Article Text

Abstract
BACKGROUND There is a difference in the location of colorectal mucosal lesions and invasive cancers.
AIMS To ascertain whether the location of colorectal neoplasms reflects the carcinogenesis pathway.
METHODS The subject material consisted of 4147 neoplastic lesions that had been resected endoscopically or surgically from 5025 patients. Mucosal lesions and submucosal cancers were classified into depressed and non-depressed types endoscopically or histologically. The relations between macroscopic type, size, histology, and location were investigated.
RESULTS (a) Non-depressed type. A total of 1774 of 3454 (51%) mucosal lesions were located in the right colon, 1212 (35%) in the left colon, and 468 (14%) in the rectum. The incidence of mucosal lesions larger than 10 mm was 10% (185/1774) in the right colon, 21% (254/1212) in the left colon, and 27% (127/468) in the rectum. The incidence of mucosal lesions with villous components was 2% (32/1774) in the right colon, 5% (63/1212) in the left colon, and 13% (62/468) in the rectum. The ratio of submucosal cancers to mucosal lesions was significantly higher in the rectum (0.064, 30/469) than in the left (0.034, 43/1279) or right (0.010, 18/1857) colon. (b) Depressed type. The incidences of depressed type mucosal lesions and submucosal cancers were 5% (83/1857) and 17% (3/18) in the right colon, 5% (67/1279) and 5% (2/43) in the left colon, and 0.2% (1/469) and 0% (0/30) in the rectum, respectively.
CONCLUSION There may be some mechanisms that promote the progression of mucosal lesions to invasive cancers in the left colon and rectum, whereas a de novo pathway from depressed type lesions may be implicated in some cancers of the right colon.
- colorectal cancer
- depressed cancer
- carcinogenesis
Statistics from Altmetric.com
The coexistence of adenomatous and cancerous components and sequential genetic alterations such as K-ras and p53 suggest that adenoma is a precursor of cancer.1-3 The adenoma-carcinoma sequence is generally accepted as a major pathway for the carcinogenesis of colorectal cancer.4-6Morphologically these adenomas are protuberant lesions. However, many Japanese authors have reported flat or depressed type colorectal tumours, and state that these lesions are de novo carcinomas as they are not associated with adenomatous components,7-10 and that the incidence of K-ras mutation is low.11-14Therefore flat or depressed type colorectal tumours may have a different pathway of carcinogenesis from the adenoma-carcinoma sequence.
In the carcinogenesis of colorectal cancers, there may be a difference between the proximal colon and distal colon, as these two subsites originate embryologically from the midgut and hindgut.15Bufill16 and Delattre17 reported distinct genetic categories based on tumour location. It is not clear whether tumour location is related to the above carcinogenesis. In this study, we investigated the clinicopathological characteristics of colorectal tumours on the basis of their location.
Methods
SUBJECTS
A total of 5025 average risk patients underwent total colonoscopy using a videocolonoscope (CF200Z and CF200I; Olympus Optical Co., Tokyo, Japan) at the National Cancer Centre Hospital East from July 1992 to December 1997. Colonoscopy was repeated until all tumours, including diminutive (⩽5 mm) polyps, had been resected endoscopically or surgically, and 4147 neoplastic lesions were used as the subject material in this study. The lesions of patients with familial adenomatous polyposis, hereditary non-polyposis colorectal cancer, and inflammatory bowel disease were excluded.
LOCATION
We categorised the location of the lesions into three groups according to the length of the colonoscope from the anus to the lesions: 0–15 cm, rectum; 16–40 cm, left colon; >41 cm, right colon.
MACROSCOPIC TYPE
Macroscopically, mucosal lesions were classified into the depressed type and non-depressed type on the basis of the presence or absence of a depressed component determined endoscopically. Submucosal cancers were histologically classified as depressed or non-depressed according to the criteria of Kato et al.18 Briefly, lesions were defined as being of the depressed type when the edge of the lesion was depressed compared with the surrounding normal mucosa, and were otherwise considered to be of the non-depressed type (fig 1). The macroscopic type of advanced cancer, which invaded beyond the submucosal layer, was not assessed.
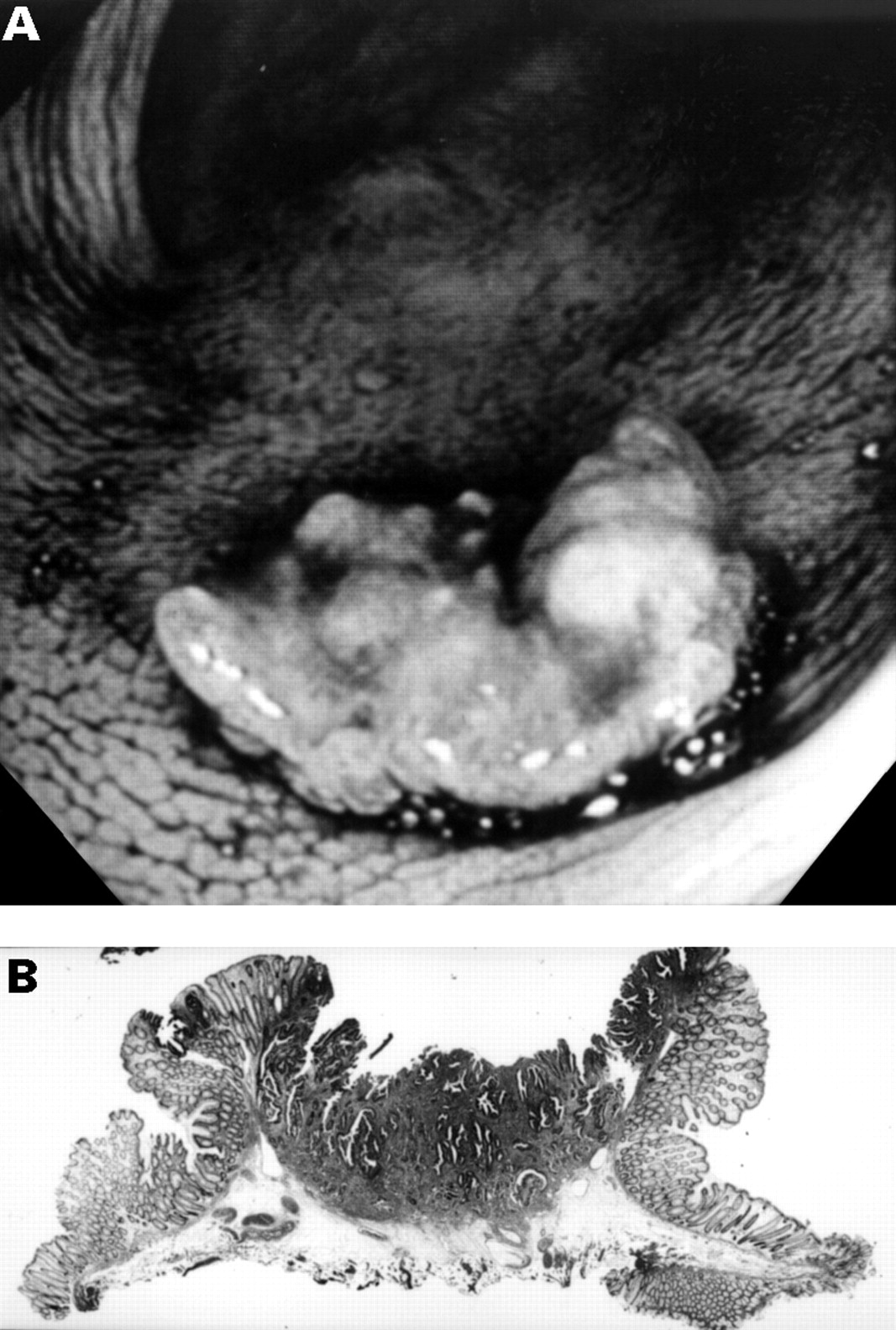
Morphological appearance of the depressed type of submucosal cancer. (A) Endoscopy shows a depressed cancer 11 mm diameter in size; (B) in the cross section of this lesion, the edge is depressed compared with the surrounding normal mucosa.
ADENOMATOUS COMPONENT
In mucosal lesions, the presence or absence of a villous component was investigated histologically. In submucosal cancers, we investigated whether or not they were associated with an adenomatous component. Other clinicopathological features were determined according to the general rules of the Japanese Research Society for Cancer of the Colon and Rectum.19
STATISTICAL ANALYSIS
We compared the clinicopathological characteristics of lesions located in the rectum, left colon, and right colon using the χ2 test and Fisher's exact probability test. A value of p<0.05 was considered significant.
Results
In total, 4147 neoplastic lesions were resected from 3087 patients. The average number of colonoscopic examinations was 1.85 (range 1–15), and the average number of lesions was 1.98 (range 1–14). In all, 684 lesions (16%) were located in the rectum, 1493 (36%) in the left colon, and 1970 (48%) in the right colon. Macroscopically, 151 of 3605 mucosal lesions (4%) and five of 91 (5%) submucosal cancers were of the depressed type. Histologically, 3353 lesions (81%) were adenomas, 252 (6%) were intramucosal cancers, 91 (2%) were submucosal cancers, and 451 (11%) were advanced cancers.
LOCATION AND MACROSCOPIC TYPE OF MUCOSAL LESIONS AND SUBMUCOSAL CANCERS
Figure 2 shows the relation between the location and macroscopic type of mucosal lesions and submucosal cancers. Among the mucosal lesions, the incidence of the depressed type in the rectum (0.2%, 1/469) was significantly lower than that in the left colon (5.2%, 67/1279) and the right colon (4.5%, 83/1857) (rectumv left colon, p<0.0001; rectumv right colon, p<0.0001) (fig 2A). Among the submucosal cancers, the incidence of the depressed type in the rectum (0%, 0/30) was lower than that in the left colon (5%, 2/43) and the right colon (17%, 3/18) (rectum vright colon, p = 0.0472) (fig2B).

Comparison of the incidence of depressed and non-depressed types of neoplastic lesion in the rectum, left colon and right colon. (A) Mucosal lesions; (B) submucosal cancers. A significant difference in the macroscopic type was noted between the rectum and colon (p<0.001). The incidence of depressed submucosal cancers in the right colon was significantly higher than that in the rectum (p = 0.0472).
LOCATION AND SIZE OF NON-DEPRESSED MUCOSAL LESIONS
Figure 3A shows the relation between the location and size of non-depressed mucosal lesions. Among 3605 mucosal lesions, the incidence of lesions 5 mm or less in diameter was 38% (178/468) in the rectum, 39% (476/1212) in the left colon, and 59% (1045/1774) in the right colon, while the incidence of lesions larger than 10 mm was 27% (127/468) in the rectum, 21% (254/1212) in the left colon, and 10% (185/1774) in the right colon. We observed significant differences in the distribution of the size of mucosal lesions among the three locations (rectum v right colon, left colonv right colon: p<0.0001; rectumv left colon: p = 0.0186).

{kind=link}
{kind=link}
{kind=link}
(A) Relation between the location and size of non-depressed mucosal lesions. (B) Relation between the location and incidence of villous components in the non-depressed mucosal lesions. (C) Location of mucosal lesions and submucosal cancers.
LOCATION AND HISTOLOGY OF MUCOSAL LESIONS AND SUBMUCOSAL CANCERS
Figure 3B,C shows the relation between location and histology. Among non-depressed mucosal lesions, the incidence of villous components was 13% (62/468) in the rectum, 5% (63/1212) in the left colon, and 2% (32/1774) in the right colon (p<0.0001 in each group) (fig 3B). None of the depressed type mucosal lesions had villous components. The ratio of submucosal cancers to mucosal lesions was 0.064 (30/469) in the rectum, 0.034 (43/1279) in the left colon, and 0.010 (18/1857) in the right colon (rectum vright colon, left colon v right colon: p<0.0001; rectum v left colon: p = 0.0105) (fig 3C).
MACROSCOPIC TYPE AND ADENOMATOUS COMPONENTS IN SUBMUCOSAL CANCERS
An adenomatous component was observed in 63 of 86 (73%) non-depressed and in none of five (0%) depressed type submucosal cancers (p = 0.0021).
Discussion
Recently, differentiating between flat and depressed type neoplastic lesions has been proposed to be important in recognising the existence of a de novo pathway different from the adenoma-carcinoma sequence.9 ,20 ,21 Some reports have considered small elevated lesions to be the flat type.22-24 However, it is not clear whether these small elevated lesions are included in the polypoid pathway or the de novo pathway. This is one of the reasons why the existence of the de novo pathway is controversial. In this study, we classified mucosal lesions endoscopically into depressed and non-depressed types, and we included small lesions of 5 mm or less in diameter.
Shimoda and colleagues25 proposed that early colorectal cancers could be histologically classified into polypoid and non-polypoid growth, and reported that this categorisation reflected the carcinogenesis pathway. Kato and colleagues18 proposed the subclassification of non-polypoid growth into depressed and flat types, and reported that the depressed type retained the characteristics of a de novo pathway morphologically and genetically, whereas the flat type did not. We classified submucosal cancers into depressed and non-depressed types histologically, and found that none of the depressed type had an adenomatous component whereas 73% of the non-depressed type did. These results suggest that our classification of submucosal cancers may reflect different carcinogenesis pathways.
Bedenne and colleagues26 and Ishii and colleagues21 reported that de novo cancers were predominant in the right colon. In our study, 83 of 151 (55%) depressed type mucosal lesions and three of five (60%) depressed type submucosal cancers were located in the right colon. Thus, some invasive cancers, especially in the right colon, may develop from depressed type mucosal lesions, although the incidence of the depressed type is much lower than that of non-depressed lesions.
In the national polyp study,27 8% of all mucosal lesions were located in the rectum, 61% in the left colon, and 31% in the right colon. In our study, of 3605 mucosal lesions, only 13% were located in the rectum, 36% in the left colon, and 51% in the right colon. In both studies, the proportion of mucosal lesions was relatively low in the rectum. However, it has been reported that about half of all colorectal cancers are localised in the rectosigmoid area.4 There is a discrepancy between the incidence and location of mucosal lesions and advanced cancers.
In the national polyp study,27 large (>10 mm) polyps were observed significantly more often in the distal colon than in the proximal colon. In our study, the proportion of lesions larger than 10 mm was higher in the rectum and the left colon than in the right colon. Histologically, a villous component in mucosal lesions was observed more often in the rectum than in the right and left colon. A villous component is considered to be associated with a high malignant potential.27-32 The ratio of submucosal cancers to mucosal lesions was 0.064 (30/469) in the rectum, 0.034 (43/1279) in the left colon, and 0.010 (18/1857) in the right colon. In patients with familial adenomatous polyposis, the initial advanced cancer is commonly observed in the distal colon.33 These results suggest that mechanisms that promote the progression of mucosal lesions may be implicated in carcinogenesis in the left colon and the rectum.
In conclusion, there may be mechanisms that promote the progression of mucosal lesions to invasive cancer in the left colon and rectum, and a de novo pathway from the depressed type may be implicated in some cancers of the right colon.
Acknowledgments
This work was supported in part by a Grant-in-Aid for Cancer Research from the Ministry of Health and Welfare of the Japanese Government.