Article Text

Abstract
BACKGROUND Hiatus hernia and lower oesophageal sphincter hypotension are often viewed as opposing hypotheses for gastro-oesophageal junction incompetence.
AIMS To examine the interaction between hiatus hernia and lower oesophageal sphincter hypotension.
METHODS In seven normal subjects and seven patients with hiatus hernia, the squamocolumnar junction and intragastric margin of the gastro-oesophageal junction were marked with endoscopically placed clips. Axial and radial characteristics of the gastro-oesophageal junction high pressure zone were mapped relative to the hiatus and clips during concurrent fluoroscopy and manometry. Responses to inspiration and abdominal compression were also analysed.
RESULTS In normal individuals the squamocolumnar junction was 0.5 cm below the hiatus and the gastro-oesophageal junction high pressure zone extended 1.1 cm distal to that. In those with hiatus hernia, the gastro-oesophageal junction high pressure zone had two discrete segments, one proximal to the squamocolumnar junction and one distal, attributable to the extrinsic compression within the hiatal canal. Inspiration and abdominal compression mainly augmented the distal one. Simulation of hernia reduction by algebraically summing the proximal segment pressures with the hiatal canal pressures restored normal maximal pressure, radial asymmetry, and dynamic responses of the gastro-oesophageal junction.
CONCLUSIONS Hiatus hernia reduces lower oesophageal sphincter pressure and alters its dynamic responsiveness by spatially separating pressure components derived from the intrinsic lower oesophageal sphincter and the extrinsic compression of the oesophagus within the hiatal canal.
- hiatus hernia
- lower oesophageal sphincter
- reflux disease
- manometry
Abbreviations
- LOS
- lower oesophageal sphincter
- SCJ
- squamocolumnar junction
- HPZ
- high pressure zone
- GOJ
- gastro-oesophageal junction
- EMG
- electromyography
Statistics from Altmetric.com
Investigations into the mechanisms of gastro-oesophageal reflux have identified transient lower oesophageal sphincter (LOS) relaxation as a dominant mechanism, but also observed that strain induced reflux or free reflux could occur during periods of LOS hypotonicity.1 ,2 These studies also emphasised the variability of each individual’s LOS pressure over time during prolonged recordings and the relatively poor sensitivity of this measurement for the detection of reflux disease. None the less, LOS hypotonicity does become increasingly common with increasing severity of oesophagitis,3 ,4 and multivariate analysis does suggest LOS hypotonicity to be an independent risk factor for both the presence and grade of oesophagitis.5 From a mechanistic viewpoint, factors which diminish the LOS pressure predispose to strain induced or free reflux and these mechanisms are more dominant with increasing grades of oesophagitis.6 Manometric data also suggest that strain induced reflux is more common in the setting of hiatus hernia.7 Another association that is difficult to ignore is that between oesophagitis and hiatus hernia. Endoscopic and radiographic studies have found that 50–94% of patients with reflux disease have hiatus hernia, whereas the prevalence of hernias in control subjects was substantially less within each study.8-10 Furthermore, stepwise regression analysis of the susceptibility to reflux by the strain mechanism identified increasing size of hiatus hernia, diminishing values of LOS pressure, and an interaction between hernia size and LOS pressure as significant independent risks.11 These observations suggest that hiatus hernia may hinder LOS function, presumably by modifying the diaphragmatic contribution to gastro-oesophageal junction competence.12 ,13 With that in mind, the aim of this study was to evaluate the effect of anatomically well defined hiatus hernia on manometric characteristics of the gastro-oesophageal junction pressure profile.
Methods
Endoscopic, fluoroscopic, and manometric landmarks of the gastro-oesophageal junction of patients with hiatus hernia and volunteer subjects were compared to examine the influence of hiatus hernia on the intraluminal pressure profile. The protocol was approved by the Northwestern University Institutional Review Board and informed consent was obtained from participants.
SUBJECT GROUPS
Subjects for this investigation were a group of normal volunteers and patients with symptomatic reflux disease categorised as having hiatus hernia and without Barrett’s epithelium on the basis of prior, clinically indicated, endoscopic evaluation. Of a total of nine volunteers and nine patients evaluated, seven in each group (four men, three women) satisfied our criteria for inclusion after endoscopic and fluoroscopic assessment of the position of the squamocolumnar junction relative to the diaphragm (see below). The mean age of the seven controls was 38 (6) years and that of the hernia patients was 44 (5) years; all of the hernia patients had reflux disease that was in endoscopic and symptomatic remission as a result of maintenance treatment with a proton pump inhibitor (n=5) or a histamine H2 receptor antagonist (n=2).
ENDOSCOPIC LANDMARKS OF THE GASTRO-OESOPHAGEAL JUNCTION MARKED BY MUCOSAL CLIPPING
Subjects fasted overnight before undergoing an oesophagoscopy under sedation with intravenous midazolam and meperidine. During this procedure, two 11 mm stainless steel clips were attached to the oesophageal and gastric mucosa using an endoscopic clip fixing device (HX-3L, Olympus America Inc., Lake Success, New York, USA). The proximal clip was attached at the squamocolumnar junction and the distal clip was attached at the greater curvature side of the entryway to the stomach as viewed in retroflexion. If the squamocolumnar junction was irregular the clip was affixed at a median location between its proximal and distal extremes. The anatomical correlate of the intragastric clip was distinct for the two groups; in the normals this correlated with the intragastric flap valve as defined by Hillet al,14 whereas in the hernia subjects the intragastric clip marked the lower margin of the diaphragmatic hiatus (fig 1). Following completion of the clipping procedure, subjects were allowed to recover from sedation for at least one hour before proceeding with the manometric and fluoroscopic studies. The oesophagus was again imaged fluoroscopically one month after the study, and all residual clips were removed endoscopically.

Positioning of mucosal clips in normal subjects and patients with hiatus hernia. The central panel is a tracing from a fluoroscopic image of a normal subject illustrating the position of the mucosal clips relative to fluoroscopic landmarks. The opposing open arrows indicate the position of the centre of the hiatal canal as determined by the impression into the barium column during a barium swallow.
MANOMETRIC AND FLUOROSCOPIC ASSESSMENT OF THE GASTRO-OESOPHAGEAL JUNCTION
Prior to manometric study, subjects were imaged fluoroscopically in a supine posture to ascertain their suitability for inclusion in the normal or hiatus hernia groups. Two 5 ml dilute liquid barium swallows (Liquid E-Z, E-Z-EM Inc., Westbury, New York, USA) were imaged to determine the end expiratory position of the diaphragmatic impression on the oesophagus or stomach. Swallows imaged fluoroscopically were recorded with a videotape recorder (Sony VO 9800). Subjects were then imaged at a time that they had not swallowed for at least 30 seconds to ascertain the position of the mucosal attachment of the squamocolumnar junction clip relative to the position of the hiatal impression that had been ascertained during the barium swallows. Measurements were made from digitised images using the vertebrae as spatial references, the length of the clips to correct for magnification, and image analysis software.15 To qualify as normal, the squamocolumnar junction clip needed to be beneath the diaphragmatic hiatus while our requirement for hiatus hernia was that the squamocolumnar junction clip be at least 1 cm proximal to the hiatus. Application of these criteria resulted in exclusion of two normal subjects whose squamocolumnar junction was slightly above the diaphragm and two patients with hiatus hernia whose squamocolumnar junction was less than 1 cm above the diaphragm.
Subjects were then studied with concurrent fluoroscopy and manometry. A silicone rubber manometric assembly with eight side hole recording sites situated at the same axial level but arranged at 45° increments radially was used (Dentsleeve Pty, 77C Gibson St, Bowden, South Australia). Asymmetric radio-opaque markings on the manometric assembly permitted fluoroscopic determination of axial position and radial orientation of the side hole sites. Each catheter lumen was perfused by a low compliance perfusion pump at 0.3 ml/min (Dentsleeve Mark II, 16 channel model), connected to a computer polygraph set at a sampling frequency of 40 Hz (Neomedix Systems Pty Ltd, Warriewood, NSW, Australia), and processed utilising Gastromac software (Neomedix). Response characteristics of each manometric channel exceeded 200 mm Hg/s. Data for determination of the gastro-oesophageal junction pressure topography were obtained during fluoroscopically imaged pull throughs of the gastro-oesophageal junction at 0.5 cm/s using a mechanical catheter pulling device (Medtronic Synectics, 3850 Victoria Street North, Mail Stop V215, Shoreview, Minnesota, USA). Manometric tracings and fluoroscopic images were synchronised using a video timer (model VC 436, Thalner Electronics Laboratories, Ann Arbor, Michigan, USA) that encoded time in hundredths of a second on each video frame and sent a 1V-10 ms pulse to an instrumentation channel of the polygraph at whole second intervals. Pull throughs were done during suspended respiration in three conditions: end expiration; strong respiratory effort with a closed glottis (Müller manoeuvre); and end expiration with an abdominal binder inflated to 100 mm Hg.
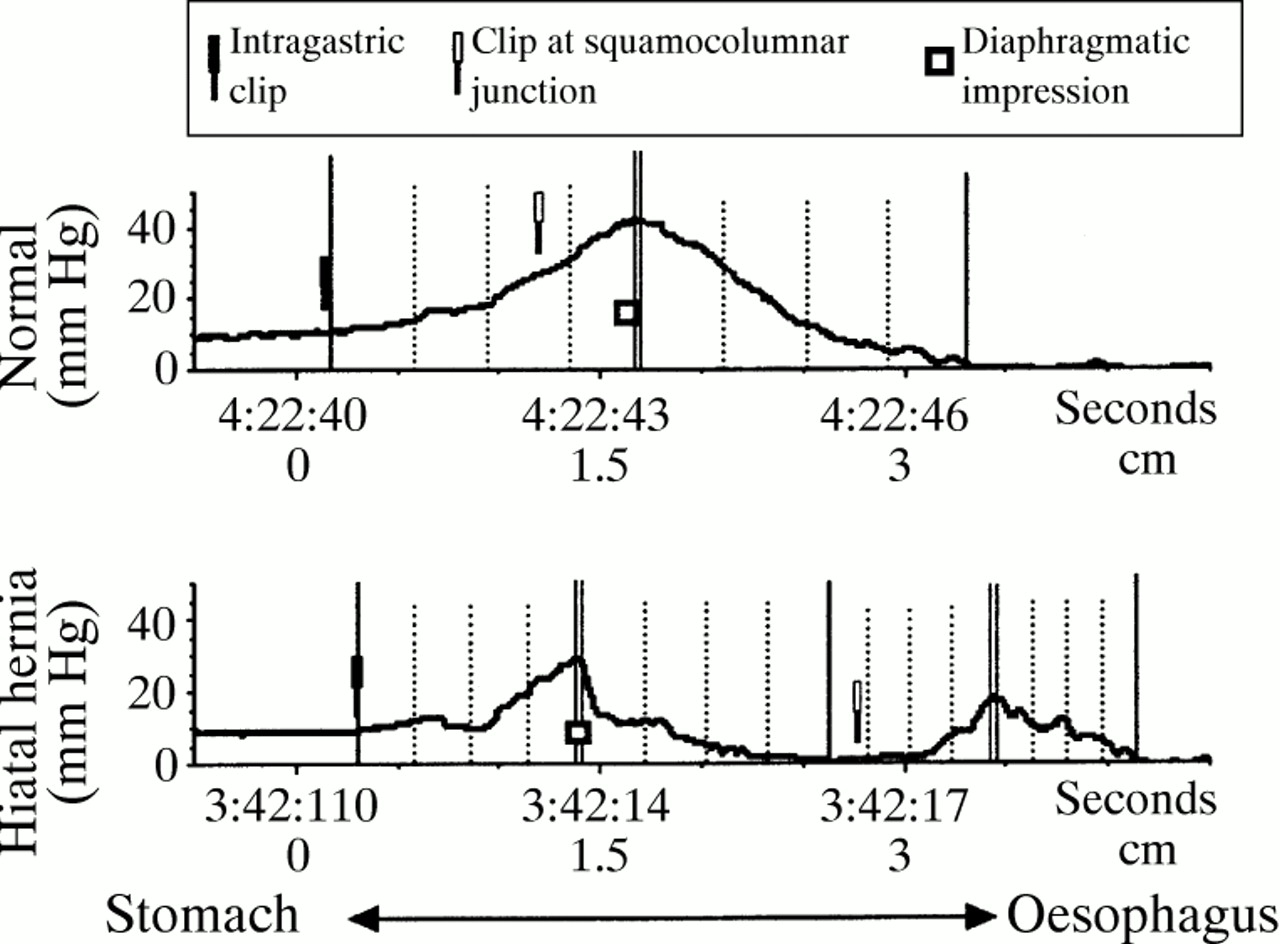
DATA ANALYSIS
The recording from each manometric lumen of each pull through was analysed to relate the pressure signal with the squamocolumnar junction, the intragastric clip, and the fluoroscopic position of the hiatal indentation as determined during the initial barium swallows. This was accomplished by digitising selected images and relating the position of the asymmetric radio-opaque markers on the manometric assembly to the mucosal attachment points of the clips at each time point of the pull through. Axial position zero was defined as the midpoint of the hiatal canal; all pressures were referenced to atmospheric. Pressure tracings were then characterised as having a single or double peak (fig 2). Each slope of each peak was further characterised by the axial location and pressure value of the peak, nadir, and three equispaced intermediate points. Thus, pressure values were obtained for nine axial positions in the case of a single high pressure zone and 17 in the case of a double peaked axial pressure profile. Group data for normals and hiatal hernia subjects were summarised by the median axial coordinate (relative to position zero) and the corresponding median pressure value of each axial position of each peak of each radial side hole orientation of each pull through condition. Three dimensional representations of gastro-oesophageal junction pressure topography relative to the hiatus and mucosal clips were created from the median data for each group and condition by aligning the radial pressure profiles relative to each other using a computer workstation (Silicon Graphics Personal IRIS; Silicon Graphics, Mountain View, California, USA) and three dimensional graphics and animation software (Advanced Visualizer, Version 4.1, Wavefront Technologies, Santa Barbara, California, USA).

Examples of manometric pull through tracings with single (top) and double (bottom) peak axial pressure profiles. The median axial position and the pressure of the maximum (double vertical lines), minimum (single vertical lines), and three equispaced intermediate positions (vertical dotted lines) of each upward and downward slope were used to summarise group data. The open clips show the position of the squamocolumnar junction, the closed clips indicate the position of the intragastric clip, and the open squares indicate the centre of the hiatal canal.
Calculations of percentage radial asymmetry for pressure peaks identified by the methodology in fig 2 were made by applying the formula: percentage asymmetry = (1 − minimal radial pressure/maximal radial pressure) × 100. Thus, a circle has 0% asymmetry. Comparisons of pressure topography characteristics between groups and conditions were made using Student’s paired or unpairedt test.
Simulation of hiatal hernia reduction was done mathematically by repositioning the squamocolumnar junction of the hiatal hernia subjects (guided by the mucosal clip) along with the associated sphincter pressures to the median subdiaphragmatic position observed in the normals. The modelled radial pressure values at each axial coordinate of the simulated hernia reduction thus equalled the algebraic sum of pressure attributable to the stationary distal high pressure zone and corresponding repositioned proximal high pressure zone values.
Results
PRESSURE TOPOGRAPHY OF THE GASTRO-OESOPHAGEAL JUNCTION
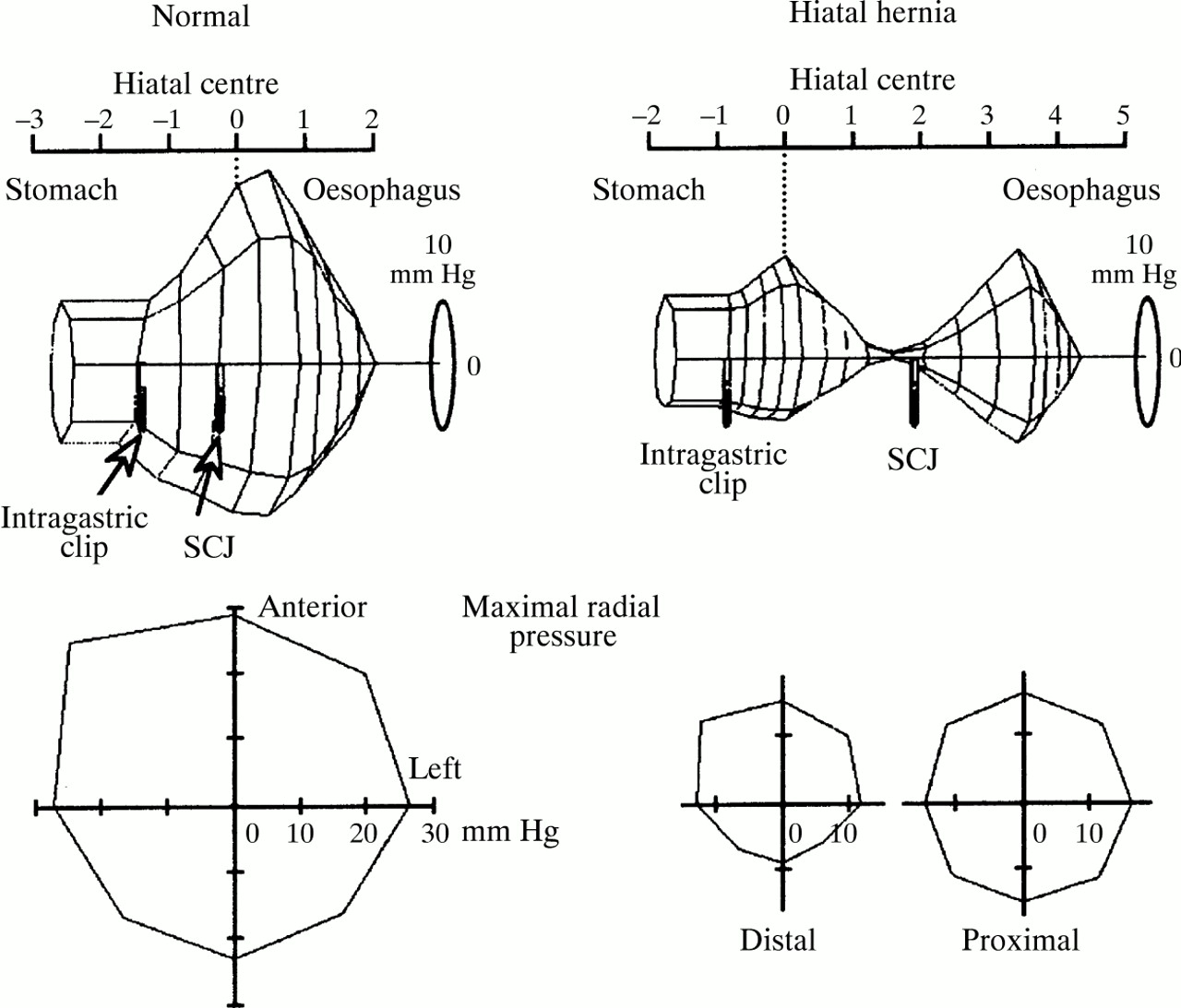
Median pressure values at axial and radial coordinates of the gastro-oesophageal junction high pressure zones of normal and hiatal hernia subjects are diagrammed as three dimensional wireframes in fig3. In each case, the median position of the squamocolumnar junction is indicated by the proximal mucosal clip while the median position of the intragastric margin of the gastro-oesophageal junction is indicated by the distal mucosal clip. Table 1 shows corresponding pressure, length, and radial asymmetry characteristics of the high pressure zones. A distinguishing feature of the hernia group was a double peaked pressure profile. As evidenced by the maximal radial pressure profiles in the lower panels of fig 3, the distal high pressure zone had notable radial asymmetry while the proximal one was nearly circular. In the hernia subjects, the centre of the distal high pressure zone occurred 2.1 (1.0) cm distal to the squamocolumnar junction, corresponding precisely with the anatomical location of the hiatal canal as determined by prior fluoroscopic analysis. In the normal subjects, however, the median position of the squamocolumnar junction was 0.5 (0.1) cm distal to the centre of the hiatal canal and the intragastric margin of the high pressure zone extended 1.1 (0.1) cm distal to the squamocolumnar junction. These spatial relations imply that the distal high pressure zone of the hernia subjects was attributable to the extrinsic effect of the hiatal canal (as opposed to the intrinsic oesophageal sphincter) as normal subjects exhibited no high pressure zone at a location so distal to the squamocolumnar junction.

Axial (top) and radial (bottom) pressure topography of the gastro-oesophageal junction of normal subjects and patients with hiatus hernia. The radial pressure profiles at the peak of each high pressure zone are diagrammed underneath. Position zero on the axial scale is the midpoint of the diaphragmatic hiatus. The wireframe representations are rotated such that the right anterior pressure is at the top and left posterior pressure is at the bottom, thereby accentuating the radial pressure asymmetry. The proximal clip indicates the median position of the squamocolumnar junction (SCJ) and the distal clip marks the median position of the intragastric aspect to the gastro-oesophageal junction as imaged endoscopically. All values of length and pressure are the medians of the subject groups.
Gastro-oesophageal junction high pressure zone (HPZ) characteristics of normal subjects and patients with hiatus hernia
DYNAMIC EFFECTS OF ABDOMINAL COMPRESSION AND THE MÜLLER MANOEUVRE
Abdominal compression augmented the gastro-oesophageal junction pressure of both the normal subjects and the patients with hiatal hernia as evident in fig 4. Abdominal compression also resulted in proximal shifting of both the hiatal centre and squamocolumnar junction relative to the vertebral reference point by approximately 0.5 cm in all cases, with no apparent discordance between the degree of diaphragmatic movement and squamocolumnar junction movement (table 2). Within the hernia group, abdominal compression augmented the pressure within the distal (hiatal) element to a degree that was equal to the pressure augmentation observed in normal subjects (table 2). Although augmentation of the proximal element of the high pressure zone was also evident in the patients with hiatus hernia, this was to a lesser degree than that of the hiatal element. Furthermore, the radial asymmetry of the proximal pressure augmentation, with anterior pressure dominating, was similar to the radial pressure asymmetry within the hiatus (fig 4).
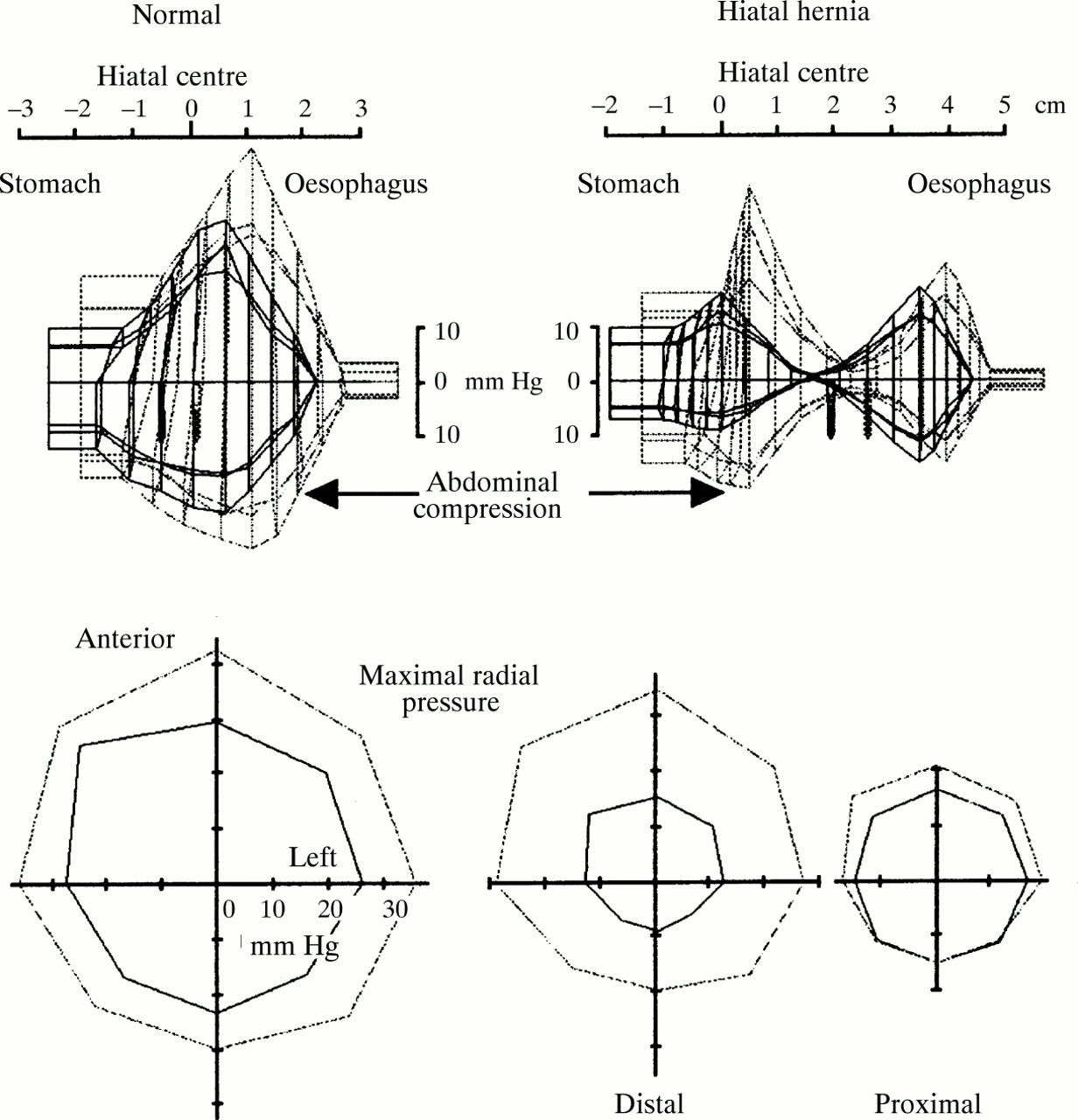
Change in the pressure topography of the gastro-oesophageal junction resulting from abdominal compression with an abdominal binder. The solid lines represent the condition at rest (represented as in fig 3) and the broken lines show movement and pressure augmentation associated with abdominal compression. Note that abdominal compression shifts the position of the squamocolumnar junction proximally by about 0.5 cm, increases the intragastric pressure, and causes a substantial increase in pressure within the hiatal canal of the hernia subjects. All values of length and pressure are the medians of the subject groups.
Changes in pressure, length, and position of the gastro-oesophageal junction (GOJ) high pressure zone (HPZ) caused by abdominal compression
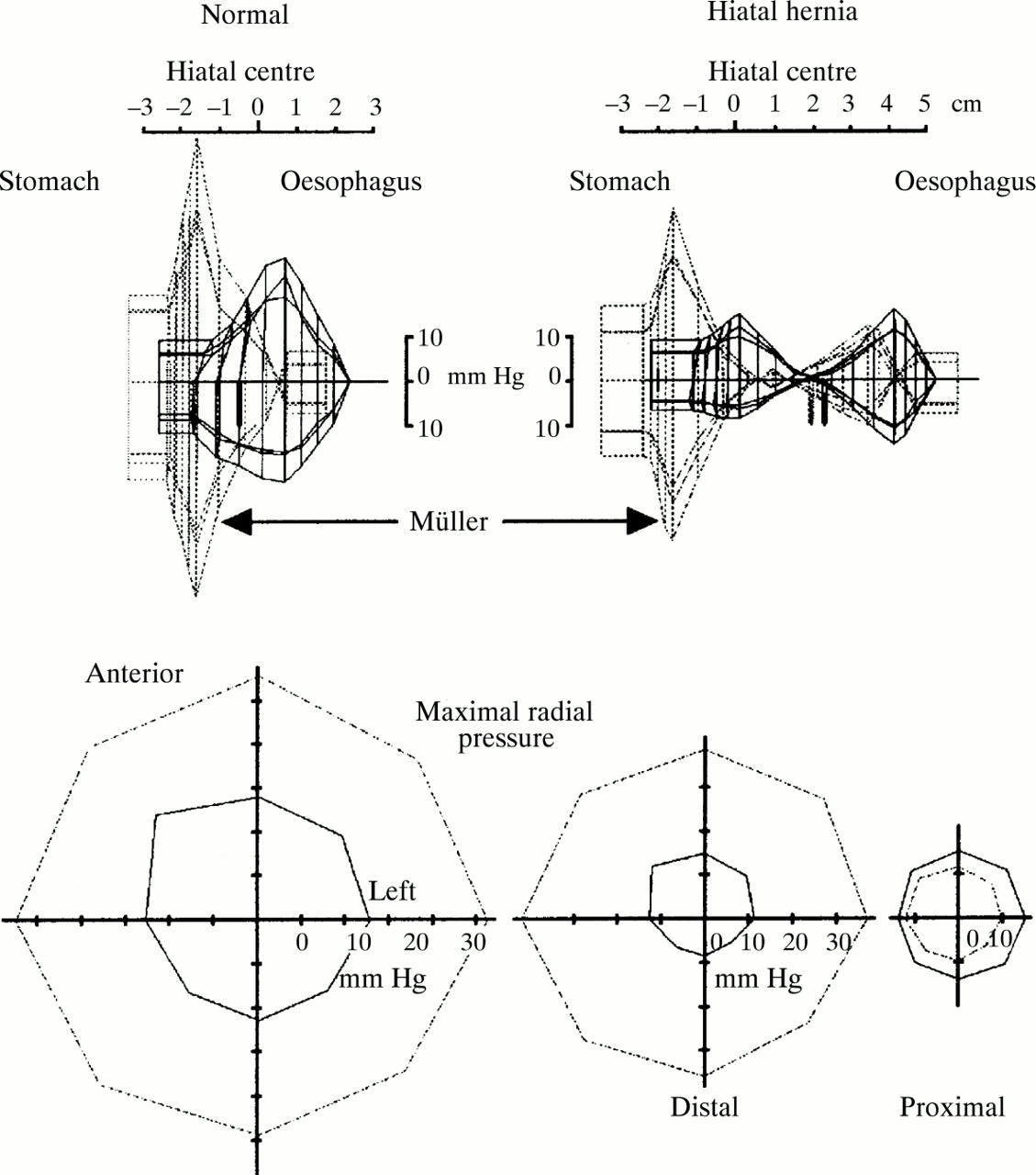
The Müller manoeuvre augmented the gastro-oesophageal junction high pressure zone and shifted both the hiatal centre and the high pressure zone distally in the normal subjects (fig 5, top left). In those with hiatal hernia, however, although the distal element of the high pressure zone was augmented to a similar degree to that seen among the normal subjects (fig 5, table 3), the magnitude of the proximal element of the high pressure zone was slightly reduced as was the pressure in the more proximal oesophagus (−5 mm Hg). Figure 5 and table 3 also show that movement of the proximal and distal high pressure zones in the patients with hiatal hernia during the Müller manoeuvre was unequal. While the distal high pressure zone shifted 1.8 cm distally with the Müller manoeuvre, consistent with that observed in the normal subjects, the proximal element moved only a third as much. Thus, while the normal subjects exhibit a 1.1:1.7 ratio of movement between the squamocolumnar junction and diaphragm, this ratio is reduced to 0.4:1.8 in those with hiatus hernia, thereby permitting more movement of the diaphragm relative to the oesophagus.

Change in the pressure topography of the gastro-oesophageal junction resulting from a Müller manoeuvre. The solid lines represent the condition at rest (represented as in fig 3) and the broken lines show movement and pressure augmentation associated with inspiration against a closed glottis. Note that the Müller manoeuvre shifts the position of the squamocolumnar junction distally by more than 1 cm in the normals but by less than 0.5 cm in the patients with hiatus hernia. In both subject groups, the Müller manoeuvre increases the intragastric pressure, and causes a substantial increase in pressure within the hiatal canal. All values of length and pressure are the medians of the subject groups.
Changes in pressure, length, and position of the gastro-oesophageal junction high pressure zone caused by Müller manoeuvre
SIMULATION OF HERNIA REDUCTION
Using the fluoroscopically ascertained position of the hiatal centre, and maintaining a fixed relation between the proximal high pressure zone and the endoscopically marked squamocolumnar junction, hiatal hernia reduction was simulated by repositioning the proximal high pressure zone a measured distance (mean 2.6 cm) into the hiatal canal. Figure 6 illustrates the resultant gastro-oesophageal junction pressure topography. As table 4 shows, this manipulation transforms the high pressure zone of the patients with hiatal hernia into one with many similarities to that of the normal subjects; in particular, maximal pressure, percentage asymmetry, and dynamic response to both abdominal compression and the Müller manoeuvre. The only significant difference between the pressure topography of the normal subjects and patients with hiatal hernia after the simulation of hernia reduction was in the overall length of the gastro-oesophageal junction high pressure zone. When this remaining difference is subdivided into segments proximal and distal to the squamocolumnar junction, it is evident that the difference results primarily from characteristics distal to the squamocolumnar junction (fig 6 (shaded areas), table4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simulation of reducing the hiatus hernia by algebraically repositioning the pressure values of the intrinsic LOS (pressure peak proximal to the squamocolumnar junction (SCJ)) to within the extrinsically determined pressure of the hiatal canal. For each subject the positioning of the proximal high pressure zone was such that the squamocolumnar junction mucosal clip attained the median normal position, 0.5 cm distal to the hiatus. The shaded area indicates the portion of the sphincter segment distal to the squamocolumnar junction in the normals and in the transposed panels. All values of length and pressure are the medians of the subject groups.
Comparison of parameters of the gastro-oesophageal junction high pressure zone and its response to abdominal compression (AC) and Müller manoeuvre of normal subjects, patients with hiatus hernia, and patients with a hernia after algebraic simulation of hiatus hernia reduction
Discussion
A high pressure zone detectable by intraluminal oesophageal manometry and attributable to the extrinsic effect of the diaphragmatic hiatus was initially described in the opossum, a species characterised by anatomic separation of the LOS and hiatus.16 In that work, Schulze et al noted this effect as the likely explanation for the double pressure peak observed in pull through recordings obtained in some patients with hiatus hernia as described by Code et al.17 In the present investigation, we used similar methodology to define the pressure topography of the gastro-oesophageal junction relative to the squamocolumnar junction and to the diaphragmatic hiatus in subjects with and without sliding hiatus hernia. Endoscopically placed clips were used to localise the squamocolumnar junction relative to radio-opaque markings on a manometric assembly as the assembly was withdrawn across the gastro-oesophageal junction during fluoroscopy. Findings in the patients with hiatus hernia showed that, even in end expiration, the hiatal canal contributed to the overall pressure topography of the gastro-oesophageal junction as evident by a double peaked pressure profile. Assuming that extrinsic and intrinsic pressures are additive when superimposed, this separation of the intrinsic LOS from the hiatal canal results in an obligate decrement of peak gastro-oesophageal junction pressure with hiatus hernia. Conversely, utilising the metal clip at the squamocolumnar junction as a landmark to gauge the appropriate degree of reduction of the hernia, repositioning the intrinsic lower oesophageal sphincter back within the hiatal canal effectively restored a normal maximal pressure. Furthermore, our findings suggest that the normal radial asymmetry of the gastro-oesophageal junction pressure is attributable to the extrinsic contribution of the hiatal canal, as the intrinsic LOS was radially symmetric in the patients with hiatus hernia.
The observation that the hiatal canal contributes to gastro-oesophageal junction pressure in patients with hiatus hernia during both inspiration and expiration is consistent with previous observations made in both humans and animals. Klein et alstudied the thoracoabdominal junction of 10 patients after surgical resection of the lower oesophageal sphincter as part of cancer therapy.18 Subsequent manometric analysis revealed an end expiratory intraluminal pressure of 6 (SE 1) mm Hg within the “sphincterless” gastro-oesophageal junction, a value very similar to the 3 (0.2) mm Hg observed within the hiatal canal of our patients with hiatus hernia. Relevant animal data come from experimentally severing the phreno-oesophageal ligament in dogs; analogous to the effect of axial hiatus hernia in which the ligament is stretched and its diaphragmatic attachments loosened.19 ,20 Severing the ligament substantially reduced peak gastro-oesophageal junction pressure, which was then restored with reanastomosis.21The only contradictory data seem to be from diaphragmatic electromyography (EMG) recordings which strongly support the notion of a phasic, but not tonic, diaphragmatic contribution to gastro-oesophageal junction pressure.12 ,13 However, relying on EMG recordings to represent completely the diaphragmatic contribution to gastro-oesophageal junction pressure ignores the possible contribution of passive forces such as diaphragmatic and ligamentous elasticity to intraluminal pressure. Certainly, in the case of the upper oesophageal sphincter, such passive forces contribute an intraluminal pressure of similar magnitude after experimental abolition of the myogenic tone.22
Patients with hiatus hernia exhibited augmentation of gastro-oesophageal junction pressure of similar magnitude to normal subjects in response to either abdominal compression or deep inspiration (figs 4 and 5; table 2). Pressure augmentation in the patients with hiatus hernia was almost entirely attributable to the diaphragmatic sphincter component; the minimal (asymmetric) changes observed proximal to the squamocolumnar junction were probably attributable to overlap with the diaphragmatic segment. This hypothesis is supported by the brisk diaphragmatic EMG responses to these sphincteric challenges described both in humans and animals. The magnitude of the resultant gastro-oesophageal junction pressure augmentation paralleled that of the integrated EMG signal and was unaffected by concomitant intrinsic sphincter relaxation induced by oesophageal balloon distension or swallowing.23-26 These observations, coupled with the observation that hiatus hernia progressively compromises the competence of the gastro-oesophageal junction to increases in intra-abdominal pressure,11suggest that axial separation of the diaphragmatic sphincter component from the intrinsic sphincter is detrimental to its function. A possible mechanism for this functional decrement is entrapment of gastric juice above the hiatus, a phenomenon exacerbated by loosening of phreno-oesophageal attachments which allows substantial movement of the intrinsic sphincter element relative to the hiatus (table 2).
The most confusing segment of oesophageal anatomy is that distal to the squamocolumnar junction, referred to by Inglefinger as an anatomic and functional “no mans land”.27 Highlighting this confusion, Wolf remarked that, “it is indeed strange that, when normally located below the hiatus, the ‘submerged segment’ resembles the esophagus while, when displaced above the hiatus, it resembles stomach. In fact, when a large hiatal hernia is present, the original submerged segment is incorporated into the hernia sac”.28 Our measurements suggest that when intra-abdominal length is defined as the segment of the high pressure zone distal to the centre of the hiatal canal, this is mainly a determination of whether or not hiatus hernia is present (fig 3). In normal subjects, this extends 1.1 cm distal to the squamocolumnar junction and 1.6 cm distal to the hiatal canal (fig 6). Anatomical studies by Liebermann-Meffert et al support this estimate of the extent that the sphincteric segment extends distal to the squamocolumnar junction.29 These authors described a “fold transition line”, evident in postmortem specimens which seems analogous to the intragastric margin of the gastro-oesophageal junction as we defined it endoscopically. Liebermann-Meffertet al describe this as the area of greatest muscle wall thickness, oriented obliquely, and related to the angle of His as identified externally. The squamocolumnar junction was 10.5 (SD 4.4) mm proximal to the fold transition line when measured along the greater curvature, almost identical to the 11 (SE 1) mm calculated using our methodology. Although the relevance of this distal sphincter segment is controversial, Hill et al found the integrity of this “flap valve” to correlate with gastro-oesophageal junction competence against an antegrade pressure gradient in postmortem experiments.14 The intriguing observation that this is the one aspect of gastro-oesophageal junction pressure topography not restored by simulated reduction of a hiatal hernia tends to support the widely held surgical opinion that effective antireflux surgery must additionally entail some reconstruction of this segment.14 ,30
In summary, this experiment correlated anatomical, manometric, and radiographic representations of the gastro-oesophageal junction in normal subjects and in individuals with hiatus hernia. The major findings of the work suggest that hiatus hernia alters the pressure topography of the gastro-oesophageal junction by reducing its maximal pressure, altering its radial asymmetry, and reducing the sub-hiatal length of the high pressure zone. All of these changes, except the latter, can be reversed by simulating reduction of hiatus hernia. The implication of these findings is that by altering the pressure topography of the gastro-oesophageal junction, hiatus hernia may increase susceptibility to reflux events associated with diminished LOS pressure—for example, strain induced or free reflux, as opposed to reflux by transient LOS relaxation.
Acknowledgments
This work was supported by grant RO1 DC00646 (PJK) from the Public Health Service.
Abbreviations
- LOS
- lower oesophageal sphincter
- SCJ
- squamocolumnar junction
- HPZ
- high pressure zone
- GOJ
- gastro-oesophageal junction
- EMG
- electromyography