Article Text

Abstract
OBJECTIVE Recent research suggests that oats do not harm intestinal villi in adults with coeliac disease. As the immunological effects of oats have not been examined in detail, it was decided to compare the immunological responses of a gluten free diet including oats with those of a conventional gluten free diet.
DESIGN A randomised controlled intervention study over 6–12 months.
SUBJECTS Forty adults with newly diagnosed coeliac disease and 52 with coeliac disease in remission were examined.
INTERVENTION The effects of a gluten free diet including oats and a conventional gluten free diet were compared.
MAIN OUTCOME MEASURES Serum levels of gliadin and reticulin antibodies as well as numbers of intraepithelial lymphocytes (IELs) in intestinal mucosa were examined before and after the intervention.
RESULTS The rate of disappearance of gliadin and reticulin antibodies did not differ between the diet groups in patients with newly diagnosed coeliac disease. Oats also had no effect on gliadin or reticulin antibody levels in the patients with remission. The number of IELs decreased similarly regardless of the diet of newly diagnosed patients, and no increase in the number of IELs was found in the patients in remission with or without oats.
CONCLUSIONS These results strengthen the view that adult patients with coeliac disease can consume moderate amounts of oats without adverse immunological effects.
- coeliac disease
- diet
- oats
- anti-gliadin antibodies
- anti-reticulin antibodies
- intraepithelial lymphocytes
Statistics from Altmetric.com
Wheat, rye, and barley have harmful effects on the small intestinal mucosa of patients with coeliac disease, whereas maize and rice are harmless.1 2 It has been recommended that wheat, rye, barley, and also oats should be avoided.3 4 However, the place of oats in the coeliac diet has been debated.5-10 We did not find any detrimental consequences of oats on duodenal villous architecture, symptoms, or nutritional status in our previous 6–12 month study on the effects of oats in patients with coeliac disease in remission or with newly diagnosed disease.11 In a recent short term Irish study with a small number of patients in remission and without any control group, oats showed no toxic or immunological effects either.12 Newly diagnosed patients were not included in that study.
The objectives of this study were to investigate in a controlled randomised study design11 whether oats in the diets of adult patients with newly diagnosed coeliac disease would have any effect on the rate of decrease in gliadin and reticulin antibody levels, as indicators of humoral immunology, or the number of intraepithelial lymphocytes (IELs), a marker of local immune response. The same variables were also measured in patients with coeliac disease in remission.
Methods
PATIENT POPULATIONS
The composition of the study population has been described in detail previously.11 The final study population consisted of two groups of patients: those with coeliac disease diagnosed earlier (n = 52) and newly diagnosed patients (n = 40).
The original diagnosis of coeliac disease in the previously diagnosed patients was based on the presence of subtotal or total villous atrophy of the duodenal mucosa before introduction of the gluten free diet. The inclusion criteria for these patients were age 18 or older and a normal or almost normal duodenal villous architecture after consumption of a gluten free diet for at least 12 months.
All newly diagnosed patients with subtotal or total villous atrophy without any reason for secondary villous atrophy diagnosed in the Kuopio University Hospital, Finland, were included in the study between 1 December 1988 and 31 December 1990. A patient was excluded if there was any medical condition that the investigator considered sufficiently serious to interfere with the conduction of the trial or to constitute an unacceptable risk to the patient.
Exclusion criteria for both groups were: previous or current corticosteroid treatment for the disease; history of complications of coeliac disease; any neurological, cardiovascular, pulmonary, metabolic, haematological, or endocrine disorder that could hinder participation in the trial; history of drug or alcohol abuse; mental impairment; lack of cooperation or refusal to take part in the trial. Patients were also excluded if the coeliac disease diagnosis was not definite, for instance if there was any other reason for villous atrophy. Also patients whose diet included oats were excluded.
STUDY DESIGN AND DIETS
Patients were randomised by sex into either the oat consuming or the control groups. The clinical nutritionist gave both verbal and written instructions about the diet. Control patients received gluten free cereal free of charge (Raisio Factories-Melia Ltd, Raisio, Finland). The oat consuming groups (oat groups) received products supplemented with oats: two types of gluten free wheat starch flour including 50% oats, muesli including 60% oats, and rolled oat breakfast cereal. Some of the oat products used in this study were also commercially available. The goal for the daily intake of oats was 50–70 g.11 All oat products were made from three Finnish oat strains (Veli, Puhti, and Ryhti). The purity of the oats was regularly monitored. Analysis of gluten content was performed at the National Food Administration in Sweden (Statens Livsmedelsverk, Sweden). Gluten was analysed by a quantitative enzyme immunoassay using a specific monoclonal antibody to ω-gliadin. This antibody detects all prolamins of wheat and rye but only part of barley prolamin. The prolamin of oats, avenin, is not detected by this antibody. All oat samples were gluten free.
EXAMINATIONS
Before the study, a screening gastroscopy was performed with an Olympus GIF Q20 end viewing gastroscope, and two duodenal biopsy specimens were obtained if possible using jumbo forceps (Olympus FB-13K). Specimens were fixed in 10% buffered formalin, processed by standard methods, and stained by van Gieson's method.13The specimens were studied without knowledge of the patient's clinical status. IELs were identified and counted in specimens under a light microscope with a × 100 flat field objective. Lymphocytes from the epithelium of the villi, or in cases of flat mucosa, from the surface epithelium were counted. In each specimen, nuclei were counted in at least 200 epithelial cells.
Serum for antibody testing was withdrawn at baseline and at one, three, six, and 12 months. IgA and IgG gliadin antibodies were measured using an inhouse solid phase enzyme linked immunosorbent assay (ELISA).14 The results were obtained from a standard curve established by dilutions of a positive reference serum and converted into concentrations of arbitrary ELISA units (EU/ml). Serum samples containing gliadin antibodies at higher concentrations than known healthy age matched controls, +2 SD, were considered positive. Serum IgA R1-type reticulin antibodies were determined by an indirect immunofluorescence method, by using unfixed cryostat sections of rat kidney, liver, stomach, and heart as antigen.15 16Patients' sera were screened at dilutions of 1:5 and 1:50 with fluorescein isothiocyanate conjugated antiserum to human IgA (goat antiserum; Sanoti Diagnostics Pasteur Inc, Chaska, Minnesota, USA; dilution 1:120). Positive sera were further titrated 1:50, 1:100, 1:200, 1:500, 1:1000, 1:2000, 1:4000, and 1:8000.
Food records, clinical assessments and laboratory screening were carried out concurrently. Endoscopies with duodenal biopsies were performed at baseline, six months, and 12 months for patients with newly diagnosed coeliac disease.
PATIENT WITHDRAWALS
There were 11 withdrawals: six in the remission group and five in the group of newly diagnosed patients. Two patients with dermatitis herpetiformis in the control and two in the oat group reported worsening of itching without any signs of dermatitis and therefore skin biopsies and histochemical analyses were not performed. Two patients in the oat group withdrew because of abdominal symptoms (one patient with earlier diagnosed disease and one newly diagnosed). They showed no clinical or histopathological evidence of deterioration of coeliac disease on examination of duodenal biopsy specimens. Three patients in the control group and two in the oat group refused to continue without giving any reason.
The study protocol was approved by the ethics committee of Kuopio University. All patients received written information about the trial, and verbal consent was obtained from each before they started the diet. Patients were also informed that they could withdraw from the study at any point.
STATISTICAL ANALYSIS
All the analyses were carried out with the intention to treat principle. Statistical analyses were performed using the SPSS-PC (SPSS Inc, Chicago, Illinois, USA) and CIA programs.17Non-parametric tests were used when variables did not have a normal distribution and equal variance. The differences between the groups were assessed by the Mann-Whitney U test. The results are presented as means (SD) or medians (range). The 95% confidence intervals were calculated for the differences in change as median or as mean values between the two groups. The Fisher exact test was used to analyse the differences between the study groups in frequency and the proportion of categorised variables as normal values. The differences between the time points were analysed by the McNemar test.
Results
The mean oat intake was 43.6 (11.3) g/day at six months and 46.6 (13.3) g/day at 12 months for the newly diagnosed patients. The consumption of oats was 49.9 (14.7) g/day at six months for the patients in remission. Of the original study groups, 14 (74%) newly diagnosed patients and 21 (81%) patients in remission consumed more than 30 g of oats a day at the end of the study.11
SERUM LEVELS OF GLIADIN AND RETICULIN ANTIBODIES
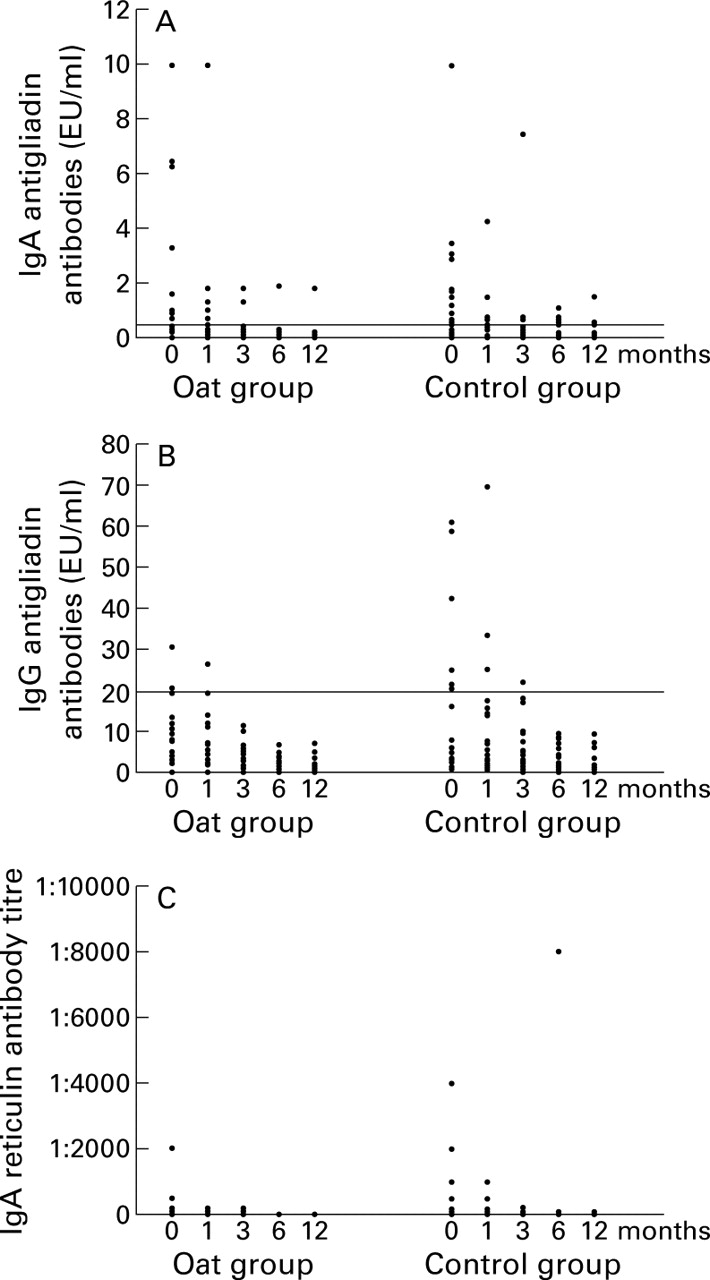
At the beginning of the study, 17% of newly diagnosed patients in the oat group and 29% in the control group were anti-reticulin IgA negative, and 50% of them were anti-gliadin IgA negative in the oat group and 38% in the control group. Respectively 84% and 72% were anti-gliadin IgG negative. In the newly diagnosed patients the rates of disappearance of the antibodies were similar regardless of the diet (table 1, fig 1). The median levels of gliadin (IgA, IgG) and reticulin (IgA) antibodies in the patients with coeliac disease in remission did not differ significantly at any point of the study in the oat group compared with the control group (table 1). The single high titre of anti-reticulin IgA in one patient of the control group at six months (fig 1C) can be explained by temporary non-compliance with the diet.
Effect of oats in the diet of adult patients with coeliac disease and gliadin and reticulin antibodies

{kind=link}
Titres of IgA (A) and IgG (B) gliadin antibodies and IgA (C) reticulin antibodies in the oat and control groups of newly diagnosed coeliac patients determined at baseline, and at one, three, six, and 12 months after the institution of the diet. There were no significant differences between the groups (p>0.10; Fisher test). Within group changes were significant for anti-gliadin IgA (p = 0.016 and p = 0.002) and for reticulin antibodies (p = 0.001 and p = 0.002) in both groups, and for anti-gliadin IgG in the control group (p = 0.031) (McNemar test). Normal levels of anti-gliadin IgA are <0.5 EU/ml and of anti-gliadin IgG <20 EU/ml; normal values of IgA reticulin antibody are titres <5. The horizontal line in (A) and (B) represent the upper cut off limit of normal values of IgA and IgG gliadin antibodies respectively. At 12 months, three patients (one in the oat consuming group and two in the control group) had positive (>0.5) anti-gliadin IgA. All patients had normal anti-gliadin IgG levels. At 12 months, three patients (one in the oat consuming group and two in the control group) had anti-reticulin IgA levels of 5–50 EU/ml.
INTRAEPITHELIAL LYMPHOCYTES
In the patients with newly diagnosed coeliac disease, the IEL counts in the oat group and the control group decreased at six and 12 months at a similar rate (table 2). There were no significant differences between the study groups at any point of the study.
Effect of oats in the diet of adult patients with coeliac disease on total intraepithelial lymphocytes (IELs)
The mean IEL counts of the patients in remission in the oat and control groups stayed at the same level for six months (table 2).
Discussion
We have previously reported the suitability of oats for adult coeliac patients as a part of their otherwise gluten free diet.11 This was based on findings of no harmful effects on duodenal mucosa, laboratory variables, nutritional status, and subjective wellbeing. Our present results show that oats do not prevent normalisation of gliadin and reticulin antibodies or the number of IELs in the duodenal mucosa of newly diagnosed patients. The use of oats in the diet also produces no unfavourable local or humoral immunological effects in adults with coeliac disease in remission. In a recent study of 10 patients in remission, 50 g of oats a day for three months did not cause any significant changes in the number of IELs or the levels of gliadin antibodies.12 The same was also true in two recent studies on patients with dermatitis herpetiformis treated with a diet including oats.18 19 The results of the present report and the former studies11 12 extend our knowledge of the effects of oats in coeliac disease and emphasise its safety as a part of a gluten free diet for adult patients with coeliac disease.
In coeliac disease, patients are sensitised to gluten, and serum gliadin antibodies are often detected. In children, gliadin antibodies are highly sensitive and specific for diagnosis of coeliac disease19 20 In the elderly, positive values for gliadin antibodies do not always indicate undetected coeliac disease, but may represent a normal response to dietary antigens.21 On the other hand, serum reticulin antibodies are both sensitive and disease specific.22 In our hands, classical serum reticulin antibody titres correlate well with endomysial antibodies.16 22
Serum IgA class gliadin antibody concentrations have been used as evidence of dietary compliance as well as as markers of mucosal damage in patients with coeliac disease who are eating gluten.23 24 In adults with coeliac disease, after two years on a strict gluten free diet, no significant difference in serum IgA class gliadin antibody concentrations has been found compared with normal subjects.25 Positive values for both IgA and IgG class gliadin antibodies seem to be more related to the lack of improvement in the jejunal lesions than to the strictness or duration of gluten withdrawal.26
Serum levels of reticulin antibodies have been shown to be reliable for predicting mucosal relapse in coeliac disease. In a study of postpubertal patients with coeliac disease, a diet containing normal amounts of gluten caused both histological relapse of coeliac disease and an increase in reticulin antibody levels in all patients, whereas gliadin antibody was positive only in 89% of these cases.27
High IEL counts in the jejunal mucosa of untreated patients with coeliac disease are typical, but some patients with coeliac disease in remission may still have high numbers of IEL.28 29 There is a dose dependent effect of ingestion of gliadin on jejunal villous morphometry and the numbers of IELs in children with coeliac disease.30 In the present study, the IEL count was similar at the end of the follow up in all diet groups, confirming the safety of oats in patients with coeliac disease.
In vitro culture experiments have shown avenin, the prolamin of oats, to activate intestinal cell mediated immunity in coeliac disease.31 32 Large quantities of avenin have also induced lymphocyte infiltration when instilled in the rectal mucosa of coeliac patients.32 These observations are not in accordance with clinical studies, which have shown reasonable amounts of oats—that is, avenin—to be well tolerated and not to cause mucosal damage of the small intestine11 12 18 19 33 or immune activation in patients with either coeliac disease or dermatitis herpetiformis in remission.12 18 19 33
It has been suggested that conventional oats may be contaminated with wheat during growth or the milling process.18 The purity of the oat products used in previous studies11 12 18 19 33 and the present one was confirmed by chemical analysis, which adds reliability to the favourable results of tolerance to oats both in coeliac disease and dermatitis herpetiformis. However, it is possible to ingest small amounts of gluten through eating contaminated processed food based on any initially gluten free products. In addition, subconscious and conscious lapses in diet have also been considered in interpreting high antibody titres during dietary treatment.34 35 The few withdrawals in our study do not seem to have been caused by oats, as the products were found to be free of contamination in the chemical analyses.
In this study, patients with severe coeliac disease—that is, those who needed corticosteroids to obtain remission—were excluded. In the Irish study, one patient who was very sensitive to trace amounts of gluten also tolerated oats.12 Two other patients showed evidence of relapse during a separate gluten “microchallenge”, although oats did not have any harmful effects.12 Thus even patients who are exceptionally sensitive to gluten seem to be able to consume oats. However, no information is available on oat tolerance in cases of refractory coeliac disease. More clinical studies are needed to ensure the safety of oats when consumed permanently in a coeliac diet as well as to determine the effect of larger amounts of oats.
In conclusion, our results show that oats used as part of an otherwise gluten free diet in adults with coeliac disease in remission do not cause any changes in humoral or local immunological responses, as measured by levels of gliadin and reticulin antibodies or numbers of IELs. More importantly, our report shows that a gluten free diet containing oats normalises gliadin and reticulin antibodies as well as the number of IELs in the intestinal mucosa of newly diagnosed patients at the same rate as in patients consuming a conventional strict gluten free diet. These results further support the conception that adult coeliac patients can eat moderate amounts of oats without harmful effect.
Acknowledgments
The work was supported by grants from the Yrjö Jahnsson Foundation and the Finnish Gastroenterological Association. The oats products were supplied by Raisio Factories-Melia Ltd, Raisio, Finland and given to the study patients free of charge.
References
Footnotes
- Abbreviations used in this paper:
- IEL
- intraepithelial lymphocyte
- EU/ml
- enzyme immunosorbent assay unit