Article Text

Abstract
BACKGROUND Some patients with faecal incontinence are not amenable to simple surgical sphincter repair, due to sphincter weakness in the absence of a structural defect.
AIMS To evaluate the efficacy and possible mode of action of short term stimulation of sacral nerves in patients with faecal incontinence and a structurally intact external anal sphincter.
PATIENTS Twelve patients with faecal incontinence for solid or liquid stool at least once per week.
METHODS A stimulating electrode was placed (percutaneously in 10 patients, operatively in two) into the S3 or S4 foramen. The electrode was left in situ for a minimum of one week with chronic stimulation.
RESULTS Evaluable results were obtained in nine patients, with early electrode displacement in the other three. Incontinence ceased in seven of nine patients and improved notably in one; one patient with previous imperforate anus and sacral agenesis had no symptomatic response. Stimulation seemed to enhance maximum squeeze pressure but did not alter resting pressure. The rectum became less sensitive to distension with no change in rectal compliance. Ambulatory studies showed a possible reduction in rectal contractile activity and diminished episodes of spontaneous anal relaxation.
CONCLUSIONS Short term sacral nerve stimulation notably decreases episodes of faecal incontinence. The effect may be mediated via facilitation of striated sphincter muscle function, and via neuromodulation of sacral reflexes which regulate rectal sensitivity and contractility, and anal motility.
- sacral nerve stimulation
- faecal incontinence
Abbreviations
- EMG
- electromyography
- PNE
- percutaneous nerve evaluation
Statistics from Altmetric.com
Patients with a simple structural defect of the external sphincter have a high surgical success rate.1-3 However, there are many patients with smooth muscle internal sphincter defects or degeneration, or a weak but structurally intact external sphincter, who are not amenable to simple surgical treatments. Some of these patients complain of substantial passive faecal leakage, while others have high colonic pressures which they cannot oppose because of external sphincter weakness, resulting in urge faecal incontinence.4 Some are helped by antidiarrhoeal drugs such as codeine or loperamide but this is not a satisfactory long term solution for many patients.
The stimulated gracilis neosphincter is now an established procedure,5 but is complicated and requires experience to achieve a good result. The artificial bowel sphincter constitutes another treatment option6 but is an invasive procedure with implantation of foreign material. Rather than reconstruct the anal sphincter mechanism directly it may be possible to improve continence by modifying the neural control of the sphincter and the proximal bowel. Continence depends on the net contributions of the sphincter muscles, coordinated rectosigmoid activity, and the presence of formed stool. If the external anal sphincter ring is structurally intact it may be possible to alter sphincter and proximal bowel behaviour using the nerves and muscles which are naturally in place.
Such an approach has been used effectively in treating urinary voiding dysfunction including incontinence, especially when the lower urinary tract seems to be structurally intact but functionally disturbed.7-10 These patients undergo a trial in which the nerves are stimulated via percutaneous electrodes placed adjacent to sacral nerves. If this procedure relieves symptoms over several days the patient has permanent electrodes implanted surgically, together with a chronic nerve stimulation apparatus implanted subcutaneously in the anterior abdominal wall.
In a preliminary study the same procedure has been tried in faecal incontinence.11 Three patients who had been found to have an improvement in anal sphincter pressures on acute testing were implanted with permanent electrodes. It was not clear from this study how many patients were evaluated with temporary electrodes prior to permanent electrode placement.
Although Matzel and colleagues11 suggested that faecal continence was restored by a direct effect on raising anal sphincter pressures, the effect may be via a more complex mechanism. In urinary incontinence chronic sacral nerve stimulation is often associated with restored continence unaccompanied by significant changes in urodynamics or other quantitative parameters and may be due to alteration of sacral reflexes.
The aim of this study was therefore to explore whether temporary spinal nerve stimulation alters symptoms of faecal incontinence over several days, and to determine the mechanism by which symptom improvement might occur.
Patients and methods
PATIENTS
Patients, selected from those referred for assessment of faecal incontinence, were assessed by anorectal physiological studies and anal endosonography. They were selected for sacral nerve stimulation in the belief that this treatment would be useful for patients with a circumferentially intact external anal sphincter, possibly by modulating external anal sphincter activity. We hypothesised that the facilitation of external sphincter activity could compensate either for a low resting or squeeze pressure. Patients with faecal incontinence therefore had to have a circumferentially intact external anal sphincter and either isolated internal anal sphincter pathology (weak and circumferentially intact or disrupted) and/or a weak external sphincter.
For inclusion the following criteria had to be fulfilled: (1) faecal incontinence (passive or urge) for solid or liquid stool at least once per week over a period of at least three months; (2) a structurally intact external anal sphincter, both clinically and as shown using anal endosonography; (3) weak external or internal sphincter function, as measured manometrically, with either resting or squeeze pressure falling within the lower quartile of the normal range or below the normal range; and (4) a psychologically stable patient, as assessed clinically, who was also suitable for surgical intervention.
Exclusion criteria included: coexistent medical illness such as cardiac disease or diabetes; pregnancy; and a past history of decreased bowel frequency or impaired evacuation.
Twelve patients, all female, median age 55 years (range 36–65 years) were studied. Four had mainly passive incontinence, two had mainly urge incontinence, and six had both passive and urge incontinence. The duration of symptoms ranged from three to 36 years with a median of six years. Four of the patients had idiopathic weakness of both sphincter muscles and two had idiopathic weakness of the external sphincter muscle. The cause of this, in the absence of clear neuropathy or structural damage, was not known. Three patients had primary internal sphincter degeneration as recently described.12 One patient had internal sphincter damage from previous fistula surgery and a small obstetric related scar in the external sphincter. One patient had scleroderma with a thin, weak internal sphincter13 and one patient was born with an imperforate anus and had a pull through operation14 shortly after birth. This patient was included in the study as her endoanal ultrasound had shown that the pull through had been brought down through the external sphincter with muscle fibres completely surrounding the neoanus. However, sacralx rays did show partial sacral agenesis with the S3 foramen visible only on the right side. Three women were nulliparous; the remaining six had had between one and four vaginal deliveries (median two).
INITIAL EVALUATION
Prior to insertion of the stimulator all patients underwent anorectal physiological tests which were performed by one investigator (CJV). These were performed according to previously described techniques and included stationary anal manometry,15pudendal nerve terminal motor latency measurements,16rectal threshold, urge and maximum tolerated volumes to rapid distension with air, anal and rectal electrosensory thresholds,17 rectal threshold, urge and maximum tolerated volumes to slow distension with water, and rectal compliance.18 The two types of sensory testing (during compliance testing and during distension with air) differed in relation to the speed and content of the infusion.
Twenty four hour ambulatory manometry was performed with an unprepared bowel. A flexible manometry probe which contained two solid state transducers (CTG-2 Gaeltec Ltd, Dunvegan, Isle of Skye, UK) was introduced into the rectum. One transducer on the probe was located 1 cm from its tip and the second 10 cm from the first. The probe was placed so that one transducer was situated in the anal canal approximately 1 cm from the anal verge and the other transducer then lay in the rectum. The probe was taped to the anal margin and buttocks, and connected to a portable solid state recorder (UPAS 2020, Medical Measurement Systems, Enschede, The Netherlands). The patients were then freely mobile within the hospital for the following 24 hours and were instructed to push event buttons to record eating, drinking, sleeping, urge to defaecate, and defecation. At 24 hours the recording was stopped and the data downloaded to a personal computer (IBM 486 PC).
The pre-entry endoanal ultrasound scans were performed by a single senior radiologist using a 10 MHz probe (B&K Medical, Gentofte, Denmark).
All patients completed a one week diary card with details of their normal bowel actions and of any episodes of incontinence of flatus, liquid, or solid stool.
PERCUTANEOUS NERVE EVALUATION
The percutaneous nerve evaluation (PNE) has an acute phase for response confirmation, and a subchronic phase for evaluation of therapeutic effect.
Acute phase
In order to establish the functional integrity of the sacral nerves, to locate and identify the nerves responsible for specific responses, and to confirm the appropriate muscle responses, percutaneous electrical stimulation of the nerve roots at the level of the third sacral foramen (S3) was attempted first, followed by S2 and S4 stimulation if the response was inadequate. The S3 foramina were located using bony landmarks with the patient in the prone position. They are typically 1 cm cephalad to the crest of the sacrum and 1 cm lateral to the midline. Acute testing was performed using 20 gauge, 3.5 inch spinal insulated needles (Medtronic 041828–004) and an external, hand held neurostimulator (Medtronic Model 3625 Screener). Response to the stimulus was assessed clinically and with simultaneous anal manometry and electromyography of the external sphincter and flexor hallucis longus. Stimulation of S3 is associated with a deepening and flattening of the buttock groove from lifting and dropping of the pelvic floor (known as a “bellows” action), a flexion of the big toe, and a pulling sensation in the perineum. Stimulation of S4 is also associated with a “bellows” action and a pulling sensation in the perineum but not with any toe movement. The current used for stimulation, to determine correct electrode placement, was that required to elicit a direct motor response in the external anal sphincter and the flexor hallucis brevis and usually ranged from 0.5 to 2 mA at a rate of 20 Hz and a pulse width of 200 seconds. Correct placement of the electrode was confirmed immediately after insertion by posteroanterior and lateral pelvic radiographs.
Subchronic phase
If adequate responses were obtained during the acute testing, subchronic test stimulation on the same side and at the same sacral level providing the best response was conducted for about one week. In 10 patients a temporary percutaneous stimulator lead (Medtronic 041830–004) was placed through the needle and connected to the same external neurostimulator as used previously. In two patients an electrode was fixed operatively with a percutaneous extension (Medtronic 3080). The stimulator used was portable and battery powered (Medtronic Model 3625 Screener). A wound dressing and tape secured the percutaneous lead. The stimulator allowed the amplitude of stimulation to be controlled by the patient. The stimulus used for subchronic stimulation was the maximum comfortably tolerated by the patient, and usually ranged between 0.5 and 3 mA at 15 pps (pulses per second) with a pulse width of 210 seconds.
A diary card to record normal bowel activity and episodes of incontinence was kept for the next seven days.
The patient returned to the ward for two days. Within 24 hours of insertion the patients were tested for anal manometry, anorectal sensory testing, and rectal compliance with the stimulator turned on and turned off. The 24 hour anal ambulatory manometry was then repeated with the device turned on.
Patients with a percutaneous lead returned home for five days. One week after insertion the stationary anorectal studies were repeated, and the device then removed. Patients with an operatively placed lead returned home for 19 days and returned to have the studies repeated at three weeks.
The data from the diary cards were analysed using the Wilcoxon rank test. An analysis of variance was used for all other variables.
Results
The best response during electrode insertion was obtained with S3 in 11 patients and S4 in one.
The stimulation ceased to produce a clinical or electromyography (EMG) effect in two of the 12 patients within the first 24 hours, and a radiograph confirmed displacement of their percutaneously placed electrode. Ten patients therefore had repeat anorectal physiology tests with stimulation. There were two further displacements of percutaneously placed electrodes before seven days. In the first of these the ambulatory manometry and day seven physiology tests were not possible. In the second patient loss of stimulation was felt on day 6 and only the day 7 tests were not performed. Nine patients completed a seven day clinical trial and diary.
SYMPTOMS
Seven of the nine patients without lead displacement had complete cessation of incontinence for solid and liquid stool (see table 1). The seven day diary card for the nine patients showed a significant decrease in episodes of incontinence for solid and liquid stool (prestimulation: median 8 (range 2–58); poststimulation: 0 (0–10); p=0.01, Wilcoxon rank test). Patient ZN (with a small scar in the external sphincter) had an impressive reduction in the number of episodes of incontinence; the amount of stool lost at each episode was also reduced from a significant volume to a small stain. Patient GM, who had imperforate anus and partial sacral agenesis, was the only patient who was not helped symptomatically by stimulation. The stimulation for patient FH stopped working before day 7 and the diary was therefore less reliable in this patient with the three episodes of incontinence occuring only after she had stopped feeling the stimulation.
Symptom diary before and during stimulation in nine patients
ANORECTAL PHYSIOLOGICAL STUDIES
The maximum resting pressure did not change significantly with stimulation (prestimulation: 40 cm H2O (25–140); 24 hours poststimulation: 53 cm H2O (25–130); days 7–21 poststimulation: 57 cm H2O (20–95)). However, stimulation seemed to produce qualitative changes in the anal pressure, often acutely inducing slow wave anal activity and decreasing the number of spontaneous relaxations (fig 1). The maximum squeeze pressure seemed to change with stimulation (prestimulation: 33 cm H2O (10–120); 24 hours poststimulation: 60 cm H2O (10–140); days 7–21 poststimulation: 75 cm H2O (25–165)). This change was significant (p<0.001) after one week of stimulation. The normal maximum resting and squeeze anal pressures in our laboratory are both greater than 60 cm H2O.
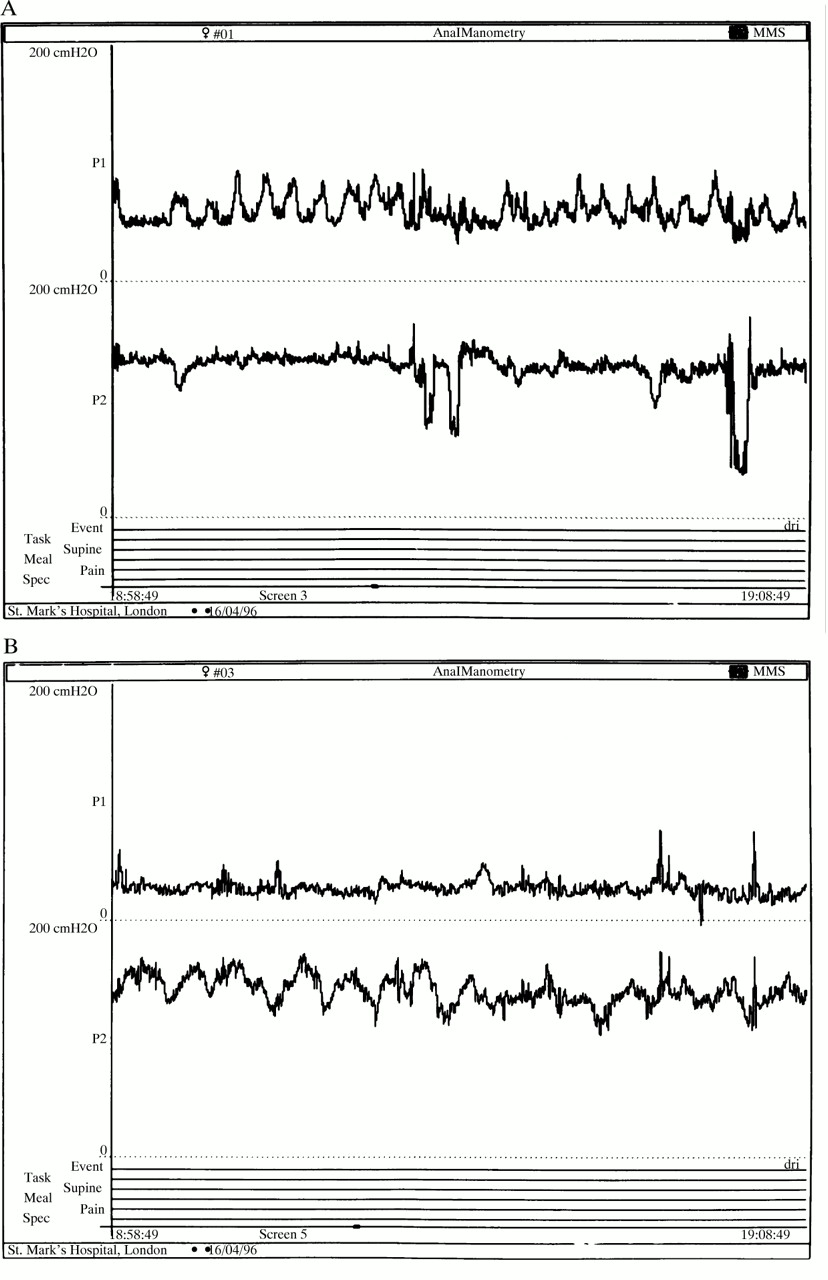
{kind=link}
Ten minute traces from the 24 hour ambulatory studies of patient FH. (A) Before stimulation; (B) after stimulation. The upper trace shows rectal activity and the lower trace anal activity. Stimulation seems to reduce rectal contractile activity and to cause qualitative changes in anal contractile activity with induction of slow wave activity and a reduction in transient relaxations.
On initial evaluation the pudendal nerve terminal motor latencies were not prolonged beyond the normal 2.4 msec on both sides in any patient. Measurement of latencies during stimulation was difficult due to electrical interference from the stimulator.
Anal and rectal sensitivity to an electrical stimulus was normal in all subjects except the patient with an imperforate anus. Sacral nerve stimulation did not change the sensory thresholds.
Percutaneous nerve stimulation seemed to alter the rectal sensory response to balloon distension with air. Initial sensation increased significantly after one to three weeks of stimulation (prestimulation: 45 ml (30–90); 24 hours poststimulation: 73 ml (45–140); days 7–21 poststimulation: 145 ml (75–230); p=0.02). Urge volume also increased significantly after one to three weeks of stimulation (prestimulation: 73 ml (40–90); 24 hours poststimulation: 107 ml (90–190); days 7–21 poststimulation: 173 ml (120–220); p=0.02). The increase in maximum tolerated volume (prestimulation: 95 ml (25–125); 24 hours poststimulation: 150 ml (80–250); days 7–21 poststimulation: 195 ml (140–250)) was significant at 24 hours (p=0.05) but was not significant at one to three weeks (p=0.16). In contrast the rectal sensory response to slow water infusion showed no increase with PNE. Rectal compliance seemed to increase on testing within 24 hours but then seemed to revert to pre-PNE levels at day 7 or 21 (prestimulation: 7.6 ml H2O/cm H2O (2.22–14.3); 24 hours poststimulation: 7.33 ml H2O/cm H2O (3.75–45.4); days 7–21 poststimulation: 7.6 ml H2O/cm H2O (2.85–14.3)).
The mean resting anal pressures during 24 hour ambulatory recording were not altered by PNE stimulation at 57 cm H2O (range 43–110) prestimulation versus 57 cm H2O (range 39–150) poststimulation in the nine patients. The number of rectal motor complexes seemed to decrease, although it was difficult to quantitate these accurately. Overall the amount of rectal contractile activity did seem to be decreased by stimulation (fig 1). The maximum amplitude of rectal contractile activity did not seem to be consistently altered. The 24 hour rectal pressures were too variable to give a meaningful representative value. Anal canal pressures were higher than rectal pressures both before and after stimulation, but more impressive was the lack of spontaneous “dips” in anal pressure, and the qualitative change in rectal contractile activity, with stimulation. It was not possible to correlate passage of flatus or episodes of incontinence with motor events.
COMPLICATIONS
There were no complications, including no infection.
Discussion
This study has shown that stimulation of the sacral nerves that innervate the anal sphincter and rectum seems to decrease notably episodes of faecal incontinence in specially selected patients. In the only published report to date, involving three patients, this seemed to be related to an increase in the maximum squeeze anal pressure. We also found an effect on the squeeze pressure, suggesting possible facilitation of external anal sphincter voluntary striated muscle activity by electrical stimulation.
In accordance with the results of Matzel and colleagues11we did not see an effect on the resting pressure. However there did seem to be qualitative changes in the resting anal pressure activity. This may relate to a direct effect on the extrinsic innervation of the smooth muscle internal sphincter via the sacral parasympathetic supply, whose effect on the internal sphincter is to maintain tone.19
The effects of stimulation are likely to be more diverse than a simple effect on the efferent motor supply to the sphincter. The stimulation may have affected rectal sensitivity and compliance, although these effects did vary depending on the rate of distension and the nature of the infusion. Chronic electrical stimulation caused an increase in the sensory volumes when air was infused rapidly, but caused a decrease in sensory volumes when water was infused slowly. Rapid and slow infusion have different effects on the rectal muscle and the sensations elicited are mediated via different pathways.20 It may be that electrical sacral nerve stimulation affects these processes differentially.
Sacral nerve stimulation was first reported for use in patients with urinary difficulties in the 1960s.21 The main areas of success have been in urinary incontinence due to detrusor instability and in evacuatory difficulties due to failure of urethral sphincter relaxation. The mechanism by which sacral nerve stimulation affects urinary incontinence is not clear. It has been postulated to alter local reflexes (“neuromodulation”) and may also affect the myelinated somatic outflow to the urinary sphincter at a lower threshold than the stimulus required to modulate the efferent autonomic supply to the bladder.22 The level of stimulation required to achieve smooth muscle contraction via autonomic myelinated efferent fibres is three to five times higher than the threshold for alpha motor neurones which innervate sphincter striated muscle. Our findings would support this hypothesis, in that no direct effect on sphincter resting smooth muscle tone was observed, but the striated sphincter activity seemed to have been facilitated.
In a mixed nerve the largest fibres with the lowest threshold are the IA sensory fibres which respond to phasic muscle stretch, followed by the alpha motor neurones.23 The level of stimulation required to activate afferent Aδ fibres is 1.5 times that required for alpha motor neurones while autonomic efferent fibres have a threshold three to five times higher than alpha motor neurones. C fibres responsible for pain have a much higher threshold. At low stimulation, therefore, when the electrodes are being placed, the lowest threshold is required to activate the alpha motor neurones to the sphincter striated muscle and toe. The reflexes are then modulated by slightly higher stimulation which affects Aδ fibres. With chronic low grade stimulation it is believed that there is insufficient stimulus to raise sphincter pressure, but the stimulus may be enough to modulate these Aδ reflexes. In neuromodulation of the bladder it is believed that Aδ sensory fibres are stimulated, resulting in inhibition of smooth muscle contractile activity and stabilisation via alteration in sacral reflexes. The same may be true for the bowel, as we did observe an effect on rectal dynamics during distension testing. Modulation of sacral reflexes that serve the rectum may stabilise rectal contractile activity, and there was some evidence for this from our ambulatory recordings of rectal activity. Whether the effect on anal continence is via a change in rectal compliance, irritability, and motor patterns, or facilitation or stabilisation of anal pressure activity requires further investigation.
Use of the percutaneous lead to assess the value of sacral nerve stimulation in faecal incontinence was not straightforward. In faecal incontinence a trial period of one week may not be sufficient to assess the clinical effects of the stimulation as some patients with severe incontinence have intermittent symptoms. Unlike urinary incontinence faecal incontinence is dependent on stool consistency and patients commonly become continent while in hospital. A longer trial period may therefore be required to determine whether a patient will benefit from a permanent implant.
Keeping the leads in place for one week proved to be difficult. A similar problem of test wire displacement has also been reported by urologists and new electrodes with enhanced anchoring properties are currently being developed. Operatively positioned and fixed electrodes avoid this problem and also allow for a longer trial period. In a previous small study24 the clinical success rates with the PNE tests were improved from 50% with percutaneously placed wire to 80% using an operatively fixed electrode.
Longer term studies with permanently placed electrodes will be required to determine the long term efficacy, with shorter term studies such as this providing information about likely responders and mechanism of action. In a small number of patients who have been permanently implanted, the therapeutic benefit seems to be maintained11 (this is borne out by personal unpublished observations).
This study has shown a symptomatic benefit in the short term using sacral nerve stimulation for patients with faecal incontinence and circumferentially intact sphincter muscles. Given that the mechanism of benefit is unlikely to be solely related to direct sphincter stimulation, this therapy may have a broader application to include selected patients with structural sphincter damage which is not amenable to simple repair. Even if the pudendal nerves are impaired in function this therapy may have a place, although this remains to be tested. Further studies are required to determine the long term benefit in patients with a range of aetiologies for their incontinence.
Acknowledgments
This work has been published in part as abstracts inGut (1997;40:A53) and Gastroenterology(1997;112:A842). We are grateful to R A Schmidt for helpful comments on the manuscript and to C Dore for statistical analysis.
Abbreviations
- EMG
- electromyography
- PNE
- percutaneous nerve evaluation