Article Text

Abstract
METHODS Four patients with clinicopathological features suggesting a new distinct entity defining extensive small intestinal CD4 T cell infiltration were observed.
RESULTS All four patients presented with chronic diarrhoea, malabsorption, and weight loss. Biopsy specimens of the small intestine disclosed extensive and diffuse infiltration of the lamina propria by pleomorphic small T lymphocytes, which were positive for CD3, CD4, CD5, and the β chain of T cell receptor in all three cases studied and negative for CD103 in all three cases studied. It is notable that, in all invaded areas, the infiltrating cells showed no histological change throughout the whole evolution. In three patients, lymphocyte proliferation was monoclonal and there was extraintestinal involvement. In one patient, lymphoproliferation was oligoclonal and confined to the small intestine. In all four patients, there was no evidence of coeliac disease. Although none of the four patients responded to single or multiple drug chemotherapy, median survival was five years.
CONCLUSION Extensive small intestinal CD4 T cell infiltration is a rare entity, distinct from coeliac disease and associated with prolonged survival.
- CD4
- T cells
- lymphocytes
- small intestine
Abbreviations used in this paper
- TCL
- T cell lymphoma
- IEL
- intraepithelial lymphocyte
- TCR
- T cell receptor
- PCR
- polymerase chain reaction
- EBER
- Epstein Barr encoded RNA
Statistics from Altmetric.com
The gastrointestinal tract is the most common site of primary extranodal lymphoma.1 Most gastrointestinal lymphomas are of B cell lineage.2 ,3 Complete remission can be obtained in a substantial proportion of patients by eradication ofHelicobacter pylori, combined radical surgery, and chemotherapy4 or chemotherapy alone.5 Five year survival rates vary between 55 and 100% and depend on the patient’s age, the site and stage of the disease, and whether surgical removal is radical or incomplete.4Gastrointestinal T cell lymphomas (TCLs) are heterogeneous6-26; the best characterised forms are associated with coeliac disease.6-12 Most of these forms are localised high grade large cell lymphomas, and carry a poor prognosis.6-12
Over the past few years, we have observed four patients with extensive small bowel infiltration by pleomorphic small T lymphocytes. These patients had distinct clinical features and outcomes and had no evidence of coeliac disease. Clinical and pathological descriptions from the literature are few and are mainly limited to isolated case reports.22 ,23 This study describes the clinical, pathological, and prognostic features of a retrospective series of four patients who had extensive small intestinal CD4 T cell infiltration without evidence of coeliac disease.
Patients and methods
PATIENTS
Eighteen patients with intestinal lymphoma, negative for B cell markers and positive for pan T cell markers such as CD3 and/or CD45RO, were studied retrospectively. Eleven had large cell high grade TCL, with coeliac disease in seven cases and without it in four. Three patients had coeliac disease and extensive small intestinal lymphoproliferation of heterogeneous immunophenotype and poor prognosis. This study focuses on the remaining four patients, who had extensive small intestinal infiltration with pleomorphic small T lymphocytes without evidence of coeliac disease. The patients were followed in two institutions; diagnosis was made in 1975 for one patient and between 1989 and 1995 for three.
PATHOLOGY
All specimens were re-evaluated by the same pathologist (AL), according to the updated Kiel classification.27Perendoscopic gastrointestinal biopsy specimens, bone marrow and liver biopsy specimens, as well as surgical specimens, were fixed in Bouin’s fluid or in 10% neutral buffered formalin, embedded in paraffin, and routinely processed. The number of intraepithelial lymphocytes (IELs) was measured by counting 200 epithelial cell nuclei with a 25 objective lens and noting the number of IELs. The mean number of IELs was expressed per 100 epithelial cell nuclei.
Immunohistochemical studies were performed on the paraffin embedded and frozen gastrointestinal sections using the avidin-biotin-peroxidase complex (ABC method; Vectastain ABC kit; Vector Laboratories, Burlingame California, USA) with the following polyclonal CD3 or monoclonal antibodies: CD19, CD20 (L26) (Dako SA, Glostrup, Denmark), CD1, CD2, CD3, CD4, CD5, CD7, CD8, CD57 (Leu 7) (Becton Dickinson Immunobiologicals, Illinois, USA), βF1 (T cell Sciences Inc, Cambridge, Massachusetts, USA), T cell receptor (TCR)-δ1, (T cell Diagnostics Inc, Woburn, Massachusetts, USA) and CD103 (HML1; Immunotech, Marseille, France). Staining was visualised with diaminobenzidine. In negative controls the primary antibody was omitted; labelling was never observed.
In situ hybridisation with Epstein Barr encoded RNA (EBER) oligonucleotides was performed with the Dako hybridisation kit (reference no Y017) which contains a mixture of fluorescein isothiocyanate conjugated Epstein-Barr virus oligonucleotides (EBER-1 and -2, both 30 bp long). Slides were deparaffined in xylene, treated with proteinase K (3 μg/ml) and dehydrated in 95% alcohol. Sections were incubated for 12 hours at 37°C with the probes. The hybridisation product was detected using three immunoglobulins: mouse monoclonal anti-fluorescein isothiocyanate (Dako M878), rabbit anti-mouse (Dako Z259), and alkaline phosphatase conjugated monoclonal anti-mouse (Dako D651). The chromogen was nitroblue tetrazolium-5-bromo-4-chloro-3-indolyl phosphate, and the slides were counterstained with light green. Appropriate positive and negative controls were run.
NUCLEIC ACID STUDIES
Clonality was studied using Southern blotting or polymerase chain reaction (PCR).
Southern blotting was performed in patient 2. DNA from mesenteric lymph nodes, jejunal tissue, and/or peripheral blood lymphocytes was isolated, digested with BamHI,EcoRI, andHindIII restriction enzymes, submitted to electrophoresis in agarose gel, and transferred to nylon membranes as described previously.28 Filters were hybridised with 0.4 kb BglII TCRβ cDNA and 2.6 kbSau3A JH probes, and washed under stringent conditions.
PCR was performed on duodenojejunal biopsy specimens from patients 3 and 4. DNA was extracted by standard procedures, and PCR Vγ-Jγ analysis was performed as described previously.29 ,30Multiplex PCR was performed using oligonucleotides specific for VgI (primer VgI cons), II (Vγ9), III (Vγ10), and IV (Vγ11), and Jγ1, Jγ2 (Jγ2S2), JγP, JγP1, and JγP2 (JγP1/2).
The size of the Vγ-Jγ junctional regions was assessed by electrophoresis on 6% polyacrylamide gels after ethidium bromide staining, thus allowing discrimination between oligoclonal and monoclonal patterns.
Results
CASE HISTORIES (TABLES 1 AND 2)
The patients comprised three men and one woman, aged 43–58 years. The case of patient 2 has already been reported.22 Median survival was five years.Two patients died, after a slow but relentless course. The remaining two are still alive.
Clinical characteristics at presentation
Outcome in extensive small intestinal T cell lymphoproliferation
Patient 1
In January 1975, this 43 year old man presented with a two year history of diarrhoea and weight loss and recent abdominal pain. Diffuse small intestinal T lymphocyte infiltration was diagnosed on the basis of duodenojejunal biopsy results. Oral tetracycline was started in April 1975 and maintained for three years. The diarrhoea improved but the duodenal T lymphocyte infiltration was unchanged. Oral chlorambucil was started in January 1978 and maintained for six years; clinical remission was obtained and the density of the infiltration decreased. During the first six months of 1983, diarrhoea and weight loss recurred, and hypophosphataemia, hypomagnesaemia, and hypocalcaemia appeared. Meanwhile, the mesenteric and retroperitoneal lymph nodes had become enlarged. In June 1983, cyclophosphamide, teniposide, and prednisone was started, but after 10 cycles, the patient failed to achieve complete remission. Between July 1985 and April 1987, his clinical status remained stable without treatment. In April 1987, the diarrhoea worsened, the mesenteric and retroperitoneal lymph nodes increased, and a combination of holoxan, doxorubicin, and etoposide was started. After six cycles there was a marked decrease in mesenteric lymph nodes, but they reappeared in January 1988. Chloraminophene was prescribed but compliance was poor. The patient’s clinical condition remained stable until November 1988. Duodenal biopsy specimens showed that diffuse small intestinal T lymphocyte infiltration was still present. Total parenteral nutrition was started in February 1989. The patient’s condition progressively deteriorated; the T lymphocytes invaded the colon and liver, and ascites and intestinal obstruction appeared. The patient ultimately died in Septeber 1989.
Patient 2
In August 1989, a 28 year old man, who was born and living in Algeria, presented with a seven year history of diarrhoea and weight loss. He had been on a gluten-free diet for six months but no improvement had resulted. In September 1989, extensive small intestinal T cell infiltration was diagnosed on the basis of duodenojejunal biopsy results. A few days later, he developed an acute small bowel obstruction and underwent emergency laparotomy. Total parenteral nutrition was started after the operation. Four cycles of chemotherapy comprising cyclophosphamide, doxorubicin, and prednisone produced no response. In January 1990, 2-deoxycoformycin was started and maintained for 31 months. Diarrhoea decreased, weight increased, and the patient’s general condition improved, but the diffuse small intestinal T infiltration did not change. In September 1992, mediastinal lymphadenopathy, interstitial lung opacities, and skin lesions appeared. Skin and bronchial biopsy specimens disclosed invasion by tumorous T cells. 2-Deoxycoformycin was stopped and replaced by chlorambucil. Mediastinal lymph nodes and skin lesions improved and a good clinical condition was maintained for 21 months. However, the patient died in June 1994 from progressive multifocal leukoencephalopathy.
Patient 3
In June 1991, this 59 year old woman presented with a six month history of diarrhoea, weight loss, and night sweating. In July 1991, extensive small intestinal T cell infiltration was diagnosed on the basis of duodenojejunal and ileal biopsy results. The patient was initially treated with three cycles of MACOP-B and six cycles of cyclophosphamide, teniposide, and prednisone. However, the duodenal infiltrate persisted, although its density seemed to have decreased. In october 1992, oral tetracycline was prescribed and has been continued until now. At the last follow up, the patient was symptom-free, although the duodenal infiltrate was still present.
Patient 4
This patient was a 57 year old man, who in January 1995 presented with a 15 month history of diarrhoea and weight loss. In November 1993, he had been followed in another institution, where duodenal biopsy was performed and coeliac disease was diagnosed. Between November 1993 and June 1994, he was successively treated with a gluten-free diet, corticosteroids, and total parenteral nutrition, but there was no sustained improvement. When the patient was admitted to our department, in January 1995, an enteroscopy was performed. Duodenojejunal and ileal biopsy specimens did not indicate coeliac disease but extensive small intestinal T cell infiltration. Daily oral chlorambucil was started in April 1995; the patient failed to respond to three months of treatment. He also failed to respond to total parenteral nutrition, corticosteroids, and antibiotics. At the last follow up, duodenal infiltrate was still present and his clinical condition was stable, with persistent diarrhoea.
CLINICAL AND MORPHOLOGICAL FEATURES
All four patients presented with longstanding chronic diarrhoea, malabsorption, exudative enteropathy, and weight loss (see table 1). None had an abdominal mass or peripheral lymphadenopathy. Two were prescribed a gluten-free diet at the beginning of their course but did not respond. Small bowel x ray photographs showed dilatation of intestinal loops, transversalisation, and thickening of the jejunal folds in all cases. Upper gastrointestinal endoscopy was normal in two patients and showed coarse duodenal folds with a nodular pattern in the other two. Ileocolonoscopy was normal in all cases. In three of three cases investigated, the search for serum anti-endomysium antibodies, performed while patients were on a normal diet, produced negative results. Patients 3 and 4, for whom HLA typing was performed, lacked the phenotype predisposing to coeliac disease.
PATHOLOGY
In all four patients, an abnormal infiltration of small lymphocytes was noted in the first duodenojejunal biopsy specimens. The lamina propria was densely and diffusely infiltrated by small pleomorphic lymphocytes; in three of four cases, this infiltration extended to the superficial part of the submucosa, but crypt architecture was always preserved (fig 1).The density of the lymphoid infiltrate was homogeneous from the duodenum to the terminal ileum, except in patient 2, whose terminal ileum was normal. Infiltrating cells were small and exhibited a pleomorphic indented nucleus (fig 2). Polymorphonuclear eosinophils and granulomas were associated with the lymphoid infiltrate in three cases (fig 3). The number of IELs was within normal limits (20–30 per 100 epithelial cells; fig 4), except in patient 4 who had an increased number of up to 80 per 100 epithelial cells in some areas. Nevertheless, the number of IELs varied from one place to another. There were no lymphoepithelial lesions.Villi were normal or slightly shortened, and except for patient 4, there was no total villous atrophy. Enterocytes were normal in patients 2 and 3 and displayed some degree of vacuolisation and flattening in patients 1 and 4. In patient 4, a tumour infiltrate with the same histological pattern was observed in the stomach, where it was associated with areas of lymphocytic gastritis containing up to 80 IELs/100 epithelial cells. In the other three cases, gastric biopsy specimens were normal. Colonic biopsy specimens were normal in all patients. On biopsy, the liver was found to be invaded in patients 1 and 2, and isolated granulomas were noted in patient 4. Bone marrow smears and biopsy specimens were normal in all four cases.

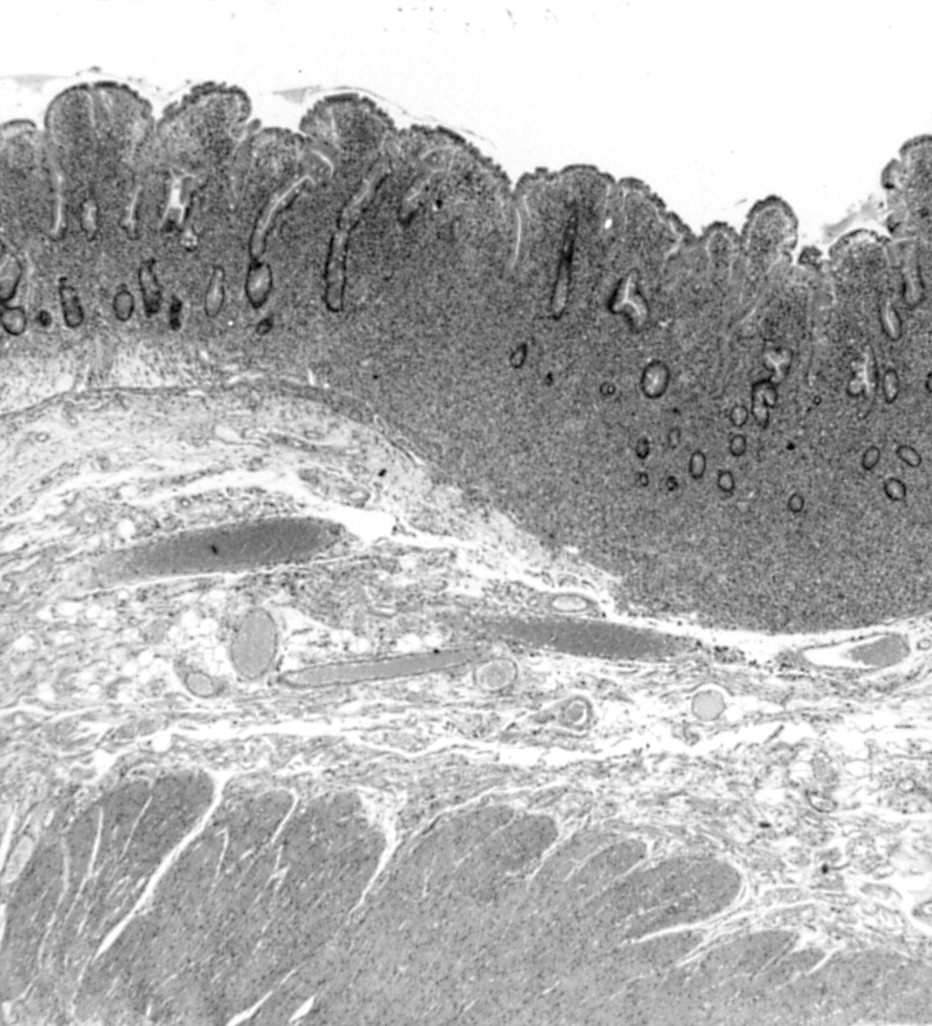
Surgical jejunal resection showing dense lymphoid infiltrate of mucosa and superficial part of submucosa and some degree of villous atrophy. There is no evidence of coeliac disease (patient 1). Haematoxylin-eosin G stain; original magnification × 75.

Surgical jejunal resection at a higher magnification, in which tumour cells appear as small pleomorphic cells with irregularly shaped indented nuclei (patient 2). Haematoxylin-eosin stain; original magnification × 3000.

Surgical jejunal resection from patient 2. Mucosal pleomorphic small T cell infiltrate, associated with a non-caseating granuloma, and extending into the muscularis mucosa. Haematoxylin-eosin stain; original magnification × 750.

Surgical jejunal resection from patient 3. Mucosal pleomorphic small T cell infiltrate is not associated with intraepithelial lymphocytosis. Enterocytes appear normal. Haematoxylin-eosin stain; original magnification × 750.
It is noteworthy that, in all invaded areas, the infiltrating cells exhibited the same histological pattern throughout the whole evolution.
Immunohistological studies disclosed a homogeneous phenotype of infiltrating cells, which were stained by the CD2, CD3, CD5 and CD7 T cell markers, and always expressed CD4 (fig 5) and TCRβ, whereas CD8, CD103 (expressed by normal IELs), and CD57 were constantly negative (table 3).[AQ:2] In the lamina propria, some CD8 reactive cells were always associated with this phenotype. In tumour areas, IELs expressed CD8, and, in patients 3 and 4, they were associated with an increased number of CD4 T cells. In the stomach and colon, which were free of tumour infiltrate, IELs expressed CD8 normally.

Immunohistochemical examination of a frozen jejunal biopsy specimen from patient 4 showing a dense intramucosal CD4+ T cell infiltrate. Anti-CD4 antibody-diaminobenzidine-peroxidase stain; original magnification × 300.
Immunohistochemistry of extensive small intestinal T cell infiltration
NUCLEIC ACID AND CYTOGENETIC STUDIES
Patient 1 had trisomy 5 which was shown on mesenteric lymph nodes. Patient 2 had a t (4;16) (q26;p13) translocation which was evidenced in the peripheral blood and mesenteric lymph nodes. The same monoclonal rearrangement of the TCRβ gene was demonstrated when Southern blot was performed on mesenteric lymph nodes and peripheral blood lymphocytes. Patient 3 had a monoclonal rearrangement of the VγI-Jγ TCR gene shown by PCR on jejunal biopsy specimens. Patient 4 had two preferential VγI-Jγ rearrangements which were identical in the antrum and jejunum, representing 10% of the material.
INVESTIGATIONS OF INFECTION
All patients were HIV negative. The search for serum anti-HTLV-1 antibodies was negative in the three patients tested (nos 2, 3, and 4). Of the four patients tested, only the duodenojejunal biopsy specimen from patient 4 was stained with EBER during in situ hybridisation (fig6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In situ hybridization on duodenojejunal biopsy specimen from patient 4 showing total villous atrophy and positivity of some cells within the lamina propria. EBER probe; original magnification × 300.
Discussion
This study describes the clinical and pathological features of patients with extensive small intestinal T cell infiltration, essentially composed of pleomorphic small lymphocytes of mature CD4+ αβ subtype. There was no evidence of coeliac disease, as suggested by the clinical history, pathological examination of duodenal biopsy specimens, and, when available, serum anti-endomysium antibodies and HLA phenotype. Patients had prolonged survival, although chemotherapy failed to achieve histological remission.
Most patients with gastrointestinal T cell lymphomas have an aggressive course and short survival. Low grade TCLs of the intestine are very rare.22 ,23 The patients described in this study had extensive small intestinal T cell infiltration with a slow relentless course and prolonged survival. They presented with longstanding diarrhoea and weight loss, and, when it was prescribed, were unresponsive to a gluten-free diet. None presented with an abdominal mass, intestinal obstruction, haemorrhage, or perforation. They had dense heavy infiltration of the lamina propria by small lymphoid cells expressing mature T cell antigens of the CD4 subtype. Although Vγ-Jγ junctional regions were not sequenced, there was evidence of monoclonal lymphocyte proliferation in three of these patients. One patient had evidence of oligoclonal proliferation. Three had extraintestinal involvement, indicating malignancy of the infiltrate. In patient 4, lymphoproliferation was oligoclonal and apparently confined to the small intestine, at least until now.
Several kinds of extensive small intestinal T cell infiltration have previously been reported in the literature. The patients described in this study must be differentiated from those presenting with coeliac disease and extensive small intestinal T cell infiltration, consisting of either histologically abnormal small lymphocytes31 ,32or histologically benign but monoclonal lymphocytes.11 ,32-36 Patients with coeliac disease often have a complicated course—that is, non-responsive coeliac disease or ulcerative jejunitis; lymphoproliferation is composed of intraepithelial T cells with an abnormal immunophenotype (CD4 negative, CD8 negative11 ,31 ,35); overall prognosis is poor and, in some of these patients, there may be subsequent evolution to overt TCL which may arise from the dominant clone found in the enteropathic duodenojejunum.33 ,34 ,36 Therefore the patients described in this study can be differentiated from those with coeliac disease on the basis of immunohistochemistry and evolution. The clinical presentation and tumour location of these patients resembled those found in α-chain disease.37 However, in this disease, the small intestine is infiltrated by plasma cells, and not by CD4 T cells.
The presence of non-caseating granulomas was probably due to the fact that neoplastic T cells release cytokines responsible for the local activation of monocytes and eosinophils. As occurs in Hodgkin’s disease, non-caseating granulomas were observed in the liver, without tumoural involvement. In patient 6, there was a t (4;16) (q26;p13) translocation which was shown in the peripheral blood and mesenteric lymph nodes.22 ,38 The breakpoint of both chromosome partners involved the IL2 gene on chromosome 4 and a new gene termed BCMA on chromosome band 16p13.1.38 The predicted sequence of the normal BCMA protein displayed no homology with previously characterised proteins. Subsequent studies showed that the BCMA protein is located in the Golgi apparatus and that its expression is linked to the stage of B lymphocyte differentiation.39 ,40 The role of a hybrid IL2-BCMA mRNA in the tumorigenesis of patient 2 remains unclear. However, studies are underway to determine whether BCMA was overexpressed or mutated in the other patients in the present series.
The aetiological agent of lymphoid infiltration remains unknown. In agreement with previous studies, we found that Epstein-Barr virus was only associated with a small proportion of cases of T cell lymphoproliferation (one of the four patients in this study41-43). Likewise, the search for serum anti-HTLV-1 antibodies produced negative results in these patients.
In conclusion, these results suggest that extensive small intestinal CD4 T cell infiltration is a distinct entity and should be considered as a differential diagnosis in malabsorption syndromes, particularly coeliac disease. Further studies are needed to define optimal treatment strategies.
Acknowledgments
The authors wish to thank Dr F P Chatelet for kindly providing his slides for reassessment. We also thank the staff of the Laboratoire d’Anatomopathologie of the Hôpital Lariboisière, particularly MA Bretel, C Sanchez, and A Gaste, for their expert technical assistance.
Abbreviations used in this paper
- TCL
- T cell lymphoma
- IEL
- intraepithelial lymphocyte
- TCR
- T cell receptor
- PCR
- polymerase chain reaction
- EBER
- Epstein Barr encoded RNA
References
Linked Articles
- Commentary