Article Text

Abstract
Objective Pouchitis is the most common complication after colectomy with ileal pouch-anal anastomosis (IPAA) for UC and the risk is the highest within the 1st year after surgery. The pathogenesis is not completely understood but clinical response to antibiotics suggests a role for gut microbiota. We hypothesised that the risk for pouchitis can be predicted based on the faecal microbial composition before colectomy.
Design Faecal samples from 21 patients with UC undergoing IPAA were prospectively collected before colectomy and at predefined clinical visits at 1 month, 3 months, 6 months and 12 months after IPAA. The predominant microbiota was analysed using community profiling with denaturing gradient gel electrophoresis followed by quantitative real-time PCR validation.
Results Cluster analysis before colectomy distinguished patients with pouchitis from those with normal pouch during the 1st year of follow-up. In patients developing pouchitis, an increase of Ruminococcus gnavus (p<0.001), Bacteroides vulgatus (p=0.043), Clostridium perfringens (p=0.011) and a reduction of two Lachnospiraceae genera (Blautia (p=0.04), Roseburia (p=0.008)) was observed. A score combining these five bacterial risk factors was calculated and presence of at least two risk factors showed a sensitivity and specificity of 100% and 63.6%, respectively.
Conclusions Presence of R. gnavus, B. vulgatus and C. perfringens and absence of Blautia and Roseburia in faecal samples of patients with UC before surgery is associated with a higher risk of pouchitis after IPAA. Our findings suggest new predictive and therapeutic strategies in patients undergoing colectomy with IPAA.
- IBD BASIC RESEARCH
- ILEOANAL POUCH
- INFLAMMATORY BOWEL DISEASE
- INTESTINAL BACTERIA
- POUCHITIS
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Up to 35% of patients with UC need a total colectomy with ileal pouch-anal anastomosis (IPAA) during their disease course.
After pouch surgery, many patients report a greatly increased quality of life, however, complications can occur, with pouchitis as the most common postoperative complication.
The cumulative risk to develop pouchitis is approximately 50% and is the highest within the 1st year after surgery.
Intestinal dysbiosis has been described in patients with pouchitis and may play a role in the pathogenesis because antibiotic and probiotic treatments are effective in pouchitis and pouchitis does not occur before restoration of the faecal stream.
What are the new findings?
The predominant microbiota in faecal samples before colectomy predict the development of pouchitis within the 1st year after IPAA.
We were able to describe a dysbiosis signature of five species associated with development of pouchitis. Predominant presence of Ruminococcus gnavus, Bacteroides vulgatus and Clostridium perfringens and absence of Blautia spp and Roseburia spp in faecal samples of patients with UC before colectomy increase the risk of pouchitis after IPAA.
We developed a risk score for pouchitis based on the predominant presence of the five signature species. The presence of two or more risk factors had a sensitivity and specificity of 100% and 63.6%, respectively.
How might it impact on clinical practice in the foreseeable future?
The ability to identify patients at risk to develop pouchitis based on their faecal microbial composition before colectomy may be helpful to perform more targeted intervention studies.
Patients at high risk may benefit from good surveillance and screening before colectomy can allow the prevention of pouchitis in these patients by an immediate initiation of a preventive treatment such as targeted antibiotics or probiotics.
Introduction
Pouchitis is the most common complication after colectomy with ileal pouch-anal anastomosis (IPAA) for UC. Between 10% and 35% of patients with UC refractory to standard treatment eventually need surgery.1 Approximately 50% of these patients develop at least one episode of pouchitis of which 40% develop pouchitis within the 1st year after surgery.2 The aetiology of pouchitis is not completely understood. In contrast to UC, pouchitis is rarely seen in patients with familial adenomatous polyposis with IPAA. This suggests that similar factors as those playing a role in the pathogenesis of UC may also be involved in the onset and perpetuation of pouchitis.3 In most patients, there is probably an abnormal immune response against the commensal microbiota and only a minority develop pouchitis secondary to Clostridium difficile or cytomegalovirus infection, non-steroidal anti-inflammatory drug use or ischaemia.4 Several risk factors for the development of pouchitis have been proposed. These include primary sclerosing cholangitis, extraintestinal manifestations, severe pancolitis, backwash ileitis, non-steroidal anti-inflammatory drug use, preoperative thrombocytosis, perinuclear antineutrophil cytoplasmic antibody and anti-CBir1 positivity, non-smoking, and genetic polymorphisms (interleukin-1 receptor antagonist (IL-1ra), tumor necrosis factor (TNF), Nucleotide-binding oligomerization domain 2 (NOD2), Toll-like receptor 1 (TLR1)).2 ,5 The findings of many reported risk factors are however inconsistent.
Also dysbiosis has been implicated as a triggering factor for pouchitis and is strongly supported by several lines of evidence pointing to a role of the microbiota. So pouchitis does not occur before ileostomy takedown and before exposure of the ileal mucosa to the faecal stream.5 The ileal mucosa undergoes morphological and functional changes after pouch construction. The mucosa changes to a more colon-like mucosa (ie, colonic metaplasia) as a result of villous atrophy, crypt hyperplasia and change in mucin composition.6 ,7 This change is even greater in pouchitis than in normal pouches (NPs).6 In addition, the pouch effluent contains higher bacterial concentrations than the normal ileum and studies reported alterations of the bacterial colonisation after IPAA.8 Treatments such as antibiotics and probiotics have a positive effect on the induction and maintenance of remission in pouchitis.9–13 Also high concentrations of antibodies directed against bacterial components such as flagellins have been associated with an increased risk for pouchitis.14
Microbial studies have shown dysbiosis in patients with pouchitis, although there is no overall consensus about the abundance of specific species.15 There is however a general agreement that the pouch microbiota is unstable over time and tends to shift to a more colon-like community.16–18
In this study we hypothesised that the faecal microbiota composition before colectomy might predict which patients undergoing IPAA are most at risk to develop pouchitis. We compared microbial profiles before surgery between patients that developed pouchitis and patients that stayed relapse-free during the first 12 months after IPAA. Our second aim was to study temporal changes of the predictive bacteria within the 1st year following ileostomy takedown and to investigate whether the predictive preoperative microbial signature may also apply after IPAA has been performed.
Methods
Patients
All patients were prospectively recruited via the University Hospital Leuven (Belgium). We included 23 patients with UC that underwent total colectomy with IPAA between 2011 and 2012. Nineteen patients completed follow-up. Two patients were lost to follow-up after month 1. One patient died due to a massive postoperative bleeding with secondary multiple organ failure and one patient still had a temporary ileostomy at the time of analysis and was excluded from the analysis. Faecal samples were collected at the time of colectomy and at predefined clinical visits at 1 month, 3 months, 6 months and 12 months after ileostomy closure. Patients underwent pouchoscopy at the predefined time points. The diagnosis of pouchitis was based on symptoms and presence of endoscopic inflammation. The characteristics of the patients are represented in table 1.
Baseline characteristics of the study population
Patients who experienced at least one event of pouchitis were compared with patients that stayed relapse-free during the first 6 months or first 12 months after IPAA (after 6 months: Nnormal pouch=13; Npouchitis=6; after 12 months: Nnormal pouch=11; Npouchitis=8). For temporal analysis, all 19 patients were divided into the pouchitis or NP group at four time points (month 1, month 3, month 6 and month 12) following IPAA.
In addition, we studied a second cohort. Baseline faecal samples were collected from 14 patients with UC undergoing a colectomy with IPAA after 2012. All patients completed the 12 month follow-up and underwent a pouchoscopy at month 1, month 3, month 6 and month 12 after IPAA.
Six (43%) patients developed endoscopic pouchitis during the 1-year follow-up period. The baseline characteristics of the second cohort are represented in the online supplementary table S1.
Samples and DNA extraction
Cooled samples were provided within 24 h after collection and aliquots were immediately stored at −80°C. Faecal bacterial DNA was extracted using a modification of the method of Pitcher et al19 as previously described and stored at −80°C.20 Dry faecal weights were calculated based on the lyophilisation of a preweighed portion between 0.2 g and 0.5 g in duplicate. The faecal samples were dried in a lyophilisator (Christ, Osterode, Germany) and weighed again. The faecal dry weight was expressed as percentage.
Faecal calprotectin
Calprotectin was measured in all faecal samples before and after surgery. Fresh cooled faecal samples were extracted within 24 h upon arrival using the Smart Prep extraction device (Roche Diagnostics, Mannheim, Germany). Faecal extracts were stored at −20°C until measurement. Calprotectin was determined using the Quantum Blue Calprotectin High Range Assay (Bühlmann Laboratories AG, Schönenbuch, Switzerland) according to the manufacturer's instructions.
Denaturing gradient gel electrophoresis profiling and analysis
Bacterial DNA extracted from the faecal samples was used for community PCR with universal bacterial primers (F357 with GC clamp and R518) targeted against the hypervariable V3 region of the 16S rRNA gene and subsequent denaturing gradient gel electrophoresis (DGGE) fingerprinting using a 40–80% denaturing gradient.21 For electrophoresis at 70 V for 990 min at 60°C, 30 µL of the PCR product was loaded. Each gel included three standard reference lanes containing amplicons of 12 bacterial reference strains for normalisation and comparison between gels. DGGE gels were stained with GelRed Nucleid Acid Gel Stain (Biotium, VWR, Leuven, Belgium) for 30 min and were visualised using a molecular imager (ChemiDoc XRS imaging system, Bio-Rad, Nazareth, Belgium). The digitised profiles were processed with BioNumerics V.4.6 (Applied Maths, St-Martens-Latem, Belgium) that assigned bands to band classes within all the profiles as previously described.22
Extraction and identification of bands
Bands belonging to the band classes of interest were excised, purified and verified as previously described.22 To check for comigration of bands, purified bands were analysed again with DGGE using an adjusted denaturing gradient. Purified bands and the original fingerprint profile from which they were extracted were analysed together on the same gel to check for correct excision of bands. After identity and quality control of the purified band, its DNA was sequenced using an ABI Prism 3130 Genetic Analyser (Applied Biosystems, USA). The sequencing results of bands assigned to the same band class of at least seven patients with UC were first aligned (using Vector NTI Advance v11.5) to confirm that they were identical. For identification, the obtained sequences were compared with sequences available in the GenBank DNA database (National Center for Biotechnology Information (NCBI)) and in the Ribosomal Database Project (RDP).
Real-time PCR
Quantification of bacterial DNA was performed using the Applied Biosystems 7500 Fast Real-Time PCR System (Applied Biosystems, Ghent, Belgium). Primers and probe sets used to quantify Clostridium perfringens, Bacteroides vulgatus, Ruminococcus gnavus, Blautia spp, Roseburia spp and Roseburia hominis are listed in online supplementary table S2. Details on primer and probe design, specificity testing, RT-PCR conditions and analysis are described in the online supplementary material.
Short-chain fatty acids measurement
Propionate was supplied by UCB (Leuven, Belgium), butyrate was supplied by Devos-Francois (Charleroi, Belgium), and acetate and 2-ethylbutyrate by Merck (München, Germany). All standards were of analytical quality (at least 99% purity). Sodium chloride (99%) was purchased from VWR (Leuven, Belgium) and sulfuric acid (99%) from Sigma-Aldrich (Bornem, Belgium). Faecal aliquots of 100 mg were used. 2-Ethylbutyrate (50 µL; 125 mg/mL) was added as internal standard. A pinch of sodium chloride and 150 µL sulfuric acid were added to the sample to salt out and acidify the solution, respectively. Diethylether (Sigma) 3 mL was added to each sample before extraction. The short-chain fatty acids (SCFAs) were analysed on a gas chromatography-mass spectrometry quadrupole (Trace GC, Thermoquest, Rodano, Italy and DSQ II, Thermo Electron, San Jose, USA) which was coupled on-line to an autosampler (AS 3000, Thermo Electron, San Jose, USA). The resulting chromatograms were processed using XCalibur software (V.1.4 SR1, Thermo Electron, San Jose, USA). Acetate, propionate and butyrate were quantified with appropriate calibration curves obtained using internal standard quantitation.
Statistical analysis
Data were analysed using SPSS (SPSS V.20.0 for Windows, SPSS, Chicago, Illinois, USA). The microbial profiles were compared between patients developing pouchitis and patients with NP during follow-up. Differences in presence of bands of DGGE profiles were determined using Pearson's χ2 test. The Mann–Whitney U test was performed for comparison of band intensity and bacterial count quantified by RT-PCR between the different groups. Principle component analysis (PCA) and partial least squares discriminant analysis (PLS-DA) was performed using The Unscrambler V.9.7 (Camo, Oslo, Norway). This multivariate analysis was used to cluster the microbial profiles according to similarities in band classes. Kaplan-Meier analysis using log-rank and Breslow testing was performed to study the occurrence of pouchitis with respect to presence and absence of the identified species. p Values <0.05 were considered statistically significant. Hierarchical clustering based on similar combinations in presence or absence of the microbial predictors was performed using the statistical package ‘pvclust’23 in R (V.3.0.2, http://www.r-project.org/). The level for statistical significance was considered at approximately unbiased (AU) >95% and these clusters were highlighted by rectangles. Frequencies of pouchitis within clusters were measured. Comparison of alteration frequencies of pouchitis between the clusters was performed using Fisher's exact test.
Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for development of pouchitis were calculated. The area under the curve (AUC) and cut-off values for the bacterial groups were determined by receiver-operating characteristics (ROC) analysis using the ‘pROC’ package in R.
Results
Study cohort
The cumulative incidence of pouchitis increased with time from 10% at month 1 to 21% at month 3, 32% at month 6 and 42% at year 1.
Patient risk factors for development of pouchitis were compared between the patients with and without pouchitis after 1 year of follow-up (see online supplementary table S3). In univariate analysis, a younger age at colectomy (p=0.017) and shorter disease duration (p=0.017) were identified as risk factors to develop pouchitis within 12 months after IPAA. No other significant differences were observed.
Prediction of pouchitis based on the microbial composition before colectomy
DGGE microbial profiling
PCA showed a moderate clustering of patients developing pouchitis during the 1 year follow-up and patients with NP during the whole follow-up based on similar microbial DGGE profiles before colectomy, although full discrimination was not achieved (figure 1A). The variance explained by the X-matrix was 36% (Principle component 1 (PC1):20% and principle component 2 (PC2): 16%). Performing supervised PLS-DA analysis on the same data set generated a clustering of both patient groups (figure 1B). The PLS-DA plot of the microbial profiles explained 27% (PC1:18% and PC2: 9%) of the X-variance and 81% (PC1:56% and PC2:25%) of the Y-variance.

(A) Principle component analysis (PCA) and (B) partial least squares discriminant analysis (PLS-DA) for discrimination of patients with pouchitis (N=8) versus patients with a normal pouch (N=11) during the 1 year follow-up period, based on the microbial profiles before colectomy.
DGGE analysis of the faecal samples before colectomy identified 63 band classes. These band classes were compared between patients developing pouchitis and patients with NP within the first 6 months or first 12 months after IPAA.
We first analysed which band-classes could predict early pouchitis (ie. within the first 6 months): five band classes differed significantly between patients with pouchitis (n=6) and patients without pouchitis (n=13). Sequencing of the purified amplicons of each band class identified the bacterial groups (see online supplementary table S4). For band class 2.82, sequencing of the purified amplicons revealed 100% homology with B. vulgatus. Amplicons belonging to band classes 10.98 and 12.43 showed 100% homology with R. gnavus and C. Perfringens, respectively.
Basic Local Alignment Search Tool (BLAST) analysis in NCBI assigned band class 10.2 with 100% homology to Blautia luti, Blautia wexlerae and Ruminococcus obeum, a species that is currently considered a member of the genus Blautia (http://www.bacterio.net/blautia.html).24 Comparison in RDP also revealed 100% sequence similarities with different species from this genus, thus band class 10.2 was assigned to the genus Blautia. Finally, the purified amplicons belonging to band class 8.67 all comigrated together. Sequence analysis of these amplicons revealed that this band class was composed of three different sequences that differed with one mismatch each. These sequences belonged to different genera of the Lachnospiraceae family. The first and most common sequence clearly belonged to the genus Roseburia. Homology search in NCBI revealed 100% similarity with Roseburia hominis. The other two sequences were less frequently present. RDP comparison did not allow classification at genus level and assigned both sequences to the Lachnospiraceae family. Both sequences showed closest homology with Roseburia, Coprococcus and Lachnospiracea incertae sedis.
The presence and/or relative band intensity of the potentially discriminatory band classes were significantly higher for those assigned to B. vulgatus, R. gnavus and C. perfringens in patients developing pouchitis compared with patients with NP within the first 6 months after IPAA. In contrast, Blautia and Roseburia genera were significantly reduced in the pouchitis group (table 2).
Band presence and relative intensity of bacterial groups in patients before colectomy associated with pouchitis within the first 6 months and 12 months after IPAA
We then tested if the band classes could also predict pouchitis within the 1st year. When comparing the patients with pouchitis after 1 year (n=8) with the patients without pouchitis (n=11) at 1 year follow-up, the significance of these findings was further confirmed for R. gnavus, C. perfringens and Roseburia spp after analysis of presence and intensity (table 2).
Three patients received antibiotics 1 month before sampling. We did not observe significant effects of antibiotic use on presence or intensity of the microbiota.
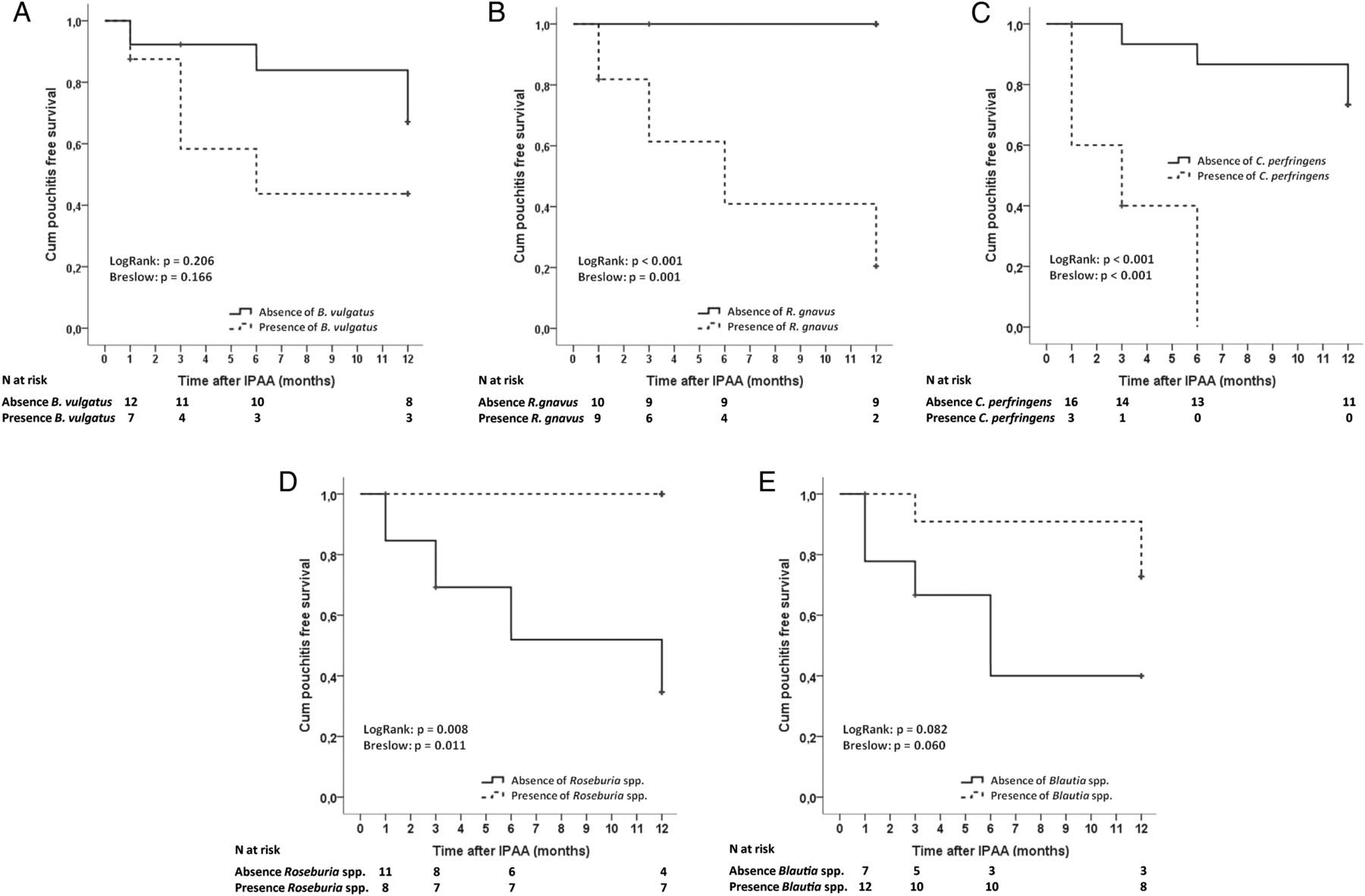
The cumulative risk for pouchitis 6 months following IPAA was higher in patients where B. vulgatus was present before colectomy (57.1%) compared with absence of the species (16.7%) (p=0.066). The increased risk for pouchitis in a similar comparison over 1 year follow-up was less pronounced (figure 2A). Remarkably, the second species R. gnavus, was present before colectomy in all patients developing pouchitis. The cumulative pouchitis-free survival after 1 year of follow-up was significantly higher in patients without R. gnavus in their predominant gut microbiota (0%) compared with patients with this species present in their predominant gut microbiota (80%. p<0.001) (figure 2B). The third species C. perfringens was only detected in patients developing pouchitis. Kaplan-Meier analysis further showed a significantly increased cumulative risk for pouchitis where C. perfringens was present (100%) before colectomy in contrast to absence of the species (30.8%) (p<0.001) (figure 2C). On the other hand, Roseburia spp was absent in the predominant microbiota before colectomy in all patients suffering from pouchitis after 1 year. The cumulative risk for pouchitis was significantly reduced in patients where Roseburia spp were present before colectomy (0%) compared with absence of the species (66.7%, p=0.008) (figure 2D). Finally, Kaplan-Meier analysis showed a significantly decreased risk for pouchitis 6 months following IPAA in presence (9.1%) versus absence (62.5%, p=0.034, data not shown) of Blautia species in the predominant microbiota. Similar analysis over 1 year follow-up showed a trend towards significance (p=0.082) (figure 2E).

Results of the Kaplan-Meier analysis for presence (dotted line) or absence (solid line) of Bacteroides vulgatus (A), Ruminococcus gnavus (B), Clostridium perfringens (C), Roseburia spp (D) or Blautia spp (E) are shown as the cumulative pouchitis-free survival. Log-rank and Breslow testing was used to measure significant differences.
We then investigated whether a predetermined combination of bacterial groups may be indicative of a specific disease outcome by performing hierarchical clustering. Seven distinct subgroups were found, each represented by a different species core (AU>95%) (figure 3). Two clusters corresponded to patients developing pouchitis, three clusters to patients with NP and two clusters contained patients with mixed outcomes after 1 year follow-up (p=0.036). Absence of the two high-risk species R. gnavus and C. perfringens in the predominant microbiota combined with presence of at least one low-risk species seemed to guarantee a normal outcome within the 1st year after IPAA with a sensitivity, specificity, PPV and NPV of 100%, 72%, 72% and 100%, respectively. In contrast, patients carrying at least two high-risk species and absence of both low-risk species before colectomy certainly developed pouchitis with a sensitivity, specificity, PPV and NPV of 63%, 100%, 100% and 79%, respectively.

Hierarchical clustering using ‘pvclust’ (binary distance, Ward's linkage) based on absence or presence of the five predictive bacterial groups in faecal samples before colectomy. Seven significant clusters (AU>95%) are highlighted in rectangles. Each cluster was represented by a different bacterial core and associated with disease outcome within the 1st year after IPAA. The frequency of each bacterial group is expressed in percentage. AU, approximately unbiased; IPAA, ileal pouch-anal anastomosis; NP, patients with normal pouch; P, patients with pouchitis.
Finally, we developed a risk score based on the five bacterial variables. Presence of a high-risk species (B. vulgatus, R. gnavus or C. perfringens) and absence of the low-risk Roseburia spp or Blautia spp before colectomy were each scored as 1 point. The risk score was calculated by summing up these five bacterial risk factors, thus ranging from 0 to 5 points. The linear trend for association of the risk scores with the development of pouchitis within the 1st year after IPAA was statistically significant (p=0.001). The risk score showed an AUC of 0.955 (95% CI 0.885 to 1). The presence of two or more risk factors had a sensitivity, specificity, PPV and NPV of 100%, 63.6%, 66.7% and 100%, respectively (table 3).
Sensitivity, specificity, PPV and NPV of the risk score based on predominant presence of the five bacterial groups before colectomy
Quantitative analysis of the predictive bacteria in faecal samples before colectomy
The count of R. hominis before colectomy was significantly lower in the pouchitis group versus the NP group (p=0.017) whereas the reduction of Roseburia spp was not significant (p=0.248). In contrast, the count of C. perfringens was significantly higher before colectomy in patients experiencing pouchitis (p=0.039) whereas the count of R. gnavus was also higher in the pouchitis group but lacked significance (p=0.322). No differences were observed for B. vulgatus and Blautia spp. Median (IQR) of the bacterial counts are shown in online supplementary table S5 and online supplementary figure S1.
A risk score was calculated based on the quantitative values of the five bacterial groups. The optimal cut-off for each bacterial group was determined by ROC analysis. Counts (log10/colony-forming unit (CFU) dry faeces) for B. vulgatus >6.9, R. gnavus >6.6, C. perfringens >3.8, Roseburia spp <7.7 and Blautia spp <6.8 were each scored as 1 point. The risk score showed an AUC of 0.818 (95% CI 0.639 to 0.998) and a significant linear-by-linear association with the development of pouchitis after 1 year (p=0.018). The sensitivity, specificity, PPV and NPV of a risk score ≥2 was 100%, 63.6%, 66.7% and 100%, respectively (online supplementary table S6).
Validation of the microbial findings in a second cohort
DGGE analysis of the second cohort revealed a similar trend for the identified microbial signature species. Comparison of the presence and relative band intensity of the microbial signature species between patients with and without development of pouchitis within the 1st year after IPAA are shown in the online supplementary table S7.
Kaplan-Meier analysis showed an increased cumulative risk for development of pouchitis in the 1st year of follow-up in patients with presence of B. vulgatus, R. gnavus and C. perfringens (67%, 63%, 100%) compared with patients with absence of the species (25%, 17%, 33%; p=0.183, p=0.095, p=0.189), respectively. In contrast, patients with presence of Roseburia spp and Blautia spp (both 22%) before colectomy had a reduced risk to develop pouchitis compared with patients with absence of these species (both 80%; p=0.061, p=0.007), respectively.
Calculation of the risk score based on presence of the five bacterial species showed an AUC of 0.979 (95% CI 0.931 to 1). Linear trend analysis showed a significant association between the number of risk factors and development of pouchitis (p=0.003). Presence of two or more risk factors had a sensitivity, specificity, PPV and NPV of 100%, 75%, 75% and 100%, respectively (see online supplementary table S8).
Quantitative analysis of the second cohort showed a significant reduction of R. hominis (p=0.01) and significant increase of C. perfringens (p=0.039) before colectomy in patients developing pouchitis after IPAA. A trend towards significance was observed for Blautia spp (p=0.071). The bacterial counts for all signature bacteria are shown in the online supplementary table S9.
The risk score for quantitative data was based on the optimal cut-off that was determined in the original cohort for each bacterial group previously. The AUC was 0.802 (95% CI 0.559 to 1) and the linear-by-linear association showed a trend towards significance (p=0.066). The sensitivity, specificity, PPV and NPV of the risk score are represented in the online supplementary table S10.
Temporal quantitative analysis of the predictive bacteria in faecal samples after IPAA
We next studied if the predictive species changed in concentration over time following IPAA in the collected samples at month 1 (N=19), month 3 (N=18), month 6 (N=17) and month 12 (N=18). Median counts of bacteria in each group (pouchitis and NP) at the different time points are shown in online supplementary table S5. The comparisons between (difference at fixed time points after IPAA) and within (changes over time) the group of patients that developed pouchitis and the group of patients with NP after 1 year follow-up are detailed described in online supplementary material.
Furthermore, we investigated whether the bacterial signature still may be predictable at month 1, month 3 and month 6 after IPAA for the development of pouchitis after 1 year. Hierarchical clustering based on similarities in the combination of the five bacterial groups at month 1, month 3 and month 6 showed no clusters that significantly corresponded to the patient’s disease outcome 1 year after IPAA (pM1=0.9, pM3=0.15, pM6=0.14).
The risk scores at month 1 and month 3 showed no linear-by-linear association with the development of pouchitis 1 year after IPAA (pM1=0.907, pM3=0.219). In contrast, a significant linear trend was found at month 6 (pM6=0.005). The AUC of the risk score was 0.894 (95% CI 0.747 to 1). The presence of three or more risk factors had a sensitivity, specificity, PPV and NPV of 66.7%, 90.9%, 80% and 83.3%, respectively. The values for each risk score are shown in online supplementary table S11.
Prediction of pouchitis based on faecal calprotectin
Faecal calprotectin levels at the time of colectomy were extremely high in all patients. No difference in calprotectin was observed at baseline between patients developing pouchitis and patients without pouchitis in the year following IPAA (p=0.934). After IPAA, there was a significant drop of calprotectin in both groups (NP group, p=0.009; P group, p=0.046) (figure 4A). Interestingly, calprotectin was significantly increased at each time point after IPAA within the group of patients developing pouchitis compared with those without pouchitis within 12 months (figure 4A). ROC analysis on calprotectin concentrations at the 1st month after IPAA showed an AUC of 0.833 (95% CI 0.635 to 1), sensitivity of 83.3% and specificity of 72.7%. Two patients with pouchitis at month 1 were excluded from this analysis. The optimal cut-off was 315.5 µg/g calprotectin. Kaplan-Meier analysis further showed an increased cumulative risk for pouchitis when calprotectin levels were higher or equal to 315.5 µg/g at the 1st month after IPAA (50%) compared with patients with calprotectin levels smaller than 315.5 µg/g (11%) (log-rank, p=0.044) (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Median faecal calprotectin levels at different time points during follow-up (month 0, month 1, month 3, month 6 and month 12) between patients with (black) and without (grey) an event of pouchitis within 12 months. Box plots represent median, IQR and 95% CI. *p<0.05. (B) Kaplan-Meier survival analysis for development of pouchitis within the 1st year after ileal pouch-anal anastomosis (IPAA) in patients with faecal calprotectin levels higher or equal to 315.5 µg/g (solid line) or lower than 315.5 µg/g (dotted line) at the 1st month after IPAA. Total number of patients in the analysis was 17, with exclusion of 2 patients with pouchitis at month 1.
Prediction of pouchitis based on SCFAs
The concentrations of SCFAs at the time of colectomy were neither associated with development of pouchitis within 12 months after IPAA in the original cohort nor in the validation cohort (table 4).
Comparison of SCFA (acetate, propionate and butyrate) concentrations in faecal samples at the time of colectomy between patients developing pouchitis and patients staying relapse-free during the 1st year after IPAA
Discussion
We investigated the predominant microbiota composition in faecal samples of patients with UC undergoing colectomy with IPAA to predict disease outcome within the 1st year after IPAA. With a cumulative incidence of pouchitis of 42% after 12 months, we identified five microbiota members predicting pouchitis when present or absent before colectomy, namely B. vulgatus, R. gnavus, C. perfringens, Blautia spp and Roseburia spp.
B. vulgatus increased the risk of developing pouchitis when present before colectomy. This commensal species is one of the most frequently isolated microorganisms from the human gut but is also known as an opportunistic pathogen.25 B. vulgatus is more prevalent in biopsies from patients with UC, and serological antibody responses against this organism were higher in UC than in healthy controls.26 ,27 Bacteroides spp have also been associated with the development of postoperative recurrence in patients with CD.28 Convincing evidence for a role of B. vulgatus in the pathogenesis of UC is coming from animal models where an induction of inflammation after monoassociation with B. vulgatus or after supplementation of bacterial cocktails containing this species was reported.29–33 Interestingly, coadministration of Bifidobacterium strains together with B. vulgatus strains reduced inflammation and the count of B. vulgatus in gnotobiotic mice.34 ,35 In addition, induction of an elemental diet led to elimination of B. vulgatus and repressed the onset of colitis.29 B. vulgatus induces an innate immune response in intestinal epithelial cells, activates Nuclear factor-kappa B (NF-κB) and induces proinflammatory gene expression.36 Furthermore, B. vulgatus strains isolated from patients with UC are able to induce proinflammatory cytokine production and to adhere to and invade colonic epithelial cells.37
R. gnavus also increased the risk of developing pouchitis 1 year after IPAA if present in the predominant microbiota before colectomy. Interestingly, this species was present in the samples before colectomy of all patients that suffered from pouchitis post-IPAA. We previously described an increase of this species also in CD.22 R. gnavus produces the bacteriocin ruminococcin A, that inhibits the growth of species phylogenetically related to R. gnavus and of various bifidobacterial and clostridial species.38 This bacteriocin can also degrade intestinal mucin.39 It furthermore expresses α-galactosidase and β-glucuronidase activity in vitro.40 ,41 β-glucuronidase activity can generate toxic metabolites in the colon which might provoke local inflammation. Png et al observed an increase of mucolytic bacteria including R. gnavus in biopsies of patients with UC and CD.42
The third species associated with an increased risk of developing pouchitis was identified as C. perfringens. This species was only present before colectomy in patients developing pouchitis. C. perfringens is an intestinal commensal that can also behave as a pathogen, for example, through the production of toxins that can destruct the host tissues.43 C. perfringens exerts proteolytic and mucinase activity, both of which may play a role in the pathogenesis of IBD.44 Several studies have reported a higher presence of C. perfringens in patients suffering from pouchitis.16 ,45–47
Even more interesting was the finding of the two genera that reduced the risk of developing pouchitis if present before colectomy. They were assigned to the genera Blautia and Roseburia, both of which belong to the Clostridium XIVa cluster of the Firmicutes phylum and are members of the Lachnospiraceae family. Members of Clostridium XIVa cluster have been repeatedly described as reduced in faeces and biopsies of patients with UC.48–53 This cluster harbours most of the butyrate-producing species in the healthy colon.54 Likewise, a lower abundance of Lachnospiraceae in patients with UC has been reported.55 ,56
Blautia spp are mainly producers of acetate but some species are also capable of producing succinate and lactate.57 Acetate is important for lowering the intestinal pH and exerts anti-inflammatory properties in vitro.58 We previously described a reduction of acetate in faeces from patients with UC.21 In the present study, Blautia spp numbers were also reduced in faecal samples of patients with pouchitis 1 year after IPAA. A recent study also reported lower levels of Blautia species in patients with pouchitis compared with patients with NP.59 Collectively, these findings suggest that monitoring Blautia spp after IPAA might be useful to discriminate between inflamed pouches and NPs.
Finally, Roseburia spp were significantly more abundant in the predominant faecal microbiota before colectomy in patients with NPs and were completely absent in the baseline predominant microbial profiles of patients experiencing pouchitis. The genus Roseburia contains species that produce butyrate as the main end product.54 ,60 Butyrate is the primary energy source for colonocytes and improves the mucosal barrier function of the colon. Butyrate furthermore exerts immunomodulatory and anti-inflammatory properties by downregulating proinflammatory cytokines and is reported to correlate negatively with severity of disease in patients with UC.61 ,62 Recent studies revealed a reduction of Roseburia spp in mucosal and faecal samples of patients with UC and implicated a role of this species in the pathogenesis of UC.49 ,53 ,63
The absence of two high-risk species R. gnavus and C. perfringens combined with presence of at least one low-risk species assured a NP within the 1st year after IPAA. In contrast, presence of at least two high-risk species and absence of both low-risk species always resulted in the development of pouchitis.
In the current study, we developed a risk score based on presence of the high risk and absence of the low risk signature species before colectomy. A major novel finding was that the score helps to identify patients at risk for development of pouchitis within the 1st year postoperatively. Moreover, the validity of the risk score has been confirmed in a second cohort. The performance of the microbial risk score after IPAA showed a good result at month 6 after IPAA but was less pronounced at the other time points during follow-up. In contrast, faecal calprotectin levels after surgery but not before, were found to be highly associated with the profound risk for pouchitis, which is a confirmation of a recent study by Yamamoto et al.64 The microbial signature before colectomy and the faecal calprotectin after IPAA might be useful biomarkers for early prediction of pouchitis.
This is an important predictive signature which should be studied in independent external validation cohorts.
Within this study we mainly focused on species or genera involved in the prediction of pouchitis. Although this clinical situation is also an excellent model to study whether dysbiosis precedes or rather is a consequence of intestinal inflammation, we cannot draw any conclusions concerning causality based on our data. So far, only few studies have investigated the use of antibiotics or probiotics in preventing pouchitis.10 ,12 VSL#3 has been shown to be more effective than placebo for the prevention of pouchitis but other studies failed.9–11 ,65 ,66 If patients at risk of developing pouchitis can be identified before colectomy, more targeted intervention studies can be performed. Therefore, future intervention trials should include microbiome analysis of the patients.
In conclusion, this is the first study on the association between the predominant microbial composition prior to colectomy and the likelihood of developing pouchitis within the 1st year following IPAA. The presence of R. gnavus, B. vulgatus, C. perfringens and absence of members of the Lachnospiraceae genera Blautia and Roseburia in faecal samples of patients with UC before surgery was associated with a higher risk of pouchitis within the 1st year after IPAA. Our findings shed new light on the aetiology of pouchitis and may lead to new predictive and therapeutic strategies.
Acknowledgments
The authors thank Isabelle Terrasson and Vera Ballet for their support in the collection of samples and Greet Vermeulen for technical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Marie Joossens at @JoossensM
Contributors KM: study concept and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, statistical analysis and technical support; JS: technical support; LV: technical support; MJ: drafting of the manuscript; IA: drafting of the manuscript; MdB: statistical analysis; VE: technical support; GVA: critical revision of the manuscript for important intellectual content; MF: critical revision of the manuscript for important intellectual content; JV: critical revision of the manuscript for important intellectual content; KVS: statistical analysis, critical revision of the manuscript for important intellectual content; FVI: material support, critical revision of the manuscript for important intellectual content; GH: material support, critical revision of the manuscript for important intellectual content; KV: material support, critical revision of the manuscript for important intellectual content; AW: critical revision of the manuscript for important intellectual content; AdBVO: critical revision of the manuscript for important intellectual content; AD: critical revision of the manuscript for important intellectual content; PR: critical revision of the manuscript for important intellectual content; SV: study concept and design, acquisition of data, interpretation of data, drafting of the manuscript, obtained funding, material support and study supervision.
Funding This work was supported by the Geconcerteerde Onderzoekacties (GOA) of the KU Leuven (grant number GOA/11/015); KM, MJ and IA are postdoctoral fellows and SV, MF and GVA are senior clinical investigators of the Fund for Scientific Research-Flanders, Belgium (FWO-Vlaanderen); MdB is a PhD student funded by a fellowship from the Agency for Innovation by Science and Technology (IWT).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of University of Leuven (Ethics committee approval, S52544 and S53684).
Provenance and peer review Not commissioned; externally peer reviewed.