Article Text

Abstract
Objective Resistance to antibiotics is the major cause of treatment failure of Helicobacter pylori infection. A study was conducted to assess prospectively the antibacterial resistance rates of H pylori in Europe and to study the link between outpatient antibiotic use and resistance levels in different countries.
Design Primary antibiotic resistance rates of H pylori were determined from April 2008 to June 2009 in 18 European countries. Data on yearly and cumulative use over several years of systemic antibacterial agents in ambulatory care for the period 2001–8 were expressed in Defined Daily Doses (DDD) per 1000 inhabitants per day. The fit of models and the degree of ecological association between antibiotic use and resistance data were assessed using generalised linear mixed models.
Results Of 2204 patients included, H pylori resistance rates for adults were 17.5% for clarithromycin, 14.1% for levofloxacin and 34.9% for metronidazole, and were significantly higher for clarithromycin and levofloxacin in Western/Central and Southern Europe (>20%) than in Northern European countries (<10%). Model fit improved for each additional year of antibiotic use accumulated, but the best fit was obtained for 2005. A significant association was found between outpatient quinolone use and the proportion of levofloxacin resistance (p=0.0013) and between the use of long-acting macrolides only and clarithromycin resistance (p=0.036).
Conclusion In many countries the high rate of clarithromycin resistance no longer allows its empirical use in standard anti-H pylori regimens. The knowledge of outpatient antibiotic consumption may provide a simple tool to predict the susceptibility of H pylori to quinolones and to macrolides and to adapt the treatment strategies.
- Helicobacter pylori
- 13C-urea breath test
- campylobacter
- molecular biology
- adenocarcinoma
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Resistance to antibiotics is the main factor of failure of Helicobacter pylori eradication therapies.
What are the new findings?
-
This large multicentre study performed in most of the European countries with a standardised protocol shows that resistance to certain antibiotics has reached a sufficient level not to prescribe them as an empirical therapy in some countries.
How might it impact on clinical practice in the foreseeable future?
-
Antibiotic use in the outpatient community was positively correlated with resistance for two major classes of antibiotics for the treatment of H pylori infection.
Introduction
The discovery of Helicobacter pylori and of its role in peptic ulcer disease constituted a breakthrough in the field of gastroenterology.1 Eradication treatments have been developed during the last 20 years leading to a decrease in H pylori-related peptic ulcer disease and in the prevalence of the infection in the Western world.2 ,3 However, the success of these treatments is now compromised by the increase in antimicrobial resistance of H pylori. 4 Clarithromycin resistance in particular has a major negative impact on the efficacy of the recommended first-line triple therapy and a progressive increase in the prevalence of resistance to this antibiotic may limit its use.5 ,6 By contrast, metronidazole resistance, although highly prevalent, can be partly overcome and is of secondary importance.7 As antibiotic resistance is an evolving process, it is mandatory to carry out point prevalence surveys on a regular basis in order to guide clinicians in the therapeutic choice. Such surveys were previously carried out in Europe in 1991 and in 1998.8 ,9 Our aim was to report on the results of the latest survey (2008–9) and to examine the association with the outpatient antibiotic consumption in Europe over an 8-year period (2001–8).
Materials and methods
A European multicentre study without intervention was planned. A common standard protocol based on a protocol previously described and approved by the Steering Committee of the study was used in all participating centres.9 Attention was given to recruit a number of centres that was proportional to the country population (ie, one centre per 10–20 million inhabitants). From April 2008 to June 2009, each participating centre was requested to collect prospectively a minimum of 50 consecutive non-duplicate clinical isolates of H pylori obtained from gastric biopsy specimens of patients attending an outpatient endoscopy clinic. These criteria were chosen on the basis of a compromise between the possibilities of the centre and the need to have sufficient data for statistical comparison. In order to evaluate the prevalence of primary antibiotic resistance (ie, resistance in the absence of any previous specific anti-H pylori treatment), isolates from patients who had been previously treated for H pylori were excluded.
Questionnaire
For each clinical isolate the participating centres were asked to provide the following items on a standardised questionnaire that was completed online and registered on a secure website: age, gender, country of birth, country and city of residency, clinical symptoms and endoscopic findings.
A validated dyspepsia questionnaire was not used since the study was not planned as a clinical trial.
Bacterial culture and susceptibility testing
Cultures and susceptibility testing of H pylori to clarithromycin, levofloxacin, amoxicillin, tetracycline, rifabutin and metronidazole were performed in each centre according to a standardised protocol using Etest strips which were provided by AB Biodisk (Solna, Sweden) and interpreted according to the guidelines of the European Committee of Antibiotic Susceptibility Testing (EUCAST) (http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Consultation/EUCAST_clinical_breakpoints_for_Helicobacter_pylori.pdf).9 Participants were asked to store the strains frozen at −70°C. Upon completion of the study, all H pylori strains reported as resistant to amoxicillin, tetracycline and rifabutin, as well as a random sample (using the software My SQL RAND) of those found either susceptible or resistant to clarithromycin and to levofloxacin, were retested centrally. Minimum inhibitory concentrations (MICs) of amoxicillin, tetracycline and rifabutin were determined by agar dilution and susceptibility to clarithromycin and to levofloxacin was determined by Etest and by the GenoType HelicoDR assay (Hain Lifescience, Nehren, Germany) which detects the various mutations associated with clarithromycin and levofloxacin resistance.10
Outpatient macrolide and quinolone consumption
In accordance with the Anatomical Therapeutic Chemical (ATC) classification and the Defined Daily Dose (DDD) measurement unit (WHO version 2011; http://www.whocc.no/filearchive/publications/2011guidelines.pdf), data on outpatient macrolide (ATC J01FA) and quinolone (ATC J01M) use were collected, aggregated at the level of the active substance and expressed in DDD per 1000 inhabitants per day (DID).
Macrolides were classified as short-, intermediate- and long-acting macrolides and quinolones were classified as first, second and third generation, as proposed by the European Surveillance of Antimicrobial Consumption project.11 ,12
Statistical analysis
A univariate analysis was carried out to assess the risk factors associated with resistance to clarithromycin, levofloxacin and metronidazole in adult patients. A multivariate analysis was also performed using a logistic regression method with a backward procedure to include all the variables selected (p≤0.25) and gradually remove the non-significant variables (p<0.05). A final model containing only the significant variables was obtained. Generalised linear mixed models (GLIMMIX procedure in SAS/STAT, SAS V.9·2; Poisson and negative binomial distribution, and logarithmic link function) were used to assess the association between outpatient macrolide and quinolone use (total class and by subgroup within each class) in DID (independent variables) and the proportion of clarithromycin and levofloxacin resistance rates, respectively. The number of resistant H pylori isolates per country was modelled using the total (logged) number of isolates as offset.
First, the model fit was assessed by means of the Akaike Information Criterion (AIC) for models including yearly use data with a time lag between use and resistance data ranging from 0 to 4 years and models including cumulative use data of 2–8 years prior to the end of the sample collection for 16 countries with complete data.
Second, the model with the best fit (lowest AIC) was used to assess the association between use and resistance data using all available use and resistance data from all participating countries. A p value <0.05 was regarded as significant.
Ethics
All collected data were transmitted anonymously to a secure website (login and password) and were analysed anonymously.
Results
A total of 2204 patients (1893 adults and 311 children) were included from 32 centres in 18 European countries. The mean number of cases per centre was 69 (range 16–198). Most of the countries with <20 million inhabitants recruited 50–100 cases while several of the larger countries (Germany, UK, Italy and Poland) recruited fewer patients than expected. Age, gender, clinical symptoms and endoscopic findings of the patients are presented in table 1.
Characteristics of patients from whom Helicobacter pylori strains were isolated
Antimicrobial susceptibility
The MICs showed a normal distribution with a clearcut separation between susceptible and resistant strains for clarithromycin (figure 1A) and for levofloxacin (figure 1B). In contrast, the MIC distribution for metronidazole showed a continuum (figure 1C). For adults, the resistance rate of H pylori was 17.5% for clarithromycin, 14.1% for levofloxacin and 34.9% for metronidazole while the prevalence was ≤1% for the other three antibiotics tested (table 2). In contrast, the rate of clarithromycin resistance was much higher in children (>30%) but was lower for metronidazole (25.7%) and for levofloxacin (2.5%). These differences in resistance between children and adults were statistically significant (p<0.001). The resistance rates are presented by country in figure 2A,B and by European region in table 3. For clarithromycin, the breakdown of resistance by country showed that all the Northern European countries had a resistance rate of <10% while all those from the rest of Europe except Germany and Spain had a resistance rate of >20%. Similar results were obtained whether the data were considered according to the country of birth or the country of residence of the patients (data not shown). By multivariate analysis, the only risk factor associated with clarithromycin resistance was to be born outside of Northern Europe (p=0.003, table 4), while an inverse association was found for patients with an endoscopic finding of ulcer disease versus those without ulcer disease (OR 0.50; 95% CI 0.32 to 0.77; p=0.002). Risk factors associated with levofloxacin resistance were age >50 years versus younger (OR 1.51; 95% CI 1.09 to 2.09; p=0.012) and being resident in Central or Southern Europe versus Northern Europe (p=0.0017), while a trend for an inverse association was found for patients with ulcer disease versus patients without ulcer disease. Resistance to metronidazole was associated with female gender (p<0.001) as well as being born outside Europe (p<0.001). Overall, roughly half of the strains (51.2%) did not show any resistance to the drugs tested, 36.8% exhibited resistance to a single class of antibacterial agents, 12.0% to two classes, approximately 2% of the isolates were resistant to three classes and only three strains were resistant to four classes of antimicrobial agents. Combined resistance to clarithromycin and metronidazole was present in 173 strains (7.8%) and represented more than 10% of the strains in four countries (Hungary, Austria, Poland and France; data not shown).
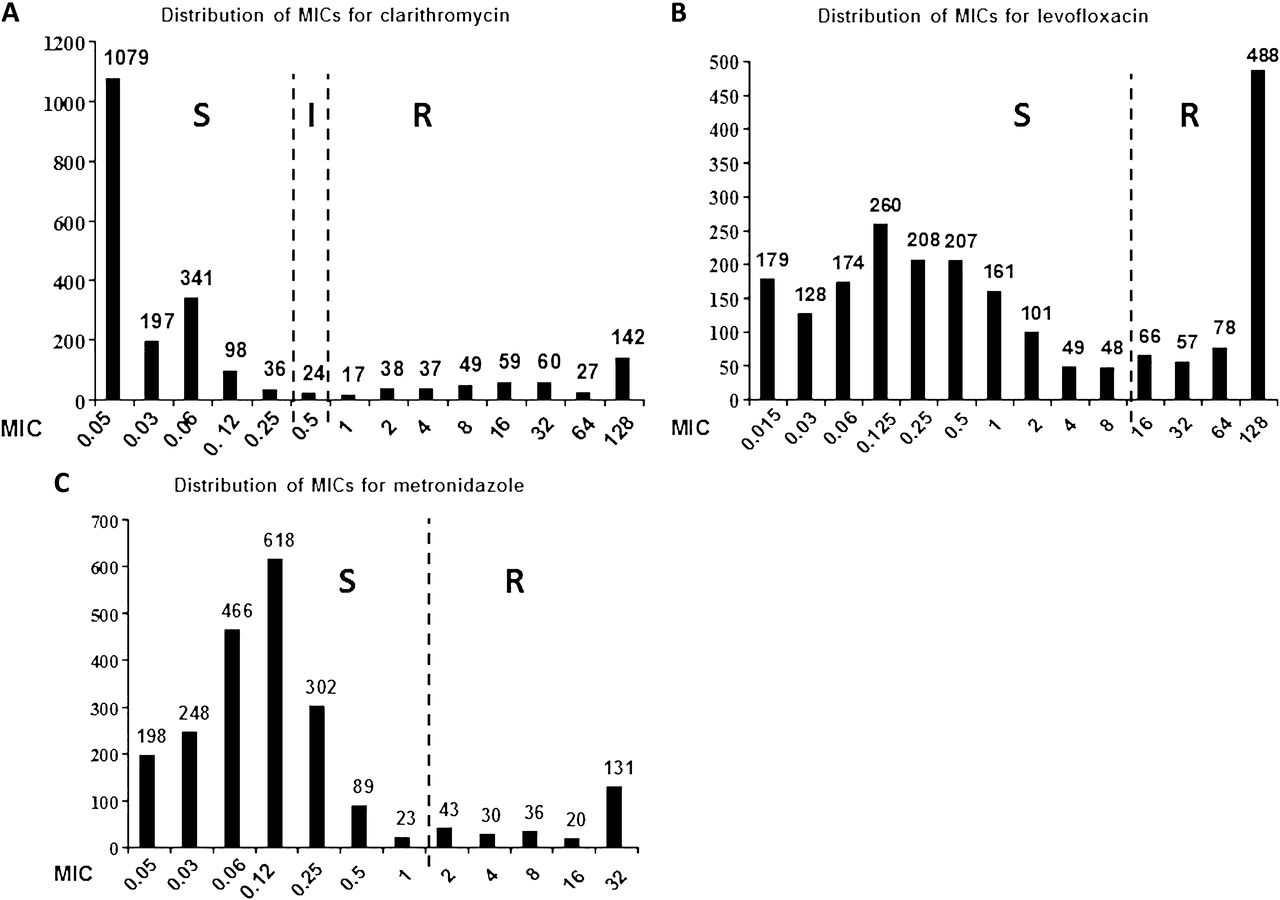
Distribution of the minimal inhibitory concentration of (A) clarithromycin, (B) levofloxacin and (C) metronidazole against Helicobacter pylori. Dashed lines correspond to the EUCAST H pylori breakpoints proposed in April 2011 (http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Consultation/EUCAST_clinical_breakpoints_for_Helicobacter_pylori.pdf) (accessed 20 Oct 2011).
Rate of resistance of Helicobacter pylori in Europe (1893 adults, 311 children)

Primary rate of (A) clarithromycin resistance and (B) levofloxacin resistance in Helicobacter pylori in Europe (2008–9) in adult patients.
Helicobacter pylori resistance to antibiotics according to country of residence in Europe in adult patients
Univariate and multivariate analysis of the risk factors of clarithromycin, levofloxacin and metronidazole resistance in Europe
There were 102 strains available for control testing. For clari-thromycin, discrepant results were found in four cases (3.9%): two strains originally labelled as resistant for which no mutation was found which were confirmed to be susceptible by Etest and two strains originally labelled as susceptible but where the molecular tests showed a mixture of wild type and mutant genotypes and which tested resistant in the control Etest. For levofloxacin, seven discrepant results (6.8%) were found: four strains resistant by Etest with no gyrA mutation and for which the control Etest indicated susceptibility and three strains labelled as susceptible (MICs ≤0.5 mg/l) but for which gyrA resistance mutations were present. None of the 12 strains supposedly resistant to amoxicillin, tetracycline or rifabutin could be confirmed as such by agar dilution control testing (data not shown).
Association with antibiotic consumption
Using the negative binomial distribution to model the link between antibiotic use and proportion of resistant H pylori strains produced lower AIC values or better fitting models than the Poisson distribution. The AIC values decreased for every added year of antibiotic use, indicating that the fit of the model improved along with the cumulative use of antibiotics over the years between 2008 and 2001. However, the best fit between macrolide and quinolone use and the proportions of clarithromycin- and levofloxacin-resistant H pylori isolates was obtained by using the yearly antibiotic use data for 2005.
Figure 3A and B shows the total outpatient use of macrolides and quinolones in 2005. Total macrolide use (figure 3A) varied by a factor of 7 between the country with the highest (9.79 DID in Greece) and the lowest use (1.42 DID in The Netherlands). Important variations were also found when use of short- (erythromycin), intermediate- (clarithromycin) and long-acting (azithromycin) macrolides were compared. On the whole, the use of macrolides was lower in Northern European countries than in Western/Central and Southern European countries, but no statistically significant association was found between total macrolide use in DID in 2005 and the proportion of clarithromycin-resistant H pylori isolates in 2008–9 (p=0.0641; for adults only p=0.071; figure 4A). However, a significant association was found between the use of long-acting macrolides alone (not short- or intermediate-acting) and resistance of H pylori to clarithromycin (p=0.0365 for 2005 use data; p=0.0042 for 2008 use data (better fit)).

Outpatient use of (A) macrolides (J01FA) and (B) quinolones (J01M) in 17 European countries in 2005. This figure is produced in colour in the online journal—please visit the website to view the colour figure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between (A) outpatient macrolide use (J01FA) in 2005 in DID (Defined Daily Dose per 1000 inhabitants) and proportion of clarithromycin-resistant Helicobacter pylori strains isolated from adults and children in 17 European countries and (B) outpatient quinolone use (J01M) in 2005 in DID and proportion of levofloxacin-resistant H pylori strains isolated from adults and children in 17 European countries. This figure is produced in colour in the online journal—please visit the website to view the colour figure.
The use of quinolones (figure 3B) also varied by a factor of 7 between the country with the highest use (3.28 DID in Italy) and the country with the lowest use (0.47 DID in Norway).
A highly significant association was found between total quinolone use in 2005 in DID and the proportion of levofloxacin-resistant H pylori strains (p=0.0013; figure 4B). A similar association between use and resistance was also found for the second and third generation quinolones (p=0.0010 and p=0.0026, respectively), but not for first generation quinolones (p=0.9352).
Discussion
The main result of this multicentre survey is a steady increase in clarithromycin resistance in comparison with a similar survey carried out in 1998 and the rapid emergence of levofloxacin resistance in H pylori.9 The almost doubling of the prevalence of clarithromycin resistance over the past 10 years from 9.8% to 17.5%9 could have be anticipated given the genetic basis of this resistance (ie, point mutations in the 23S rRNA gene which are transmitted vertically)4 and the long-lasting character of H pylori infection when left untreated.
However, it is important to keep this evolution in mind because clarithromycin resistance in H pylori decreases the efficacy of the standard clarithromycin-amoxicillin-proton pump inhibitor triple therapy by 70%.5 ,6 H pylori now falls into the inconsistently susceptible category (10–50% resistance) with regard to clarithromycin.13 Consequently, the Maastricht III Conference recommended abandoning clarithromycin in empirical treatment, or testing susceptibility for this antibiotic before using it when the prevalence of resistance is higher than 15–20%.7 Such a prevalence rate has now been reached in most countries in Western/Central and Southern Europe. In countries with 25–30% clarithromycin resistance, the eradication rates with standard triple therapy are expected to succeed at best in 60–70% of cases5 while they initially reached 90%.14 As an alternative to clarithromycin, the empirical use of levofloxacin has been proposed but the success rate of this treatment regimen is also very much dependent on the level of levofloxacin resistance.15 The prevalence of levofloxacin resistance was not tested in the previous European study because levofloxacin-based treatment only emerged later.16 Several reports have indicated that the prevalence of resistance of H pylori to quinolones has increased rapidly over the last decade17 ,18 and that it could soon reach the level of clarithromycin resistance.17 On the other hand, metronidazole resistance remains at the same high level (34.9%) as 10 years ago with no major changes in the regional distribution. In contrast to clarithromycin and levofloxacin resistance, the impact of metronidazole resistance on the eradication rate is limited5 and can be overcome in the majority of cases by increasing the length of treatment or by prescription of bismuth-containing quadruple therapy including metronidazole.19
This survey mainly included bacterial isolates from adult patients, but 311 H pylori clinical isolates of children from eight countries were also tested. They showed a constantly higher resistance rate to clarithromycin than those obtained from adults (table 2), and even higher than the resistance rate of 24% reported in another European multicentre survey in children.20 However, the inclusion of children did not occur in all the centres and the proportion was not the same for all the countries, so the resistance data for H pylori isolates from children obtained in our study should be interpreted with caution.
One of the major interests of this study lies in the correlation between H pylori resistance rates and outpatient antibiotic use in Europe. The chronic character and unknown time of acquisition of infection justified considering total cumulative outpatient antibiotic use data in the analysis in addition to single yearly use. Indeed, the fit of the models improved for each additional year of antibiotic used accumulated, although the best fit between quinolone and macrolide use and the proportion of levofloxacin and clarithromycin H pylori resistance rates was achieved when using 2005 outpatient use data. For macrolides, the lack of a statistically significant association between outpatient use data in 2005 and the proportion of clarithromycin-resistant strains could have been due to the insufficient sample size in this survey. However, this association became significant when the use of long-acting macrolides only (azithromycin) was considered in the analysis. Azithromycin is known to achieve high concentrations in the gastric mucus and gastric juice for several weeks after its administration, and this may lead to local subinhibitory concentrations in the vicinity of H pylori which could favour the selection of macrolide-resistant mutants.21 ,22
On the other hand, a strong association was found between quinolone use (mainly ciprofloxacin, except in Italy where levofloxacin was mostly used) and the proportion of resistance of H pylori to levofloxacin.
Several comments should be made about the observations concerning the link between antibiotic use and H pylori resistance in Europe. First, the DDD is a technical measurement unit which may not adequately translate variations in dosage and in length of treatment between countries. Other indicators of antibiotic use such as the number of packages or prescriptions could have complemented the current analysis23 but, as package data has only been available since 2006 for a limited number of countries, this could not be investigated.
Also, data concerning the time lag between antibiotic use and shift in antibiotic resistance are lacking. H pylori constitutes a paradigm of long-lasting infection and it should be stressed that the time of antibiotic exposure of this organism to antibiotics may be much longer than for most other pathogens. In contrast to other bacteria, with H pylori only selection of resistant strains occurs with no spread of resistance through horizontal transfer of mobile genetic elements. Moreover, the very low transmission rate of H pylori and the lack of expansion of particular clones in the community suggest that resistance in H pylori is essentially driven by the direct exposure of patients to antimicrobial agents.
The strengths of this study include the use of a uniform methodology, the online reporting system and central control susceptibility testing by phenotypic and molecular methods of a random subset of isolates which together suggest that the picture obtained of resistance in Europe is probably more reliable than that previously reported in other surveys.8 ,9 ,20 There were, however, certain limitations; it was impossible to involve any centre in some countries, either because we could not find microbiology laboratories that would perform H pylori culture on specimens from untreated patients or because bacteriologists were not willing to participate.
Despite the firm request to keep all the strains frozen, for various reasons it was not possible to obtain part of these for the control tests; however an excellent overall concordance was found between local and central testing with regard to clarithromycin and levofloxacin susceptibility results on those strains that were available for retesting.
In conclusion, our results from almost 2000 H pylori-infected adult patients before their first treatment have major implications for the first-line treatment and show that clarithromycin-based regimens can no longer be recommended without previous susceptibility testing in countries from Central and Southern Europe where more than 20% of the patients are infected with a macrolide-resistant strain. The increasing resistance to levofloxacin in several countries in Europe is also of concern because it precludes its empirical use in anti-H pylori rescue regimens without prior susceptibility testing. For the first time, we could show a significant positive association between outpatient antibiotic usage and the level of primary resistance observed in H pylori to key antimicrobial agents. The knowledge of antibiotic consumption in a given region may provide a simple tool to predict the susceptibility of H pylori to quinolones and macrolides, and to adapt the treatment strategies in settings where diagnostic laboratory facilities are not available.
While this study does not allow firm conclusions to be drawn for each individual country, it definitely stresses the need for local national resistance surveys with appropriate sample sizes that are representative of the general population. We strongly believe that it may be essential to obtain such data to improve the effectiveness of current anti-H pylori treatment regimens in these countries.
Acknowledgments
We would like to thank A Langlais for his contribution to the statistical analysis and S Mégraud for design of the online report system. This study was performed under the auspices of the European Helicobacter Study Group.
Appendix
Study group participants
Alarcon T, Hospital de la Princesa, Instituto de Investigación Sanitaria del Hospital La Princesa, Madrid, Spain; Albrecht P, Department of Pediatrics and Gastroenterology, Medical University of Warsaw, Warsaw, Poland; Barna Z, National Center for Epidemiology, Budapest, Hungary; Burucoa C, Laboratoire de Bactériologie, CHU de Poitiers, Poitiers, France; Calvet X, Digestive Diseases Department, Hospital de Sabadell, Institut Universitari Parc Taulí, Departament de Medicina, Universitat Autònoma de Barcelona, Spain; Cambau E, Service de Bactériologie-Virologie-Hygiène, CHU Henri Mondor, Créteil, France; Cellini L, Department of Drug Sciences, School of Pharmacy, Chieti, Italy; Conroy M-C, Laboratoire de Bactériologie, Hôpital Central, Nancy, France; Deforges L, Service de Bactériologie-Virologie-Hygiène, Hôpital Henri Mondor, Créteil, France; Dzierzanowska-Fangrat K, Department of Clinical Microbiology and Immunology, Children's Memorial Health Institute, Warsaw, Poland; Franzin L, Specialist Microbiology Research Laboratory, Amedeo di Savoia Hospital, Torino, Italy; Gisbert J, Gastroenterology Unit, La Princesa University Hospital, IP and CIBEREHD, Madrid, Spain; Gosciniak G, Department of Microbiology, Wroclaw Medical University, Wrocław, Poland; Huang Te-Din, Laboratoire de Bactériologie, CHU Mont-Godinne and Centre National de Référence des H pylori, Yvoir, Belgium; Jeverica S, Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia; Kuipers E, Department of Gastroenterology and Hepatology, Erasmus MC University Medical Center, Rotterdam, The Netherlands; Kupcinskas L, Institute for Digestive Research, Lithuanian University of Health Sciences, Kaunas, Lithuania; Lario S, Digestive Diseases Department, Hospital de Sabadell, Universitat Autònoma de Barcelona, Barcelona, Spain; Lawson A, Health Protection Agency, Centre for Infections, London, UK; Marzio L, Unita' di Fisiopatologia Digestiva, Universita' G d'Annunzio, Ospedale Civile, Pescara, Italy; McNulty C, Microbiology Laboratory, Gloucestershire Royal Hospital, Gloucester, UK; Melby K, Department of Microbiology, Oslo University Hospital, Oslo, Norway; Mentis A, Department of Medical Microbiology, Institut Pasteur Hellenique, Athens, Greece; Monno R, Department of Internal Medicine and Public Health Hygiene Section, School of Medicine, Bari, Italy; Montes M, Biodonostia Research Institute, San Sebastián, Spain; Oleastro M, Departamento de Doenças Infecciosas, Instituto National de Saúde Dr Ricardo Jorge, Lisbon, Portugal; O'Morain C, Department of Gastroenterology, Meath/Adelaide Hospital, Dublin, Republic of Ireland; Pellicano R, Department of Gastro-Hepatology, S Giovanni Battista (Molinette) Hospital, Turin, Italy; Perez-Trallero E, Microbiology Department, Hospital Donostia, St Sebastián, Spain; Pieramico O, Division of Internal Medicine, General Hospital ‘F Tappeiner’ Merano, Italy; Rasmussen L, Department of Microbiology, Rigshospitalet, Copenhagen, Denmark; Raymond J, Service de Bactériologie, Hôpital Cochin, Paris, France; Royo G, S. Microbiology, Hospital General Universitario de Elche, Elche, Spain; Stoof J, Department Gastroenterology and Hepatology, Erasmus MC University Medical Center, Rotterdam, The Netherlands; Szkaradkiewicz A, Department of Microbiology, Poznan University of Medical Sciences, Poznan, Poland; Taneike I, Department of Clinical Medicine, AMNCH, Dublin, Republic of Ireland; Tonkic M, Department of Clinical Microbiology, University Hospital Split, Split, Croatia; Villar Pérez H, Servicio de Microbiologie, Hospital San Agustin, Aviles, Spain; Wüppenhorst N, Institute of Medical Microbiology and Hygiene, National Reference Centre for H pylori, University Hospital Freiburg, Germany; Zanetti M, Division of Internal Medicine and Laboratory of Microbiology, General Hospital ‘F. Tappeiner’ Merano, Italy.
References
Footnotes
↵* Study Group participants are listed in appendix 1.
Funding The authors acknowledge the support of AB Biodisk, now AB bioMerieux, who provided the Etests for the study, and Axcan Pharma, now Aptalis Pharma, who helped us for the logistic part of the study.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.