Article Text

Abstract
Objective Operative link on gastritis assessment (OLGA) staging for gastritis ranks the risk for gastric cancer (GC) in progressive stages (0–IV). This prospective study aimed at quantifying the cancer risk associated with each gastritis stage.
Design A cohort of 1755 consecutive patients with dyspepsia underwent initial (T-0) oesophagogastroduodenoscopy with mapped gastric biopsies, OLGA staging and assessment of Helicobacter pylori infection. Patients were followed for 55 months (median); patients with stages II III and IV underwent a second endoscopy/restaging (T-1), and those with stages 0 and I were followed clinically and through in-depth clinical and record checking. Endpoints were OLGA stage at T-1 and development of gastric epithelial neoplasia.
Results At T-0, 77.6% of patients had stage 0, 14.4% stage I, 5.1% stage II, 2.1% stage III and 0.85% stage IV. H. pylori infection was detected in 603 patients at T-0 and successfully eradicated in 602 of them; 220 had a documented history of H. pylori eradication; and 932 were H. pylori naïve-negative. Incident neoplastic lesions (prevalence=0.4%; low-grade intraepithelial neoplasia (IEN)=4; high-grade IEN=1; GC=2) developed exclusively in patients with stages III–IV. The risk for epithelial neoplasia was null in patients at stages 0, I and II (95% CI 0 to 0.4), 36.5 per 1000 person-years in patients at stage III (95% CI 13.7 to 97.4) and 63.1 per 1000 person-years in patients at stage IV (95% CI 20.3 to 195.6).
Conclusions This prospective study confirms that OLGA staging reliably predicts the risk for development of gastric epithelial neoplasia. Although no neoplastic lesions arose in H. pylori-naïve patients, the H. pylori eradication in subjects with advanced stages (III–IV) did not abolish the risk for neoplastic progression.
- gastric cancer
- pre-malignancy - gi tract
- gastritis
- helicobacter pylori
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Helicobacter pylori is a class I carcinogen, and its infection results in a spectrum of phenotypic modifications of the gastric mucosa (inflammation and gastric mucosa atrophy).
Atrophic gastritis is a premalignant condition associated with increased cancer risk. The current international guidelines do not consistently ‘rank’ the severity/topographical extension of gastric atrophy (and its associated cancer risk).
Gastritis staging distinguishes atrophic versus non-atrophic gastritis, and links to the most advanced gastritis stages III–IV, the highest risk for cancer progression.
No prospective long-term follow-up studies are available to support the prognostic impact of gastritis staging in clinical practice.
What are the new findings?
This prospective, long-term follow-up study involved 1755 consecutive European patients with dyspepsia who underwent endoscopy and gastritis staging. At the end of the follow-up, neoplastic lesions were only found in patients enrolled as stage III–IV gastritis.
No cases of cancer progression were documented in naïve H. pylori-negative subjects.
In high-stage (III–IV) gastritis, H. pylori eradication does not nullify the neoplastic risk.
Significance of this study
How might it impact on clinical practice in the foreseeable future?
In the absence of predictive (serological or molecular) markers of gastric cancer risk, endoscopy/biopsy assessment of the gastritis stage represents a solid clinical-biological rationale for establishing personalised strategy for gastric cancer secondary prevention.
In H. pylori-eradicated patients, follow-up strategies aimed for gastric cancer secondary prevention can be reliably restricted to the subgroup of patients harbouring high-stage (III–IV) gastritis.
Because of their ‘intrinsic’ cancer risk, a dedicated endoscopic/histological follow-up is recommended in patients with high-stage gastritis, even among H. pylori-eradicated patients.
In patients with high-stage (III–IV) gastritis, an endoscopy follow-up interval of 2 years is advisable.
Introduction
Gastric cancer (GC) is a highly lethal malignancy with an overall 5-year survival rate lower than 25%. Most gastric adenocarcinomas, particularly those of the intestinal type, are associated with a sequence of phenotypic changes of the native mucosa triggered by long-standing inflammation.1 Helicobacter pylori infection is, by far, the most common aetiological agent of chronic active gastritis and the most common aetiological factor of gastric non-syndromic oncogenesis.2–10 Primary prevention of H. pylori infection and H. pylori eradication before the development of atrophic changes are the most effective methods of preventing GC. H. pylori eradication in older patients with extensive gastric mucosa atrophy has also been shown to reduce the incidence of metachronous and primary GCs.11–13 There is now a broad consensus that all infected patients should be treated, irrespective of their age or the severity of the gastric mucosal lesions.9
More than 95% of gastric adenocarcinomas arise in atrophic mucosa.14–18 Gastric mucosal atrophy consists of both the absolute loss of resident glandular units and the transformation of native glands to intestinal metaplasia or spasmolytic polypeptide expressing metaplasia.19–22 These new populations of metaplastic or transdifferentiated epithelia may undergo dedifferentiation and acquire most of the biological profile of neoplastic cells, except for the ability to invade (intraepithelial neoplasia (IEN), formerly known as dysplasia). Eventually the cells may acquire the phenotype of invasive cancer by losing their cohesiveness.23
Available data indicate that both extension and topographic distribution of gastric atrophy parallel the risk for GC, and several international guidelines suggest that patients with ‘extensive’ atrophic gastritis should be candidates for endoscopic follow-up protocols.8 9 24–29 Conversely, no unequivocal indication for endoscopy follow-up has been established for non-atrophic gastritis. Gastritis staging systems based on the atrophy score in biopsy samples obtained from both antral and oxyntic mucosa have ranked the risk for GC in progressive stages from 0 to IV and have designated high-risk stages III and IV as precancerous lesions deserving dedicated follow-up.30–39
The overarching aim of this prospective study of a cohort of 1775 patients was to quantify the cancer risk associated with each different operative link on gastritis assessment (OLGA) stage of gastritis as assessed by the histopathological examination of a set of standardised gastric biopsy specimens obtained at the initial endoscopic procedure. A corollary aim was to determine whether the eradication of H. pylori infection in patients with more advanced OLGA stages could reduce or eliminate the risk for GC.
Patients and methods
Patients at enrolment (T-0)
This prospective follow-up study included a cohort of 1755 patients with dyspepsia who underwent an initial (T-0) oesophagogastroduodenoscopy (EGD) between 2011 and 2013 at the Gastroenterology Department of the Rovereto Hospital, a county hospital located in a subalpine region of Northeastern Italy with a regional GC incidence (standardised on world population) of 8.6/100 000/year. Patients were referred by their community-based general practitioners and evaluated by the hospital gastroenterologists. All procedures were conducted under oropharyngeal anaesthesia in patients sedated with midazolam by two experienced endoscopists (AM and CP) using Olympus videoscopes (Model GIF-HQ190).
All patients stopped proton pump inhibitors (PPI) therapy (if any) at least 10 days before the endoscopy procedure. Adult patients (ie, aged 18 years or older) who agreed to participate and provided informed consent were included if they had no previous gastro-oesophageal surgery of any kind and no neoplastic gastro-oesophageal lesions either by history or detected by the initial (T-0) EGD.
Biopsy protocol
Gastric biopsy specimens were obtained according to the Updated Sydney System protocol (two samples from the oxyntic mucosa, two samples from the antral mucosa and one sample from the incisura angularis).40 Specimens from each patient were submitted to the pathology department in two separate 10% formalin jars, one containing the samples from the corpus and one from the antrum and incisura angularis.17
H. pylori status
Patients were stratified into the following categories according to their H. pylori status: (1) H. pylori-positive, when histopathological examination (Giemsa stain modified for H. pylori) revealed the typical curved bacteria in the gastric mucosa; (2) naïve H. pylori-negative, when no active infection was documented histologically and no history of eradication therapy was reported; and (3) H. pylori-eradicated, when there was a documented history of eradication either before the patient’s enrolment or during the period of the present study. At enrolment, H. pylori eradication therapy was recommended to all the H. pylori-positive patients.
Histopathology report
In all cases, the histology report included the gastritis OLGA stage assessed according to the OLGA 2008 guidelines tutorial.17 37 The Padova International classification was used to classify the histological spectrum of neoplastic lesions into three major categories: (1) low-grade IEN (LG-IEN), (2) high-grade IEN (HG-IEN) and (3) invasive adenocarcinoma. Invasive GCs were staged pathologically according to the current WHO criteria.23 32
The interobserver consistency (two pathologists, one local and the other belonging to the coordinating centre) in assessing the gastritis stage and the IEN grade was evaluated on a representative biopsy set of 73 cases using k statistics.41 The k value was 0.69 (95% CI 0.46 to 0.92) for gastritis stage and 0.65 (95% CI 0.41 to 0.88) for the IEN grade. Both k values represented ‘substantial agreement’.
Follow-up (T-1)
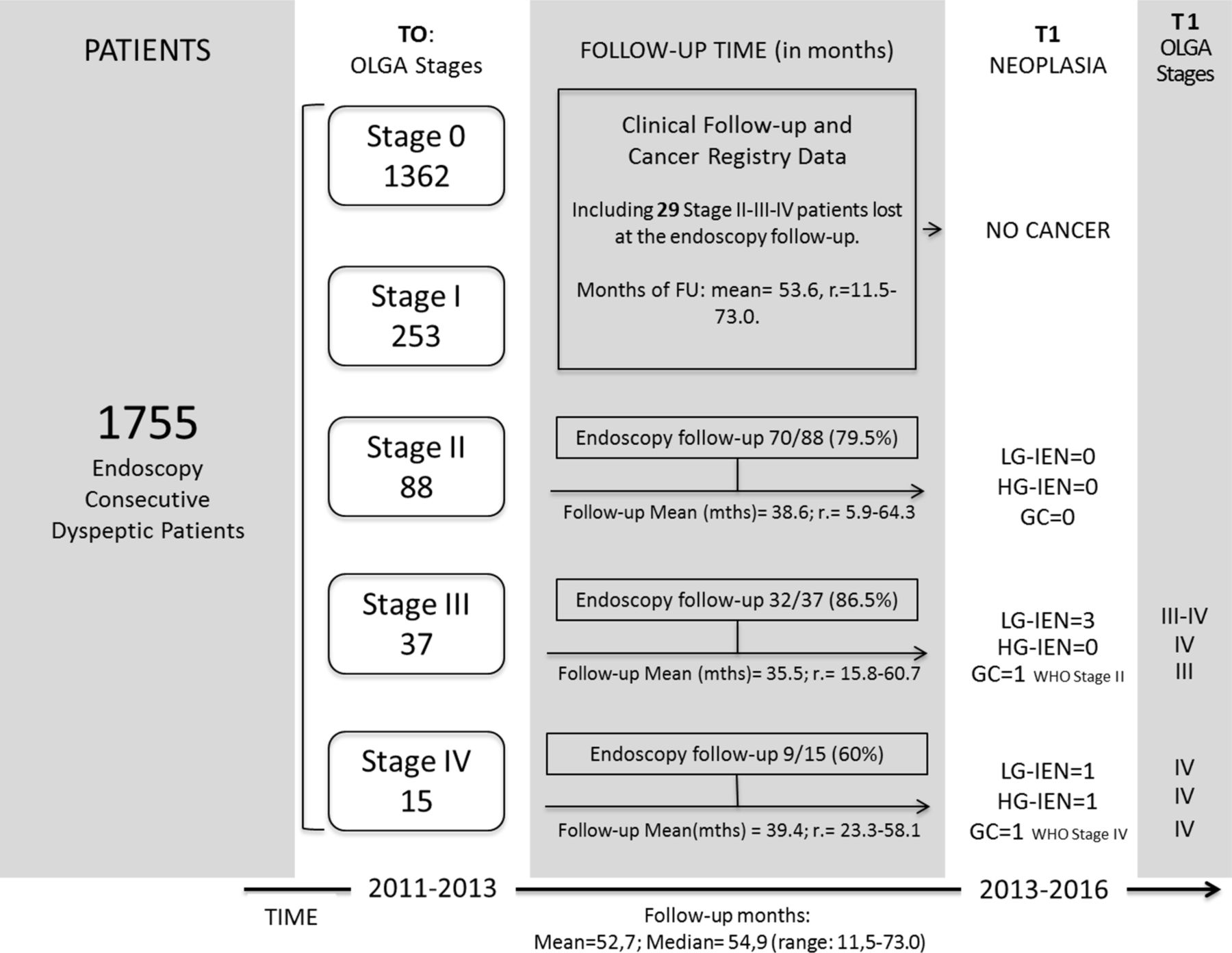
The follow-up schedule, established according to the gastritis stage, is detailed below. Figure 1 shows patients’ distribution by gastritis stage at both T-0 and T-1 (time of the last endoscopy). The adherence to the follow-up schedule by gastritis stage is also shown together with the follow-up times. All patients involved in the endoscopy follow-up (stages II, III and IV) underwent at least two endoscopy procedures. In total, 254 endoscopic procedures were performed. As for the 25 patients who underwent more than two endoscopies, only the initial (T-0) and the last procedures (T-1) were considered.

The figure shows the patients’ distribution by stage at enrolment (T-0) and at the end of the follow-up ((T-1) only for the 111 patients who underwent check-up endoscopy). The prevalence of neoplastic lesion is also shown together with the stage of gastritis at the time of the neoplasia’s detection. FU, follow-up; GC, gastric cancer; HG-IEN, high-grade intraepithelial neoplasia; LG-IEN, low-grade intraepithelial neoplasia; OLGA, operative link on gastritis assessment; mths, months; r, range.
Gastritis stages 0–I
For ethical reasons and according to current guidelines, no endoscopy follow-up was recommended to patients with gastritis stage 0 or I. At the end of the study (December 2016), the clinical history of all these patients was reassessed. In addition to inviting each patient for a clinical evaluation and a complete history, their referring physicians were interviewed, the regional hospital discharge records were searched, and regional cancer and death registries, available from the Regional Healthcare System, were consulted. Endpoints searched for included any gastric epithelial malignancy (including intraepithelial) and non-epithelial gastric neoplasia. Any GI clinical events were also noted.
Gastritis stages II, III and IV
Patients harbouring stage II gastritis were asked to undergo a follow-up endoscopy 2 years after the initial endoscopy. Patients with stage III or IV gastritis were asked to undergo endoscopy 1 year after the initial procedure. The protocol of biopsy sampling was the same adopted at the initial (T-0) endoscopy; additional biopsy samples were obtained from any visible focal lesion.
Vital status
The vital status of all patients was assessed through record linkage with the population file of residents, as available from the Regional Healthcare System. Each patient accumulated person-time for follow-up analysis from the date of enrolment to the date of gastric neoplasia incidence, death, emigration or last available follow-up (ie, 31 December 2016), whichever came first.
Statistical methods
The Χ2 test was used to assess the difference in proportions and the one-way analysis of variance to assess the difference in means among OLGA stages. Somers’ D test was used to measure the ordinal association between histology at T-0 and at T-1.
The low number of neoplastic events that emerged at the end of the follow-up (7/1755) prevented the use of multivariate analyses by applying the Cox proportional hazards model. Therefore, only Kaplan-Meier analysis was performed to compare the incidence of neoplasia in patients with T-0 stages 0–II with the incidence in patients with T-0 stages III and IV.
All P values are two-sided; P values of less than 0.05 were considered significant. All statistical analyses were performed using SAS V.9.4.
Results
Patients’ population at enrolment (T-0) and follow-up times
The study included 1755 consecutive patients with dyspepsia (mean age=52.7, range=18–88; there were 789 men and 966 women, with a male to female ratio (M:F) of 0.82). Patients’ distribution by stage at T-0 is depicted in table 1. The largest group of patients had stage 0 gastritis (1362 subjects; 77.6%), followed by stage I (253 subjects; 14.4%) and stage II (88 subjects; 5.1%). There were 37 patients with stage III (2.1%) and 15 patients (0.85%) with stage IV. Thus, the total number of patients with a high-risk stage (III–IV) was 52 (2.9% of the entire study population (T-0)).
Patient demographics by OLGA stage at enrolment (T0)
Table 2 shows the M:F ratio, the mean age with its range and the H. pylori status mean age of the patients increased significantly from stage 0 to stage IV (P<0.001). Women were more represented in low-risk stages (0, I and II), with an M:F of 0.81. The ratio increased slightly for stage III (0.85), while there were twice as many men as women in stage IV (M:F=2).
Patient demographics, Helicobacter pylori status and diagnosed neoplasia by OLGA stage, at enrolment (T0) and at the end of the follow-up (T1)
At T-0, 603 patients (34.4%) had active H. pylori infection and 220 (12.5%) had a documented history of H. pylori eradication; there were 932 (53%) H. pylori-naïve negative patients. Thus, 46.9% of all patients had either documented active or past H. pylori infection. The H. pylori prevalence in patients stratified by OLGA stage is depicted in table 2.
The mean and median follow-up time of the 1755 patients was 52.7 and 54.9 months, respectively (range: 11.1–73.0). The mean and median follow-up time of the 1644 patients who were clinically followed up was 53.6 and 55.6 months, respectively (range: 11.5–73.0). Among the 111 patients who underwent endoscopic follow-up, the mean and median follow-up time was 37.8 and 37.1, respectively (range: 11.1–64.3).
Clinical follow-up (T-1)
According to the current international guidelines and because of ethical considerations,25 27 no endoscopic follow-up was recommended to patients with stage 0–I gastritis (in total 1615 subjects). Twenty-nine of the 140 (20.7%) patients with stage II, III or IV (18, 5 and 6 cases, respectively) at T-0 were lost to follow-up (see below). The information on the clinical outcome of these patients was obtained by interviewing the patients or their referring physicians, and by checking different records as outlined above. The mean follow-up time of these 1644 patients was 53.6 months (range: 11.5–73.0). Among these patients, no epithelial gastric malignancies were identified over the study period. Available records documented two incident cases of GI stromal tumours (GISTs) and one case of schwannoma.
Follow-up endoscopy (T-1)
Among the 140 patients with stage II, III or IV at T-0, 111 (79.3%) underwent the endoscopic follow-up with biopsy sampling. Among the 29 patients who did not undergo endoscopy (mean and median time of clinical follow-up=48.0 months and 54.9 months, respectively; range: 10–73), no neoplastic lesions were diagnosed clinically. The M:F ratio, mean age and mean follow-up time of the 111 patients who underwent follow-up endoscopy are shown in table 2. Table 2 also depicts the H. pylori status of this cohort at the end of the follow-up period.
Gastritis outcome by OLGA stages
Table 3 shows the results of the follow-up endoscopy of patients with stages II, III and IV gastritis at T-0. The gastritis stage remained unchanged in 54 of the 111 patients (37 stage II, 14 stage III and 3 stage IV).
Patients’ distribution (111 subjects) by OLGA stage at either their initial and at the final endoscopy/biopsy check-up
All 70 patients enrolled with stage II were H. pylori-negative at T-1 (table 2); among these patients, 13 had progressed to stage III and 20 had regressed to stages 0–I (table 3). None of these 20 patients who regressed were H. pylori-positive at T-0; 17 had H. pylori eradication during the study period; and 3 were H. pylori-naïve.2 7 10
Of the 32 patients with stage III at T-0, 3 progressed to stage IV. All three had been successfully treated for H. pylori between T-0 and T-1. Regression from stage III to stage II was documented in 10 patients, and from stage III to stage I in 5 patients (no regression to stage 0 was observed). All of these 15 patients had documentation of H. pylori eradication (tables 2 and 3).
There were nine patients enrolled as stage IV: two of them regressed to stage III, and four regressed to stage II. In eight of these patients H. pylori eradication was successful between T-0 and T-1. Of note, one of the two cases who regressed from stage IV to stage III showed a synchronous LG-IEN at T-1.
By categorising cases according to their clinicopathological behaviour (regression or unchanged vs progression), a significantly more favourable behaviour (P=0.0002) was associated with stage II (low-risk) compared with stages III and IV (high-risk). No neoplastic lesions occurred in patients with stages 0, I and II at enrolment (table 2).
Incident neoplasia (T-1)
Neoplastic lesions developed exclusively in patients enrolled as stages III and IV who underwent follow-up for a total of 159.6 person-years. Overall, seven incident neoplastic lesions were documented (LG-IEN=4 cases; HG-IEN=1 case, GC=2 cases; incident neoplastic lesions=0.4%) (tables 2 and 3). All neoplastic lesions occurred in patients with extensive atrophy (stages III=4 cases; stage IV=3 cases). All incident neoplasias were detected in H. pylori-eradicated patients, with no neoplasia identified in H. pylori-naïve patients. Three of the seven patients who developed neoplasia (2 LG-IEN and 1 HG-IEN) had been H. pylori-positive at T-0 and successful eradication was documented histologically at the T-1 follow-up. Both locally invasive cancers (T (pTNM) values: 2, and 3) were of the intestinal type.
Among the seven patients who developed neoplastic lesions, the mean time elapsed between enrolment (T-0) and the documentation of a neoplastic lesion (T-1) was 31 months (median 24; range 23–49). The mean age of the patients who developed neoplastic lesions was 66.9 (range: 61–77). Of note, among the 37 patients enrolled with a stage III gastritis, 14/37 were 60 years old or younger, and none of them developed neoplastic events. Among the 23/37 subjects older than 60, at the end of the follow-up 4/23 neoplastic lesions were documented (incidence=60.0 per 1000 patient-years). Additionally, no patients younger than 60 years were included in stage IV.
The risk of developing neoplastic lesions significantly varied with the baseline stage of gastritis, being null in patients with stages 0, I and II (95% CI 0 to 0.4), 36.5 per 1000 person-years in patients enrolled with stage III (95% CI 13.7 to 97.4) and 63.1 per 1000 person-years in those enrolled with stage IV (95% CI 20.3 to 195.6). Figure 2 shows the neoplastic risks associated with the OLGA stages at enrolment (P<0.0001), when patients were stratified into low-risk (0, I and II) and high-risk (III and IV) stages.

{kind=link}
{kind=link}
Kaplan-Meier analysis of the proportion of patients who developed gastric neoplastic lesions distinguished by the gastritis OLGA stage at their enrolment (T0). Stages 0, I and II versus stages III–IV (P<0.0001).
Discussion
In 2017, about one million new cases of GC will be diagnosed worldwide; most of them will be in an advanced stage, with an expected 5-year survival of less than 25%.1 More than 90% of these malignancies will arise in patients with current or past H. pylori infection, mostly in a background of gastric mucosal atrophy.3
H. pylori is the central aetiological agent of gastric atrophy, which is in turn the background on which most non-syndromic GCs arise.2 3 14 32 42 On this solid evidence, the staging of gastritis, a semiquantitative assessment of the extent and topography of gastric atrophy, has received wide acceptance for stratifying patients according to their predicted cancer risk.18 32 33 The evidence supporting the clinical reliability of this staging approach was mostly derived from retrospective cohort studies, in which the prognostic impact of gastritis staging was only retrospectively validated. These early experiences provided an invaluable body of unimpugnable evidence on which the recommendations to use one of the two staging systems (OLGA and operative link for gastric intestinal metaplasia assessment (OLGIM)) are founded.8 9 26 27
The current study is the first to apply the OLGA stage in a prospective manner: our cohort of 1755 consecutive patients with dyspepsia was recruited between 2011 and 2013 in the gastroenterology unit of a subalpine Italian region hospital specifically for the purpose of this study; all gastric biopsies were taken according to protocol and OLGA staged at the time of the initial diagnosis. This was crucial to determine how each patient should be followed, since both ethical considerations and current clinical guidelines clearly indicate that patients with no or minimal gastric mucosal atrophy (OLGA stages 0 and I) should not undergo further invasive diagnostic procedures.
This approach, to which no alternatives existed, resulted in a lack of direct histopathological information on the evolution of the gastric mucosa in low-risk stage patients and could be seen as a shortcoming of the study. However, this was offset by the combination of a stable community, a reliable interconnected network of primary care providers and gastroenterologists in the region, and by the central registries maintained at the Regional Healthcare System. Using a multifaceted approach involving interviews with patients and their providers, perusal of the centralised registries, and review of each patient’s discharge summaries from any regional hospitals where they may have been admitted during the study period, we could confidently determine that none of the patients who did not undergo follow-up endoscopy had gastric events or had a diagnosis of any relevant gastric epithelial lesion. An indirect confirmation of the accuracy of our extensive (multifaceted) enquiries was the finding of three cases of non-epithelial malignancies (two GISTs and one schwannoma) that were diagnosed in the low-risk stage population. Admittedly, however, we may still have missed the development of lesions occurring in asymptomatic patients who did not seek medical attention.
The patients’ distribution by stage at enrolment was basically comparable with that reported in other studies conducted in both similar34–36 and different30 38 39 epidemiological contexts. The number of patients significantly decreased with each increasing stage (from 78% at stage 0 to 1% at stage IV), while both age and M:F ratio increased, particularly in stage IV. This pattern is consistent with both the biological concept of multistep gastric oncogenesis (ie, cancer risk increasing along with age) and the epidemiological profile of the gastric preneoplastic and neoplastic lesions.32 33 Among patients enrolled as stage III, neoplastic events (4) only developed in subjects older than 60 years old, and all patients enrolled as stage IV were older than 60: these features would qualify the seventh decade as that at elective cancer risk; prudentially, the number of the considered patients would suggest caution in accepting 60 as ‘discriminant’ age.
Atrophy either regressed or did not progress in 57 of the 70 (81%) T-0 stage II patients who underwent endoscopic follow-up, but progressed to stage III in 13 patients (18%). Among the 32 patients enrolled as stage III, a downstaging to low-risk stages occurred in 15 cases (47%), while 4 of 9 patients (44%) enrolled as stage IV regressed to a low-risk stage. Overall, 7 of 41 patients with a T-0 stage of III or IV (17%) developed neoplasia. All of these changes occurred in patients who had been successfully treated for H. pylori. These findings support the statement, as expressed in section 4 of the Kyoto Global Consensus Report, that while eradication therapy is beneficial in both low-risk and high-risk stages ‘it cannot completely reset the clock to zero’ (ie, it does not nullify the GC risk induced by the previous long-standing infection).26 43–46
Three possible shortcomings of our study need to be considered. First, we assessed the presence of H. pylori by histology only, a method that has a reduced sensitivity in the presence of extensive intestinal metaplasia. Therefore, it is possible that a small proportion of the patients we classified as H. pylori-eradicated might still have been harbouring H. pylori in (non-sampled) non-intestinalised mucosa. Second, as in all situations that depend on the limited sampling of a wide process, we cannot exclude the possibility that, in some instances, cases interpreted as regression or progression were related to sampling error. The third limitation is the lack of the multivariate analysis (Cox regression analysis) in evaluating the risk of gastric neoplasm due to the structural limit represented by the small number of the neoplastic events encountered during the follow-up. The wider use of high-magnification endoscopy (an accurate method for the detection of atrophy) will potentially improve the sensitivity of the atrophy assessment by combining endoscopy with histological staging.47
At the end of the follow-up (T-1), the overall prevalence of neoplastic lesions was 0.4% and all cases of neoplastic progression were detected in patients who had high-risk stages at enrolment. The risk of developing neoplastic lesions varied significantly with the baseline stage of gastritis, being null in patients with stages 0, I and II, 36.5 per 1000/year in patients enrolled with stage III, and 63.1 per 1000/year in those enrolled with stage IV. These data confirm the clinical and ethical priority of offering endoscopic follow-up to patients in high-risk OLGA stages (III and IV) after H. pylori eradication, and provide further support for the guidelines of the Kyoto Global Consensus Report on H. pylori gastritis.26
Our data do, however, suggest that the 3-year interval for patients with antrum-to-corpus spreading gastric atrophy (recommended by the Management of Precancerous Conditions and Lesions in the Stomach and other national guidelines25 27) may be too long. In our series, the shortest interval between enrolment and the detection of neoplasia was 23 months (in a patient who enrolled with stage III gastritis). Thus, it might be prudent to offer patients a follow-up endoscopy 24 months after the initial diagnosis of a high-risk stage (and the age older than 60 could be also included among the ‘alerting-clinical-situations’).
In summary, this long-term prospective study of a clinically and epidemiologically well-defined stable cohort of 1755 patients with dyspepsia has achieved three major goals. First, it confirms that OLGA staging provides a standardised easy-to-interpret diagnostic format, and more importantly it is a reliable predictor of the risk for gastric epithelial neoplastic lesions, including GC. Second, it shows that over a period of 5 years, no neoplastic lesions emerged in H. pylori-naïve patients, providing further support for the leading role of H. pylori in gastric carcinogenesis. Finally, it provides evidence that the eradication of H. pylori in high-stage patients cannot abolish the risk for neoplastic progression.43 45 This latter finding needs to be evaluated in other epidemiological contexts, where both host and environmental factors (including the modulation of the microbiota) may affect the neoplastic risks.31 48–50
Acknowledgments
The authors are grateful to Stefano Guzzinati (Veneto Tumor Registry) for his critical evaluation of the statistical analysis. The authors also thank Silvano Piffer (Head of the Trento Tumor Registry) for his supportive collaboration.
References
Footnotes
MR and AM contributed equally.
Contributors Study concept and design: MR, AM, GDP; acquisition of data: AM, CP, MB, MF, GDP; analysis and interpretation of data: MR, AM, MG, MZ, DYG, RMG; drafting of the manuscript: MR, AM, DYG, RMG; statistical analysis: MG, MZ; obtained funding: MR.
Funding This work was partly supported by a grant from the Italian Association for Cancer Research (AIRC regional grant n. 6421 to MR).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.