intracellular staining for Bcl-2, Bcl-xL, and Bax protein levels in normal peripheral blood T cells (PBT) and control lamina propria T cells (LPT).

Flow cytometric analysis of intracellular staining for Bcl-2, Bcl-xL, and Bax protein levels in normal peripheral blood T cells (PBT) and control lamina propria T cells (LPT). Results are mean (SEM) fluorescence intensity for eight PBT and 10 LPT isolates. **p<0.002, ***p<0.001.

Flow cytometric analysis of intracellular staining for Bcl-2, Bcl-xL, and Bax protein levels in normal unseparated and CD45RO enriched (+) peripheral blood T cells (PBT). Results are mean (SEM) fluorescence intensity for eight PBT isolates. No statistically significant differences were observed for Bcl-2, Bcl-xL, and Bax.
IMBALANCE OF Bcl-2 FAMILY PROTEIN EXPRESSION IN CONTROL LPT
Both the type and level of specific Bcl-2 family proteins contribute to death or survival of individual cells. However, what actually dictates the final outcome is a tightly regulated balance of Bcl-2 family proteins.15 ,16 Therefore, to better understand the significance of the results shown in fig 1, we investigated the relative proportion of anti- to proapoptotic protein levels in both PBT and LPT. The Bcl-2/Bax ratio was similar in PBT and LPT (0.34 (0.01) and 0.37 (0.04), respectively; p=0.78) but the Bcl-xL/Bax ratio was significantly lower in LPT than PBT (0.69 (0.04) and 0.76 (0.01), respectively; p<0.001).
In addition, we also investigated whether there was a positive or negative correlation among individual Bcl-2 family proteins in PBT and LPT. In PBT a near perfect and highly significant positive correlation was observed among Bcl-2, Bcl-xL, and Bax (fig 4, top panels). When LPT were evaluated, markedly different results were obtained. In contrast with PBT, LPT did not display any correlation between Bcl-2 and Bax but a very strong and highly significant positive correlation between Bcl-xL and Bax was present in LPT (fig4, bottom panels), similar to that seen in PBT.

Correlation of anti- and proapoptotic Bcl-2 family protein levels in normal peripheral blood T cells (PBT) (top) and control lamina propria T cells (LPT) (bottom). Individual data points represent mean fluorescence intensity of intracellular staining measured by flow cytometric analysis.
DECREASED BAX EXPRESSION IN CD LPT
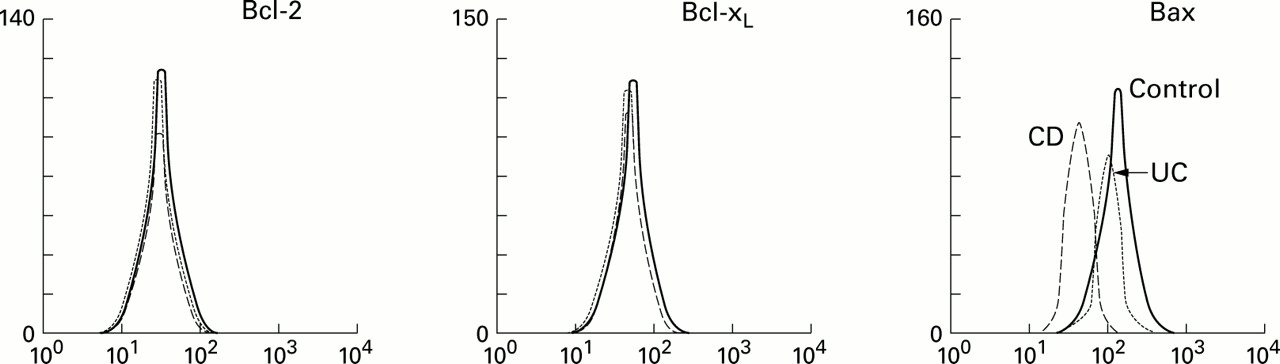
Some reports have demonstrated that mucosal T cells derived from IBD mucosa are less susceptible to apoptosis compared with cells from normal control mucosa.13 ,14 Therefore, we next investigated if the expression level of Bcl-2 family proteins was different among control, CD, and UC LPT. No differences were observed in the LPT level of Bcl-2 and Bcl-xL among control, CD, and UC patients (fig 5). In contrast, CD LPT expressed significantly lower levels of the proapoptotic Bax protein compared with that of both control and UC LPT (p<0.03 for both) (figs 5, 6). These findings were independent of the clinical parameters of the patients.

Representative flow cytometric analysis of intracellular staining for Bcl-2, Bcl-xL, and Bax protein levels in control, Crohn's disease (CD) and ulcerative colitis (UC) lamina propria T cells (LPT).

Flow cytometric analysis of intracellular staining for Bcl-2, Bcl-xL, and Bax protein levels in control, Crohn's disease (CD), and ulcerative colitis (UC) lamina propria T cells (LPT). Results are mean (SEM) fluorescence intensity for 10 control, seven CD, and eight UC isolates. **p<0.003, CD versus control and UC.
INCREASED RATIO OF ANTI- TO PROAPOPTOTIC Bcl-2 FAMILY PROTEIN IN CD LPT
In view of the decreased expression of Bax by CD LPT, an abnormal proportion of anti- to proapoptotic protein levels might be present in this condition. Therefore, we evaluated Bcl-2/Bax and Bcl-xL/Bax ratios in control and IBD LPT. The Bcl-2/Bax ratio was comparable and not significantly different in control, CD, and UC LPT (0.37 (0.04), 0.39 (0.02), and 0.37 (0.03), respectively). In contrast, compared with control LPT (0.32 (0.01)), the Bcl-xL/Bax ratio was significantly higher in CD (0.39 (0.02); p<0.02) but not UC LPT (0.36 (0.02); p=0.13). We also investigated if there was some correlation among the Bcl-2 family proteins of control and IBD LPT. The strong and highly significant positive correlation between Bcl-xL and Bax we found in control LPT (fig 4) was preserved in CD, but not in UC LPT (fig 7). As in control LPT, there was no correlation between Bcl-2 and Bax in CD or UC LPT (data not shown). Because control and CD LPT displayed a similar positive and significant correlation between Bcl-xL and Bax, we directly compared the slope of the correlation curve of these proteins in both groups. The slope of CD LPT was markedly and significantly lower (p=0.011) than that of control LPT (fig 8). These findings were also independent of the clinical parameters of the patients.
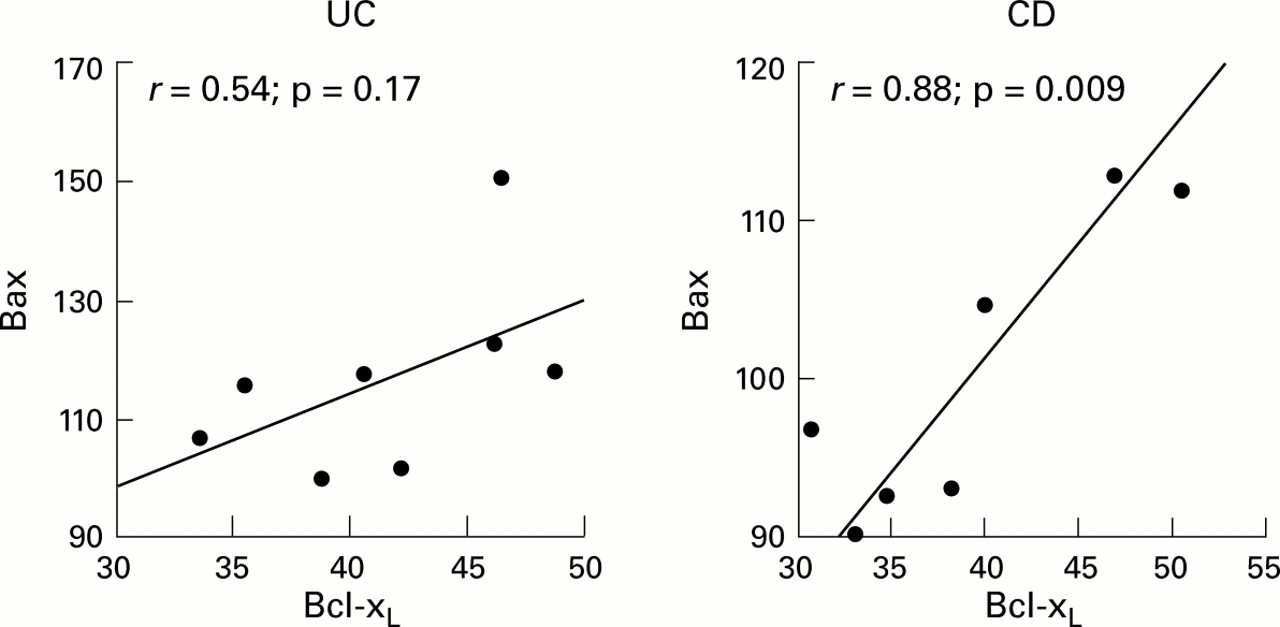
Correlation of proapoptotic Bax and antiapoptotic Bcl-xL protein levels in Crohn's disease (CD) and ulcerative colitis (UC) lamina propria T cells (LPT). Individual data points represent mean fluorescence intensity of intracellular staining measured by flow cytometric analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparative correlation of proapoptotic Bax and antiapoptotic Bcl-xL in control and Crohn's disease (CD) lamina propria T cells (LPT). Individual data points represent mean fluorescence intensity of intracellular staining measured by flow cytometric analysis.
Discussion
To define the status of Bcl-2 family proteins and gain a better understanding of their regulatory influence on the susceptibility of mucosal T cells to apoptosis, we evaluated three distinct parameters: absolute expression levels, ratio of anti- to proapoptotic proteins, and the correlation between them. The same parameters were also evaluated in PBT, where apoptosis is tightly regulated by these proteins.24 In normal PBT, anti- and proapoptotic proteins must be closely co-regulated to achieve an intracellular balance that provides integration of competing signals for prolonged survival.16 LPT are distinct from PBT in several ways, including a dominant CD45RO+ phenotype,25 high activation marker expression, distinct proliferation in response to CD3 and CD2 binding, and different patterns of production of and response to cytokines.26-28 In addition, LPT reside and function in the highly specialised antigen rich microenvironment of the intestinal mucosa.29 Considering all these variables, it is reasonable to expect that the balance of anti- and proapoptotic proteins in LPT differs from that of PBT.
When absolute expression levels of Bcl-2, Bcl-xL, and Bax were measured, some differences became readily apparent as both Bcl-2 and Bax were expressed at significantly higher levels in LPT than PBT. This increase was not simply due to the memory status of LPT as levels of Bcl-2 and Bax in CD45RO+ PBT were comparable with those of unseparated PBT. Because of the increase in Bax expression, the Bcl-xL/Bax ratio was significantly lower in LPT. The decreased ratio was exclusively due to the significantly higher level of Bax expression as there was no significant difference between LPT and PBT with regard to Bcl-xL. The lower Bcl-xL/Bax ratio was compatible with and may contribute to the increased susceptibility of mucosal T cells to cell death, as previously suggested.6 ,30
As the expression level of Bcl-2 family protein is altered during T cell activation and deactivation,31 ,32 another approach to investigate possible changes in inflamed intestine is to assess whether Bcl-2, Bcl-xL, and Bax vary coordinately among themselves. Under physiological circumstances, increasing or decreasing levels of proapoptotic proteins should be accompanied by an opposing increase or decrease in levels of antiapoptotic proteins. This expectation was confirmed by the essentially perfect correlation of Bcl-2 to Bax and Bcl-xL to Bax in PBT. In LPT, in spite of the significantly different ratio of Bcl-xL/Bax, these two proteins were also perfectly correlated as in PBT. In contrast, even though the ratio of Bcl-2/Bax was not significantly different between PBT and LPT, the correlation between these two proteins was lost.
Having defined Bcl-2 protein levels, ratios, and correlation in normal PBT and LPT, we next investigated possible abnormalities of these parameters in IBD LPT. This is important in view of recent reports of decreased susceptibility of mucosal T cells to apoptosis in IBD and particularly in CD.13 ,14 This decrease was supported by our finding of a significantly diminished expression level of the proapoptotic Bax protein in CD compared with both control and UC LPT. Levels of Bcl-2 in both CD and UC cells were similar to those present in control LPT. Boirivant et al also found normal Bcl-2 levels in freshly isolated CD LPT, which increased after culture or stimulation with anti-CD2 antibodies, but levels in UC LPT were not investigated.13 Ina et al quantified expression of Bcl-2 and Bax by lamina propria mononuclear cells in control, CD, and UC mucosa.14Compared with control mucosa, these authors found comparable levels of Bcl-2 in CD and decreased levels in UC, whereas Bax levels were decreased in CD and increased in UC, resulting in a significantly increased Bcl-2/Bax ratio in CD. These observations, although performed in a complex population of mononuclear cells, are in general agreement with the results of the present study. However, as previously pointed out,15 ,16 it is critical to assess multiple Bcl-2 protein levels in a comprehensive fashion as their relative concentrations ultimately decide the death or survival of any given cell. Thus this investigation expanded previous reports by studying purified mucosal T cells, including measurement of Bcl-xL, and correlating Bcl-2, Bcl-xL, and Bax expression levels. When ratios among Bcl-2 proteins were examined in IBD cells, CD LPT displayed a significantly higher Bcl-xL/Bax ratio due to decreased levels of the anti-apoptotic Bax protein. Decreased Bax expression leading to a higher Bcl-xL/Bax ratio however is most likely not the only factor involved in the decreased susceptibility of CD LPT to apoptosis. In fact, we previously reported preserved survival of T cells in UC in spite of decreased Bcl-2 and increased Bax in the mucosa resulting in a significantly lower Bcl-2/Bax ratio.14Nevertheless, these findings provide new molecular insights into some of the possible mechanisms underlying the resistance of mucosal T cells to cell death in CD.
When the relationship among Bcl-2 proteins was assessed in CD and UC LPT, no significant correlation was detected between Bcl-2 and Bax, as found in control cells. As this was true in all LPT regardless of the normal or inflamed condition of the mucosa, the lack of Bcl-2 and Bax correlation may represent a feature intrinsic to all mucosal T cells that differs from PBT, where Bcl-2 and Bax are significantly correlated. In contrast, the positive and significant correlation between Bcl-xL and Bax in control LPT was preserved in CD but lost in UC LPT. This difference between the two forms of IBD may represent a unique phenomenon that cannot simply be attributed to the presence of mucosal inflammation. This suggests that the molecular mechanisms regulating gut T cell death and survival differ in CD and UC, a possibility also supported by elevated Fas ligand expression of mucosal T cells infiltrating UC but not CD lesions.33
Overall, these results show that the correlation patterns of Bcl-2 protein are essentially the same in control and CD LPT. Yet CD LPT are less susceptible to apoptosis than control LPT. To investigate this in greater detail, we directly compared the correlation of Bcl-xL to Bax in control and CD mucosa. In control LPT, increasingly higher levels of Bcl-xL were accompanied by a proportional increase in Bax. In contrast, in CD LPT the increase in Bcl-xL was not accompanied by a proportional increase in Bax. This indicates that the balance of death and survival regulatory proteins in control versus CD cell populations is differently regulated in spite of both displaying significant positive correlations, and may explain the intrinsic resistance of CD mucosal T cell to various apoptotic stimuli.14
In conclusion, compared with control LPT, the combined results of lower Bax levels and the consequent increase in the Bcl-xL/Bax ratio in CD LPT skew the balance of anti- to proapoptotic proteins in favour of resistance to apoptosis in CD. This imbalance may provide, at least in part, an explanation for the resistance of mucosal T cells to cell death in CD. This mechanism may be unique to this condition as UC LPT did not exhibit a similar imbalance even though they derive from a chronically inflamed intestine. Resistance of T cells to apoptotic death may extend their lifespan and retain activated T cells in CD mucosa, resulting in an exceedingly prolonged immune response leading to chronic inflammation.
Acknowledgments
This work was supported by grants from the National Institutes of Health (DK30399 and DK50984 to C Fiocchi; DK54213 and CA77717 to AD Levine). The authors thank the members of the Division of Gastroenterology, Department of Surgery, and Institute of Pathology of University Hospitals of Cleveland. Some tissue samples were provided by the Cooperative Human Tissue Network which is funded by the National Cancer Institute.
Abbreviations used in this paper
- CD
- Crohn's disease
- IBD
- inflammatory bowel disease
- LPT
- lamina propria T cells
- PBT
- peripheral blood T cells
- UC
- ulcerative colitis
References
Linked Articles
- Commentary