Article Text

Abstract
BACKGROUND The cause of inflammation in cardiac mucosa at the gastro-oesophageal junction (GOJ) is unclear, both gastro-oesophageal reflux disease (GORD) andHelicobacter pylori having been implicated.
AIMS To describe patterns of gastritis in patients with symptomatic GORD.
METHODS In 150 patients (126 normally located Z-line, 24 Barrett's oesophagus) with symptoms of GORD, biopsies were taken of the GOJ, corpus, and antrum. Inflammation was assessed using the updated Sydney System.
RESULTS For the 126 patients with a normally located Z-line, biopsies of the GOJ revealed cardiac mucosa in 96, fundic mucosa in 29, and squamous mucosa in one. Inflammation in glandular mucosa at the GOJ was present in 99/125 specimens (79%), including 87/96 (91%) with cardiac mucosa and 12/29 (41%) with fundic mucosa. Inflammation in fundic mucosa was closely related toH pylori and active inflammation was only seen in its presence. Inflammation in cardiac mucosa was less closely linked to H pylori. WhenH pylori was present in cardiac mucosa (28/96, 29%) active inflammation was usually present (25/28, 89%). However, active inflammation was also found in 34/68 (50%) cardiac mucosa specimens without H pylori. Overall, 28/87 (32%) biopsies with carditis were colonised withH pylori and 59/87 (68%) were not. InH pylori colonised patients, inflammation was seen throughout the stomach, while in non-colonised patients, it was confined to cardiac mucosa.
CONCLUSIONS Patients with symptomatic GORD had a high prevalence of carditis. This was of two types, H pylori associated and unassociated. Except on Giemsa staining, the two were morphologically identical, suggesting mediation by a similar immunological mechanism.
- cardiac mucosa
- carditis
- gastro- oesophageal junction
- gastro-oesophageal reflux
- Helicobacter pylori
- inflammation
Abbreviations used in this paper
- GOJ
- gastro-oesophageal junction
- GORD
- gastro-oesophageal reflux disease
Statistics from Altmetric.com
- cardiac mucosa
- carditis
- gastro- oesophageal junction
- gastro-oesophageal reflux
- Helicobacter pylori
- inflammation
The reasons for the increasing incidence of adenocarcinoma of the lower oesophagus and gastro-oesophageal junction (GOJ) are unclear.1 ,2 Specialised intestinal metaplasia is accepted to have a premalignant potential when it is associated with a columnarised oesophagus measuring 3 cm or more in length.3-10 The hypothesis that shorter lengths of specialised intestinal metaplasia underlie the genesis of adenocarcinoma at the GOJ has prompted clinicians to biopsy the “no go area” of the GOJ zone. With this approach, specialised intestinal metaplasia has been identified at this site in up to 25% of unselected patients undergoing gastroscopy examination.11-20 Whether this observation has a relation to the subsequent development of adenocarcinoma at this site remains to be established.
As experience with biopsy of the GOJ has grown it has been recognised that histologically the area is often characterised by a heavy chronic inflammatory cell infiltrate.16 ,21 ,22 The term “carditis” has been popularised to describe these observations.16 ,21 ,22 Early reports identified a relation between carditis and gastro-oesophageal reflux disease (GORD),16 ,21 while other investigators have correlated carditis with Helicobacter pyloriinfection.19 Despite these observations there is considerable confusion over what constitutes inflammation within the mucosa of the GOJ.
The purpose of this study was to use a previously validated scoring system (updated Sydney System)23 ,24 to describe the patterns of gastritis in patients with symptomatic GORD. Particular reference was given to inflammation at the GOJ and its relation toH pylori infection.
Patients and methods
Patients undergoing gastroscopy at our institution between November 1996 and July 1998 for the symptoms of GORD, defined by a history of heartburn and/or regurgitation at least twice weekly for at least three months were invited to participate in the study. Exclusion criteria were a past history of foregut surgery apart from cholecystectomy; malignant disease; anticoagulant therapy; andH pylori eradication therapy within the previous three months. The study was approved by Bro-Taf Local Research Ethics Committee; each patient gave informed consent.
ENDOSCOPY
Proton pump inhibitors were discontinued for two weeks prior to endoscopy and H2 receptor antagonists for 48 hours. We postulated that cardiac mucosa would behave in a similar fashion to antral mucosa.25 An earlier pilot study had indicated a 98% concordance rate between urea breath test and antral biopsy culture, for the detection of H pylori, when antisecretory therapy had been discontinued according to the above guidelines.26 Cessation of proton pump inhibitor therapy for shorter intervals was associated with lower concordance rates.
Endoscopy was performed in a standard fashion, with visualisation of the oesophagus, stomach, and duodenum. The presence of oesophagitis was identified and graded according to the Savary-Miller classification. Barrett's oesophagus was defined according to the American College of Gastroenterology guidelines as “a change in the oesophageal epithelium of any length that can be recognised at endoscopy and is confirmed to have intestinal metaplasia by biopsy”.27Barrett's oesophagus was defined as long segment when at least 3 cm in its endoscopic extent, and short segment Barrett's when less than 3 cm in length.
BIOPSY PROTOCOL
In subjects with no endoscopically visible columnar lining to their lower oesophagus, biopsy specimens were obtained from the GOJ (n=3), the mid posterior wall of the gastric corpus (n=2), and the prepyloric antrum (n=2). Specimens from the GOJ were obtained using the retroflexed endoscope, attempting to include the squamocolumnar junction (Z-line) within the biopsy samples. For patients with a visible columnar lining in their lower oesophagus, the GOJ specimens were obtained from the point where the tubular oesophagus blended with the gastric rugal folds. These patients had additional four quadrant biopsy specimens taken, every 2 cm along the columnar segment.
HISTOLOGY
Biopsy specimens were fixed in 4% buffered formalin, embedded in paraffin wax, sectioned, and mounted on glass slides. Sections were stained with haematoxylin and eosin, and Giemsa.
Fundic mucosa was defined histologically by the presence of straight, tightly packed tubular glands composed of parietal and chief cells. Cardiac and antral mucosae were identified by their tubular or coiled racemose glands composed of mucus secreting cells.28 In some patients, cardiac and antral mucosae contained small numbers of parietal cells. Intestinal metaplasia was defined by the presence of goblet cells in glandular mucosa (specialised intestinal metaplasia). Alcian blue (pH 2.5)/periodic acid Schiff staining was employed in selected cases where there was uncertainty about the presence of intestinal metaplasia, which was then defined by the presence of goblet cells containing alcianophilic acid mucins.
Sections were reviewed by a single pathologist who was blinded to the endoscopic findings. For each section the mucosal type was recorded (cardiac, fundic, antral). The degree of neutrophil infiltration and the degree of lamina propria mononuclear cell infiltration were graded 0–3 according to the updated Sydney System.23 The presence of intestinal metaplasia was recorded as present or absent. Where there was disparity within sections between biopsy specimens from a single anatomical site, the score for the most abnormal area was recorded. The presence of H pylori in any Giemsa stained section from the cardia, corpus, or antrum was considered diagnostic of infection.
Following initial histological examination of sections from all patients, adjacent sections of biopsy specimens showing intestinal metaplasia were stained with high iron diamine/alcian blue (pH 2.5) in order to identify sulphomucin expressing incomplete intestinal metaplasia (type 3 intestinal metaplasia).29 ,30
In the Results, biopsy location has been termed anatomically as GOJ, gastric corpus, or gastric antrum; mucosal type has been termed squamous, cardiac, fundic, or antral. Carditis has been used to indicate inflammation in cardiac mucosa, but not fundic mucosa, located at the GOJ.
STATISTICS
Continuous data were compared using the Mann-Whitney U test. Comparison of proportions was by Fisher's exact test or the χ2 test. Significance was taken at the 5% level.
Results
The study population comprised 150 patients with reflux symptoms (90 men, 60 women) of median age 57 years (range 21–85). No patient had previously undergone gastroscopy. Sixty six patients had been taking proton pump inhibitors and 26, H2 receptor antagonists. The remaining 58 patients had not received any form of antisecretory therapy. The endoscopic findings were: 89 (59%) grade 0/I oesophagitis, 30 (20%) grade II/III oesophagitis, and 31 (21%) grade IV oesophagitis. The 31 patients with grade IV oesophagitis comprised seven patients with peptic strictures and 24 patients with Barrett's oesophagus; in 16 patients this was long segment in type, and in the remaining eight, it was short segment in type.
Overall, 44 patients were colonised with H pylori (29%). Bacteria were identified at all three sites (GOJ, corpus, and antrum) in 30 patients (68%). According to anatomical location the rates of H pylori colonisation were 34/44 (77%) for the GOJ, 41/44 (93%) for the corpus, and 39/44 (89%) for the antrum. There were no significant differences in the colonisation rates of patients with GORD when stratified according to Savary-Miller grade of oesophagitis: grades 0 and I (28/89, 31%), grades II and III (5/30, 17%), and grade IV (11/31, 35%).
In the 126 patients with a normally positioned Z-line, biopsy specimens from the GOJ revealed cardiac mucosa in 96 patients (76%), fundic mucosa in 29 patients (23%), and squamous mucosa in one patient (1%). Figure 1 summarises these findings and indicates theH pylori status of the patients. In 54 of the 126 subjects (43%) with a normally located Z-line, the squamocolumnar junction was present in the histological sections. In all patients the junction comprised a squamous to cardiac mucosal interface. There were no examples of a squamous to fundic mucosal interface in these patients—that is, none of the 29 patients with fundic mucosa in biopsy specimens from the GOJ had the squamocolumnar junction included in the histological sections.
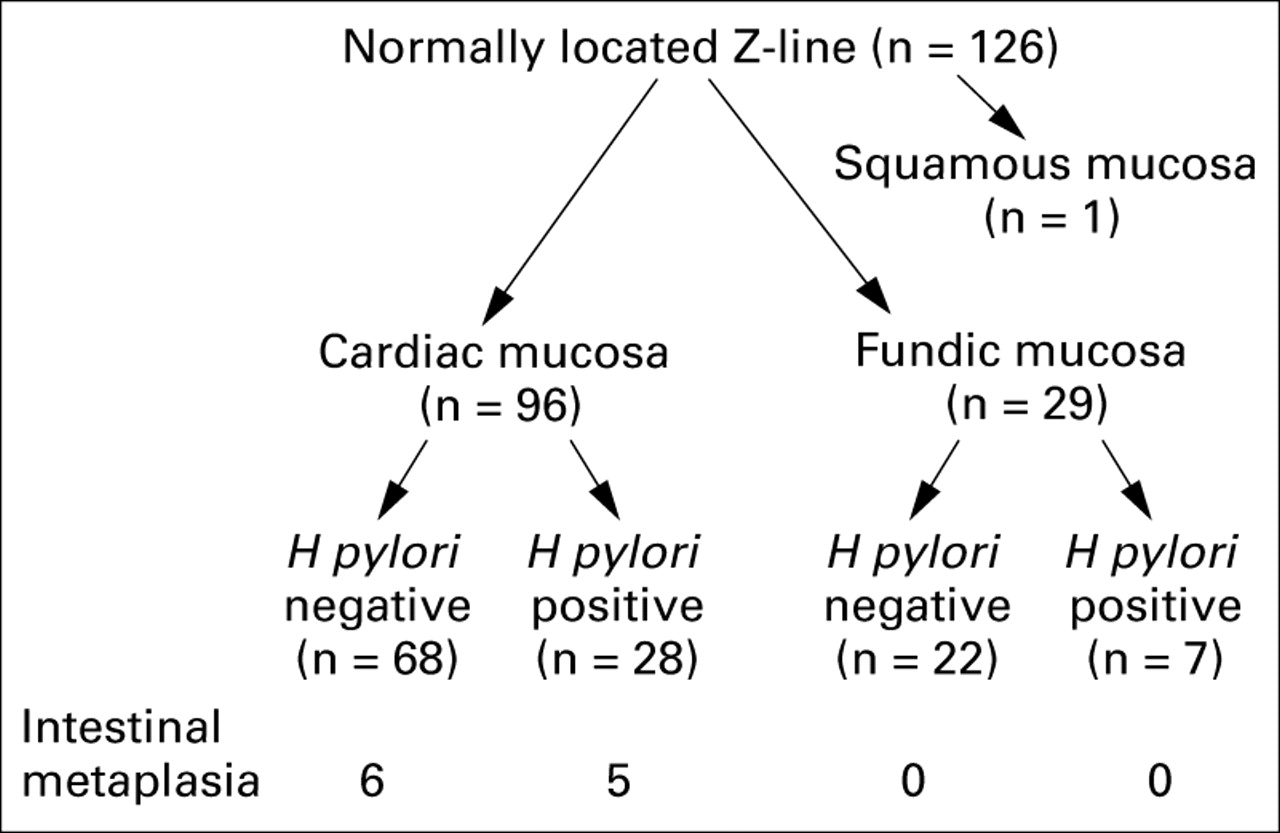
Histology of gastro-oesophageal junction biopsy specimens for the 126 patients with a normally located Z-line. Patients have been subdivided according to mucosal type (cardiac, fundic, squamous) and Helicobacter pylori status. The prevalence of intestinal metaplasia in the gastro-oesophageal junction specimens is indicated.
Inflammatory cell infiltration was present in 99/125 (79%) GOJ biopsy specimens, including 87/96 (91%) specimens with cardiac mucosa and 12/29 (41%) specimens with fundic mucosa (p<0.01). Inflammation of fundic mucosa was closely related to H pylori infection (fig 2) and active inflammation with neutrophils was only seen in the presence of this organism. Inflammation of cardiac mucosa at the GOJ was less closely linked toH pylori. When the organism was present (28/96, 29%) active inflammation was almost invariably present (25/28, 89%). However, active inflammation was also found in 34/68 (50%) cardiac biopsy specimens without H pylori. Overall, 28/87 (32%) GOJ biopsy specimens with carditis were colonised by H pylori and 59/87 (68%) were not.

Prevalence of neutrophil and mononuclear cell infiltration in columnar mucosa obtained from biopsy specimens of the gastro-oesophageal junction in 126 patients with a normally positioned Z-line. For each type of columnar mucosa prevalence of inflammatory cell infiltration is presented according to the presence or absence of Helicobacter pylori infection. Note the high prevalence of acute and chronic inflammation in cardiac type mucosa which was unrelated to H pylori. *p<0.05 v fundic H pylori negative, **p<0.01 v cardiac H pylori negative or fundic H pylori negative, †p<0.01 v fundic H pylori negative.
In H pylori colonised patients inflammation was observed throughout the stomach in each of the three mucosal types (table 1). In contrast, in uncolonised patients, inflammation was confined to cardiac mucosa. Figures 3 and 4 show the prevalence of neutrophil and mononuclear cell infiltration throughout the stomach according to H pylori status. Unlike cardiac mucosa, active inflammation with neutrophils was almost never seen in fundic or antral mucosae in the absence of H pylori.
Relation between histology of cardiac mucosa and more distal gastric mucosa

Prevalence of neutrophil infiltration in columnar mucosa at different locations throughout the stomach for 96 patients with reflux symptoms and cardiac type mucosa on biopsy of the gastro-oesophageal junction. The patients are stratified into Helicobacter pylori positive (n=28) and H pylori negative (n=68). *p<0.05 v fundic H pylori negative and antral H pylori negative, †p<0.05 v all sites in non-colonised individuals, ‡p<0.05 v fundic H pylori negative and antral H pylori negative.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of mononuclear cell infiltration in columnar mucosa at different locations throughout the stomach for 96 patients with reflux symptoms and cardiac type mucosa on biopsy of the gastro-oesophageal junction. The patients are stratified into Helicobacter pylori positive (n=28) and H pylori negative (n=68). *p<0.05 v fundic H pylori negative and antral H pylori negative, **H pylori positive versus H pylori negative.
Table 2 compares the severity of neutrophil and mononuclear cell infiltration for the three mucosal types according toH pylori status. Compared with fundic and antral mucosae the density of neutrophil and mononuclear cell infiltrate was significantly greater in cardiac mucosa in patients without evidence of H pylori colonisation (p<0.01).
Comparison of the severity of acute and chronic inflammation in 96 patients with cardiac type mucosa at the GOJ stratified according to mucosal type and Helicobacter pylori status
INTESTINAL METAPLASIA AT THE GOJ
Biopsy specimens of the anatomical GOJ from the 24 patients with Barrett's oesophagus revealed cardiac mucosa in 17 patients and fundic mucosa in seven. Intestinal metaplasia was present within these specimens in 11/17 with cardiac type mucosa and 0/7 with fundic type mucosa.
Of the 126 patients with a normal appearing Z-line the GOJ biopsy specimens showed intestinal metaplasia in 11 (9%; fig 1). Intestinal metaplasia was present in 11/96 patients with cardiac mucosa but in 0/29 patients with fundic mucosa at the GOJ. There was no significant difference in the prevalence of intestinal metaplasia in cardiac mucosa between patients colonised with H pylori(5/28, 18%) and non-colonised patients (6/68, 9%). The prevalence of cardia intestinal metaplasia in patients with grades 0 and I oesophagitis (7/89, 8%) and those with grades II and III oesophagitis (4/30, 13%) was not significantly different. Patients with cardia intestinal metaplasia were more likely to have intestinal metaplasia identified at more distal gastric sites (5/11, 45%) than patients without cardia intestinal metaplasia (12/114, 11%; p<0.01).
Table 3 shows the prevalence of type 3 intestinal metaplasia according to biopsy location for all patients in whom intestinal metaplasia was identified. There was a high frequency of type 3 intestinal metaplasia in the oesophagus and GOJ, but a low frequency in the distal stomach.
Prevalence of type 3 intestinal metaplasia (IM) according to biopsy location for all 150 patients
Discussion
Using a previously validated scoring system for the assessment of gastritis,23 ,24 our study identified two distinct patterns of carditis in patients with symptomatic GORD. One was associated with H pylori infection and was characterised by inflammation in cardiac, fundic, and antral mucosae (pangastritis). The other, which was unassociated withH pylori infection, comprised inflammation confined to cardiac mucosa (isolated carditis).
There is controversy about the aetiology of carditis; both GORD16 and H pyloriinfection19 have been suggested. In a report by Oberget al,16 inflammation in cardiac mucosa was shown in 237/246 patients (96%) with foregut symptoms. Its presence was significantly associated with defective lower oesophageal sphincter function, but not increased oesophageal acid exposure. The investigators found no significant association between carditis and H pylori colonisation. In contrast, Goldblum and colleagues19 found no difference in the prevalence of carditis between 58 patients with reflux symptoms (40%) and 27 control subjects (41%). As all except one patient with carditis was H pylori colonised, the authors concluded that H pylori was the principal cause of carditis.
There have been two additional publications describing carditis.31 ,32 Both evaluated only H pylori colonised patients. Genta and colleagues31were the first to report that cardiac mucosa was as frequently colonised by the bacterium as mucosa from more distal gastric sites. The authors observed a similar intensity of inflammatory response in cardiac and antral mucosa, both being greater than that seen in fundic mucosa. In the second study, Hackelsberger and colleagues32 found a lower density ofH pylori colonisation in the cardiac mucosa of patients with erosive oesophagitis compared with the bacterial density in other gastric mucosal types.
In our study, when cardiac mucosa was identified at the GOJ of patients with a normally located Z-line, inflammation was present in 91% (87/96). It was H pylori associated in one third of patients and was unassociated in the remaining two thirds. By comparison, when fundic mucosa was identified at this site, inflammation was more closely related to H pylori infection. Indeed, active inflammation with neutrophils was only seen in the presence of this organism.
Based on our observations, it appears that there are three possibilities. Firstly, that all carditis is due toH pylori, but that we failed to identify the organism in two thirds of the patients. This seems unlikely as the sensitivity and specificity of Giemsa staining for the detection ofH pylori are around 90% and 98% respectively based on biopsy specimens from one or two locations.33-35 In our study, biopsy specimens were obtained from three locations. Furthermore, inflammation in all three mucosal types would be expected if H pyloriwere responsible. The second possibility is that carditis is completely unrelated to H pylori. Its identification in one third of patients with carditis is merely coincidental, because this is the frequency of H pyloricolonisation in our study population. Indeed, this value is in agreement with previous studies reporting the prevalence ofH pylori in Western populations.36-39 The third possibility and our favoured explanation is that there are two causes for carditis,H pylori being implicated in one third of cases and another agent in the remaining two thirds. Gastro-oesophageal reflux, in particular bile reflux, has been proposed as a cause of carditis. However, if reflux carditis is the analogue of antral bile reflux gastritis, its histological hallmarks should be a paucicellular response.40-43 As this is not the case, it seems unlikely that bile reflux alone is responsible. It is possible, however, that bile reflux increases the susceptibility of cardiac mucosa to injury by another agent. Purely on histological grounds, it appears that this second agent causes carditis by a mechanism similar toH pylori, given that H pylori negative and H pylori positive carditis were morphologically indistinguishable except on Giemsa staining.
We identified unsuspected intestinal metaplasia at the GOJ in 11/126 patients (9%). This has been termed ultra short segment Barrett's oesophagus and has been noted by other investigators with a frequency ranging from 6 to 36% (median 13%).11-20 44-46 The significance of ultra short segment Barrett's oesophagus is unclear as its relation to adenocarcinoma of the GOJ remains unknown. We did not identify a significant association between H pylori infection and intestinal metaplasia at the GOJ. Previous reports examining this association have yielded conflicting results, with four of the eight papers reporting negative findings,15-17 ,45 and the other four, positive findings.14 ,19 ,20 ,46
The origin and nature of cardiac mucosa itself has been a source of controversy, some investigators believing it to arise by metaplasia of oesophageal squamous mucosa as a response to reflux disease. We, however, consider cardiac mucosa to be a normal finding. Supportive evidence for this is fivefold. Firstly, although it was symptomatic individuals that we studied, when the squamocolumnar junction was included in the histological section, it comprised squamocardiac mucosal apposition in each subject. Secondly, biopsy specimens of the GOJ from 15 subjects (median age 48 years, range 20–84) free of reflux symptoms revealed squamocardiac mucosal apposition in the 12 subjects with a histologically identified squamocolumnar junction (unpublished data). Thirdly, in earlier reports, cardiac mucosa has been identified at the GOJ of healthy volunteers undergoing endoscopy and biopsy.47 ,48 Fourthly, postmortem examination of the GOJ in foetuses, neonates, children, and adults has consistently revealed a zone of cardiac mucosa.49-54 Finally, cardiac mucosa has been identified in every mammal studied to date.49-51 ,55
For intestinal metaplasia of the distal stomach, it is the sulphomucin expressing form (type 3) that has been most closely linked to adenocarcinoma at this site, with little or no excess risk apparent for types 1 and 2 intestinal metaplasia.56 ,57 Patients with Barrett's oesophagus have been previously noted to have a high prevalence of type 3 intestinal metaplasia in the oesophagus, although cancer risk at this location remains to be quantified.58-62 In our study, we identified a high frequency of type 3 intestinal metaplasia at the GOJ, an observation not previously reported. Moreover, the proportion of type 3 metaplasia at the GOJ (50%) was similar to that found in the oesophagus (63%). This is noteworthy given the epidemiological similarities between adenocarcinoma arising in the oesophagus and that arising at the GOJ.1 ,2 We speculate that it is patients with type 3 intestinal metaplasia at the GOJ who are at increased risk for the development of malignancy at this site. The results of surveillance studies of such patients are awaited to confirm or refute this hypothesis.
In summary, this study, which is the first to document carefully the histological features of the entire stomach in patients with symptomatic GORD, indicates a high frequency of carditis in this population. The carditis appears to be of two aetiological types, oneH pylori associated, the other unassociated. The challenge before us is to elucidate the nature and cause of non-H pylori carditis.
Acknowledgments
D J Bowrey was salaried by a Royal College of Surgeons of England/Welsh Office Research Fellowship. Laboratory costs were funded by a grant from the Wales Office of Research and Development for Health and Social Care.
Abbreviations used in this paper
- GOJ
- gastro-oesophageal junction
- GORD
- gastro-oesophageal reflux disease
References
Linked Articles
- Commentary