Article Text

Abstract
BACKGROUND There is significant geographic variation in the reported incidence of ulcerative colitis.
AIMS To update the incidence and prevalence of ulcerative colitis in Olmsted County, Minnesota, examine temporal trends, and determine overall survival.
PATIENTS All Olmsted County residents diagnosed with ulcerative colitis between 1940 and 1993 (incidence cases), and all residents with ulcerative colitis alive on 1 January 1991 (prevalence cases).
METHODS Incidence and prevalence rates were adjusted using 1990 US census figures for whites. The effects of age, sex, and calendar year on incidence rates were evaluated using Poisson regression. Survival from diagnosis was compared with that expected for US north-central whites.
RESULTS Between 1940 and 1993, 278 incidence cases were identified, for an adjusted incidence rate of 7.6 cases per 100 000 person years (95% confidence interval (CI), 6.7 to 8.5). On 1 January 1991, there were 218 residents with definite or probable ulcerative colitis, for an adjusted prevalence rate of 229 cases per 100 000 (95% CI, 198 to 260). Increased incidence rates were associated with later calendar years (p<0.002), younger age (p<0.0001), urban residence (p<0.0001), and male sex (p<0.003). Overall survival was similar to that expected (p>0.2).
CONCLUSIONS The overall incidence rate of ulcerative colitis in Olmsted County increased until the 1970s, and remained stable thereafter. Incidence rates among men and urban residents were significantly higher. The prevalence rate in Rochester in 1991 was 19% higher than that in 1980. Overall survival was similar to that of the general population.
- ulcerative colitis
- incidence
- prevalence
- survival
- prognosis
- epidemiology
Statistics from Altmetric.com
There is significant geographic variation in the reported incidence of ulcerative colitis.1-5 Whether this reflects differences in case definition and ascertainment or true variation owing to environmental or genetic factors remains unclear. Many centres, predominantly in northern Europe, have reported stable or slightly increasing incidence rates for ulcerative colitis over the past five decades,6-22 in contrast to a sharp increase in incidence followed by a plateau beginning in the 1970s for Crohn's disease. Early reports suggested considerable excess mortality associated with ulcerative colitis, but more recent studies have shown little or no significant decrease in survival.23-26
Data from North America27-34 have suggested similar trends of incidence, prevalence, and survival, but many studies have been limited by incomplete case ascertainment. The health care delivery and record keeping systems in the United States are not conducive to population based studies of disease, especially if hospitalisation for the given disease or its complications does not routinely occur. In Olmsted County, Minnesota, population based studies are possible, because the small number of institutions that provide health care share a linked diagnostic index.35 36 Population based epidemiological studies may reflect the true spectrum of illness, in contrast to studies based on patients seen at referral centres.35 36
The incidence and prevalence rates of ulcerative colitis in Rochester, Minnesota (the central city of Olmsted County) have been reported previously.29 30 Sedlack et alnoted a twofold increase in incidence between 1935 and 1975 when cases of Crohn's colitis were excluded.29 Stonningtonet al determined the incidence of ulcerative colitis between 1960 and 1979, and noted a slight decrease in incidence between 1960–69 and 1970–79.30 Both groups noted a high proportion of cases of proctitis and a male predominance of incident cases. The prevalence of ulcerative colitis in 1980 was the highest reported at that time, perhaps because of inclusion of probable cases.30 In a separate analysis of prognosis, overall survival was found to be similar to that expected for the general age and sex matched population.31 Both studies showed that the clinical spectrum of disease, when studied in a population based fashion, is often milder than that derived from referral centres.29-31 35 36
Continued study of the trends in incidence and prevalence rates and mortality of ulcerative colitis may shed light on its aetiology. Furthermore, an updated, population based inception cohort may serve as a platform for further detailed epidemiological study of ulcerative colitis. In the current study, the inception cohort of Olmsted County residents with ulcerative colitis was updated to 1993, previously identified cases were reviewed to ensure consistent diagnostic criteria, and the prevalence of ulcerative colitis in Olmsted County on 1 January 1991 was determined. Temporal trends in the incidence of ulcerative colitis over a 54 year period were examined. Finally, overall survival was estimated and potential risk factors for death were examined.
Methods
SETTING
Olmsted County, situated in south-eastern Minnesota, comprised approximately 106 000 people in the 1990 US Census. The county's urban centre, Rochester, comprised approximately 71 000 people in 1990. The largest employers in 1990 were Mayo Medical Center and International Business Machines. The remainder of the county is predominantly rural. In 1990, 96% of the population was white. Although 25% of the residents are employed in health care services (versus 8% nationwide) and the level of education is higher (30% have completed college versus 21% nationwide), the residents of Olmsted County are socioeconomically similar to the US white population.36
ROCHESTER EPIDEMIOLOGY PROJECT
The resources of the Rochester Epidemiology Project were used to identify permanent residents of Olmsted County, Minnesota, who were diagnosed with ulcerative colitis between 1970 and 1993. This unique medical records linkage system exploits the fact that virtually all the health care of the residents of Olmsted County is provided by two organisations: Mayo Medical Center, consisting of Mayo Clinic and its two affiliated hospitals, St Mary's and Rochester Methodist; and Olmsted Medical Center, consisting of a smaller multispecialty group and its affiliated hospital.35 36 In any three year period, over 90% of county residents are examined at either one of the two health care systems.36 Diagnoses generated from all outpatient visits, emergency room visits, hospitalisations, nursing home visits, surgical procedures, autopsy examinations, and death certificates are recorded in a central diagnostic index. Thus, it is possible to identify all cases of a given disease for which patients sought medical attention.35 36
CASE ASCERTAINMENT
The study was approved by the institutional review boards of Mayo Medical Center and Olmsted Medical Center. The complete (inpatient and outpatient) medical records of all potential cases identified through the diagnostic index were reviewed, and a diagnosis of “definite” ulcerative colitis was made if a potential case met the following criteria on two studies separated by at least six months: diffusely granular or friable colonic mucosa on endoscopy; and continuous involvement as observed by endoscopy or bariumx ray. Potential cases with only one diagnostic study, or two diagnostic studies separated by less than six months, were deemed “probable” ulcerative colitis. Cases with involvement outside of the colon, with the exception of “backwash ileitis”, were excluded. Cases with another readily identifiable cause for colitis, such as infectious colitis (including pseudomembranous) or ischaemic colitis, were excluded. These diagnostic criteria were identical to those used in a previous study of ulcerative colitis in Olmsted County.30 The medical records of a random sample of 100 patients with a diagnosis of “non-specific colitis” were reviewed for evidence of idiopathic inflammatory bowel disease. No cases of ulcerative colitis or Crohn's disease were identified in this sample.
The medical records of all patients in previous studies of ulcerative colitis29 30 or Crohn's disease37 38 in Olmsted County were re-reviewed to confirm the diagnosis of ulcerative colitis. Specifically, patients with evidence of distal colonic sparing, linear or aphthous colonic ulcers, or ileal involvement who had been classified as having ulcerative colitis in previous studies were reclassified as having Crohn's colitis. Patients with rectal sparing alone were not reclassified.
We performed a concurrent study of the incidence, prevalence, and survival of county residents with Crohn's disease.39Potential cases in both studies were categorised as having ulcerative colitis or Crohn's disease based on all available clinical, radiographic, endoscopic, and histological evidence. By definition, an individual patient could not be counted in both studies, and there was no category of “indeterminate colitis”.
The date of onset of symptoms, date of diagnosis, residency on 1 January 1991, last follow up date, and vital status at last follow up were recorded. Death certificates were obtained for all patients who had died. All cases from previous studies were also re-reviewed for the above data. Follow up was complete to death or 1 January 1994 in 84%.
INCIDENCE AND PREVALENCE CALCULATIONS
The entire population of Olmsted County from 1940 to 1993 was considered at risk for ulcerative colitis. The denominators age and sex specific person years were derived from decennial US Census figures. When applicable, rates were age and sex adjusted using US whites in 1990 as the standard. All residents of Olmsted County with ulcerative colitis on 1 January 1991 were included in the prevalence calculation (including patients with ulcerative colitis who had moved to Olmsted County after diagnosis or less than one year before diagnosis). Ninety five per cent confidence intervals (95% CI) of incidence and prevalence rates were estimated assuming a Poisson distribution of cases. Potential factors that influence the incidence of ulcerative colitis, including age at diagnosis, sex, residence (urban versus rural), and calendar year of diagnosis, were evaluated with a Poisson regression model. Age at diagnosis (mid points of 10 year age groups) was considered as a continuous variable, and an age squared term was included in the model to account for non-linear trends in age. Calendar year of diagnosis was evaluated as both a continuous variable and as a categorical variable (five year calendar year intervals).
SURVIVAL
Overall survival for the entire ulcerative colitis inception cohort (date of diagnosis to date of last follow up or death) was estimated using the product limit life table method. Observed survival was compared with expected survival using age and sex specific expected death rates for Minnesota whites in 1990 (log rank test). This analysis was also stratified by sex, and decade of diagnosis (1944–53, 1954–63, etc). A Cox proportional hazards regression model examined the association of survival with age at diagnosis, sex, and calendar decade of diagnosis.
Results
DEMOGRAPHIC CHARACTERISTICS
Between 1940 and 1993, 278 Olmsted County residents were diagnosed with ulcerative colitis (251 definite cases and 27 probable cases). There were 156 men (56%), resulting in a male to female ratio of 1.3:1. The median age at diagnosis was 34.5 years (range 7–90). The median interval between symptom onset and diagnosis was 0.1 years range (0–17). The diagnosis was most commonly made in the third and fourth decades of life (53%; fig 1). However, there was a significant difference in the distribution of age at diagnosis between men and women. In women, the age specific incidence rates decreased considerably after the fourth decade of life, but it remained relatively high in men (fig 1). Seventy seven patients (28%) had proctitis, 68 (25%) had left sided involvement (up to and including splenic flexure), and 131 (47%) had extensive or pancolonic involvement. The extent of involvement could not be determined in two patients who sought medical care elsewhere.

Crude incidence of ulcerative colitis in Olmsted County, 1940–93, by age at diagnosis and sex.
INCIDENCE
The crude incidence rate of ulcerative colitis in Olmsted County between 1940 and 1993, including probable cases, was 7.0 cases per 100 000 person years. If probable cases are excluded, the crude rate was 6.3 definite cases per 100 000 person years. The age and sex adjusted incidence rate, including probable cases, was 7.6 cases per 100 000 person years (95% CI, 6.7 to 8.5). The adjusted rate for definite cases only was 6.8 cases per 100 000 person years (95% CI, 5.9 to 7.7). The adjusted incidence rate (definite and probable cases) in the city of Rochester was 9.6 cases per 100 000 person years (95% CI, 8.3 to 10.8), significantly higher than the adjusted rate of 3.9 cases per 100 000 person years in rural Olmsted County (95% CI, 2.9 to 5.0). (The overall incidence rate in Olmsted County in the current study should not be directly compared with incidence rates from previous studies, as they included only the city of Rochester, and not the rural county where the incidence was significantly lower.29 30) The adjusted incidence rates, stratified by maximal extent of ulcerative colitis, were 3.6 cases per 100 000 person years for pancolitis (95% CI, 3.0 to 4.2), 2.0 cases per 100 000 person years for left sided disease (95% CI, 1.5 to 2.5), and 2.2 cases per 100 000 person years for proctitis (95% CI, 1.7 to 2.7).
TEMPORAL TRENDS
The percentage of incidence cases who were men increased from 37% in 1944–53 to 52% in 1954–73 to 60% in 1974–93. The mean age at diagnosis did not change significantly over time (see below). The median interval between onset of symptoms and actual diagnosis was 0.5 years (range 6 days to 17.0 years) in patients diagnosed between 1944 and 1953. This interval shortened in subsequent decades. In the final decade of the study, the median interval between symptom onset and diagnosis was 0.1 years (range 0–8.3).
The incidence of ulcerative colitis increased greatly during the study period in both men and women (fig 2). The adjusted incidence rate rose from 0.6 cases per 100 000 person years in 1940–43 to 8.3 cases per 100 000 person years in 1984–93, with a peak rate of 9.4 cases per 100 000 person years in 1974–83 (table 1). For men, the adjusted incidence rose from 1.2 cases per 100 000 person years in 1940–43 to 11.6 cases per 100 000 person years in 1974–83, and declined slightly thereafter. In women, the adjusted incidence rose from 0 cases per 100 000 person years in 1940–43 to a peak of 8.4 cases per 100 000 person years in 1964–73, with a small decline thereafter (7.1 and 6.1 cases per 100 000 person years in 1974–83 and 1984–93, respectively).

Adjusted incidence of ulcerative colitis in Olmsted County, 1940–93, by year of diagnosis and sex. Sex specific rates are age adjusted to the US white population, 1990; the total rate is age and sex adjusted to the US white population, 1990.
Incidence of ulcerative colitis in Olmsted County by sex, age, and calendar year1-150
The incidence of pancolitis rose from 1.4 cases per 100 000 person years in 1944–53 to 4.5 cases per 100 000 person years in 1964–73, and stabilised thereafter (table 2). The incidence of pancolitis continued to rise in men (from 4.8 cases to 6.2 cases per 100 000 person years in 1964–73 and 1984–93, respectively). However, in women, the pancolitis incidence dropped from 4.3 to 3.1 cases per 100 000 person years in 1964–73 and 1984–93, respectively. For left sided disease, the incidence peaked in 1974–83 for both men and women, although rates were consistently 30 to 100% higher in men during any given calendar decade (table 2). Proctitis incidence rates peaked in 1964–83, and declined thereafter. Rates for proctitis were not significantly different among men or women (table2).
Incidence of ulcerative colitis in Olmsted County by year, extent, and sex2-150
The incidence of ulcerative colitis rose over time in both the city of Rochester and rural Olmsted County (fig 3). In the rural areas, the peak incidence rate seemed to occur a decade later (1974–83) than in the city (1964–73). Only in the last two decades of the study did the incidence rates in the urban and rural areas begin to converge. Sex differences in incidence were more apparent among Rochester cases than among rural cases (fig 3). The Rochester and rural cases did not differ significantly by median age at diagnosis (35 years for Rochester versus 33 years for rural Olmsted County); median interval between symptom onset and diagnosis (55 versus 34 days); or sex distribution (55% versus 58% male). There was a trend towards differences in extent of disease (43% pancolitis and 31% proctitis in Rochester versus 62% pancolitis and 15% proctitis in rural Olmsted County), but this was of borderline statistical significance (p=0.053, Fisher's exact test).

Adjusted incidence of ulcerative colitis in Olmsted County, 1944–93, by year of diagnosis, sex, and rural versus urban residence. Rates are age adjusted to the US white population, 1990.
The distribution of age at onset of ulcerative colitis did not change significantly over the course of the study. The median age at diagnosis decreased slightly, from 37.0 years in 1944–53 to 34.5 years in 1984–93. In contrast to Crohn's disease, where a striking increase in incidence among 20–29 year olds occurred out of proportion to other age groups after 1964,39 the rise in incidence of ulcerative colitis seemed to occur in all age groups. The highest incidence rate recorded was in 20–29 year olds between 1964 and 1973 (18.9 cases per 100 000 person years). In later decades, the peak age specific incidence rate shifted to the 30–50 year old age groups. Although the shift in peak age specific incidence rates occurred in both sexes, it seemed more pronounced in men (table 1). The frequency of paediatric cases of ulcerative colitis relative to all cases diagnosed did not change over the course of the study (9% of all cases until 1973, versus 10% of all cases after 1973).
A Poisson regression model was used to examine the effects of age at diagnosis, sex, residence, and calendar year of diagnosis on incidence rates. Both age at diagnosis (p<0.0001) and its square (p<0.0001) were independently associated with incidence rates, suggesting a non-linear relation between age and incidence rates. Evaluating calendar year at diagnosis as a categorical variable and using the 1984–93 incidence rate as a baseline, the incidence rates before 1964 were significantly lower (p<0.03). The overall trend of rising incidence rates was significant (p<0.001). Calendar year at diagnosis was significantly associated with incidence rates when evaluated as a continuous variable as well (p<0.002). Incidence rates were higher in men than in women (p<0.003). Urban residence was significantly associated with higher incidence (p<0.0001). There seemed to be a significant interaction between urban/rural residence and calendar year (p<0.008), which reflects the rising incidence rate in the rural areas versus the stable incidence rate in Rochester for the last two decades of the study. Similar results were noted when probable cases were excluded from the Poisson regression analysis.
PREVALENCE
On 1 January 1991, there were 218 Olmsted County residents alive with a diagnosis of ulcerative colitis (201 definite cases and 17 probable cases). Sixty eight prevalence cases (31%) were not incidence cases. The crude prevalence rate on this date was 206 cases per 100 000 persons. If probable cases are excluded, the crude rate was 190 cases per 100 000 persons. Table 3 shows the age and sex specific prevalence rates, including probable cases. The age and sex adjusted prevalence rate was 229 cases per 100 000 persons (95% CI, 198 to 260). If probable cases are excluded, the adjusted prevalence rate was 210 cases per 100 000 persons (95% CI, 181 to 240).
Prevalence of ulcerative colitis in Olmsted County on 1 January 1991 by age and sex3-150
There was a significant difference in prevalence in Rochester versus the remainder of Olmsted County. In rural Olmsted County, the adjusted prevalence rate was 144 cases per 100 000 persons (95% CI, 103 to 184). The adjusted rate in the city of Rochester was almost twice as high at 268 cases per 100 000 persons (95% CI, 227 to 309). The latter rate is 19% higher than the prevalence of ulcerative colitis in Rochester in 1980 (225 cases per 100 000 persons; 95% CI, 184 to 266),30 and 127% higher than the prevalence in 1965 (118 cases per 100 000 persons).29 The highest prevalence rate of any demographic group in 1991 was that of Rochester men between the ages of 40 and 49 (717 cases per 100 000).
SURVIVAL
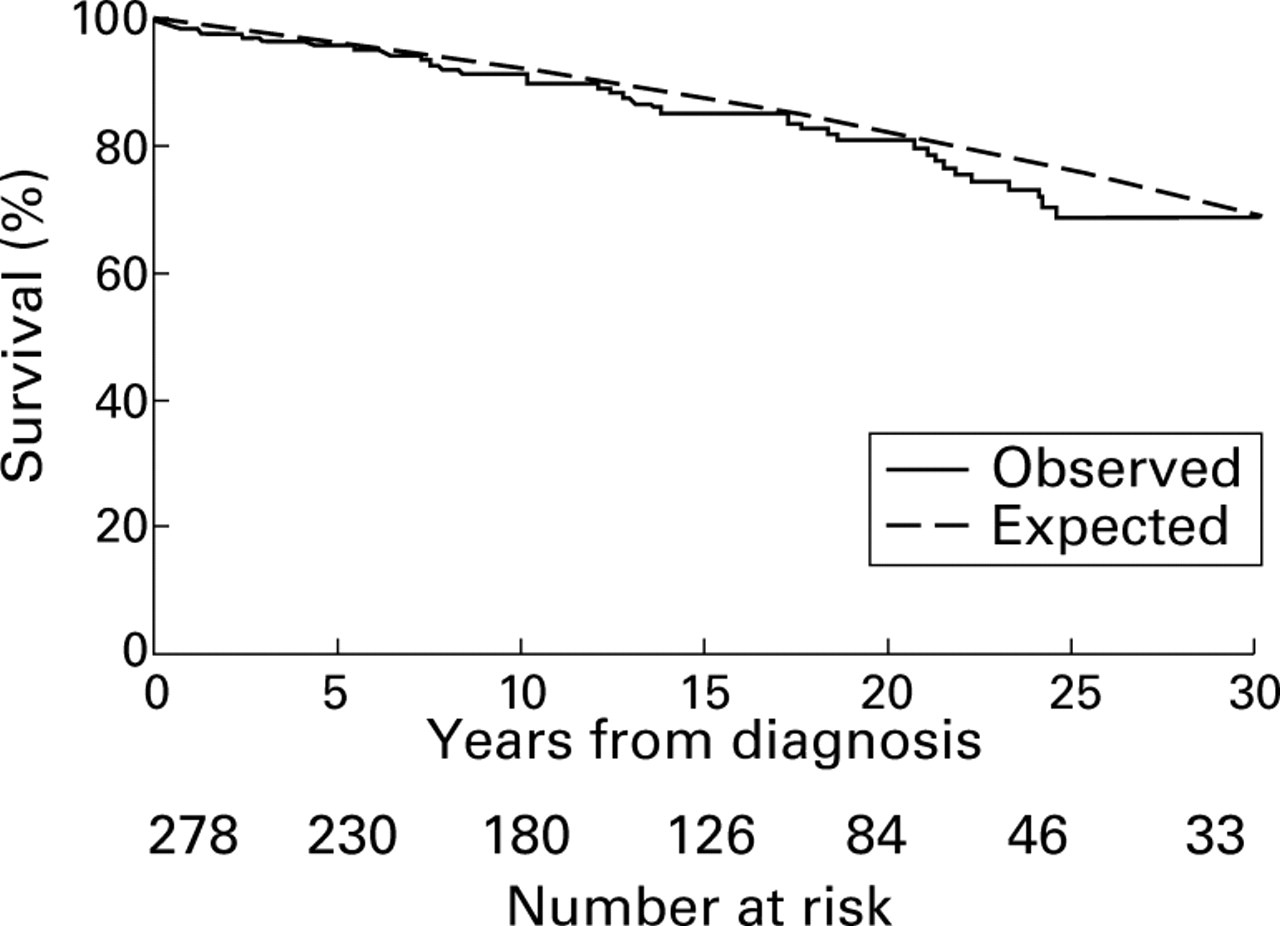
The inception cohort of ulcerative colitis patients (1940–93) was observed for a total of 4348 person years. The median duration of follow up was 14.1 years (range 0.1–51). Fifty two patients died (19%). Table 4 lists the causes of death. Overall survival was similar to that expected (p>0.2, log rank; fig 4). For example, 20 year survival was 81% (versus 83% expected), and 30 year survival was 69% (versus 69% expected). When stratified by sex, survival was significantly decreased in men with ulcerative colitis compared with that expected in age and sex matched men (p<0.03, log rank). In men, 20 year survival was 75% (versus 80% expected), and 30 year survival was 63% (versus 65% expected). However, when probable cases of colitis were excluded, these differences were not statistically significant (p>0.07). Actual survival in women was similar to that expected (p>0.5, log rank). In women, 20 year survival was 88% (versus 85% expected), and 30 year survival was 76% (versus 74% expected).
Causes of death in an inception cohort of patients with ulcerative colitis, Olmsted County, 1940–93

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall survival of ulcerative colitis inception cohort in Olmsted County, 1940–93 and expected survival of age and sex matched Minnesota whites in 1990 (p>0.2, log rank test).
A Cox proportional hazards regression model examined the association of age at diagnosis, sex, and calendar year of diagnosis with time to death. Male sex was associated with diminished survival (p<0.01). As expected, older age at diagnosis was associated with diminished survival (p=0.0001). Neither calendar year of diagnosis nor disease extent were associated with survival.
Discussion
The incidence of ulcerative colitis in Olmsted County, Minnesota, rose between 1940 and the 1970s and has stabilised at or slightly declined to a rate of roughly double that of the 1940s. The prevalence rate in the city of Rochester increased by 19% between 1980 and 1991. The incidence rate was significantly higher (almost threefold) in the city of Rochester than in rural Olmsted County, and the prevalence rate in 1991 was almost twice as high in Rochester as in the remainder of the county. The rise in incidence has been steeper in men than women. The distribution of age at diagnosis differs between the sexes. The overall survival of this inception cohort was similar to that expected for Minnesota whites of the same age and sex. Less than one fourth of all deaths could be attributed to ulcerative colitis or its complications.
The main strength of this study is that ascertainment of cases within a defined geographic region approached 100%. Complete medical records for all potential cases were available for review, and stringent but consistent diagnostic criteria were applied. Follow up to 1994 was available in 84% of the patients. Moreover, we were able to build on previous reports of ulcerative colitis in Olmsted County29-31 and extend the period of study to 54 years, allowing analysis of temporal trends in incidence and survival. Thus, the study provides true population based information on the incidence and prevalence of ulcerative colitis in a small region of the United States.
Our study had several limitations. Firstly, the small size of the geographic region restricted the study to a relatively small number of cases. However, even with the small number of cases, the differences in incidence rates by sex, county residence (urban versus rural), calendar year of diagnosis, and age of diagnosis were significant in a Poisson regression analysis. Secondly, only limited follow up was available for recent years (vital status after 1 January 1994 was unavailable in 16% of patients). The majority of patients lost to follow up seem to have moved out of the county. Mortality may have been underestimated, but only if patients lost to follow up were somehow at increased risk of death. Thirdly, the results of our study may not be generalisable to the United States as a whole, because of racial and ethnic differences. As of 1990, only 4% of the Olmsted County population was non-white, and a substantial portion of whites were of northern European heritage.
The adjusted incidence rate of ulcerative colitis in the last decade of our study (1984–93) was 8.0 cases per 100 000 person years, one of the highest reported rates in North America (table 5). Hiattet al reported a crude incidence rate of 10.9 cases per 100 000 person years among members of a northern California prepaid health plan33; however, it is not clear if this rate was standardised to the US population. One might expect members of such a plan to be younger than the general population, and therefore have a higher incidence of inflammatory bowel disease. When compared with crude rates obtained in 1991–93 under the auspices of the European collaborative study of inflammatory bowel disease (EC-IBD),5 the incidence rate in Olmsted County is similar to the mean rate. In contrast, the incidence rate of Crohn's disease in Olmsted County was high compared with most EC-IBD centres.5 39 The incidence rate of ulcerative colitis in the county was comparable to rates in EC-IBD centres in southern Europe, while the incidence of Crohn's disease was comparable to that in northern Europe.5 39 The incidence rate of ulcerative colitis in the present study may still be compatible with previous hospital based observations of a north-south gradient of inflammatory bowel disease within the United States.3 4
Comparison of ulcerative colitis incidence rates in North America
The increase in incidence of ulcerative colitis in Olmsted County between the 1940s and 1960s has been as precipitous as that seen in Crohn's disease.39 This stands in contrast to the experience at some centres with longitudinal incidence data, where the rise in ulcerative colitis incidence has been less pronounced or even absent.10 12 20 22 The two major modalities used to diagnose ulcerative colitis are barium radiography and endoscopy. Barium radiography of the gastrointestinal tract and proctoscopy were in widespread use in Olmsted County before the dramatic rise in incidence, whereas colonoscopy was introduced after the rise had taken place. Although the median interval between symptom onset and diagnosis shortened from 0.5 to 0.1 years between the first and fifth decades of the study, suggesting increased health care seeking and/or diagnostic awareness, we do not believe this can explain a twofold increase in incidence.
The distribution of age at diagnosis differed between the sexes, with a persistently higher incidence rate among men in the later decades of life (fig 1). This finding has been described in a number of recent epidemiological studies,7 8 13 15-17 19-22 most notably in the multicentre EC-IBD study.5 The present study also noted that the rise in incidence over time has been steeper among men than women. Indeed, male sex was independently associated with incidence in the Poisson regression analysis. Some5 7 9 11 13 15-19 21 22 but not all8 10 12 20 centres have reported that ulcerative colitis incidence is significantly higher in men. Interestingly, in the EC-IBD study, a male preponderance was seen in the southern centres only.5 It has been theorised that the sex divergence in age distribution and the male preponderance are because of the high prevalence of former cigarette smoking among older men,40but this theory has not yet been confirmed independently. Smoking status was not specifically addressed in the present study.
The incidence of ulcerative colitis in the city of Rochester was 146% higher than in rural Olmsted County, and the prevalence in 1991 was nearly twice as high. Urban residence was independently associated with increased incidence in the Poisson regression analysis. In our concurrent study of Crohn's disease, incidence in Rochester was 40% higher than in the rural areas of the county. Data on rural–urban differences in incidence of inflammatory bowel disease are sparse and conflicting.9 10 13 14 16 18 21 32 The prevalence of ulcerative colitis in urban areas of northern Alberta in 1981 was nearly twice as high as that in rural areas.32 Some of these differences may be related to increased health care seeking among urban residents, but the magnitude of the differences in the present study and the Albertan study suggests that environmental exposures may play a role in the expression of inflammatory bowel disease.
The adjusted prevalence of ulcerative colitis in 1991 (229 cases per 100 000 persons) is one of the highest reported in North America. If the results of the study are extrapolated to the United States white population of 1990 (approximately 209 million), there may have been as many as 479 000 patients with ulcerative colitis among US whites in the early 1990s, and each year another 16 000 patients are diagnosed. This calculation most likely underestimates all cases in the entire US population, as African-Americans, who numbered almost 31 million in the 1990 census, may have an incidence approaching that of US whites.33 The assumption of a similar prevalence rate among African-Americans would yield another 71 000 cases, for a total of 550 000 cases among US whites and African-Americans in the early 1990s.
If one assumes a stable incidence rate of eight cases per 100 000 person years and a median survival of 40 years after diagnosis (conservative estimate based on our survival curve), the prevalence in our county should eventually stabilise at roughly 320 cases per 100 000 persons, 40% higher than the prevalence in 1991. If this estimate is extrapolated to the projected US white population in 2005 (232 million), there may be as many as 742 000 cases of ulcerative colitis among US whites in the middle of the next decade. This projection does not include cases among African-Americans and other minority groups.
The normal life expectancy in members of our ulcerative colitis cohort is not surprising. Most recent population based studies have identified a nearly normal23-25 or even im- proved26overall survival in ulcerative colitis compared with that expected in the general population. Mortality directly related to ulcerative colitis (perforation, haemorrhage, ileus) seems to have decreased, as only one of five such deaths occurred after 1970. This might imply that inflammatory bowel disease related mortality may have decreased as medical and surgical treatments have improved. When the observed versus expected survival comparison was stratified by decade of diagnosis, there was no association between decade of diagnosis and decreased overall survival. More- over, formal analysis with the Cox proportional hazards regression model could not detect an association between survival and calendar year of diagnosis. When the log rank analysis was stratified by sex, decreased survival among men with ulcerative colitis compared with men in the general population was noted. However, when probable cases were excluded, this difference was not statistically significant. In the Cox model, male sex was associated with decreased survival. Although much of this decreased survival may be related to the decreased life expectancy seen in all men, it raises the possibility that the clinical behaviour of ulcerative colitis is more severe in men, or that men receive inadequate therapy for ulcerative colitis.
The finding of four deaths from gastrointestinal cancer, including three colorectal cancers and one cholangiocarcinoma, suggests that mortality from intestinal cancer may be increased. Although a previous study in Olmsted County detected a twofold increased risk of colorectal cancer in ulcerative colitis, it was not statistically significant.31 Other recent population based studies of the mortality of colorectal cancer relative to the general population have yielded conflicting results.23-26 Further study of the risk of gastrointestinal cancer in this cohort may be warranted.
Acknowledgments
This work was presented in part at the annual meeting of the American Gastroenterological Association, 11–14 May 1997, Washington, DC (Gastroenterology1997;112:A1027). Support was by Schering-Plough, grant number AR30582 from the National Institutes of Health, and Mayo Foundation for Medical Education and Research.
References
Footnotes
- Abbreviations used this paper:
- EC-IBD
- European collaborative study of inflammatory bowel disease