Article Text

Abstract
BACKGROUND Treatment of acromegaly with octreotide increases the proportion of deoxycholic acid in, and the cholesterol saturation of, bile and induces the formation of gallstones. Prolongation of intestinal transit has been proposed as the mechanism for the increase in the proportion of deoxycholic acid in bile.
AIMS To study the effects of octreotide on intestinal transit in acromegalic patients during octreotide treatment, and to examine the relation between intestinal transit and bile acid composition in fasting serum.
METHODS Mouth to caecum and large bowel transit times, and the proportion of deoxycholic acid in fasting serum were measured in non-acromegalic controls, acromegalic patients untreated with octreotide, acromegalics on long term octreotide, and patients with simple constipation. Intestinal transit and the proportion of deoxycholic acid were compared in acromegalic patients before and during octreotide.
RESULTS Acromegalics untreated with octreotide had longer mouth to caecum and large bowel transit times than controls. Intestinal transit was further prolonged by chronic octreotide treatment. There were significant linear relations between large bowel transit time and the proportion of deoxycholic acid in the total, conjugated, and unconjugated fractions of fasting serum.
CONCLUSIONS These data support the hypothesis that, by prolonging large bowel transit, octreotide increases the proportion of deoxycholic acid in fasting serum (and, by implication, in bile) and thereby the risk of gallstone formation.
- deoxycholic acid
- octreotide
- acromegaly
- gallstones
- large bowel transit time
- mouth to caecum transit time
Abbreviations
- CA
- cholic acid
- CDCA
- chenodeoxycholic acid
- DCA
- deoxycholic acid
- IGF-1
- insulin-like growth factor 1
- LBTT
- large bowel transit time
- LCA
- lithocholic acid
- MCTT
- mouth to caecum transit time
- UDCA
- ursodeoxycholic acid
Statistics from Altmetric.com
Octreotide, the long acting somatostatin analogue, suppresses circulating growth hormone and insulin-like growth factor 1 (IGF-1) levels; it is an effective treatment for acromegaly.1 ,2However after one to two years octreotide treatment, 10–63% (mean 29%) of patients develop cholesterol rich gallstones.3 ,4
We5 and others6-9 have shown that octreotide not only impairs meal stimulated gall bladder emptying; it also induces changes in gall bladder bile composition and physical chemistry10 similar to those seen in “conventional” cholelithiasis (that is, gallstone disease, unrelated to acromegaly or octreotide treatment). These changes include: supersaturated bile, excess biliary cholesterol transported in vesicles, a high vesicular cholesterol:phospholipid molar ratio, and abnormally rapid nucleation of cholesterol microcrystals.10
Octreotide treatment is also associated with a twofold increase in the proportion of deoxycholic acid in gall bladder bile. Paired studies (before and during octreotide treatment) have suggested that this increase in deoxycholic acid in bile is due to the octreotide treatment, independent of stone formation.10 Increases in biliary deoxycholic acid have long been implicated in the pathogenesis of cholesterol rich gallstones.11
In man, deoxycholic acid is formed by the bacterial conversion (deconjugation, followed by 7α-dehydroxylation) of conjugated or amidated (taurine or glycine) cholic acid, in the caecum and colon.12 ,13 Some of the newly formed unconjugated deoxycholic acid is then absorbed, mainly by passive non-ionic diffusion.14 ,15
There is increasing evidence that changes in intestinal transit influence both deoxycholic acid formation in, and absorption from, the large bowel. Thus, when colonic transit is prolonged, the proportion of deoxycholic acid in bile increases.16 To date, however, most observations on the effects of octreotide on intestinal transit have been confined to acute studies in the small bowel.17-20 There are few data on the effects of chronic octreotide administration on large bowel transit, which is important since, as noted above, deoxycholic acid formation and absorption occur mainly in the right colon.12 ,13
The aims of this study, therefore, were: to extend our previous observations5 on the effects of octreotide on both small and large bowel transit in acromegalic patients studied before and during therapy; and to examine the relation between intestinal transit and bile acid composition in fasting serum. In particular, we wished to know if the increase in the proportion of deoxycholic acid seen during octreotide treatment resulted from prolonged large bowel transit.
Methods
SUBJECTS
Four groups of individuals were studied. Sixteen non-acromegalic control subjects (mean age 37 (SEM 3.2) years, range 22–64; seven women) were recruited from laboratory staff volunteers from Guy’s Hospital.
Sixteen acromegalic patients (mean age 50 (3.9) years, range 23–72; 10 women) were untreated with octreotide. The clinical diagnosis of acromegaly was confirmed by the following criteria: failure of suppression of serum growth hormone (GH) levels to less than 2 mU/l after oral glucose (75 g); a raised mean daily serum GH level of more than 5 mU/l (averaged from five samples taken over a 12 hour period); and increased age adjusted IGF-1 levels.21
Sixteen acromegalic patients (mean age 50 (3.6) years, range 23–67; eight women) were treated for 3–48 (median 12) months with 300–600 μg octreotide/day by subcutaneous injection. Before treatment, these patients also fulfilled the diagnostic criteria for acromegaly as defined above.
Sixteen patients (mean age 43 (3.4) years, range 28–70; 13 women) with simple idiopathic constipation were recruited from the outpatient clinic at Guy’s Hospital.
None of the individuals studied had abnormal liver function tests or known intestinal disease. All were gallstone free, as judged by ultrasound. None had taken antibiotics or laxatives within four weeks of serum sampling.
STUDY DESIGN
Mouth to caecum and large bowel transit times, and the proportion of deoxycholic acid in fasting serum were measured in the four groups of individuals. We also carried out a paired study in a subgroup of nine acromegalic patients (mean age 45 (5.7) years, range 23–67; five women) who were examined before and during octreotide treatment 300–600 μg/day for 3–24 (median 4) months.
As well as measuring the proportion of deoxycholic acid (total and also unconjugated and conjugated fractions) in fasting serum, we also calculated the proportions of the other major bile acids (cholic, chenodeoxycholic, ursodeoxycholic, and lithocholic acids) in the same serum samples. We then performed univariate analyses to examine the relations between mouth to caecum and large bowel transit times, and the proportions of the unconjugated, conjugated, and total bile acids in serum.
There was no pharmacological manipulation of intestinal transit, other than the octreotide treatment in 16 of the acromegalic patients. Furthermore, all 64 individuals were advised to maintain their regular diet. In other words, for the correlations between intestinal transit and the proportions of bile acids in serum, we were relying on a spontaneous scatter of results, rather than on induced changes.
PROTOCOL
Intestinal transit time
We used established protocols5 for the measurement of mouth to caecum and large bowel transit times on a single visit to the hospital. In brief, following a 12 hour overnight fast, a fasting blood sample (10 ml) was taken from which the serum was collected and stored at −20°C until analysed. The individuals then consumed a fat rich, liquid test meal (250 ml “Ensure”) together with 20 ml of lactulose as a substrate for breath hydrogen production. Thereafter, the mouth to caecum transit time was measured using the lactulose breath hydrogen technique.22 End expiratory breath samples were collected in a 20 ml plastic syringe, 30 minutes and immediately before the test meal, and then every 15 minutes, until either there was a late peak of breath hydrogen (a rise of greater than 10 ppm above baseline on two consecutive occasions), or 300 minutes after meal ingestion, when the measurements were abandoned. Breath samples were analysed immediately using a precalibrated, hydrogen sensitive electrochemical cell (Key Med), which measures hydrogen concentrations within 30 seconds, to an accuracy of 2 ppm.
Large bowel transit time was assessed by monitoring the progress of radio-opaque marker shapes through the intestine.23 On three successive mornings, the individuals ingested a single gelatine capsule containing 20 radio-opaque marker shapes, at 9.00 am. On day four, a plain abdominal radiograph was taken, again at approximately 9.00 am, and from this the mean total colonic transit time was calculated, as described by Metcalf et al.23
Serum bile acids
The bile acids were extracted from 1 ml of fasting serum using Isolute MF C18 cartridges.24 The conjugated and unconjugated fractions were then separated as described by Setchell and Matsui,25 using Lipidex-DEAP lipophilic anion exchange chromatography. The conjugated fraction was hydrolysed enzymatically using cholylglycine hydrolase26 and the unconjugated bile acids, thus formed, extracted using a Lipidex 1000 column.27 After the addition of 500 μl of 1 μM deuterated chenodeoxycholic acid (2H4-CDCA, the internal standard) to each fraction, the conjugated and unconjugated bile acids were derivatised to pentafluorobenzyl (PFB) ester, trimethylsilyl (TMS) ether derivatives, and analysed by gas chromatography-mass spectrometry (GC-MS).28 ,29 A 2 μl aliquot of the solution of the derivatives was chromatographed on a fused silica capillary GC column (BPX1, 25 m × 0.32 mm internal diameter, SGE Europe Ltd, Milton Keynes, UK) using helium as the carrier gas and a cold programmed temperature injector (Gerstel UK Ltd, Reading, UK). The HP 5890A gas chromatograph (Hewlett Packard Ltd, Manchester, UK) was directly coupled to the source of a VG 70SEQ tandem mass spectrometer (Micromass Ltd, Manchester, UK). Negative ion electron capture ionisation, with ammonia as the moderating gas, was performed. The individual bile acids were quantified using selected ion recording for the (M-PFB)− ions (m/z 447, 535, 539, and 623, monohydroxy, dihydroxy, deuterated dihydroxy, and trihydroxy bile acids, respectively), together with the2H4-CDCA.
To ensure a constant and precise recovery of the individual bile acids, a reference serum was analysed with each batch of eight serum samples. The coefficients of variation for measurement of the individual total, conjugated, and unconjugated bile acids ranged from 0.46% to 7.97%.
ETHICAL CONSIDERATIONS
The study was approved by the East London and The City Health Authority Research Ethics Committee (St Bartholomew’s Hospital) and by the Lewisham and North Southwark Committee on Ethical Practice (Guy’s Hospital). All 64 individuals gave their written informed consent before the study.
STATISTICAL ANALYSIS
The statistical significance of differences in results between the four study groups, and in the paired studies, was tested with the non-parametric heteroscedastic t test, and univariate regression analyses, as appropriate, using Excel software, version 5.0 (Microsoft Corporation, Redmond, Washington, USA). Values of p<0.05 were considered to be statistically significant. Unless otherwise stated, the results are given as mean (SEM), with range.
Results
MOUTH TO CAECUM TRANSIT TIME
Figure 1 shows the mouth to caecum transit time (MCTT) in the four groups of individuals studied. In the non-acromegalic control subjects, the mean MCTT of just under two hours (113 (8.3) minutes) was comparable to that in the patients with simple constipation (125 (6.7) minutes; NS). However, in the acromegalic patients untreated with octreotide, the mean value of 175 (8.3) minutes was 48% greater than that in the volunteer controls (p<0.001), while that in the acromegalics on long term octreotide was 116% greater (255 (7.8) minutes; p<0.001).

Group data for MCTT in non-acromegalic control subjects, acromegalic patients untreated with octreotide (OT), acromegalic patients on long term octreotide treatment (LTOT), and patients with simple constipation.
There was a similar pattern of results for the paired studies in the subgroup of nine acromegalic patients in whom the mean MCTT increased from 181 (9.5) minutes before, to 250 (10.0) minutes during octreotide treatment (p<0.001; fig 1).
LARGE BOWEL TRANSIT TIME
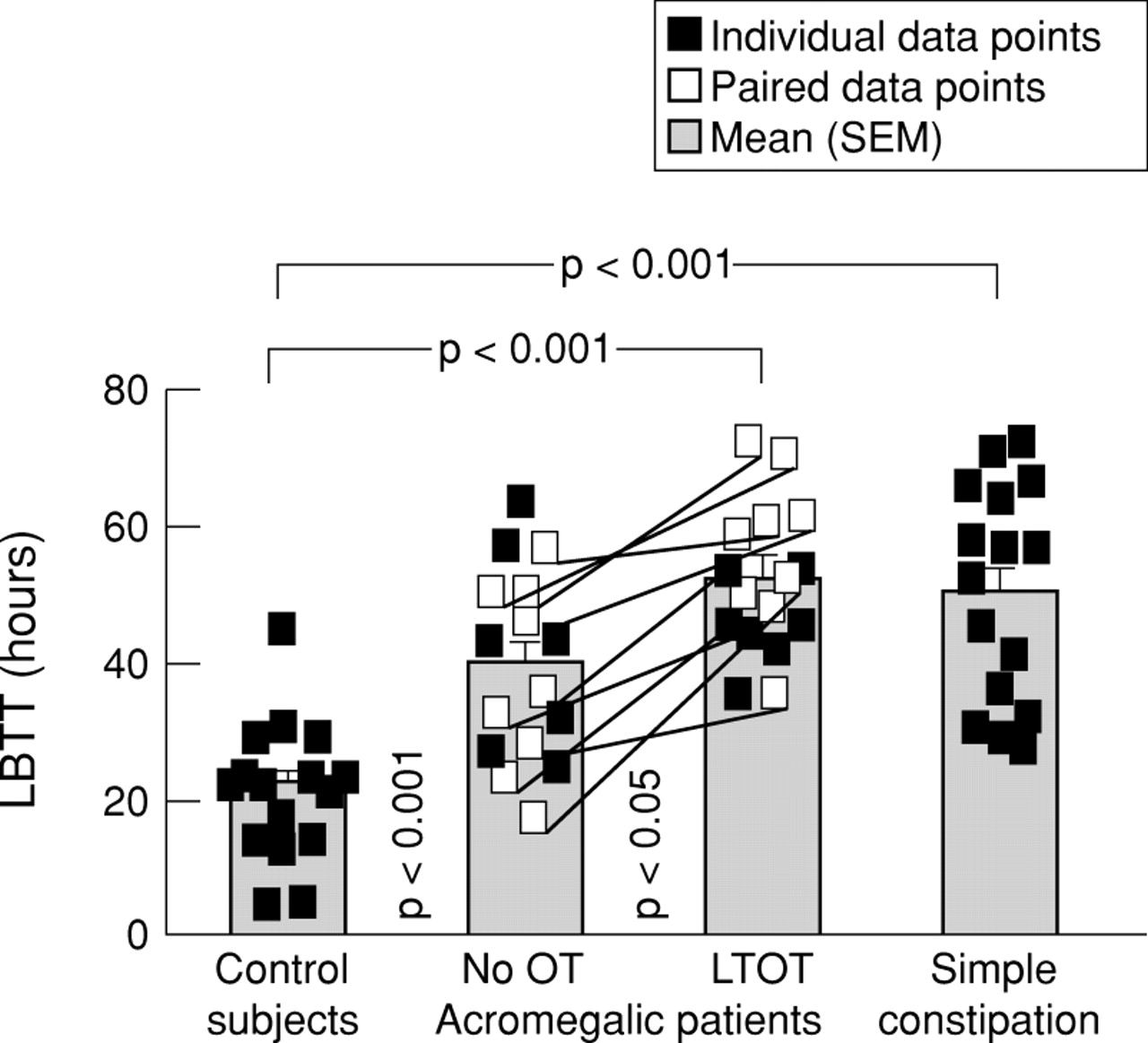
Figure 2 shows the results for large bowel transit time (LBTT). Despite a greater scatter of results than was found for the MCTT, the overall pattern was similar to that shown in fig 1, with the important exception of the results in the constipated disease controls. In these individuals, the mean LBTT (51 (4.0) hours) was significantly (p<0.001) longer than that in the non-acromegalic controls (21 (2.5) hours). However, as with small bowel transit, the LBTT was significantly greater in acromegalic patients untreated with octreotide (40 (3.5) hours; p<0.001), and was further prolonged in those treated long term with octreotide (52 (2.8) hours; p<0.05 versus the untreated acromegalics and p<0.001 versus the controls). Furthermore, in the nine paired (before and during octreotide treatment) studies, the 46% increase in mean LBTT (from 39 (4.6) to 57 (3.9) hours) was again statistically significant (p<0.001).

Group data for LBTT in non-acromegalic control subjects, acromegalic patients untreated with octreotide (OT), acromegalic patients on long term octreotide treatment (LTOT), and patients with simple constipation.
FASTING SERUM BILE ACID COMPOSITION
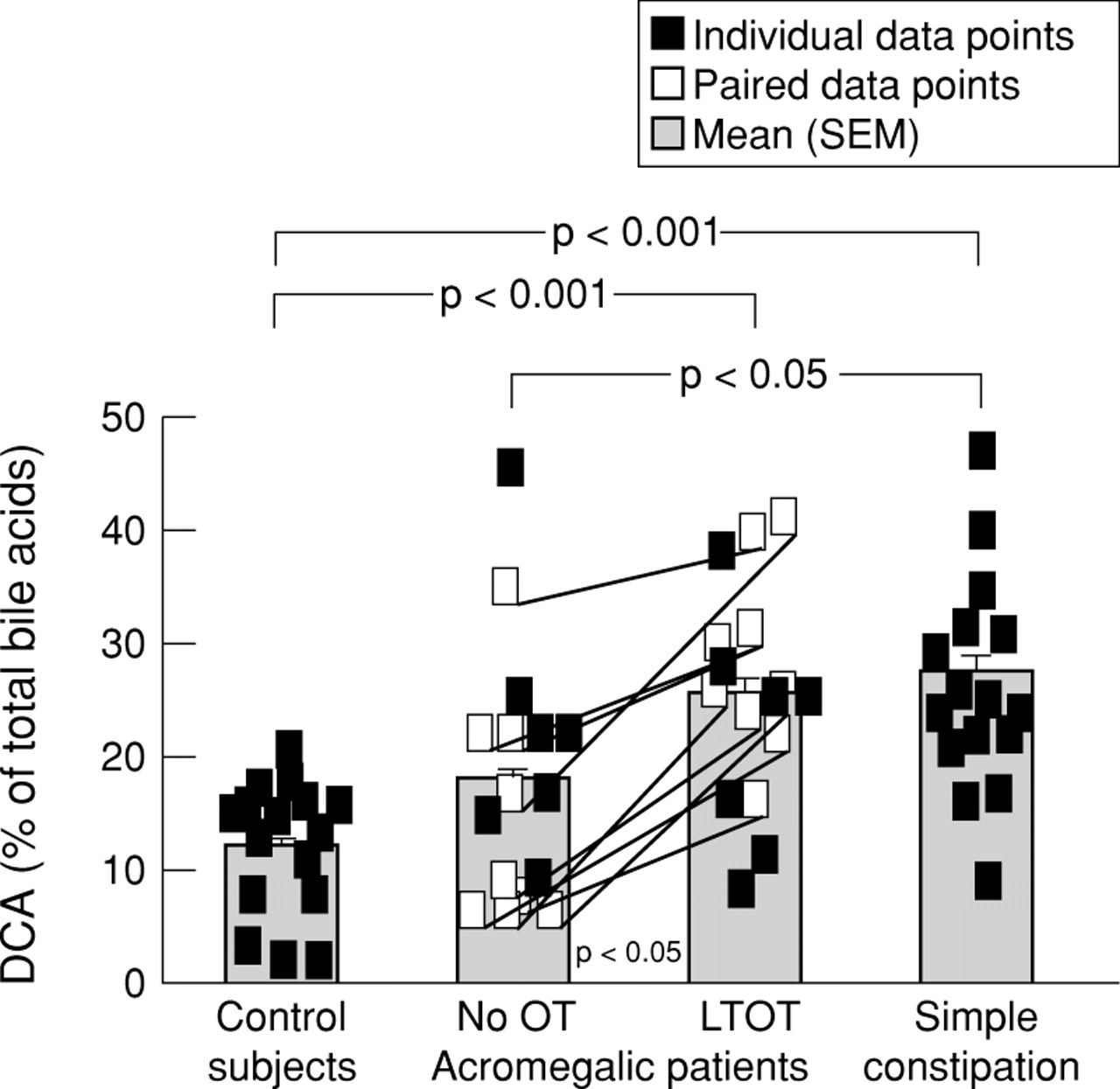
Figure 3 shows fasting total serum deoxycholic acid values, expressed as a percentage of total serum bile acids. Table 1 gives the corresponding data for the proportions of all the major bile acids (including deoxycholic acid). The pattern of results for fasting total serum deoxycholic acid was broadly similar to that described above for LBTT. In all four groups, there was again an appreciable scatter of results and there was no significant difference between the means in control subjects and in patients with acromegaly who had not been given octreotide. However, the means in the acromegalic patients on long term octreotide and in the patients with simple constipation were twice as great as that in the control group (p<0.001). Furthermore, for both the non-paired and paired comparisons in acromegalic patients untreated and treated with long term octreotide, there were 44% and 93% increases in the mean proportion of deoxycholic acid in patients given the somatostatin analogue (p<0.05 and 0.001, respectively).

Group data for the proportion of deoxycholic acid (DCA), expressed as a percentage of the total serum bile acids, in non-acromegalic control subjects, acromegalic patients untreated with octreotide (OT), acromegalic patients on long term octreotide treatment (LTOT), and patients with simple constipation.
Group and paired data for serum bile acid composition
In the paired, before and during treatment studies, the octreotide induced increase in the proportion of serum deoxycholic acid was accompanied by a reciprocal decrease in the proportion of the “parent” primary bile acid, cholic acid (p<0.05). However, there was no significant change in the percentages of the other serum bile acids, when the pretreatment and during treatment results were compared.
Despite the reciprocal fall in the proportion of cholic acid in the paired studies, there was no significant difference in the proportion of serum cholic acid between the four study groups. Indeed, as the results in table 1 show, apart from deoxycholic acid the only significant difference in serum bile acid composition was in the proportion of chenodeoxycholic acid which was significantly higher in the control subjects than in the other three groups (p<0.05).
RELATION BETWEEN INTESTINAL TRANSIT TIMES AND SERUM BILE ACID COMPOSITION
Figure 4 shows the relation between the proportion of total serum deoxycholic acid and large bowel transit time in all 64 individuals studied. Table 2 presents the results for the univariate analyses relating MCTT and LBTT to the proportions of the unconjugated, conjugated, and total serum bile acids. There was a significant (p<0.001) linear relation between LBTT and the total serum deoxycholic acid, expressed as a percentage of the total serum bile acids, with a correlation coefficient of 0.70 (fig 4). Furthermore, as the data in table 2 show, there were also significant (p<0.001) linear relations between LBTT and the unconjugated (r=0.55) and the conjugated (r=0.64) deoxycholic acid proportions in fasting serum. However, the correlation coefficients between LBTT and the percentages of the other serum bile acids were all low and insignificant, as were the correlation coefficients for the plots relating MCTT to all 15 serum bile acid percentages measured.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relation between LBTT and the proportion of deoxycholic acid (DCA), expressed as a percentage of the total serum bile acids.
Univariate analyses for the pooled data (n=64) from the four groups
Discussion
For studies of large bowel transit, we used the simple, but relatively crude technique of documenting the progress of radio-opaque marker shapes through the intestine.23 This may explain why we observed a greater scatter of data for colonic transit than was found for the mouth to caecum transit. It is equally possible, however, that the scatter of results for colonic transit is due to the inherent variability of colonic function. Whatever the explanation, the spectrum of results for colonic transit may explain why, in the past,5 we did not find a statistically significant difference for colonic transit between acromegalic patients treated, and those untreated, with octreotide. The clear cut and significant results of the present study emphasise the importance of carrying out paired studies in an adequate number of patients. Nonetheless, the magnitude of the prolongation of large bowel transit with octreotide was modest.
Most previous studies of bile acid composition have been based on either gall bladder bile (obtained at laparotomy,30 by percutaneous gall bladder puncture31 ,32) or on bile rich duodenal fluid.30 In the present study we used the minimally invasive method of measuring bile acids in fasting serum. However, one cannot assume that the proportions of the bile acids in fasting serum are necessarily comparable to those in bile. Indeed, in the short term (1–3 hours after meals), the proportions of bile acids are not comparable at these two sites but ultimately (over 24 hours), the bile acid pools in serum and bile must equilibrate. This is the justification for using serum sampling to measure bile acid pool sizes and synthesis rates with stable isotope dilution.33Furthermore, when Nagengast et al compared bile acid composition in serum and bile from 74 individuals, they found that within an 8% variation, the molar percentage of deoxycholic acid in bile could be predicted from the percentage of deoxycholic acid in serum, using a simple equation.34 Using this approach, we showed that there is a linear relation not only between large bowel transit time and serum deoxycholic acid, but also between colonic transit and both deoxycholic acid formation rate (input rate into the enterohepatic circulation) and pool size.35
There are few previous studies of the effects of octreotide on colonic motility. Thus, van der Ohe and colleagues36 used manometric techniques to study the cleansed colon of control subjects given a single 50 μg subcutaneous injection of octreotide. They found that octreotide had no effect on colonic motility. However, measurements of intracolonic pressure in cleansed colons are obviously very different from recording the transit of radio-opaque marker shapes through the colon of non-fasted subjects. The results of the present study clearly show that chronic octreotide treatment (300–600 μg/day) prolongs transit through the large bowel.
As the results in table 2 show, there was no correlation between mouth to caecum transit time and the proportions of any of the five major bile acids studied in serum. These findings contrast with reports by Shoda and colleagues37 and Azzaroli et al,38 who found linear relations between small bowel transit time, and the proportion of deoxycholic acid in bile. The reason for these contrasting findings is unclear, but may relate to the type of patients studied. Thus, in the Japanese and Italian studies, the authors examined only control subjects and gallstone carriers. In the present study, the inclusion of individuals with simple constipation may have affected the results.
As figs 1, 2, and 3 show, the pattern of results for mouth to caecum and large bowel transit times, and the proportion of deoxycholic acid in serum, was similar in the healthy controls and in the two groups of acromegalic patients. However, in the patients with simple constipation, although the mouth to caecum transit time was comparable to that seen in the controls, the large bowel transit time and the proportion of deoxycholic acid in serum were significantly greater than those in the other groups. Indeed, when the results for the constipated patients were excluded from the analyses, there was a significant linear relation between mouth to caecum and large bowel transit times (r=0.68, p<0.001). This may explain the weak, but significant (r=0.42, p<0.005), relation between the mouth to caecum transit time and the proportion of deoxycholic acid in serum, but again only when the results in the constipated group were excluded. As always however, significant linear relations between two variables can never prove causality.
In the paired study (fig 3), the twofold increase in the proportion of deoxycholic acid was accompanied by a reciprocal change in the proportion of the parent bile acid, cholic acid, in the serum (table1). Therefore, one might have expected a reciprocal linear relation between large bowel transit time and the proportion of cholic acid in serum. However, as the results in table 2 show, when the data for all 64 individuals were pooled, there was no such relation. The reasons for this are unclear, and equally there is no obvious explanation for the high proportion of chenodeoxycholic in the serum from the 16 control subjects.
Although studies of intestinal transit and deoxycholic acid metabolism in acromegalic patients before and during octreotide treatment are of interest, if the lessons learned were confined to octreotide induced stones, their value would be limited. There is increasing evidence that changes in intestinal transit also play a role in the pathogenesis of “conventional” gallstone disease.39 Thus, when Heaton and colleagues40 studied normal weight women with no other risk factors for gallstones, they found that whole gut transit time was greater, and faecal wet weight less, in gallstone carriers than in matched controls. In other words, the women with gallstones seemed to suffer from slow transit constipation.
The Bristol group modified intestinal transit pharmacologically and showed that this led to changes in the proportion of deoxycholic acid in bile. Thus, when they slowed intestinal transit with loperamide, the proportion of deoxycholic acid in bile increased, with an associated increase in biliary cholesterol saturation. Conversely, when transit through the intestine was accelerated with senna or bran, the proportion of deoxycholic acid in bile fell, as did the biliary cholesterol saturation indices.16 They also went on to show that there was a linear relation between thechange in whole gut transit and thechange in the proportion of deoxycholic acid in bile.16
The mechanisms whereby prolongation of intestinal transit increases the proportion of deoxycholic acid in serum and bile are complex and multifactorial. Thus, Berr and colleagues41 have shown that there is a relation between the input rate into the enterohepatic circulation and the pool size of deoxycholic acid, and not only the quantity of faecal 7α-dehydroxylating bacteria, but also the activity of the 7α-dehydroxylase enzyme. Furthermore in preliminary publications, we have shown that not only were large bowel transit time and the proportion of deoxycholic acid greater in patients with cholesterol gallstones than controls, but also that the gallstone carriers had more Gram positive anaerobes and increased activities of the bile acid metabolising enzymes cholylglycine hydrolase and 7α-dehydroxylase, than normal.42 Perturbation of intestinal transit may also induce changes in colonic luminal and/or faecal pH.42-44 Thus, acceleration of colonic transit is associated with a reduction in faecal pH. In turn, this may influence not only the activities of the bile acid metabolising enzymes, but also the solubilisation (and therefore the bioavailability) of the newly formed bile acids.
Acknowledgments
This work was supported, in part, by grants from the Special Trustees of Guy’s Hospital and Sandoz (UK) Ltd. These data were presented, in part, at the Meetings of the British Society of Gastroenterology (Gut1996;38(suppl 1):A53, andGut 1996;39(suppl 1):A9 and the 5th United European Gastroenterology Week (Gut 1996;39(suppl 3):A134.
Abbreviations
- CA
- cholic acid
- CDCA
- chenodeoxycholic acid
- DCA
- deoxycholic acid
- IGF-1
- insulin-like growth factor 1
- LBTT
- large bowel transit time
- LCA
- lithocholic acid
- MCTT
- mouth to caecum transit time
- UDCA
- ursodeoxycholic acid