Article Text

Abstract
BACKGROUND Lymphocytic gastritis is characterised by an accumulation of lymphocytes in the surface epithelium of the stomach. Lymphocytic gastritis has been linked to coeliac disease and Helicobacter pyloriinfection.
AIMS To determine whetherH pylori eradication leads to resolution of the lymphocytic infiltrate and clinical improvement in patients with lymphocytic gastritis, and to determine their HLA status.
METHODS The Leeds Dyspepsia Questionnaire (LDQ) was administered to 13 patients with lymphocytic gastritis. H pylori serology,13C urea breath test (UBT), and upper gastrointestinal endoscopy with sampling of the duodenum, antrum, and corpus were done in all cases and the HLA status was determined. Eleven patients had at least one positive test for H pylori. Patients with lymphocytic gastritis and H pylori infection were treated with a one week course of omeprazole, clarithromycin, and metronidazole. Gastric and duodenal intraepithelial lymphocyte (IEL) counts were performed, along with histological assessment of gastric and duodenal biopsies before and after H pylori eradication.
RESULTS Two months after treatment there was a significant reduction in gastric IEL counts in both antrum and corpus. There was no significant change in duodenal IEL counts before and after eradication. According to the Sydney grading there was significant improvement in corpus inflammation after eradication. The patients histologically H pylori positive before treatment became H pylori negative. Dyspepsia scores also improved significantly after treatment.
CONCLUSIONS H pylori eradication treatment in patients with lymphocytic gastritis causes significant improvement in the gastric IEL infiltrate, corpus inflammation, and dyspeptic symptoms. H pylori serology is frequently positive when histology and UBT are negative. Lymphocytic gastritis may represent a specific immune response to H pylori infection.
- lymphocytic gastritis
- intraepithelial lymphocytes
- Helicobacter pylori
- HLA status
- coeliac disease
Abbreviations used in this paper
- IEL
- intraepithelial lymphocyte
- PBMC
- peripheral blood mononuclear cell
- UBT
- urea breath test
Statistics from Altmetric.com
Lymphocytic gastritis is characterised by an accumulation of lymphocytes in the surface and foveolar epithelium of the stomach. It is found in approximately 1% of gastric biopsy specimens from dyspeptic patients.1 ,2 The diagnostic threshold for lymphocytic gastritis is usually taken as greater than 25 intraepithelial lymphocytes (IELs) per 100 epithelial cells.1 ,3 This special type of gastritis may be associated with a normal appearing gastric mucosa. However, the classical endoscopic appearance comprises prominent rugal folds bearing small nodular elevations surmounted by small grey-white erosions with hyperaemic margins, maximal in the body and fundus.1 ,3This endoscopic picture is generally termed “varioliform” gastritis.
The aetiology of lymphocytic gastritis is unknown. It has been attributed to an atypical response to Helicobacter pylori infection.1 Although many patients with lymphocytic gastritis are seropositive for H pylori, its presence is not usually confirmed histologically. Lymphocytic gastritis is frequently found in patients with coeliac disease. In one study of 22 patients with coeliac disease, 50% had lymphocytic gastritis.4 The IELs in the stomach and small bowel were positive for MT-1, indicative of T cell infiltration. It has also been suggested that lymphocytic gastritis may represent part of a diffuse lymphocytic gastroenteropathy which varies in its expression from site to site.5
Gut intraepithelial lymphocytes are almost entirely CD3+ T cells, and approximately 80% of them are CD8+.6 ,7 In humans up to 15% of IELs carry the T cell receptor, which is found on less than 3% of peripheral blood lymphocytes.6 ,7
We investigated the effects of H pylorieradication on the natural history of lymphocytic gastritis and also determined the HLA status of our patients with lymphocytic gastritis in an attempt to explore further the relation of lymphocytic gastritis with coeliac disease.
Methods
Thirteen newly diagnosed patients with a histological diagnosis of lymphocytic gastritis were identified and were invited to take part in the study. Table 1 presents their clinical details. Informed consent was obtained from all patients. Prior to endoscopy the Leeds Dyspepsia Questionnaire, a validated symptom questionnaire,8 was performed. Venous blood was taken for H pylori serology and HLA status. A carbon-13 urea breath test was performed. At endoscopy, two biopsy specimens were taken from the second part of the duodenum, gastric antrum, and body using standard biopsy forceps.
Clinical details of patients with lymphocytic gastritis
HISTOLOGY
Specimens were fixed in 10% buffered formalin, embedded in paraffin wax, and sections stained with haematoxylin and eosin (H&E). A modified Giemsa stain was used to detect H pylori. The H&E stained sections were examined at ×400 magnification and the number of IELs and epithelial cell nuclei in an uninterrupted length of surface and foveolar epithelium were counted. Based on previous studies,3 ,5 the ratio of 25 IELs:100 epithelial cells was used as a limit for inclusion into this study. Gastritis was classified according to the updated Sydney System.9
IMMUNOHISTOLOGY
Duodenal and gastric biopsy specimens were also immunostained using a three step immunoperoxidase technique with anti-CD3 (pan T cell) monoclonal antibodies (from Dako, High Wycombe, UK) and IEL counts were performed.
IMMUNOSTAINING
The ABC technique was employed for immunostaining using the Duet kit (Dako Ltd, Denmark). The paraffin wax sections were pretreated by pressure cooking in citrate buffer at pH 6 for 90 seconds at full pressure. The polyclonal H pylori antibody was used at a dilution of 1/100.
HLA STATUS
DNA isolation
Genomic DNA was obtained from peripheral blood mononuclear cells (PBMC) according to the method of Miller et al.10 Extracted DNA was redissolved in TE buffer, adjusted to 1 μg/μl by ultraviolet spectrophotometry and stored at 4°C until use.
HLA genotyping
PBMC DNA samples were typed for HLA-DRB and DQB antigens using a 40 reaction PCR-SSP system with amplification primers as described by Bunce et al.11 PCR product was electrophoresed in a 1.5% agarose gel containing 0.5 μg/ml ethidium bromide and visualised using ultraviolet illumination.
H PYLORI SEROLOGY
Serum samples from all 13 subjects were assayed forH pylori IgG antibodies (Sigma Diagnostics).H pylori IgG antibody titres were also assayed by Premier H pylori kit (supplied by Launch Diagnostics, UK), before and after H pylori eradication in seven patients (patients 2, 4–9; table2).
Laboratory findings in patients with lymphocytic gastritis
Patients were classed as H pylori positive on the basis of at least one positive test. Previous study from our unit5 has shown that in patients with lymphocytic gastritis H pylori serology is frequently positive when the histology is negative. Past studies have also suggested that lymphocytic gastritis could be a manifestation of an atypical host immune response to H pylori.1 We therefore classed our patients asH pylori positive on the basis of positive serology even when the histology and/or the 13C urea breath test was negative. On this basis patients with lymphocytic gastritis and H pylori infection were treated with a standard one week triple therapy course of omeprazole 20 mg once daily, clarithromycin 250 mg twice daily, and metronidazole 400 mg twice daily. After an interval of two months, the Dyspepsia Questionnaire, endoscopy with duodenal and gastric biopsies, and 13C urea breath test were repeated. In seven patients (patients 2, 4–9) who received H pylorieradication, H pylori serology was repeated after an interval of one year to document a fall in antibody titre to H pylori. Gastric and duodenal IEL counts were performed along with Sydney grading9 of gastric biopsy specimens and histological assessment for chronic inflammation and degree of villous atrophy of duodenal biopsy specimens, before and after H pylorieradication by an experienced pathologist (MFD) who was blinded to any clinical data. CD3 counts on gastric and duodenal biopsy specimens were performed by a second pathologist (DSA). The study was approved by the local research ethics committee.
STATISTICAL ANALYSIS
For comparison of paired non-parametric data the Wilcoxon sign rank test was used. To assess the correlation of CD3 and H&E lymphocyte counts, Pearson’s test was used. A p value less than 0.05 was regarded as significant.
Results
ENDOSCOPY
Of 13 patients, endoscopy was normal in five. In two patients endoscopic appearance was that of varioliform gastritis. One endoscopy showed erythema of the antrum. Two patients had erythematous gastritis, one had gastric erosions, one had duodenitis, and one had a small gastric ulcer (table 1).
One patient (no 5) also had portal hypertensive gastropathy and early oesophageal varices secondary to chronic ethanolic liver disease.
H PYLORI HISTOLOGY AND SEROLOGY
Of 13 patients with lymphocytic gastritis, 11 had at least one positive test for H pylori (table 2). All 11 were seropositive for H pylori. In three of 11, H pylori was found on histology; one of these also had a positive 13C urea breath test and one other had a positive 13C urea breath test. Two patients (nos 10, 11) with lymphocytic gastritis who were H pylori positive were lost to follow up and were excluded from the analysis. We measured paired pre- and posteradication IgG antibody titres in seven patients. Titres fell in five and rose in two (table3). Intraepithelial lymphocyte counts were performed in nine patients (nos 1–9) before and after H pylorieradication. In seven of these, lymphocytic gastritis was corpus predominant.
Helicobacter pylori titres pre- and post-H pylori eradication in seven patients
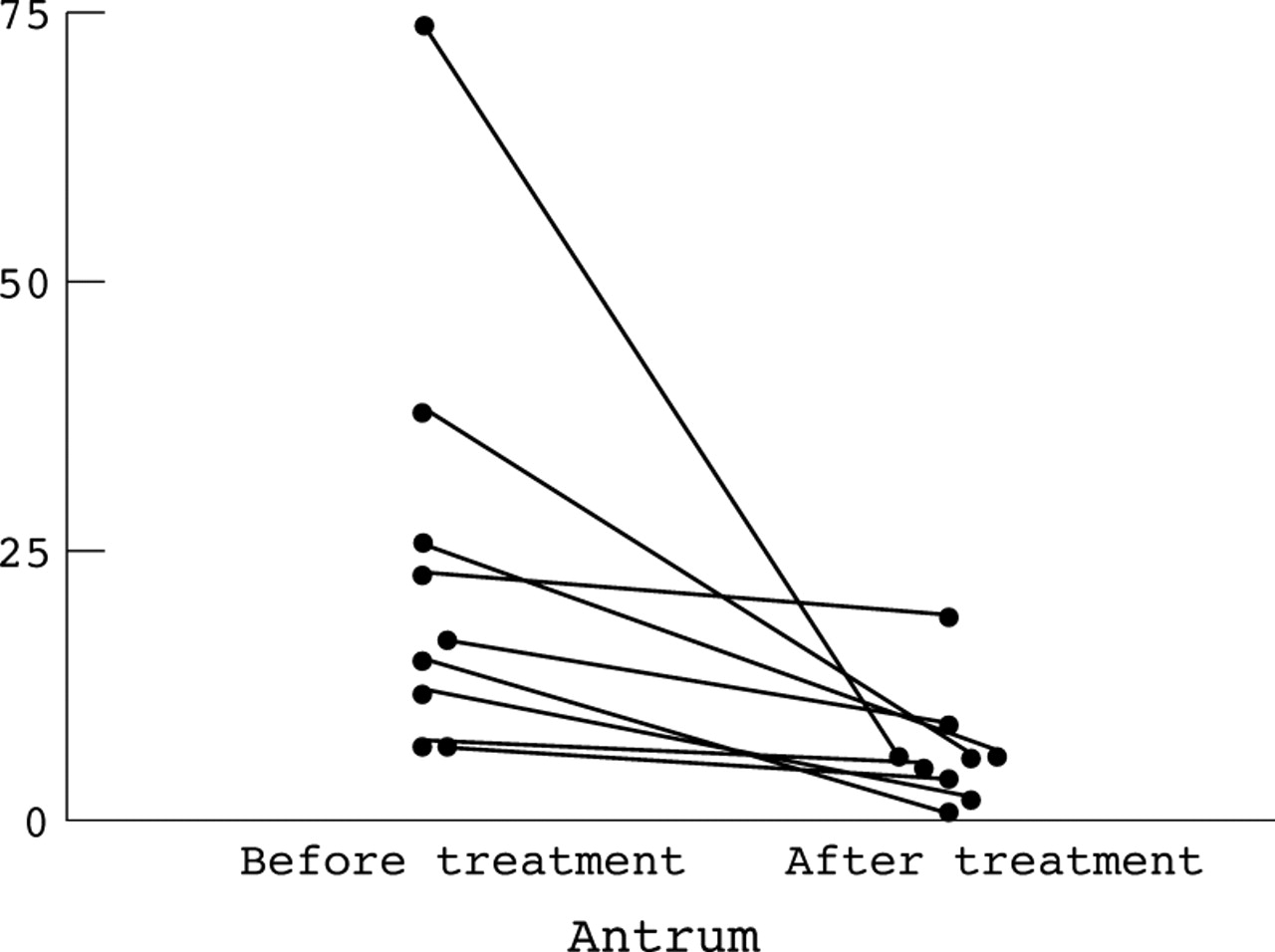
On H&E stained sections the median IEL count in the antrum was 17.0 per 100 epithelial cells (range 7.0–74.0) and 6.0 (range 1.0–19.0) before and after H pylori eradication respectively. Gastric body IEL counts were performed on seven patients as in two patients (nos 2, 3) the pre-eradication biopsies were all of antral type mucosa. The median IEL count in the corpus pre-H pylori eradication was 44.0 (range 28.0–81.0) and posteradication was 10.0 (range 3.0–30.0). There was a significant reduction in the IEL count in both antrum (p=0.003; fig 1) and corpus (p=0.015; fig 2) after H pylorieradication treatment.

Effect of H pylori eradication on antral intraepithelial lymphocytes.

{kind=link}
{kind=link}
Effect of H pylori eradiation on corpus intraepithelial lymphocytes.
The median IEL count in the duodenum was 16.0 (range 7.0–71.0) and 10.0 (range 6.0–67.0) pre- and post-H pylori eradication respectively, and although there was a trend towards a fall in the duodenal IEL count after H pylori eradication, it was not statistically significant. On sections stained with anti-CD3 monoclonal antibodies the median IEL count in the antrum was 11.6 (range 3.6–34.4) and 2.7 (range 0.19–9.2) before and after H pylorieradication respectively, and median corpus counts were 30.35 (range 19.1–72.7) pre-H pylori eradication and 5.3 (range 1.14–25.7) post-H pylorieradication.
There was a significant reduction in the CD3 and IEL counts in both antrum (p=0.046) and corpus (p=0.007) post-H pylori eradication. There was also a significant correlation (p<0.0001, coefficient = 0.852 (two tailed)) between the H&E and CD3 IEL counts. However H&E counts were almost invariably higher than CD3 counts, the mean difference being 7.48. Duodenal (second part) histology was normal in 7/13 patients. Two patients had mild villous atrophy, while four had increased IELs with a normal villous architecture. The two patients with mild villous atrophy were not commenced on a gluten free diet, as the degree of villous atrophy was thought to be insufficient to diagnose coeliac disease. Sydney grading of the gastric biopsy specimens before and after H pylori eradication revealed a significant improvement in the corpus inflammation (p<0.03) after H pylorieradication. Patients H pylori positive on histology and 13C UBT, turned negative posteradication.
IMMUNOSTAINING
Eighteen pre- and post-treatment biopsy specimens (patient nos 1–9) were immunostained by the technique as described above. The slides were examined “blind” to previous histological results. Two cases (nos 3, 7) were designated positive; both were pretreatment biopsies.
DYSPEPSIA SCORES
Dyspepsia scores in the patients receiving H pylori eradication therapy, as assessed by the Leeds Dyspepsia Questionnaire were also significantly improved posteradication (p<0.03). The median dyspepsia scores were 4.0 (range 0–6.0) and 0, pre- and posteradication respectively.
HLA STATUS
HLA status was available on 10/13 patients; seven of the 10 (70%; nos 1,3,4,5,7,8,11) possessed the DQ2 molecule encoded by the allele DQB1*0201 as compared with 24% of the controls, a relative risk of 3%. DQB1*0201 is possessed by 95% of coeliac patients compared with 20–30% of controls.12 ,13 The control population comprised 100 “normal” individuals (volunteer donors), randomly selected from the local population, and were tissue typed by the same methods as the study group.
Discussion
Previous studies have suggested that lymphocytic gastritis could be a manifestation of an atypical host immune response toH pylori.1 ,14 In our study 11/13 patients with lymphocytic gastritis wereH pyloripositive; we have shown histological and symptomatic improvement in 9/11 of these patients following H pylorieradication, which lends some support to this hypothesis. The relatively low prevalence of the organism on histology,1 ,15 and the discrepancy between the histological and serological H pylori status in patients with lymphocytic gastritis is in keeping with previous studies.1 ,5 Thus despite positive serology in all these patients, even the “gold standard” histological test has failed to reveal Helicobacter organisms, either bacterial or coccoid. Given the beneficial effect of eradication treatment we assume that bacteria are present in very low numbers and are not represented in the histological sections.
We have also found that the histological expression of lymphocytic gastritis is variable throughout the stomach and duodenum, as shown in previous studies,1 ,3 and confirm that the endoscopic appearances in lymphocytic gastritis can vary from normal to the characteristic varioliform gastritis picture. In this study six patients with lymphocytic gastritis had variable degrees of histological abnormality in the duodenum, consistent with a previous study.5 Two patients had mild patchy villous atrophy, while the other four patients had increased IEL but with normal villous architecture. Increased small intestinal IEL counts are present in patients with treated coeliac disease following gluten challenge,16 dermatitis herpetiformis,17first degree relatives of patients with coeliac disease,18and those with low grade small intestinal enteropathy.19The finding of these histological abnormalities in the duodenal mucosa gives strength to the hypothesis that at least some patients with lymphocytic gastritis have a more generalised disturbance of mucosal immunity, predisposing them to gluten related enteropathy.
We have also shown that the majority of patients with lymphocytic gastritis possess the DQ2 molecule encoded by the allele DQB1*0201 which is also possessed by 95% of the patients with coeliac disease. These findings tentatively suggest a strong association of lymphocytic gastritis with coeliac disease, and lymphocytic gastritis may be a genetically restricted, specific immune response toH pylori infection.
In summary, we have shown that in non-coeliac patients with lymphocytic gastritis who have at least one positive test for H pylori, eradication treatment results in both histological and clinical improvement.
Acknowledgments
We wish to thank Dr Mark Wilcox, Consultant Microbiologist, for providing the H pylori serology data, and Miss Julie Mackintosh for preparing the manuscript.
Abbreviations used in this paper
- IEL
- intraepithelial lymphocyte
- PBMC
- peripheral blood mononuclear cell
- UBT
- urea breath test