Article Text

Abstract
Objective: Colonoscopy is the accepted gold standard for screening of neoplastic colorectal lesions, but the substantial miss rate remains a challenge. Computed virtual chromoendoscopy with the Fujinon intelligent colour enhancement (FICE) system is a new dyeless imaging technique that might allow higher rates of adenoma detection.
Methods: This is a prospective randomised five tertiary care centre trial of colonoscopy in the FICE mode versus standard colonoscopy with targeted indigocarmine chromoscopy (control group) in consecutive patients attending for routine colonoscopy. Histopathology of detected lesions was confirmed by evaluation of endoscopic resection or biopsy specimens.
Results: 871 patients were enrolled, and 764 patients (344 female, mean age 64 years) were subjected to final analysis (368 in the FICE group, 396 in the control group). In total, 236 adenomas (mean of 0.64 per case) were detected in the FICE group and 271 adenomas (mean of 0.68 per case) in the control group (p = 0.92). There was no statistically significant difference in the percentage of patients with ⩾1 adenoma between the control group (35.4%) and the FICE group (35.6%) (p = 1.0). For the differential diagnosis of adenomas and non-neoplastic polyps, the sensitivity of FICE (92.7%) was comparable with that of indigocarmine (90.4%) (p = 0.44).
Conclusions: At colonoscopy, adenoma detection rates are not improved by virtual chromoendoscopy with the FICE system compared with white light endoscopy with targeted indigocarmine spraying. However, FICE can effectively substitute for chromoscopy concerning the differentiation of neoplastic and non-neoplastic lesions.
Statistics from Altmetric.com
Colonoscopy is considered the gold standard for screening for colorectal neoplasias. Detection of adenomas at colonoscopy is of utmost importance since endoscopic resection of these neoplastic lesions has been shown to prevent colorectal cancer effectively.1 In order to avoid unnecessary polypectomies of non-neoplastic lesions, differentiation between neoplastic and non-neoplastic polyps at colonoscopy is crucial.
Unfortunately, at standard colonoscopy, classification of lesions is often difficult and a substantial percentage of adenomas are missed during the procedure. According to several reports, 10 and 15% of lesions remain undiagnosed at colonoscopy, even by experienced practitioners.2–5 Potential explanations for failure at colonoscopy include poor bowel preparation or inadequately short withdrawal times.6 7 Moreover, an important technical factor that determines the detection of lesions is the level of mucosal contrast provided by the imaging method. Low contrast might contribute to the miss rate of small and flat lesions that show only subtle changes in mucosal topography, such as loss of vascular net pattern, focal pallor and marginal irregularity.8 9
Consequently, auxiliary techniques that enhance mucosal contrast might improve the adenoma detection rate and optimise the potential of colonoscopy for the prevention of colorectal cancer. In this context, conventional chromoscopy with indigocarmine was proposed for enhancement of the mucosal surface. The chromoscopic methods are variable. Some authors have used targeted chromoscopy only for detection of subtle mucosal irregularity diagnosed by conventional colonoscopy10–12; others have advocated total colonic chromoscopy.13–15 While a comprehensive body of literature demonstrates improvement of pit pattern classification,16–21 less consistent results have been reported for improvement of detection rates by randomised controlled studies.13–15 22 Some studies indicate that chromoendoscopy might increase detection rates of small and flat adenomas in diagnostic colonoscopies,13–15 and one trial suggested that pan-colonic chromoscopy is superior to targeted chromoscopy.14 However, others did not find any overall difference in the adenoma yield achieved by chromoendoscopy.13 22 In addition, staining of the entire colon during colonoscopy requires extra training, is labour intensive and time consuming, and is therefore unsuitable for routine application.
Virtual chromoendoscopy imaging with the “Fujinon intelligent colour enhancement” system (FICE)23 or “narrow-band imaging” (NBI)24 is a novel optical approach to enhance mucosal contrast. Both techniques narrow the bandwidth of light components, resulting in dyeless contrast enhancement of mucosal and vascular details. While the NBI system depends on optical filters within the light source, FICE is based on a computed spectral estimation technology that arithmetically processes the reflected photons to reconstitute virtual images for a choice of different wavelengths. Due to its variable setting functions (up to 10) it is possible to select flexibly the most suitable wavelengths required for examination.
Based on technical considerations, it is conceivable that advanced virtual imaging techniques might highlight adenomas during colonoscopy and may even be superior to conventional chromoendoscopy in some aspects: it might (1) reduce procedural time and (2) facilitate lesion assessment by allowing the endoscopist to alternate between conventional and virtual images with just a single touch of an operative button on the grip of the scope.
Indeed, several pilot studies indicate that NBI might be useful for classification of colorectal lesions,19–21 25 but three recent single-centre trials failed to demonstrate improvement of adenoma detection rates.26–28 Preliminary studies on FICE suggest that it may improve detection of early neoplasias in the oesophagus,29 but its utility for identification of adenomas has not been investigated.
The present study investigated the value of the FICE system for detection and classification of colonic polyps and compared its performance with that of standard colonoscopy with targeted indigocarmine chromoendoscopy. It represents the first prospective randomised multicentre trial on the value of virtual chromoscopic imaging techniques.
MATERIALS AND METHODS
Patients
During a 12 month study period, consecutive patients presenting to the five study centres were recruited, as permitted by the availability of the study colonoscopists and the study instrument. Patients were eligible for study inclusion if they were aged 45 years or older and presented for screening or diagnostic colonoscopy for a variety of reasons (table 1). Patients with known inflammatory bowel disease, overt bleeding, polyposis syndrome, previous surgical resection of the colon and patients receiving anticoagulant medication were excluded from the study. All patients gave informed consent before participating in the study. The study protocol was approved by the clinical research ethics committee of the General Ethical Council of the state of Hessen (Germany) (no. 39/2006) and conformed to good clinical practice.
Endoscopic procedure
All examinations were performed with high-resolution zoom endoscopes (EG 590 ZW, Fujinon, Saitama, Japan). However, the zoom function of the device was not utilised for this study. The system was equipped with the EPX 4400 processor (Fujinon) that provides the FICE technology. Colonoscopies were performed by 15 experienced endoscopists in five medical centres. Endoscopists were required to have carried out at least five examinations with FICE in order to become acquainted with the FICE imaging. Based on preliminary experience of the participating endoscopists, FICE set D was favoured over other FICE sets for application in the colon and was therefore exclusively used in this study.
Before the procedure started, patients were randomly assigned to conventional colonoscopy with targeted indigocarmine spraying (control group) or FICE imaging.
Group allocation of patients was performed by dedicated nurses using standard randomisation lists. These lists contained consecutive patient numbers and each number was linked to allocation to one of the two study arms (FICE or control group). Randomisation lists were not accessible to the endoscopists. After randomisation, the colonoscope was inserted into the caecum using white light. At each procedure, the quality of bowel preparation was rated by the endoscopist as excellent (clean and empty), good (clear fluids), moderate (brown fluid), bad (semisolid stool) or very bad (solid stool) according to Ell et al.30 Patients with bad or very bad preparation were excluded from final analysis. Assessment of the colon to search for lesions was systematically performed only during withdrawal of the instrument with a minimum diagnostic extubation time that was set at 6 min.6 Special care was taken to wash and clean the entire colon during instrument introduction and withdrawal, in order to provide optimal conditions. Patients randomised to the control group underwent withdrawal with conventional colonoscopy in the white light mode and particular attention was paid to subtle mucosal signs such as the presence of erythema, focal pallor, absence of a vascular network pattern and discrete mucosal unevenness. In the case of a positive finding, selective chromoscopy (application of 2–5 ml of indigocarmine by a spraying catheter inserted in the working channel of the colonoscope followed by a 10 ml air “push”) was performed for further assessment of the lesion. In the FICE group, withdrawal was performed with activated FICE set D (corresponding to R 500 nm, G 480 nm and B 420 nm). Switching back to conventional imaging was allowed at the discretion of the endoscopist only for polypectomies. Any other occasion and the reason for switching back to white light were documented in the FICE group.
In both groups, lesion morphology according to the Paris classification, size (estimated by the endoscopist) and anatomical location were documented during withdrawal. Importantly, the histology of the detected lesion was predicted and documented by the endoscopist.
At conventional chromoendoscopy with indigocarmine, the mucosal crypt pattern of each lesion was determined according to the classification of Kudo and co-workers (with pit patterns I and II defining non-neoplastic and pit patterns III–V neoplastic lesions). The FICE mode enhances both the pit pattern and vascular pattern, and therefore prediction of histology was based on the Kudo classification18 as well as on the vascular pattern intensity. Hyperplastic polyps were suspected when the surface showed a pale colour with only minute thin superficial (couperose-like) vessels and absence of a ceribriform pit pattern. In contrast to non-neoplastic lesions, adenomas are hypervascular. FICE emphasises the capillary network, which can be appreciated as a darkening of the mucosal pattern, or as a fine meshwork of brown/bluish vessels. Therefore, adenomas were suspected if increased vascular density and pit patterns III–V were enhanced by FICE. An example of an adenoma imaged with white light, FICE and indigocarmine is shown in fig 1. Predicted histopathology was confirmed by evaluation of endoscopic resection or biopsy specimens. An important feature of the study design is that rectal lesions were excluded from study assessment since high numbers of small hyperplastic rectal polyps are common, and complete sampling of these lesions for histological assessment might not be feasible and might confound the study results.

The primary outcome parameter of the study was the total number of adenomas detected in each arm of the study. Assuming a prevalence of 30% of adenoma-bearing patients with an average of two adenomas, and an increase of 15% with FICE, 240 subjects were required in each arm of the study (80% power; significance level of 0.05). Secondary outcome measures included the number of patients with adenomas, accuracy of histological prediction of lesions and withdrawal times for each technique.
Statistical analysis
Wilcoxon rank sum tests with continuity correction were performed to compare the two groups for differences in the number of adenomas per subject. Fishers exact tests and Welch two-sample t tests were performed as indicated. For indigocarmine spraying and FICE imaging, sensitivities, specificities, and positive and negative predictive values for the diagnosis of colorectal lesions were evaluated by comparing the endoscopic diagnosis with final histopathological diagnoses. The GEE package31 of the statistical analysis software R was used to determine the confidence interval of sensitivity and specificity from multiple observations per patient. The logit of a rate (sensitivity or specificity) is the intercept of a logistic model with the investigator’s finding as response and without predictors. Applying a GEE model instead of logistic regression takes into account the correlation in the data. The standard error of the intercept yields a confidence interval of the logit which is transformed to a confidence interval of the rate.
RESULTS
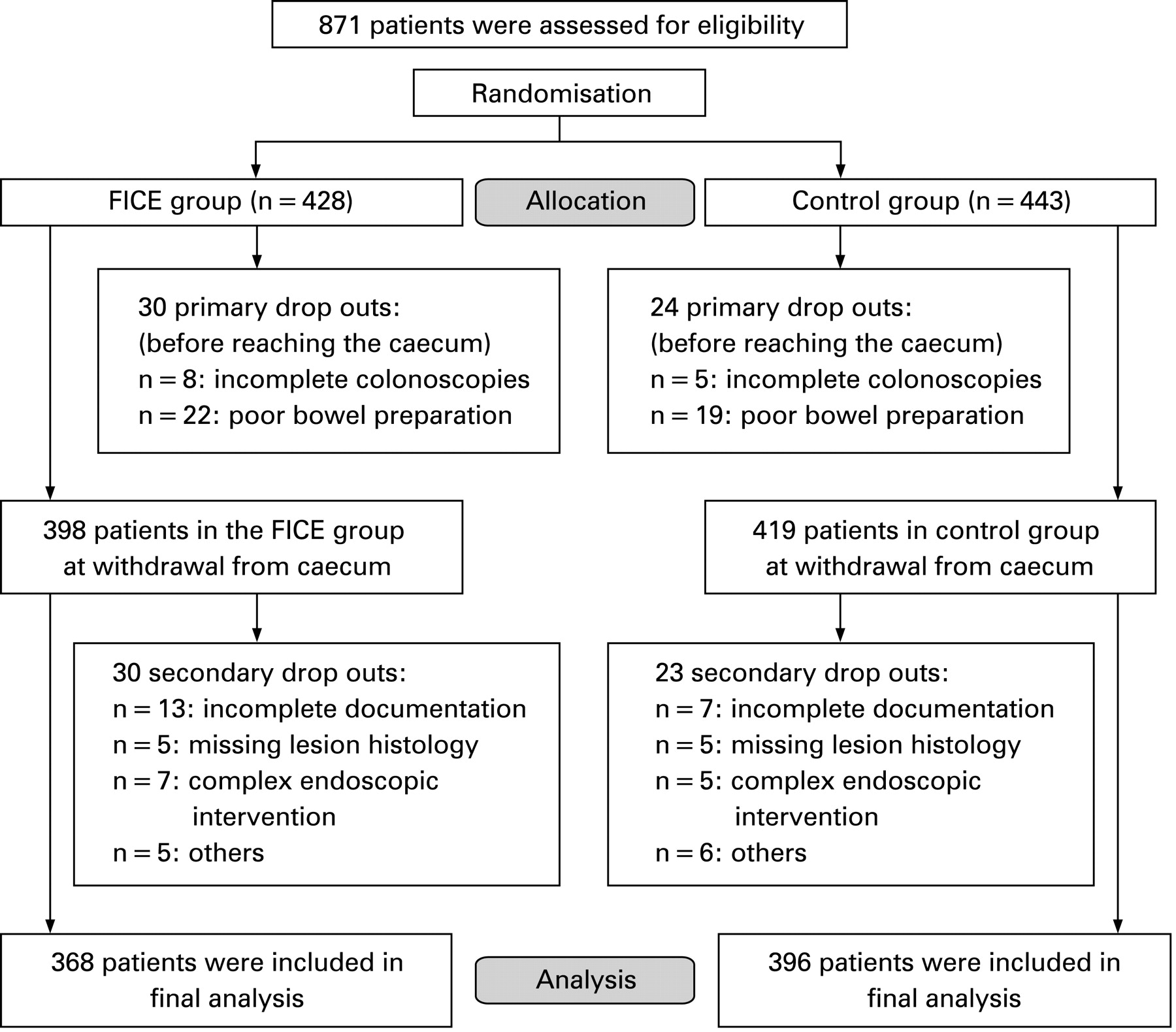
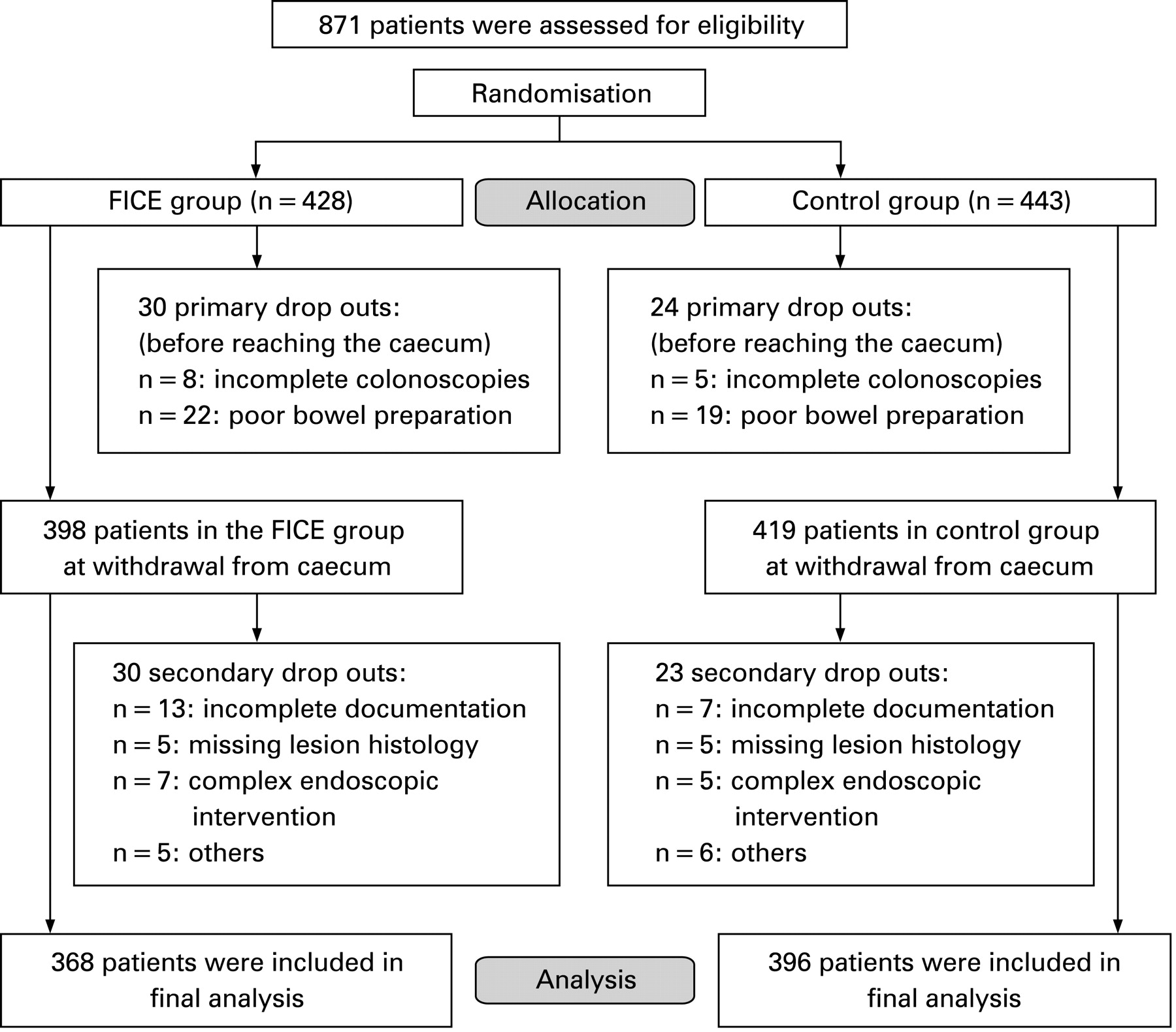
Between May 2006 and May 2007 a total of 871 patients were randomised to the FICE group (n = 428) or to the control group (n = 443). Quality of bowel preparation was rated as excellent in 275, good in 396, moderate in 146 and bad to very bad in 41 patients. According to the study protocol, patients with bad or very bad preparation or incomplete colonoscopy (n = 13) were excluded from final analysis (fig 2). Another 20 cases were excluded due incomplete documentation, 10 cases due to missing lesion histology, 12 patients who required complex endoscopic interventions (eg, mucosectomy), 7 patients for technical problems with endoscopic devices, and 4 patients for non-compliance and/or agitation, leaving a total of 764 patients (55.0% male) with a mean age of 64 years (range 45–86) for final analysis (fig 2). The FICE group included 368 patients and the control group included 396 patients. Patient demographics and indications for colonoscopy are shown in table 1. There were no statistically significant differences between the FICE and control group with respect to sex, age, indications for colonoscopy and rating of bowel cleansing.
{kind=link}
{kind=link}
In the FICE group, 186 patients (50.5%) had at least one lesion compared with 191 patients (48.2%) in the control group (p = 0.51). Altogether, colonoscopies in 764 patients detected 740 lesions with a mean size of 7.5 mm (range 2–65 mm). In table 2, prevalence rates of lesions in the FICE and control group are demonstrated in a per lesion analysis.
A total of 391 lesions were diagnosed in the control group compared with 349 lesions in the FICE group. There was no significant difference of the overall mean lesion per patient rate in the FICE or control group (p = 0.78). There were a total of 507 adenomas (67.6%), with 26 (5.1%) of them containing high grade neoplasias. Concerning the morphological appearance, 81.7% adenomas were <1 cm in size, and 22.7% were flat adenomas. The overall adenoma detection rate in the FICE group (mean of 0.64 per patient) was not different from that of the control group (mean of 0.68 per patient) (p = 0.92). Moreover, in the subgroup of adenomas <10 mm there was no significant difference between groups (p = 0.41). Although in the subgroup of flat lesions there was a tendency towards a higher detection rate in the control group (mean of 0.18 per patient) compared with the FICE group (mean of 0.11 per patient), this trend did not reach statistical significance (p = 0.09).
Table 3 demonstrates the prevalence of patients with lesions. In the FICE and the control group, the prevalence of patients with one or more lesions of any histology was 50.5% versus 48.2% (p = 0.51), of patients with ⩾1 adenoma 35.6% versus 35.4% (p = 1.0), of patients with ⩾1 carcinoma 3.3% versus 3.0% (p = 0.85) and of patients with ⩾1 hyperplastic polyp 18.5% versus 16.9% (p = 0.64).
Compared with colonoscopy with targeted indigocarmine spraying, FICE did not shorten the procedural time (mean (SD) 14.6 (8.8) vs 15.0 (8.3) min, respectively, p = 0.16).
During withdrawal, the medium volume of indigocarmine used in the control group was 6.5 ml per patient. In the FICE group, switching back from FICE to conventional imaging for reasons other than polypectomy was done in 113 procedures (for a median of 1.19 min), mostly to confirm uncertain findings by their conventional appearance (n = 68) or because of obstructed vision (n = 44).
Table 4 shows the performance of FICE and indigocarmine chromoendoscopy in differentiation of adenomas and hyperplastic polpys and the subgroup of lesions <10 mm. Visualisation of colonic lesions with the FICE system revealed a sensitivity of 93.2% and a specificity of 61.2% for classification of adenomas. There was no statistical significant difference compared with the scores achieved with indigocarmine. Moreover, performance of FICE and indigocarmine was comparable for classification of the subgroup of lesions <10 mm.
DISCUSSION
Detection of adenomas is essential at screening colonoscopy, but the miss rate, especially for small and flat lesions, remains unacceptably high. Although pan chromoendoscopy might be effective in improving detection and detailed morphological assessment of adenomas in some operators’ hands, it appears to be too time consuming and therefore not yet implemented to any great extent in clinical practice. To overcome the problems of conventional chromoendoscopy, the virtual chromoendoscopic techniques FICE and NBI were newly developed. Both techniques are safe, rapid and easy to apply, and several preliminary studies reported enhancement of vascular and mucosal contrast.
The present study is the first randomised, prospective multicentre trial that investigates the clinical feasibility of FICE for detection and classification of neoplastic colonic lesions. Altogether 871 patients with screening and diagnostic colonoscopies were randomised either to a FICE group or to a control group with targeted indigocarmine spraying. The overall adenoma prevalence was 35.5% and compared well with the adenoma rates of 37.5 and 28% that were found in recent large American32 and German33 screening trials, respectively. In the present study, application of FICE during withdrawal improved neither the overall yield of adenomas nor the number of patients with adenomas detected. For the subgroup of flat lesions there was even a trend towards poorer detection, although this did not reach statistical significance. Moreover, FICE did not shorten the procedural time during withdrawal compared with targeted indigocarmine spraying. On the other hand, for prediction of lesion histology, FICE imaging yielded excellent sensitivities for adenomas and was equivalent to indigocarmine chromoendoscopy.
Preliminary reports showed that in the oesophagus the detection rate for neoplasias of FICE29 and NBI34 appears similar to that of conventional chromoendoscopy. In the lower gastrointestinal tract the role of NBI has been assessed by a comparative approach in three recent single-centre studies, with somewhat disappointing results. For routine clinical indications26 27 and surveillance colonoscopies in patients with longstanding ulcerative colitis,28 NBI did not result in improved detection of adenomas compared with standard colonoscopy. Somewhat more encouraging findings were published recently by East and co-workers,35 suggesting that NBI might have a role for adenoma detection in a high risk group. They reported a back-to-back colonoscopic surveillance study on 62 patients with hereditary non-polypoosis colorectal cancer and found that a second additional examination with NBI almost doubled the total number of adenomas detected. In contrast to our findings on FICE, NBI might also improve detection rates of hyperplastic polyps27 35 that might be colorectal cancer precursors via the serrated pathway.36
It might be argued that in the current study results would have become more advantageous for FICE with increasing experience of the endoscopists using virtual chromoendoscopy. However, an opposite effect was shown in a recent trial on the value of NBI colonoscopy.27 Whereas the adenoma detection rate of NBI remained stable, in the control group the adenoma detection rate rose continuously during the course of the study. According to the authors, this effect probably represented a cognitive training effect of better polyp recognition on NBI.
A secondary end point of the present study was the performance of FICE in prediction of lesion histology compared with indigocarmine chromoendoscopy. Reliable classification of colorectal polyps at endoscopy saves time, reduces costs and minimises the risk of complications associated with polypectomy. To this end, several studies proposed that pit pattern analysis of colorectal lesions via chromoendoscopy using indigocarmine dye17 19 20 is an effective and objective tool for differentiating between neoplastic and non-neoplastic lesions. In the present study, application of the FICE system yielded excellent sensitivities for adenomas that were comparable with the results of conventional chromoendoscopy. However, as in some previous studies on indigocarmine37 38 and NBI,25 good sensitivities were associated with poorer specificities.
It is noteworthy that significantly more patients were included in each study arm than required based on a priori calculations. This over-recruitment was due to the study design and the policy of monitoring visits that caused some unintended time lag between inclusion of patients and evaluation of case report forms.
To the best of our knowledge, the present study is the first randomised multicentre trial investigating the value of the novel virtual chromoendoscopy techniques. Since this study involved a large case number and multiple endoscopists at five study centres it provides a true picture of the benefits and disadvantages of this technique. The present results and the published data on the value of NBI26 27 indicate that virtual chromoendoscopy in its present form does not significantly increase the adenoma yield at screening colonoscopy. There are two technical aspects inherent to both virtual chromoendoscopy techniques that may account for the failure to improve sensitivity for adenomas. First, the brightness of the image is sometimes insufficient to ensure a good overview in large luminal diameter sections of the bowel. Moreover, poor bowel preparation obstructs the view to a greater extent compared with standard colonoscopy, necessitating extra washing and suction. Both aspects might also lead to extension of the procedural time. Secondly, the structures enhanced by virtual imaging techniques are best appreciated by detailed inspection of areas of interest, preferably in a high magnification mode.19 21 25 Therefore, FICE and NBI might be less suitable for primary detection of abnormalities but should ideally be applied for detailed inspection of lesions for prediction of histology. In contrast, in defined mucosal areas, for example Barrett’s oesophagus, virtual chromoendoscopy might be helpful for primary detection of lesions.29 34 In this setting, the area of interest is limited and the lumen of the oesophagus is certainly much smaller compared with the colon, preventing generation of dark images.
In summary, the current study shows that for detection of lesions the FICE mode is not superior to standard colonoscopy with targeted chromoendoscopy. However, this does not necessarily exclude a benefit of FICE compared with standard colonoscopy alone. Differentiation between neoplastic and non-neoplastic mucosal patterns with FICE yielded results comparable with indigocarmine dye spraying. Therefore, FICE constitutes an easy to apply supplemental tool that might aid the endoscopist in differentiation between neoplastic and non-neoplastic mucosal patterns and delineation of subtle lesion boundaries.
REFERENCES
Footnotes
▸ Competing interests: Declared (the declaration can be viewed on the Gut website at http://www.gut.bmj.com/supplemental).
Funding: This study was supported by Fujinon, Saitama, Japan.
Ethics approval: The study protocol was approved by the clinical research ethics committee of the General Ethical Council of the state of Hessen (Germany) (no. 39/2006) and conformed to good clinical practice.
Patient consent: Obtained.
Linked Articles
- Digest