Article Text

Abstract
Background: Colonoscopic surveillance for hereditary non-polyposis colorectal cancer (HNPCC) reduces death rates, but early interval cancers still occur, probably due to missed small, aggressive adenomas. Narrow band imaging (NBI), a novel endoscopic technology, highlights superficial mucosal capillaries and improves contrast for adenomas. This study examined whether a second pass with NBI in the proximal colon helped detect additional adenomas in patients with HNPCC.
Methods: 62 patients from HNPCC families (Amsterdam II or genetic criteria) attending for colonoscopic surveillance were examined twice from caecum to sigmoid–descending junction, first with high definition white light and then a second pass with NBI in a back-to-back fashion. All polyps detected were removed for histopathological analysis.
Results: At least one adenoma in the proximal colon was detected during the initial white light pass in 17/62 (27%). NBI detected additional adenomas in 17/62 (27%). 26/62 (42%) patients had at least one adenoma detected after both white light and NBI; absolute difference 15% (95% CI 4–25%), p = 0.004 versus white light alone. The total number of adenomas increased from 25 before NBI to 46 after NBI examination, p<0.001. The proportion of flat adenomas detected in the NBI pass, 9/21 (45%), was higher than in the white light pass, 3/25 (12%), p = 0.03. Including white light examination of the sigmoid and rectum, overall 28/62 (45%) patients had at least one adenoma detected.
Conclusions: Use of NBI in the proximal colon for patients undergoing HNPCC surveillance appears to improve adenoma detection, particularly those with a flat morphology. NBI could help reduce interval cancer rates. ClinicalTrials.gov Identifier:NCT00313755.
Statistics from Altmetric.com
Familial risk predisposition accounts for up to 20% of all colorectal cancers, whilst 2–3% of cancers are specifically due to the autosomal dominantly inherited condition hereditary non-polyposis colorectal cancer (HNPCC) also known as Lynch syndrome.1 This confers an 80–85% lifetime risk of colorectal cancer at a young age, predominantly in the proximal colon, as well as an increased risk of other associated cancers of the small bowel, renal pelvis and ureter, endometrium and brain.1 2
International guidelines recommend colonoscopic surveillance for patients who meet clinical or genetic criteria for HNPCC every 1–2 years starting from 25 years of age.3 4 Colonoscopic surveillance in HNPCC has been shown in case–control and cohort studies to reduce the risk of death from colorectal cancer by up to 70%; however, some of the deaths prevented represent early detection of colorectal cancer at a curative stage rather than prevention through polypectomy.2 5 6 Colonic adenomas appear to have an accelerated progression to carcinoma in HNPCC, perhaps in as little as 2 years.7 Some studies suggest that adenomas in HNPCC patients are found more commonly in the proximal colon and that they are often advanced, containing high-grade dysplasia, despite their small size.8 It seems likely that some cancers are developing during surveillance due to missing small, early, but aggressive adenomas; therefore, comprehensive detection is critical.
In a recent systematic review of published back-to-back colonoscopy studies, colonoscopy had a miss rate for adenomas of all sizes of 22% (95% CI 15% to 32%).9 Pan-colonic chromoendoscopy “dye-spray” has been shown to improve the detection of polyps, particularly small or flat adenomas in the right colon, in randomised studies.10–13 Two recent studies performing back-to-back colonoscopy in patients with HNPCC, with pan-colonic chromoendoscopy during the second pass, both showed a significant increase in the number of adenomas, including flat adenomas, detected with the addition of chromoendoscopy14 15; however, it is time consuming, requires extra training and equipment, and is not widely practised by Western endoscopists.
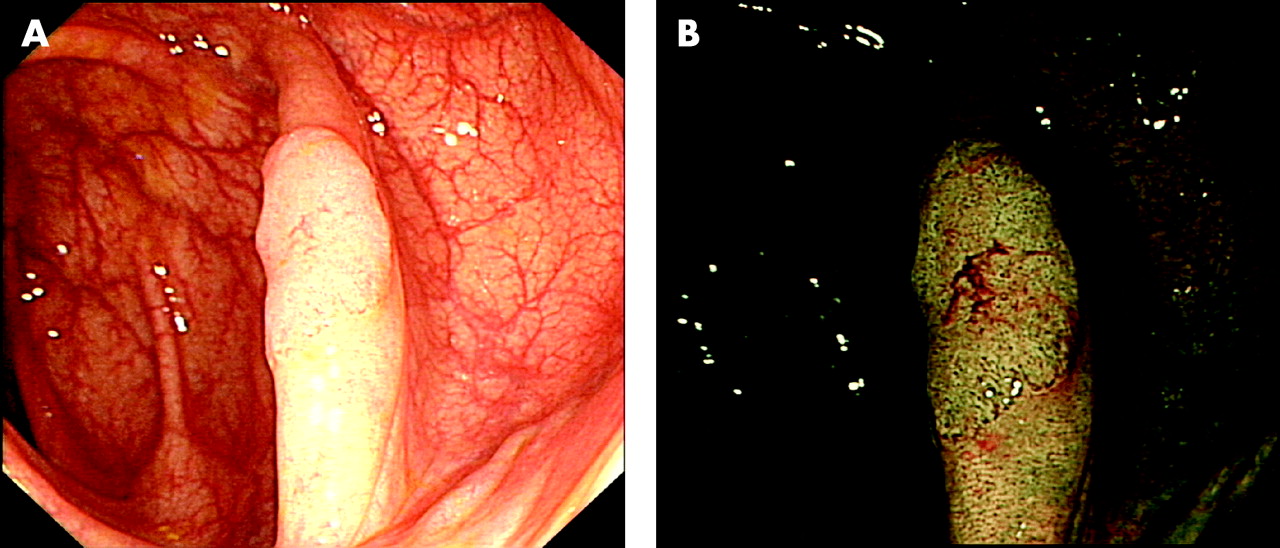
Narrow band imaging (NBI) is a novel endoscopic technology sometimes described as “electronic chromoendoscopy”. It uses optical filters in the light source to highlight superficial capillaries in the mucosa at the press of a button16; with NBI, epithelial neoplasia, which has an increased microvascular density compared with normal mucosa, stands out as brown-black areas against the blue-green background (fig 1).17 18 NBI has been used to help detect and define early dysplastic change at endoscopy in the oesophagus, stomach, colon, oropharynx, bronchus and bladder.18–23 It can produce images similar to those of chromoendoscopy, and may help improve adenoma detection at colonoscopy with a standard, “wide field” view in patients at high risk of further adenomas.24
This study aimed to see whether a second pass with NBI in the proximal colon after meticulous white light examination could increase adenoma detection of patients undergoing surveillance colonoscopy for HNPCC.
METHODS
Study population
Consecutive at-risk members of HNPCC families (Amsterdam II criteria or known genetic alteration) attending for colonoscopic surveillance for HNPCC between April and November 2006 were identified from the St Mark’s Hospital Cancer Research UK Family Cancer Clinic database and offered participation in the trial.25 These patients are currently offered colonoscopic screening every 2 years at our institution. All patients gave written informed consent, and the study was approved by the local research ethics committee. The flow of patients through the study is outlined in fig 2.

{kind=link}
{kind=link}
Study procedures
Preparation was with 24 h of dietary restriction followed by two sachets of magnesium citrate (Citramag; Sanochemia Diagnostics UK Ltd, Bristol, UK) and senna 13 g by weight for bowel cleansing. Patients were given the option of sedation with a combination of intravenous midazolam and pethidine (meperidine). All patients received intravenous antispasmodic, either hyoscine butylbromide (Buscopan®; Boehringer Ingelheim, Bracknell, UK) or glucagon (GlucaGen® HypoKit; Novo Nordisk, Crawley, UK). We used high definition (HDTV) colonoscopes and a third-generation prototype NBI system (XCF-H240FZL/I and CF-H260AZL video colonoscopes, XCLV-260HP xenon light source and XCV-260HP video system centre; Olympus, Japan). The NBI system used sequential illumination with standard red, green and blue filters in the light source reflected to a monochrome high definition charge-coupled device to produce the high definition white light image. NBI was with blue and green filters only which had narrowed spectral bandwidths centred on 415 nm (bandwidth 30 nm) and 540 nm (bandwidth 20 nm), respectively. Patients were excluded if the caecum could not be reached within 20 min (classified as technically difficult) or if the bowel preparation was poor (>10% of the mucosa obscured by solid stool after suctioning).
Once the caecum (or neo-terminal ileum) was reached and identified, patients were examined from caecum to sigmoid–descending junction (defined by the endoscopist, and at approximately 35 cm on withdrawal) initially with high definition white light. Once a polyp was detected, its morphology was classified according to the Japanese Research Society for Cancer (JRSC) of the Colon and Rectum; size was measured using biopsy forceps, colonic segmental location was recorded and the polyp was resected and sent for histopathological analysis.26 An experienced gastrointestinal pathologist reviewed all lesions. Once the sigmoid–descending junction was reached, the caecum was re-intubated and the NBI function was activated by pressing a button on the endoscope control head. The area from caecum to sigmoid–descending junction was re-examined using NBI, and any additional polyps found were assessed and resected as above. Although in the original trial protocol (ClinicalTrials.gov Identifier:NCT00313755) the use of magnification was permitted to examine lesions detected with NBI before the decision to resect, in practice this was almost never used, and all detected lesions using a wide field view with either white light or NBI were resected. Finally, the segment from sigmoid–descending junction to anal verge was examined using high definition white light alone. In the rectum/recto-sigmoid segment, if a lesion was small (⩽5 mm) and macroscopically clearly hyperplastic, it could be left in situ and was not recorded, at the endoscopist’s discretion, in line with our normal clinical practice. Retroflexion was routinely employed in the rectum.27 Intubation and extubation times were recorded.
Meticulous attention was paid to slow, careful examination, suctioning fluid pools, re-examining flexures, pressing down folds and using appropriate changes of patient position to improve luminal distension during each pass, to maximise adenoma detection.28–31 The minimum withdrawal time for each pass from caecum to sigmoid–descending junction was 6 min, in line with international guidelines.4 Examinations were performed by three endoscopists (B.P.S., N.S. and J.E.E.), all of whom had experience of >1000 colonoscopies and >100 using NBI; however, the majority of the colonoscopies (>90%) were performed by one endoscopist (J.E.E.).
Statistics and outcome measures
The primary outcome measure was the number of patients with at least one adenoma after white light endoscopy compared with the number of patients with at least one adenoma after white light and NBI in the proximal colon, defined as the colon proximal to the sigmoid–descending junction.32 From the two trials of chromoendoscopy in HNPCC, 9–28% of participants had at least one adenoma before chromoendoscopy. For a power (1–β) of 80% to detect a 100% increase in the number of patients with at least one adenoma using the more conservative adenoma prevalence estimate of 9% with a significance level (α) of 5%, at least 60 patients needed to be recruited. Predefined secondary outcome measures comparing white light and NBI were: total number of lesions detected; number of advanced neoplasms detected (defined as any of: high grade dysplasia or carcinoma; >20% villous elements; size ⩾10 mm); number of flat (width >twice the height) and depressed lesions (JRSC class II) detected; and number of hyperplastic polyps detected. Proportions were compared with the paired exact test and Fisher exact test; continuous variables were compared with Wilcoxon matched-pairs and Mann–Whitney tests for paired and non-paired data, respectively.
RESULTS
Sixty-two patients were recruited and completed the study with a full data set. Their demographics are described in table 1. Intubation and extubation times are summarised in table 2.
The number of patients with at least one adenoma detected in the proximal colon, the primary outcome measure, rose from 17/62 (27%) before NBI to 26/62 (42%) after a second pass with NBI, absolute difference 15% (95% CI 4% to 25%), p = 0.004; 17/62 (27%) patients had at least one additional adenoma detected during the NBI pass. The total number of adenomas detected in the proximal colon rose from 25 before NBI to 46 after NBI, p<0.001. Only one advanced adenoma was detected, size 10 mm, flat (IIa) morphology, found during NBI examination. No lesions with high grade dysplasia or >20% villous architecture were detected. Nine of 21 (45%) adenomas detected during the NBI pass were flat lesions (JRSC II) compared with three of 25 (12%) seen during the initial white light pass, p = 0.03 (table 3).
Median adenoma size in the white light pass was 3 mm (1.5–6 mm) and in the NBI pass 2 mm (1–10 mm), p = 0.23. On a per patient basis, the number of patients with at least one hyperplasic polyp detected increased from 24% to 37%, absolute difference 13% (95% CI 3% to 23%), p = 0.008. The total number of hyperplastic polyps in the proximal colon detected was 23 after white light alone and 43 after white light and NBI, p<0.001, median size 3 mm (1–15 mm). Eleven of these measured 6–9 mm and three measured ⩾10 mm. Including other lesions identified as polyps, such as lymphoid follicles, inflammatory polyps and normal mucosa, the total number of polyps detected in the proximal colon was 58 after white light, and 110 after white light and NBI, p<0.001. The overall proportion of flat polyps detected with white light was 13/58 (22%), and 21/52 (40%) with NBI, p = 0.06.
Eight adenomas were detected in the distal colon and rectum (from sigmoid–descending junction to anal verge) in five patients, median size 4 mm (2–7 mm); none had a flat morphology or advanced histology. The final adenoma prevalence with high definition (HDTV) white light alone (white light initial pass plus white light examination of the distal colon and rectum) was 20/62 (32%). The final prevalence for pan-colonic white light examination plus the second NBI pass in the proximal colon was 28/62 (45%). The total number of adenomas detected was 54 in 62 patients for a mean adenoma detection rate of 0.87 per patient. We examined whether there was an association between patients with at least one hyperplastic polyp and patients with at least one adenoma in the whole colon after both white light and NBI examination (table 4). Of patients who had a hyperplastic polyp, 13/24 (54%) had an adenoma, compared with 15/38 (39%) of those who did not have a hyperplastic polyp. The Phi coefficient of association was 0.14, p = 0.30, indicating no or minimal association between the presence of hyperplastic polyps and adenomas in our patient cohort.
DISCUSSION
This study, the largest by 2-fold to examine the use of a technique to improve adenoma detection in HNPCC, indicates that a second pass with NBI in the proximal colon almost doubles the total number of adenomas detected and increases the proportion of patients with at least one adenoma detected by 50%. Assuming that interval cancers arise from missed adenomas, this new and easily applied technology has the potential to improve the effectiveness of HNPCC surveillance significantly in terms of cancer prevention. The proportion of flat adenomas detected during the NBI pass was higher than in the initial white light pass, suggesting that a different, additional population of adenomas is being detected, whose morphology makes them difficult to detect with white light alone. The ability of NBI to improve contrast for adenomas by highlighting increases in microvascular density is consistent with this observation. This improvement in detection may have implications for surveillance of other high risk groups such as those who have had multiple adenomas or a previous colorectal cancer. Early data from a randomised study involving such patient groups is encouraging24; however, results from other randomised studies in lower risk groups have not shown benefit.33 The use of a very sensitive technique to detect small and flat adenomas more comprehensively might also help with screening for colorectal cancer by allowing better risk stratification based on numbers of adenomas, as well as a more complete “clearing colonoscopy”. Adenoma-negative patients, having undergone screening by NBI, may be able to extend surveillance intervals safely, reducing cost and inconvenience. NBI might therefore increase the efficiency and effectiveness of colonoscopy-based National Bowel Cancer Screening Programmes in younger patients to reduce colorectal cancer incidence. Whether NBI is helpful in faecal occult blood test-based screening programmes, which have been initiated recently in the UK for patients aged 60–69, where large polyps and early cancers are the primary lesions of interest, remains to be seen. Diminutive adenoma detection in an older average risk population may have less biological relevance. Interestingly, chromoendoscopy has recently been shown to increase adenoma detection during flexible sigmoidoscopy screening, and therefore there might be a role for NBI as “electronic chromoendoscopy” in a hybrid faecal occult blood test–flexible sigmoidoscopy-based bowel cancer screening programme that has been proposed as the most cost-effective model for the UK.34 35
Our results with NBI are similar to those seen in two back-to-back studies which used pan-colonic chromoendoscopy in HNPCC, where a greater number of adenomas and flat lesions were seen after the use of dye-spray.14 15 Combining the results of these two chromoendoscopy studies, one screening (initial colonoscopy) and one surveillance (follow-up colonoscopy), gives a total of 61 adenomas detected in 58 patients, for an overall mean adenoma detection rate of 1.05 per patient, compared with 0.87 in our NBI study14 15; however, most of the adenomas detected were found in the screening study when a previous “clearing” colonoscopy had not been performed in the majority of patients.14 All patients in our study had undergone at least one high-quality “clearing” colonoscopy. The overall mean adenoma detection rate in the chromoscopic surveillance study was 0.55 per patient, less than in our study.15 The proportion of flat adenomas, 22% (12/52) overall, is also similar to that seen in the chromoscopic surveillance study (ie, 24%) but was slightly less than the 32% seen in a large study of unselected patients from the UK.15 36 The additional proximal adenomas detected with NBI came at the cost and small added risk of performing polypectomy on more non-adenomatous polyps. Over one additional polypectomy was performed for each adenoma removed; but no complications were reported and the risk of removing small polyps is very low.37 The proportion of neoplastic to non-neoplastic polyps removed was similar in the white light and NBI passes. A similar phenomenon of overdetection of non-neoplastic lesions is seen in chromoendoscopy studies. When combined with high magnification “zoom” endoscopes, NBI can rapidly and accurately predict whether polyps are neoplastic or non-neoplastic using the Kudo pit pattern or measures of microvascular density, “meshed brown capillary vessels” or “vascular pattern intensity”.18 38–40 Some of the polypectomies might have been avoided if these techniques had been used to provide in vivo “endohistology”; however, as part of the study protocol, all polyps detected were resected regardless of macroscopic appearance or endoscopist assessment of neoplastic potential. The three back-to-back studies (two chromoendoscopic and our study with NBI) which have used techniques to improve adenoma detection indicate that there is a very substantial adenoma miss rate at conventional colonoscopy for HNPCC.14 15 Combined with the data regarding interval cancers during colonoscopic surveillance it would seem difficult to justify future surveillance without using a technique to enhance adenoma detection.2 5 6
The time taken to perform pan-colonic chromoendoscopy in the two back-to-back studies was 14–17 min, compared with 7 min for NBI in our study, although we did not examine the recto-sigmoid with NBI. Our time for NBI examination, which was approximately 30 s longer than the initial white light pass, may reflect the fact that with NBI, as with chromoendoscopy, even minor failings in bowel preparation make comprehensive detection more difficult. Residual stool and mucus appear brick red and blood black, respectively, needing extra washing and suction. This is despite the initial pass with white light which should have removed the majority of poorly prepared areas but may have led to blood in the endoscopic field from polypectomy. A recent study has emphasised the need to take at least 6 min during colonoscope withdrawal to ensure a high quality, meticulous examination30; however, additional time beyond this for techniques which might increase adenoma detection effectiveness must be balanced against the need for colonoscopic efficiency given the very high demand for colonoscopy resources. Chromoendoscopy is felt to be too time consuming to be practical in routine clinical practice.41 Use of NBI may maximise effectiveness of adenoma detection whilst maintaining examination efficiency.
As a back-to-back study, the increase in adenomas seen during the NBI pass may be due to just looking again, and a similar result might have been seen with a white light second pass. Against this interpretation are a number of factors. First, the number of adenomas not detected—that is, the “miss rate”, during the first white light pass (ie, 21/46 (46%)), substantially exceeds the 95% CI for summary miss rates in back-to-back studies (15–32%), suggesting that at least some of the adenomas would not have been detected with a second look with white light.9 Secondly, the proportion of flat adenomas detected during the NBI pass was significantly higher than in the initial white light pass, implying that the improved contrast produced by the use of the NBI system is required for detection of additional flat lesions. It is possible that the initial white light examination was inadequate, leaving missed adenomas to be found on the second pass regardless of use of NBI. Compared with other studies looking at white light adenoma detection rates in HNPCC screening and surveillance, our overall white light adenoma prevalence rate of 32% exceeds the range of 14.5–30% reported in the literature.14 15 The results for adenoma detection in our study using white light alone, compared with the result for the same patient group at their previous colonoscopy, are almost identical (at least one adenoma detected, 20 vs 22, p = 0.81; total adenomas detected 33 vs 34, p = 0.92). The number of patients with at least one adenoma with white light exceeded that of a previous study of colonoscopic surveillance at HNPCC at our institution published in 1995 (20/62 (32.2%) vs 34/127 (26.8%), p = 0.49).42 This is consistent with a high quality initial white light examination; although it suggests that high definition white light examination has not substantially improved adenoma detection compared with standard definition colonoscopy in our patient cohort with HNPCC looking at historical data over the short or medium term. A further weakness of the study relates to the fact that the majority of colonoscopies were performed by only one of the three endoscopists. It is not possible therefore to conclude that each of the endoscopists had improved adenoma detection using NBI; however, no randomised study comparing white light with NBI for adenoma detection has reported a significant decrease in numbers of patients with at least one adenoma detected, with three of four studies reporting increases of between one-third and one-eighth with NBI, although these are only reported in abstract form at present.24 43 44 The method used in this study of complete back-to-back examination of the proximal colon meant that two patients (3%) were excluded due to a technically difficult insertion, although re-intubation was rapid and simple for the remainder. Colonoscopists in clinical practice might instead re-examine short segments of colon with each modality to ensure a difficult to achieve position in the right colon was not lost.
Our HNPCC study population was defined predominantly using clinical (Amsterdam II) criteria, only 13% of whom had a confirmed DNA mismatch repair gene mutation, with a further 17% having a relative with a known mismatch repair gene mutation. If the analysis is restricted to only those who had a confirmed personal mismatch repair gene mutation (n = 7), two of seven (29%) patients had at least one adenoma detected after white light examination, with three of seven (43%) having at least one adenoma after both white light and NBI examination. A total of four adenomas were detected after white light compared with a total of 10 after white light and NBI. Although this group is too small to analyse statistically, it suggests that the results seen in the entire clinically defined cohort are representative of the effect seen when only those with a definite gene mutation are considered.
The reported distribution of adenomas throughout the colon in HNPCC is variable throughout the literature, with some sources citing a left-sided or relatively even distribution, and others suggesting a right-sided preponderance.2 8 14 15 Our data using white light alone suggest a right-sided distribution, with eight (24%) adenomas distal to the sigmoid–descending junction versus 25 (76%) proximal in a surveillance population. The larger number of right-sided adenomas is consistent with the right-sided distribution of 7:3 of colorectal cancer in HNPCC.1 The ability of NBI to increase detection of adenomas at the hepatic and splenic flexures, areas known to be high risk for polyp or cancer misses at colonoscopy, appeared less than at other sites, although absolute numbers were small. This may relate to difficulties keeping close to the mucosal surface as the flexure is traversed, which is needed with NBI as the image is somewhat darker than with white light.
Some studies have reported a high proportion of small but aggressive adenomas in HNPCC, particularly in the proximal colon. In our sample of 54 adenomas, none contained high grade dysplasia or >20% villous elements. This may reflect the effectiveness of intensive modern video colonoscopic surveillance, as results similar to ours were seen in a recent trial of chromoendoscopy-enhanced surveillance.15 An alternative explanation is that the surveillance intervals in current guidelines are so short that no advanced lesions could develop; however, the high adenoma detection rate reported in this study and the potential for small lesions to develop rapidly into advanced lesions and thence to carcinomas would suggest that current surveillance intervals should remain unchanged. The total number of hyperplastic polyps after a second pass with NBI was significantly increased compared with after white light alone. NBI detected an additional three intermediate (6–9 mm) polyps and two large polyps (⩾10 mm). Hyperplastic polyps, particularly larger ones, have been proposed as part of an alternative “serrated” pathway to colorectal cancer although their biological role is, as yet, not entirely clear.45 The mechanism by which carcinomas with extensive microsatellite instability (MSI-high) occur may be different in HNPCC compared with sporadic MSI-high carcinomas. Sporadic MSI-high carcinomas have a high incidence of BRAF mutations, which are not seen in HNPCC carcinomas, but are seen in sporadic sessile serrated adenomas which are now thought to be a preneoplastic lesion.46 In our study, there was no association between the presence of hyperplastic polyps and the presence of adenomas, suggesting that hyperplastic polyps are not risk markers in HNPCC, although an association has been seen in other studies not using advanced imaging techniques.47
In summary, in this prospective study assessing the new technique of NBI to enhance adenoma detection, we found that a second, additional examination of the proximal colon with NBI almost doubled the total number of adenomas detected. These results for adenoma detection are comparable with those of studies using chromoendoscopy, but took half the examination time when using NBI. These results lead us to conclude that when available, NBI examination at colonoscopy will become the new the standard of care for HNPCC cancer prevention.
Acknowledgments
The authors would like to thank: Nicky Palmer, Wolfson Unit for Endoscopy, and Maggie Stevens, Family Cancer Clinic, for assistance with finding and booking patients and data collection; Carole Cummings, Family Cancer Clinic, for help interrogating and interpreting the Family Cancer Clinic database; Paul Bassett, Statsconsultancy, UK, for statistical advice; John Northover and Joan Slack who established the Family Cancer Clinic; Olympus Keymed, UK and Olympus Medical Systems Corp., Japan for the loan of the prototype narrow band imaging system; and finally the individuals and families who participated in this study.
REFERENCES
Footnotes
Funding: Data from this study have been presented as an oral presentation at the Royal Society of Medicine, Section of Coloproctology, Short Papers Meeting, February 2007, the British Society of Gastroenterology Conference, Glasgow, March 2007, Gut 2007;56(Suppl II):A14, and at Digestive Diseases Week, Washington DC, May 2007, Gastrointest Endosc 2007;65:AB126.
Competing interests: None.