Article Text

Abstract
Background White light endoscopy with random biopsies is the standard for detection of intestinal metaplasia (IM) and neoplasia in patients with Barrett's oesophagus (BO). Narrow band imaging (NBI) highlights surface patterns that correlate with IM and neoplasia in BO.
Objective To compare high-definition white light (HD-WLE) and NBI for detection of IM and neoplasia in BO.
Design International, randomised, crossover trial comparing HD-WLE and NBI. Patients referred for BO screening/surveillance at three tertiary referral centres were prospectively enrolled and randomised to HD-WLE or NBI followed by other procedures in 3–8 weeks. During HD-WLE, four quadrant biopsies every 2 cm, together with targeted biopsies of visible lesions (Seattle protocol), were obtained. During NBI examination, mucosal and vascular patterns were noted and targeted biopsies were obtained. All biopsies were read by a single expert gastrointestinal pathologist in a blinded fashion.
Results 123 patients with BO (mean age 61; 93% male; 97% Caucasian) with mean circumferential and maximal extents of 1.8 and 3.6 cm, respectively, were enrolled. Both HD-WLE and NBI detected 104/113 (92%) patients with IM, but NBI required fewer biopsies per patient (3.6 vs 7.6, p<0.0001). NBI detected a higher proportion of areas with dysplasia (30% vs 21%, p=0.01). During examination with NBI, all areas of high-grade dysplasia and cancer had an irregular mucosal or vascular pattern.
Conclusions NBI targeted biopsies can have the same IM detection rate as an HD-WLE examination with the Seattle protocol while requiring fewer biopsies. In addition, NBI targeted biopsies can detect more areas with dysplasia. Regular appearing NBI surface patterns did not harbour high-grade dysplasia/cancer, suggesting that biopsies could be avoided in these areas.
- Narrow band imaging
- Barrett's esophagus
- esophageal neoplasm
- esophagoscopy
- image enhancement
- gastroesophageal reflux disease
- low-grade dysplasia
- Barrett's carcinoma
- adenocarcinoma
- Barrett's oesophagus
- endoscopy
- cost-effectiveness
- decision analysis
- colorectal cancer screening
Statistics from Altmetric.com
- Narrow band imaging
- Barrett's esophagus
- esophageal neoplasm
- esophagoscopy
- image enhancement
- gastroesophageal reflux disease
- low-grade dysplasia
- Barrett's carcinoma
- adenocarcinoma
- Barrett's oesophagus
- endoscopy
- cost-effectiveness
- decision analysis
- colorectal cancer screening
Significance of this study
What is already known about this subject?
-
Oesophageal surface patterns visualised with narrow band imaging (NBI) can be used to predict the presence of intestinal metaplasia and dysplasia.
-
The exact clinical utility of NBI in patients with Barrett's oesophagus (BO) undergoing screening and surveillance endoscopy has not been established.
What are the new findings?
-
When compared with high-definition white light endoscopy, NBI detected the same number of patients with intestinal metaplasia but with fewer biopsies.
-
NBI detected a higher proportion of areas with dysplasia.
-
Regular appearing NBI surface patterns did not harbour high-grade dysplasia/cancer.
-
The accuracy of NBI for the detection of low-grade dysplasia is low.
How might it impact on clinical practice in the foreseeable future?
-
The use of NBI targeted biopsies may improve the efficiency of BO endoscopic screening and surveillance of BO.
-
Biopsies could be entirely avoided in patients who have only regular appearing NBI surface patterns.
Introduction
Endoscopic screening and surveillance has been the foundation in the management of Barrett's oesophagus (BO) and is practised by the majority of endoscopists in the USA and Europe.1–3 BO is the only known precursor lesion to oesophageal adenocarcinoma (OAC), the cancer with the fastest rising incidence in the Western world.4 Previous studies of BO screening and surveillance have had conflicting results, specifically with regards to the efficacy in detection of intestinal metaplasia (IM) and dysplasia and reduction in OAC mortality attributed to surveillance.5–7 Guidelines from gastroenterology societies recommend endoscopic surveillance of BO using white light endoscopy (WLE) with targeted biopsies of any endoscopically visible lesions and random four quadrant biopsies every 2 cm of the BO segment (Seattle protocol).8 ,9 However, this protocol has several limitations. Dysplasia and early OAC in patients with BO result in subtle changes that may not be visible during WLE examination. In addition, random biopsies have significant sampling error since IM and dysplasia have a patchy distribution and only a small fraction of the BO segment is biopsied. As a result, techniques to improve the efficacy of screening and surveillance strategies are highly desirable.
Narrow band imaging (NBI) is a recent advance in endoscopic technology, which uses spectral narrow band filters (red, green and blue bands) that allow for visualisation of oesophageal mucosal and vascular patterns, similar to chromoendoscopy without the time or expense of spraying dye. In addition, the narrow band filters can be turned on and off with the push of a button on the endoscope, enabling examination with WLE as well. In a study of 51 patients with known or suspected BO, images obtained using NBI were graded according to the mucosal (ridge/villous, circular and irregular/distorted) and vascular patterns (normal and abnormal) and correlated with histology in a prospective and blinded manner.10 The sensitivity and specificity of the ridge/villous pattern for the diagnosis of IM without high-grade dysplasia (HGD) were 93.5% and 86.7% and that of the irregular/distorted pattern for HGD were 100% and 98.7%, respectively. A recent meta-analysis of eight studies (446 patients, 2194 areas) reported an overall sensitivity and accuracy for detecting IM using NBI of 95% and 65%, respectively.11 The same study found a sensitivity and specificity for detection of HGD of 96% and 94%, respectively. However, the exact clinical utility of NBI in patients with BO undergoing screening and surveillance endoscopy has not been established.
The aim of this prospective, international, randomised controlled trial, was to compare high-definition white light endoscopy (HD-WLE) using the standard Seattle biopsy protocol with NBI targeted biopsies in patients with BO with respect to (1) the proportion of patients with IM and neoplasia; (2) the proportion of neoplastic areas and (3) the number of overall biopsies performed.
Patients and methods
Patients and study protocol
This was a multicentre, randomised, crossover trial comparing HD-WLE and NBI for the detection of IM and neoplasia in patients with BO. After obtaining written and informed consent, patients over the age of 18 undergoing screening or surveillance for BO were prospectively enrolled at three tertiary referral centres (Veterans Affairs Medical Center in Kansas City, Medical University of South Carolina and Amsterdam Medical Center). The institutional review boards at all three participating sites approved the study protocol and the trial was registered at clinicaltrials.gov (NCT00576498). Patients with erosive oesophagitis, grossly visible nodules or lesions (>5 mm) within the BO segment suggestive of invasive OAC and those with contraindications to oesophageal biopsies such as anticoagulation or varices were excluded. Patients with BO length <1 cm were also excluded as previous studies have documented poor interobserver agreement in diagnosing BO of this length.12
Patients meeting the inclusion criteria were randomised to undergo upper endoscopy with either HD-WLE or NBI on day 1. Patients were randomised in a 1:1 ratio using a computer-generated list of random numbers and administered by study coordinators in sealed opaque envelopes that were opened after patient enrolment and immediately before the first study procedure. The same patient then returned for the alternative procedure performed by a different endoscopist within 3–8 weeks. During this time interval, all patients were maintained on twice a day proton pump inhibitor therapy with the aim of healing the biopsy sites. Every attempt was made to keep the performing endoscopists blinded to the patient's previous endoscopy and biopsy results (ie, non-dysplastic BO, low-grade dysplasia (LGD), HGD, OAC). The patient was excluded from the study if the performing endoscopist became aware of the patient's previous endoscopy or biopsy results before or during any study procedure.
Study procedures
All patients were sedated according to standard protocols at each centre and every study procedure was performed by endoscopists with extensive experience in NBI. Study endoscopies were performed using a high-definition endoscope with NBI capability (Olympus GIF-H180, Center Valley, Pennsylvania, USA; available at all centres) and all biopsy specimens were taken using standard biopsy forceps (Radial jaw 3; Boston Scientific, Massachusetts, USA). During each endoscopy procedure, the presence and length of the BO was measured using the Prague classification system and the endoscopist carefully inspected the BO segment for the presence of any subtle visible lesions using the assigned imaging modality.12
Standard white light endoscopy
Patients were evaluated using HD-WLE during the entire examination (no examination with NBI). After inspection of the BO segment, any endoscopically visible lesions were described, biopsied and placed in separate specimen jars. Afterwards, four quadrant biopsy specimens were taken every 2 cm of the BO segment (Seattle protocol) and placed in separate jars.
Narrow band imaging
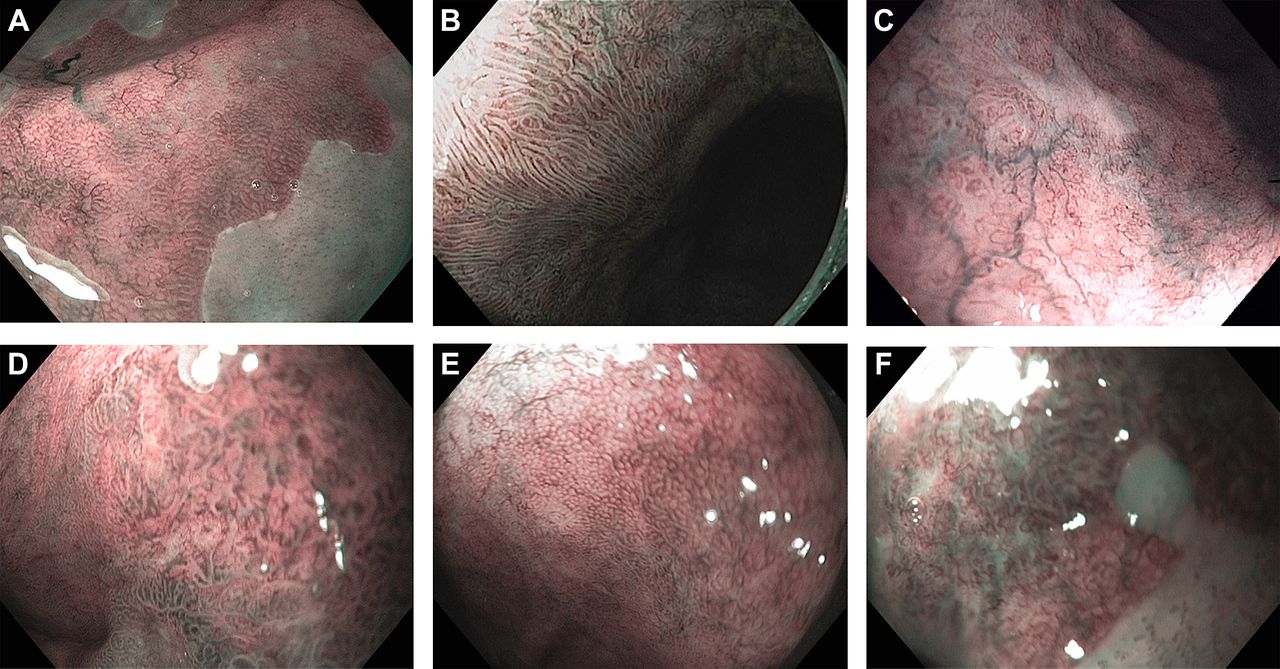
Patients were evaluated with NBI activated during the entire examination (no examination with high-definition white light). NBI mucosal and vascular patterns (figure 1) were standardised between the three study centres, in person, a priori. Based on previous publications, the patterns described and noted were as follows: (a) mucosal—circular, ridged/villous, absent or irregular, (b) vascular—regular or irregular.10 After inspection of the BO segment, any endoscopically visible subtle lesions were described, biopsied and placed in separate specimen jars. Then targeted biopsy specimens were taken from each of the different NBI patterns visualised and placed in separate specimen jars. For example, if only a ridge/villous mucosal pattern was identified in a patient, one to two target biopsies were obtained; if more than one pattern was noted, one to two additional target biopsies were obtained and placed in separate jars for each pattern identified.

Examples of the different oesophageal surface patterns seen during examination with narrow band imaging: (A) Circular mucosal pattern. (B) Ridged/villous mucosal pattern. (C) Absent mucosal pattern. (D) Irregular mucosal pattern. (E) Regular vascular pattern. (F) Irregular vascular pattern.
Histology
All biopsy specimens at all three centres were embedded in paraffin, stained with haematoxylin and eosin and then reviewed by a single expert gastrointestinal pathologist (SCM) who was blinded to the endoscopy results (including NBI patterns). The degree of dysplasia was classified as no dysplasia, LGD, HGD and adenocarcinoma according to the revised Vienna classification of gastrointestinal neoplasia.13
Study outcomes
The primary outcome was the proportion of patients with biopsy-confirmed IM. Secondary outcomes included the proportion of patients with dysplasia/cancer, proportion of areas with dysplasia and/or cancer and number of biopsies obtained using each procedure.
Data collection and statistical analysis
Patient demographics, order of randomisation, endoscopy findings (BO extent, hiatal hernia length, presence of subtle visible lesions, NBI patterns), number of biopsies and corresponding histology reports were collected and recorded by the study coordinators. All of the study information was stored in a centralised database.
Statistical analysis was performed using Stata/IC V.10.1 (StataCorp) and was done using a ‘per protocol’ method. McNemar's test was used to compare paired categorical data while continuous paired data were compared using a paired t test. The Stuart–Maxwell test was used to evaluate marginal homogeneity of paired categorical data when more than two outcomes were possible. Non-paired categorical and continuous data were compared using Fisher's exact test and an unpaired t test, respectively. A p value of <0.05 was considered significant.
Sample size
We assumed that examination using HD-WLE with biopsies according to the Seattle protocol could diagnose IM in 70% of patients while NBI targeted biopsies could diagnose IM in 90% of patients. Based on these detection rates, we calculated that we would need 122 patients to give 80% power to detect a significant difference between HD-WLE and NBI (with a type I error rate of 5%) using McNemar's test for paired dichotomous responses.
Results
Patient demographics and characteristics
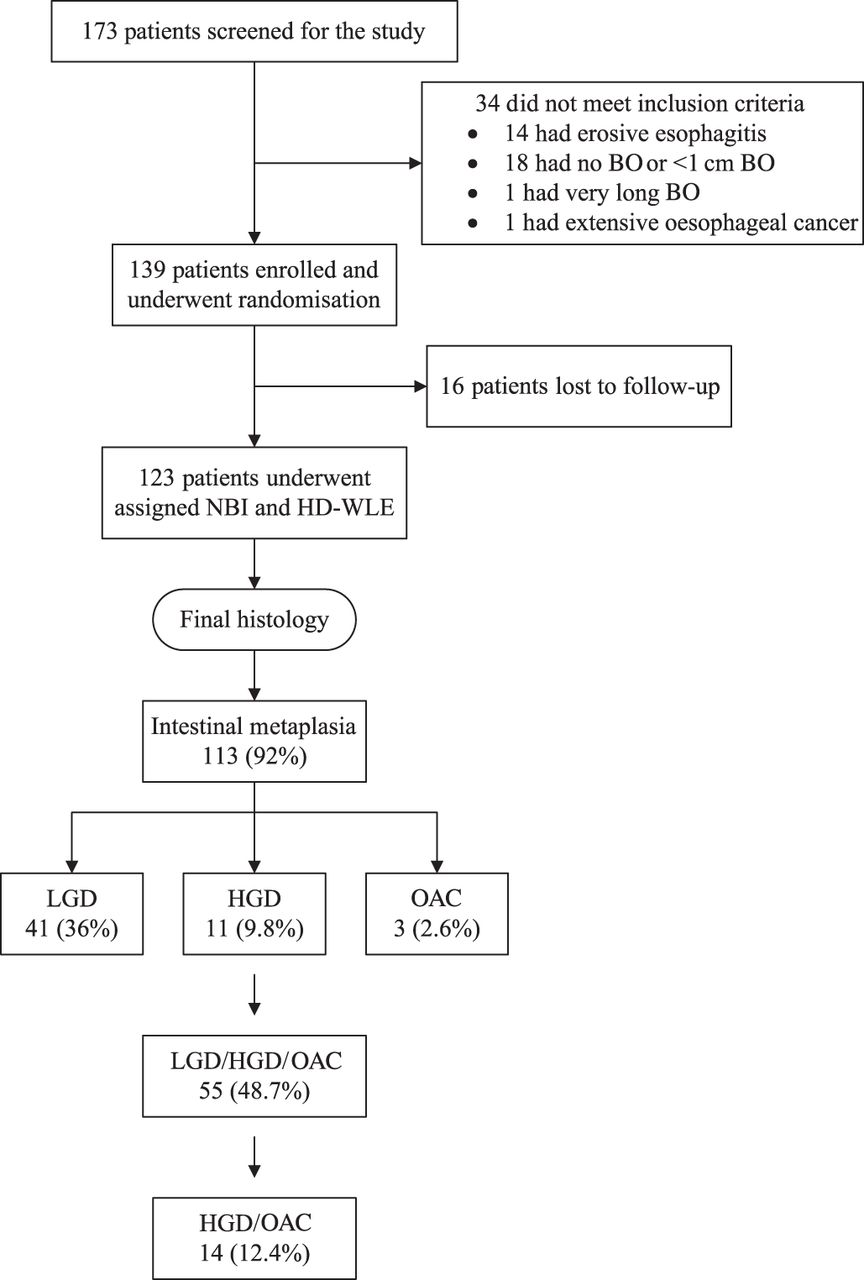
From October 2005 to April 2009 a total of 173 patients were prospectively enrolled in the study. Fifty patients were excluded for reasons highlighted in figure 2. Of the 123 patients included in the final analysis (67 Veterans Affairs Medical Center in Kansas City, 39 Amsterdam Medical Center, 17 Medical University of South Carolina), 115 (93%) were male, 119 (97%) were Caucasian and the mean age was 61 years (range 38–85). The mean extent of BO was 1.8 cm (range: 0–13 cm) for circumferential (C) extent and 3.6 cm (range: 1–14 cm) for maximal extent (M). A total of 117 (95%) patients had a hiatus hernia and the mean hiatal hernia size was 2.5 cm (range 1–10 cm).
{kind=link}
{kind=link}
Flow chart of patients eligible for study enrolment. BO, Barrett's oesophagus; OAC, oesophageal adenocarcinoma; HD-WLE, high-definition white light endoscopy; HGD, high-grade dysplasia; LGD, low-grade dysplasia; NBI, narrow band imaging.
Final diagnosis was defined as the overall worst histology found using either imaging technique (HD-WLE or NBI). IM was detected in 113 (92%) patients. Of the 113 patients with IM, the final diagnoses were as follows: 58 (51%) non-dysplastic BO, 41 (36%) LGD, 11 (9.8%) HGD and 3 (2.6%) OAC.
Overall detection of intestinal metaplasia: patient-based analysis
A comparison of HD-WLE with NBI (targeted and random biopsies for HD-WLE and targeted biopsies for NBI) showed no difference in the number of patients found to have IM. Both imaging techniques correctly identified 104/113 (92%) patients each with IM (p=NS). Each technique missed IM in nine patients where it was detected by the subsequent technique. Of the patients with IM missed by NBI examination, six had ridged/villous mucosal and normal vascular patterns, one had circular mucosal and normal vascular patterns, one had absent mucosal and abnormal vascular patterns and one had ridged/villous mucosal and abnormal vascular patterns.
A total of 934 biopsies (46 targeted and 888 random) were obtained during HD-WLE examination compared with 442 targeted biopsies during NBI examination. While there was no difference in the detection of patients with IM, NBI examination required significantly fewer biopsies than HD-WLE (HD-WLE: mean 7.6/patient vs NBI: mean 3.6/patient, p<0.0001).
Overall detection of dysplasia: patient-based analysis
Table 1 shows the distribution of patient histology based on each imaging modality. In 68 patients, HD-WLE and NBI obtained the same histological diagnosis. In 33 patients NBI detected a higher grade of neoplasia than HD-WLE, while in 22 patients HD-WLE detected a higher grade of neoplasia (table 1; marginal heterogeneity p=0.44). When HGD and OAC were combined into one histological diagnosis category, there continued to be no statistically significant difference in the number of patients with more severe grades of neoplasia between NBI and HD-WLE (marginal heterogeneity p=0.63). Two patients with HGD/OAC were found by HD-WLE without four quadrant biopsies, seven patients with HGD/OAC were found by four quadrant biopsies during HD-WLE examination only and 12 patients with HGD/OAC were found by targeted (from areas with either a macroscopically visible lesion or abnormal vascular, absent mucosal, or irregular mucosal pattern) biopsies by NBI. Of the 14 patients with LGD detected by HD-WLE but with either no IM or IM by NBI, two patients had irregular mucosal and abnormal vascular patterns, nine had ridged villous mucosal and normal vascular patterns, two had circular mucosal and normal vascular patterns and one had an absent mucosal and abnormal vascular pattern. Of the two patients with HGD detected by HD-WLE but with IM and LGD by NBI, one had an irregular mucosal pattern and an abnormal vascular pattern and one had an absent mucosal pattern and regular vascular pattern.
Overall histological yield of HD-WLE and NBI
Detection of dysplasia: area-based analysis
A total of 267 areas were examined and biopsied during NBI examination compared with 321 during HD-WLE. There was no difference in the proportion of areas with HGD and OAC detected by HD-WLE or NBI (HD-WLE: 13 (4%) vs NBI: 19 (7%), p=0.1). For the detection of any neoplasia (LGD/HGD/OAC), NBI targeted biopsies detected a statistically significant higher proportion of areas with any neoplasia (HD-WLE: 67 (21%) vs NBI: 81 (30%), p=0.01).
Detection of subtle visible lesions
Macroscopically visible lesions were found in more patients during examination with HD-WLE than with NBI (17.1% vs 4.9%, p<0.01). A total of 22 lesions (three elevated surface, two abnormal mucosa, one erosion, three ulcers, nine nodules, one plaque, one stricture and two not specified) were detected in 21 patients during HD-WLE examination and a total of 11 lesions (three ulcers, three nodules and five not specified) were detected in five patients during NBI examination. Sixteen patients had macroscopically visible lesions detected during HD-WLE but not during NBI. Eight of these patients had abnormal mucosal or vascular patterns seen during NBI, although it is unknown whether these were present at the same location (as the HD-WLE findings) owing to the study design. While more macroscopically visible lesions were seen by HD-WLE, the majority of them were non-dysplastic. There was no statistically significant difference in the proportion of dysplastic visible lesions identified by NBI compared with HD-WLE (5/11 vs 6/22, p=0.44).
Characteristics of NBI surface patterns
A total of 267 areas were examined and biopsied with NBI. In three areas (two macroscopically visible lesions), the mucosal pattern was not recorded. The histology of these areas was one IM, one LGD and one HGD. Of the four areas where the vascular pattern was not recorded, three had no mucosal pattern recorded (see above) and one had a ridged/villous mucosal pattern with a final histology of IM.
Table 2 shows the distribution of histology for each combination of mucosal and vascular patterns. IM and LGD were found in areas from all four types of mucosal patterns. Of the 143 ridged/villous mucosal pattern areas, IM was detected in 56% and 17% had LGD. Of the 33 circular mucosal pattern areas, IM was detected in 70% and 9% had LGD. HGD and OAC were only found in areas containing an irregular mucosal pattern.
Distribution of histology for oesophageal surface patterns seen during NBI
Utility of NBI targeted biopsies
Targeted detection of intestinal metaplasia
A total of 393 biopsies targeted for IM (from areas with a macroscopically visible lesion, an abnormal vascular pattern, or ridged/villous, absent, or irregular mucosal pattern) were obtained during examination with NBI. NBI targeted biopsies detected 99/113 (87.6%) patients with IM compared with 104/113 (92%) in the HD-WLE group (p=0.36). The five additional patients who were not detected by NBI targeted biopsies had only circular mucosal and normal vascular patterns. HD-WLE (targeted and random biopsies) had a sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) for the detection of patients with IM of 92%, 100%, 53% and 100%. NBI (targeted biopsies only) had a sensitivity, specificity, NPV and PPV for the detection of patients with IM of 87.6%, 100%, 41.7% and 100%.
Targeted detection of dysplasia
A total of 152 biopsies targeted for dysplasia (from areas with either a macroscopically visible lesion or abnormal vascular, absent mucosal, or irregular mucosal patterns) were obtained during examination with NBI. Comparison of these NBI targeted biopsies alone with both targeted and random biopsies for HD-WLE showed that NBI did not detect more patients with higher grades of neoplasia. In 65 patients NBI and HD-WLE obtained the same histological diagnosis. In 25 patients NBI detected a higher grade of neoplasia than HD-WLE, while in 33 patients HD-WLE detected a higher grade of neoplasia (table 3; marginal heterogeneity p=0.07). When HGD and OAC were combined into one histological diagnosis category, there continued to be no difference between NBI and HD-WLE (marginal heterogeneity p=0.08).
Histological yield of HD-WLE and NBI targeted biopsies
If NBI targeted biopsies were only obtained from macroscopically visible lesions and areas with either an irregular mucosal pattern or abnormal vascular pattern, then 90 areas would be examined using 152 biopsies. There would be no difference in the total number of areas with HGD or OAC detected in comparison with NBI examination with targeted biopsies obtained from all mucosal patterns. However, 29 fewer areas with LGD would be detected. HD-WLE (targeted and random biopsies) had a sensitivity, specificity, NPV and PPV for the detection of patients with dysplasia of 63.6%, 100%, 77.3% and 100%. NBI (targeted biopsies only) had a sensitivity, specificity, NPV and PPV for the detection of patients with dysplasia of 52.7%, 100%, 72.3% and 100%.
Subgroup analysis: results by centre and Barrett's length
Examination of each study centre's results individually showed that there were no statistically significant differences in the detection of patients with dysplasia between HD-WLE and NBI. However, the study was not powered for the outcome of dysplasia detection. In addition, there were no statistically significant differences in the prevalence of IM or dysplasia between the different centres. Furthermore, during subgroup analysis based on BO length, there was no statistically significant difference in the detection of patients with IM or patients with dysplasia in either the short or the long BO length subgroups. However, NBI examination required fewer biopsies than an HD-WLE examination in both patients with <3 cm disease (3.0 vs 3.9, p=0.02) and ≥3 cm disease (4.1 vs 10.9, p<0.0001).
Discussion
A number of preliminary studies have demonstrated that new imaging techniques including electronic chromoendoscopy (NBI (Olympus America, Center Valley, Pennsylvania, USA), Fujinon Intelligent ChromoEndoscopy (Fujinon Inc, Saitama, Japan), Pentax I-Scan (Pentax Inc, Tokyo, Japan)) disclose specific surface mucosal patterns that correlate with the histological presence/absence of IM (confirming BO during endoscopic screening) and/or dysplasia (diagnosing neoplasia during endoscopic surveillance).10 ,14 However, this is the first randomised, controlled, international, crossover trial that has directly compared the yield of NBI targeted biopsies versus the standard practice of obtaining four quadrant biopsy specimens every 2 cm (Seattle protocol but NBI achieved this with half the number of biopsies.
Screening and surveillance of BO using WLE with random biopsies is the accepted practice and supported by the gastroenterology societies.8 ,9 The frequency of endoscopic surveillance once BO has been confirmed (presence of IM) is determined primarily by the highest grade of dysplasia diagnosed during the biopsy protocol. However, endoscopists often do not follow the recommended biopsy protocol, which is labour intensive and tedious, with one study showing an overall compliance rate of 51.2% in the USA.15 Similar poor adherence rates have also been reported from other countries, with worsening compliance as the length of the BO segment increases.16 Finally, even if performed appropriately, only 4–6% of the BO area is sampled. Given these limitations, several enhancements to our current practice of endoscopic screening and surveillance are desired. As shown in this study, using the commercially available system, NBI did not differ from the currently accepted practice of random four quadrant biopsies for the detection of IM but required significantly fewer biopsies. Although not the primary aim of this study, the use of NBI also led to detection of more neoplastic BO areas than with HD-WLE (30% vs 21%).
Using NBI in patients with BO, different mucosal (regular, round, oval, villous, irregular or abnormal) and vascular (normal, regular, irregular or abnormal) patterns can be recognized, and these patterns have the ability to predict histology. In this study, we have shown that all areas of HGD and/or OAC (areas requiring endoscopic or surgical treatment) had an irregular mucosal/vascular pattern. More importantly, none of the areas showing a regular mucosal/vascular pattern by NBI harboured these lesions suggesting that biopsies could be avoided from such areas, thereby improving the efficiency and costs of BO screening and surveillance endoscopic practices. However, the accuracy of NBI for the detection of LGD was limited.
Only a few randomised controlled trials have compared the efficacy of NBI with either standard endoscopy or other techniques such as chromoendoscopy. In a study by Kara et al, NBI was compared with chromoendoscopy for the detection of HGD or early OAC in 28 patients with BO and showed that the detection achieved by both techniques was comparable.17 However, this study was probably underpowered to detect such a difference. More recently, Wolfsen et al compared NBI with standard resolution WLE in patients with BO undergoing surveillance for previously detected dysplasia and showed a significantly higher rate of dysplasia detection (57% for NBI vs 43% for standard) with fewer biopsies (4.7 per patient vs to 8.,5 respectively; p < 0.001) for NBI.18 The study had a tandem design and used older-generation white light endoscopes and not the high-definition system as used in our study.
Our study does have some limitations. It was conducted in three tertiary BO referral centres with a special interest in BO and the results may not be generalisable. All histology slides were evaluated by a single experienced pathologist and not by consensus and interobserver agreement on the reading of dysplasia was not tested. In order to achieve our secondary aim of comparing the yield of dysplasia/cancer detection between WLE and NBI, we did enrich our patient population with such patients. The study was also not powered to detect a difference in the number of patients diagnosed with neoplasia, and the time required to perform each procedure was not systematically recorded. Although the results in this trial using NBI represent a significant scientific advance compared with HD-WLE, certain challenges still need to be overcome, such as the interobserver variability for pattern recognition with NBI, increased duration and complexity of the procedure, training, lack of reimbursement and the lack of consensus about the interpretation of mucosal and vascular patterns with these techniques. These concerns need to be dealt with in future trials.
In conclusion, the results of this large, international randomised controlled trial show that use of NBI targeted biopsies and the current standard of random four quadrant biopsies diagnosed similar proportions of patients with BO, although NBI could achieve this with significantly fewer biopsies. For screening, NBI with target biopsies can be used for the detection of IM. Use of NBI resulted in the diagnosis of more neoplastic areas than with HD-WLE. Finally, regular appearing NBI surface patterns did not harbour HGD and/or OAC, suggesting that biopsies could be avoided in these areas. However, since this was not the primary goal of our study, the routine use of NBI target biopsies only for detection of HGD/cancer cannot be recommended. These results show that new imaging targeted biopsies have the ability to improve the efficiency of current endoscopic screening and surveillance practices in patients with BO and also reduce costs.
References
Footnotes
Results of this study presented in part at as an oral presentation at Digestive Diseases Week 2009, Chicago, Illinois, USA.
-
Funding This study was funded through an ASGE research award and an investigator initiated grant from Olympus America. The study sponsor had no role in study design, data collection, analysis or interpretation.
-
Competing interests PS has received previous grants/research support from Olympus America Inc, BARRX Medical Inc and Takeda Pharmaceutical Company Ltd. RHH serves as a consultant for Olympus America. PF serves as a consultant for Boston Scientific and Torax Medical. He has received grant/research support from Olympus Medical Systems and royalties from Elsevier. AR has received previous grant/research support from Olympus America. JJB has received previous grant/research support from BARRX Medical, Cook Medical, Olympus and Astra Zeneca. All other authors have no conflicts of interest to declare.
-
Ethics approval Ethics approval was provided by three local institutional review boards.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- PostScript