Article Text

Abstract
Objective The introduction of anti tumour necrosis factor-α (anti-TNFα) therapy might impact healthcare expenditures, but there are limited data regarding the costs of inflammatory bowel diseases (IBD) following the introduction of these drugs. We aimed to assess the healthcare costs and productivity losses in a large cohort of IBD patients.
Design Crohn's disease (CD) and ulcerative colitis (UC) patients from seven university hospitals and seven general hospitals were invited to fill-out a web-based questionnaire. Cost items were derived from a 3 month follow-up questionnaire and categorised in outpatient clinic, diagnostics, medication, surgery and hospitalisation. Productivity losses included sick leave of paid and unpaid work. Costs were expressed as mean 3-month costs per patients with a 95% CI obtained using non-parametric bootstrapping.
Results A total of 1315 CD patients and 937 UC patients were included. Healthcare costs were almost three times higher in CD as compared with UC, €1625 (95% CI €1476 to €1775) versus €595 (95% CI €505 to €685), respectively (p<0.01). Anti-TNFα use was the main costs driver, accounting for 64% and 31% of the total cost in CD and UC. Hospitalisation and surgery together accounted for 19% and <1% of the healthcare costs in CD and 23% and 1% in UC, respectively. Productivity losses accounted for 16% and 39% of the total costs in CD and UC.
Conclusions We showed that healthcare costs are mainly driven by medication costs, most importantly by anti-TNFα therapy. Hospitalisation and surgery accounted only for a minor part of the healthcare costs.
- Inflammatory Bowel Disease
- Crohn's Disease
- Ulcerative Colitis
- Economic Evaluation
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Inflammatory bowel disease (IBD) is associated with a high economic burden to society.
-
In cost-of-illness studies conducted in the prebiological era, over half of the healthcare costs were driven by surgical and medical hospitalisation.
-
In the prebiological era, productivity losses due to decreased work productivity accounted for approximately 50% of the total costs in Europe.
What are the new findings?
-
This is the first cost-of-illness study in IBD following the introduction of infliximab and adalimumab in a large patient cohort, analysing both healthcare costs and productivity losses.
-
The traditional cost profile has changed and healthcare costs are now mainly driven by medication use, in particular antitumour necrosis factor-α (anti-TNFα) therapy.
-
Surgery and hospitalisation accounted for only 19% and <1% of the healthcare costs in Crohn's disease (CD) patients and 23% and 1% in ulcerative colitis (UC) patients.
-
Productivity losses due to sick leave accounted for 16% of the total costs in CD and 39% of the total costs in UC.
How might it impact on clinical practice in the foreseeable future?
-
By identifying and quantifying the relative contribution of different resources to the overall healthcare and productivity losses, this study provides important insights into the economic burden of IBD on the society in this era of widespread anti-TNFα therapy use. This is relevant for healthcare providers, policy makers and clinicians.
Introduction
Inflammatory bowel disease (IBD), comprising Crohn's disease (CD) and ulcerative colitis (UC), is characterised by a chronic relapsing intestinal inflammation that may lead to severe complications and disability. As there is no curative treatment, most patients need life-long drug treatment and many will face surgery.1 Consequently, IBD is associated with a high economic burden to society, in which hospitalisation and surgery account for more than half of the healthcare costs.2–4 Moreover, due to its early onset and chronic character, IBD profoundly affects work productivity with productivity losses resulting from sick leave and work disability amounting to almost 50% of the total costs.2 ,3 ,5–7
In the current era of escalating healthcare costs and growing constraints on healthcare budgets, there is a need for more accurate information regarding costs of chronic diseases. Most cost-of-illness studies in IBD have been performed before the introduction of the highly effective, but expensive biological therapies and can therefore be considered outdated.2–4 ,7 It has been suggested that costs of antitumour necrosis factor-α (anti-TNFα) therapy are being offset by a reduction in surgery and hospitalisation rates on the one hand,8–11 and increased work productivity on the other,12–14 but accurate data on total costs in Europe are presently lacking.
To address these issues, we recently initiated the ‘Costs Of Inflammatory bowel disease in the Netherlands’ or ‘COIN’ study in order to (1) estimate the total healthcare and productivity losses in a large cohort of IBD patient attending both university medical centres and general hospitals and (2) identify the main cost drivers.
Methods
Patient population
In The Netherlands, most patients with an established diagnosis of IBD and need for medical or surgical therapy are treated in university hospitals or general hospitals. We identified CD patients and UC patients using the diagnosis treatment combinations (DTCs) for respectively CD and UC. DTCs are based on the International Classification of Disease, Ninth Revision.15 ,16 DTCs were introduced in 2005 and can be considered the Dutch version of the Diagnosis Related Groups as used in other countries, for example, the USA. DTCs form the basis to pay inpatient services provided by hospitals and physicians. DTCs have been used to identify IBD patients in The Netherlands previously and have been found to be useful and reliable in this respect.17 ,18 All patients from seven university medical centres and seven general hospitals aged 18 years or older were eligible for participation. The study was centrally approved by the ethics committee of the University Medical Centre Utrecht.
Web-based questionnaire
We developed a secure web-based questionnaire and participants were provided with a unique username and password combination. Patients were invited to enter the username and password-secured and firewall-protected website and were asked to fill out the questionnaires. After completing the baseline questionnaire, patients received an invitation to fill out the 3-month follow-up questionnaire and an email reminder 2 weeks after the initial invitation.
Demographic and disease characteristics
The baseline questionnaire included questions on demographics (gender, age, smoking habits and education) and disease characteristics. Education was categorised as low education (no education, primary education, secondary education and technical or professional school) or high education (higher vocational education and university). Disease characteristics included type of IBD, year of diagnosis, disease localisation, penetrating disease course, abdominal surgery in the past and self-reported disease activity. Patients in whom medical treatment was initiated or changed or who received IBD-related surgery were considered to have active disease.
Healthcare utilisation
We obtained information on resource utilisation from the 3-month follow-up questionnaire. IBD-related resource utilisation within healthcare was categorised under the following subgroups: (1) outpatient clinic, including the number of outpatient physician consultations (eg, gastroenterologist, internist, surgeon and rheumatologist), visits to IBD or stoma nurses and dieticians, visits at the emergency department and visits to the general practitioner; (2) diagnostic procedures including number and type of endoscopies, radiological procedures and blood tests; (3) medication use, which included all IBD-specific drug use such as mesalazine, corticosteroids, immunomodulators and anti-TNFα therapies. The mean number of daily doses over the 3-month time frame was estimated. We assumed that all maintenance therapies were used without interruption over the study period; (4) hospitalisation, defined as the number of days hospitalised, including number of days at the intensive care unit; and (5) type of IBD-related surgery.
Productivity losses
Productivity losses (also referred to as ‘indirect (non-healthcare) costs’) refer to the costs associated with lost or impaired ability to work of paid and unpaid (voluntary) work. To assess productivity losses we used sick leave (absenteeism) of patients and their caregivers as outcome measurement. Patients were asked which of the following situations applied best to their situation: being employed, fully or partially disabled, retired or early retired, homemaker, student or unemployed. Employed patients or partially disabled patients with a paid job indicated the number of work hours and number of workdays per week. Patients were asked to report the number of sick leave days from both paid and unpaid (voluntary work) work within the previous 3 months. Additionally patients were asked to report whether caregivers were absent from paid work in order to take care of them, and for how many days. For caregivers we assumed an average work day of 6.28 h, based on data from the Statistics Netherlands.19
Out-of-pocket costs
Patients were asked to report IBD-related out-of-pocket costs within the previous 3 months. These expenditures included patient's deductibles for healthcare insurance, travel costs and over-the-counter drug use (eg, antidiarrhoeals, analgesics and vitamins).
Calculation of costs
We performed a cost-of-illness study from a societal perspective. For each patient, costs were calculated by multiplying units of resource utilisation as reported by the patients by their unit costs. Reference prices are listed in online supplementary appendix 1. Costs are expressed per 3 months in 2011 Euros, using Dutch consumer price indices where appropriate. Discounting was not applied as all costs were made within the same year. As practice patterns and the patient case mix may vary between university medical centres and general hospitals, we compared healthcare costs between university and general hospitals. The number of days patients and caregivers were absent from paid or unpaid work due to sick leave over 3 months could not exceed 65 days (weekends days were excluded) and were valued using age- and sex-specific productivity losses.20 Out-of-pocket costs were calculated according to patient specifications, and where necessary updated to 2011 Euros. In order to provide decision makers with explicit information, and allow health-economic analyses from different perspectives (ie, societal vs healthcare-payer perspective), costs are presented according to the classification of Drummond et al, that is, healthcare costs, productivity losses and patient costs.21
Non-responders
To control equality between the study population (responders) and the patients who did not respond (non-responders), we performed a non-responder study. All non-responders from one participating centre (n=685) were sampled to assess the demographic (age, gender) and disease characteristics (disease duration, penetrating disease course and abdominal surgery in the past) of a subset of the non-responders. The demographic and disease characteristics between the responders and the non-responders were compared.
Statistical analysis
Data analysis was performed using SPSS V.18.0. Descriptive statistics were used to characterise patients with CD and UC. We reported means with an SD and medians with an IQR. Comparisons between CD and UC patients were analysed with Student t test for continuous variables and χ2 for dichotomous variables. To compare disease duration between CD and UC patients, the Mann–Whitney U test was used. To increase transparency, all unit costs are stated in online supplementary appendix 1 and frequency tables of resource utilisation are displayed. Despite the skewed nature of cost data, we reported mean patient costs, as overall total costs—which matters most—can then be calculated. Costs were expressed as mean costs with 95% CI estimated using non-parametric bootstrap sampling. To compare costs between the general hospitals and university medical centres, the Mann–Whitney U test was used. To identify independent predictors of high healthcare costs, we included demographic and disease-specific characteristics associated with top 10% high healthcare in a multivariable logistic regression analysis.
Results
Study population
Figure 1 shows the study flowchart. In total 2252 patients were included in the cost analysis.

Study flowchart. CD, Crohn's disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.
Table 1 presents the demographic and disease characteristics of the CD (n=1315) and UC (n=937) study population. Distinction was made based on self-reported type of IBD. Patients who did not know their type of IBD, reported UC with disease localisation in the ileum or reported UC with fistulas were excluded from the cost analysis and categorised as IBD-unspecified (n=324, 13%).
Demographic and disease characteristics of the study participants
Online supplementary appendix 2 shows data on gender, age, disease duration, penetrating disease course and previous abdominal surgery in both the responders (CD: n=1315 and UC: n=937) and a subset of non-responders (CD: n=405 and UC: n=247). There were no relevant statistical significant differences between these groups.
Healthcare costs
The mean healthcare costs per CD patients per 3 months were €1625 (95% CI €1476 to €1775). With a mean of €1145 (95% CI €1042 to €1249), medication costs were the major cost driver of healthcare costs (71% of healthcare costs). Of the CD patients, 297 (23%) were on anti-TNFα therapy, accounting for 64% of the healthcare costs in this 3-month intercept. Hospitalisation and surgery accounted for 19% and <1% of the healthcare costs, respectively. The relative contribution of each cost item or service category as a proportion of the total healthcare costs is summarised in table 2.
Healthcare resource utilisation and costs of CD patients during 3 months in 2011 Euros
The components of resource utilisation and healthcare costs of UC patients are presented in table 3.
Healthcare resource utilisation and costs of UC patients during 3 months in 2011 Euros
The mean healthcare costs over 3 months for UC were significantly lower as compared with CD, namely, €595 (95% CI €505 to €685), p<0.01. Again, with 59% of the healthcare costs, the main cost driver was medication use. In UC, mesalazine (€136; 95% CI €130 to €143) and anti-TNFα therapy (€187; 95% CI €128 to €246) together accounted for over half of the healthcare costs (54%), with 602 (64%) patients treated with mesalazine and 37 (4%) with anti-TNFα therapy.
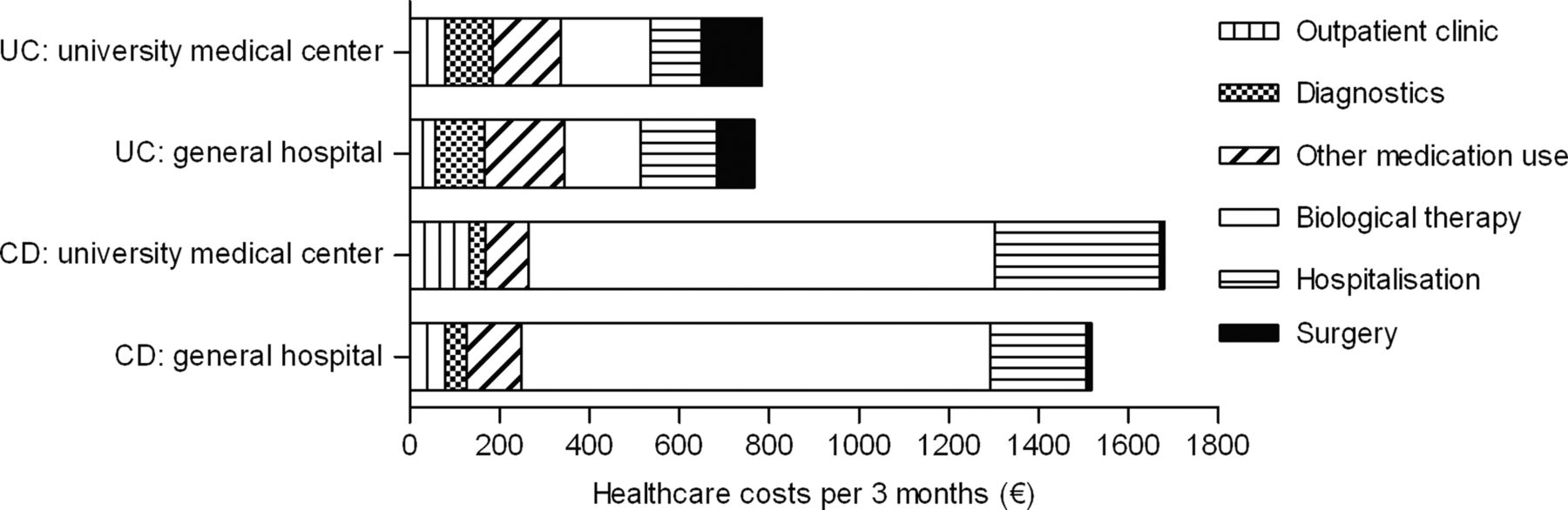
There were no statistically significant differences in healthcare costs of CD and UC patients between university medical centres and general hospitals, as shown in figure 2. The top 10% high-cost patients accounted for 40% of the healthcare costs in CD and 59% in UC. In CD, factors associated with high healthcare costs were current flares (adjusted (adj.) OR 4.00; 95% CI 2.74 to 5.82) and penetrating disease course (adj. OR 2.30; 95% CI 1.54 to 3.44). In UC patients, self-reported flares (adj. OR 2.35; 95% CI 2.50 to 3.68) and current ileostomy (adj. OR 2.35; 95% CI 1.06 to 5.23) were associated with top 10% high-cost patients.

{kind=link}
{kind=link}
Comparison of distribution of healthcare costs between university medical centres and general hospitals. CD, Crohn's disease; UC, ulcerative colitis.
Productivity losses
A total of 705 (54%) CD and 573 (61%) UC patients were currently employed. Of all CD patients currently employed, 18% reported sick leave with a mean loss of employment days of 2.5 (95% CI 1.8 to 3.4), translating in a mean loss of earnings of €289 (95% CI €198 to €379) over 3 months (table 4). In UC patients, 13% were absent from work due to sick leave with a mean loss of work days of 2.5 (95% CI 1.6 to 3.4), with associated loss-of-productivity of €362 (95% CI €231 to €493); p<0.01. Total productivity losses were €326 (95% CI €234 to €418) in CD and €395 (95% CI €261 to €529) in UC (table 4).
Productivity losses in CD and UC patients in 2011 Euros
Out-of-pocket costs
Out-of-pocket costs were €75 (95% CI €65 to €84) in CD and €57 (95% CI €49 to €66) in UC. According to patient specifications, most expenditure was on deductibles of healthcare insurance, vitamins and other over-the-counter expenditures, and memberships of patient associations.
Total costs
The total costs (healthcare costs+productivity costs+out-of-pocket costs) were €2001 (95% CI €1808 to €2194) for CD patients and €1023 (95% CI €838 to €1208) for UC patients. Productivity costs accounted for 16% of the total costs in CD patients and 39% in UC patients. Out-of-pocket costs accounted for <1% of the total costs in both patient groups.
Discussion
This study provides the most comprehensive update on the cost profile of IBD since the introduction and expanding use of anti-TNFα therapy in Europe. Up to the 2000s, hospitalisation and surgery were the major cost drivers in IBD. We report that nowadays medication use, anti-TNFα in particular, represents the main source of healthcare costs while costs related to hospitalisation and surgery are substantially reduced as compared with previous studies.2–4
Interestingly, total healthcare costs in IBD patients over time do not seem to increase. Extrapolating the 3-month healthcare costs from our study towards annual costs yielded mean costs of €6501 and €2380 per year in CD and UC patients. A cross-sectional, single centre study conducted in the UK, with an almost similar study population, reported 6-month healthcare costs of £1652 and £1256 in CD and UC patients for the year 2004.2 Extrapolating these costs to a 1-year period, and using UK consumer price index to inflate (1.23) and convert (1£=€1.56 on 1 December 2011) these costs to 2011 Euros would equal €6338 for CD and €4819 for UC. In this study, medical and surgical hospitalisation contributed to over half of total costs, but only 18% of healthcare costs in CD and 24% in UC was due to direct medication expenditure. This contrasts with data from our study, in which medication costs accounted for up to 71% and 59% of the healthcare costs for CD and UC, respectively. Results from a large European cohort study by Odes et al4 were in line with the UK study. They reported that over half of the healthcare costs were due to hospitalisation and surgery, while only 30% of total costs were due to medication use, with mesalazine being the most expensive drug.4 The same cost profile was reported in a hospital-based nationwide Spanish study conducted in 1997 in which medical and surgical hospitalisation accounted for 53% of the healthcare costs.3
Even though healthcare costs between the USA and Europe differ to a large extent, comparable trends in treatment paradigms should have induced the same alterations in cost profiles as observed in our study. Kappelman et al studied healthcare costs using medical and pharmacy claims from an administrative database between 2003 and 2004, in which 10% of all CD patients had at least two claims of infliximab infusions.22 In this study, pharmaceutical claims accounted for the largest proportion of healthcare costs (35%), in which infliximab was the most costly medication. But none of the cost studies in the past have taken the economic impact of adalimumab into account, as this agent was registered only in 2007 for CD. Thus, it seems that there is a shift in cost profile from surgery and hospitalisation towards anti-TNFα treatment. Apparently, the high costs of these drugs are partly compensated for by a significant reduction of surgery and hospitalisation rates. Obviously, a longer follow-up period of 2–5 years is needed to confirm this trend. Recent published reviews and cohort studies, however, showed a decrease in surgery and hospitalisation rates as well, underscoring our findings.11 ,23 A similar development has been reported in the treatment of rheumatoid arthritis, with a decline in surgery rates since the introduction of anti-TNFα therapy for this indication.9 ,24–26
We also examined productivity losses due to IBD-related sick leave, accounting for 16% of total costs in CD and 39% in UC. Comparisons between this study and older studies are limited due to varying methodologies in measurement and valuation of productivity losses, as well as differences in social security policies. We therefore focused on sick leave in days to illustrate changes in productivity losses. We found that 18% of employed CD patients and 13% of employed UC patients reported sick leave in the previous 3 months. Previous studies found that 14%–50% of CD patients and 15%–32% of UC patients reported sick leave.2 ,3 727 Higher age was found to be an independent predictor of sick leave.27 Although patients from our study cohort were older with longer disease duration as previously reported, we found similar or even lower rates of sick leave. We did not incorporate productivity losses due to work disability, as we did not know the cause of work disability. Inclusion of these costs would have therefore overestimated the total productivity costs. From literature, however, we know that the impact of work disability is considerable. A German study employing a 4-week diary reported that 49% of the total costs were due to work disability in CD and 32% in UC, respectively.7 Similarly, a Swedish study reported that 36% of the total costs of IBD were due to work disability.5 Finally, we did not include productivity losses while at work due to the disease (presenteeism). At this point, there are no validated questionnaires to assess presenteeism with a longer recall time than 7 days. Therefore we might have underestimated the productivity losses.
The strengths of this study included both the size and the diversity of the case mix by including patients from both university and general hospitals throughout The Netherlands. In order to enrol a large number of patients, we opted for the present web-based design. An inherent limitation of such a strategy is sampling bias. Although internet access among IBD patients has been reported to be high and The Netherlands has a very high internet penetration of 89%,28 our sample is not necessarily representative of the IBD population as a whole. It was expected that relatively few elderly subjects would participate, but we did recruit a total of 302 (10%) patients over the age of 65.
In general, participation rates for single questionnaires can be expected to be higher. However, we asked patients to participate in a longitudinal cohort study, possibly explaining the lower participation rate. We assessed the representativeness of our study by performing a non-responder study and could not detect major differences in demographic and disease characteristics between responders and non-responders. Reassuringly, we were able to confirm previously reported outcome data, supporting the internal validity of our cohort. For example, prior studies found slightly more frequently UC in men, whereas CD occurs 20%–30% more frequently in women,29–31 as we found in our study. Furthermore, we found comparable rates of abdominal surgery of 54% in CD patients and 18% in UC patients as previously reported.23 ,32 Additionally, over 10% of the CD patients will eventually require permanent faecal diversion,32 similar to the 12% reported in our population. Finally, during disease course, the cumulative risk for perianal involvement was 50%,32 ,33 comparable with the 53% of reported penetrating disease course in our CD population. As such, in spite of potential limitations, we believe that our study provides reliable and generalisable data on total costs in IBD.
It could well be possible that due to the relatively short observation period healthcare costs have skewed in favour of the medical costs. However, we have chosen to set a strict time limit for the observation period, as it is known from previous studies that the reliability of productivity and healthcare data is decreasing if the recall times exceed more than 3 months. Our large study size, however, provides a substantial cumulative observation time of nearly 600 patient years.
Our study provides valuable information which, if interpreted with caution, can be used for theoretical modelling and cost-effectiveness studies, and aids to put the high costs of anti-TNF drugs into perspective. Its selective use could lead to a reduction of hospitalisation and surgery rates and in an increase in work productivity thereby rendering these drugs cost-effective. In conclusion, this is the first cost-of-illness study since the introduction of anti-TNF therapy in Europe. Total costs do not seem to increase, but cost profiles have changed markedly. Healthcare costs are now mainly driven by medication costs. Hospitalisation and surgery did only account for small percentages of healthcare costs.
Acknowledgments
We would like to thank all research nurses from the participating centres, in particular Janneke van den Brink, for their help with the COIN study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online appendix
Footnotes
-
Contributors MEvdV, BO, MJJM, MGHvO: Study concept and design. MEvdV, BO, MJJM, MGHvO: Acquisition of data. MEvdV, BO, MJJM, MGHvO: Interpretation of data. MEvdV: Drafting of manuscript. All authors: Critical revision of the manuscript. All authors: Final approval of the submitted manuscript.
-
Funding This study was supported by an unrestricted grant from Abbott.
-
Competing interests AAvB has acted as a consultant for Abbott and MSD and received payments for lectures from Abbott and Ferring. HHF has acted as a consultant for Abbott. DJdJ has acted as a consultant for Synthon Netherlands and received payments for lectures from Abbott, Ferring and MSD. JvdW has acted as a consultant for Abbott, Ferring, Shire and MSD and received payment for lectures from Abbott, Falk Pharma and MSD. CYP has acted as a consultant for Abbott and received payments for lectures from Ferring and MSD. AEvdMJ has acted as consultant for Abbott. MGHvO has acted a consultant for Abbott. BO has acted as a consultant for Abbott and MSD and received payment for lectures and manuscript preparation from Ferring.
-
Ethics approval This study was carried out with the approval of the Medical Ethics Committee (MEC) of the University Medical Center Utrecht.
-
Provenance and peer review Not commissioned; externally peer reviewed.