Article Text

Abstract
BACKGROUND AND AIMS To test the contribution of portal pressure gradient (PPG) and neurohumoral factors to sodium handling in cirrhotic patients without ascites, by comparing preascitic cirrhotic patients with patients with transjugular intrahepatic portosystemic stent shunt (TIPSS) and previous ascites.
PATIENTS Ten patients with TIPSS and 10 preascitic cirrhotic patients.
METHODS Changes in glomerular filtration, renal plasma flow, urinary sodium excretion (UNaV), and neurohumoral factors were measured before and for two hours after infusion of one litre of 0.9% saline over one hour.
RESULTS Glomerular filtration rate and renal plasma flow were significantly higher in patients with TIPSS compared with preascitic cirrhotic patients. Following saline infusion both parameters increased significantly; this increase was significantly greater in patients with TIPSS. UNaV increased significantly in both groups following saline infusion. The increase in UNaV was significantly greater in the TIPSS group. Plasma renin activity and angiotensin II decreased significantly in both groups. Basal UNaV was independently correlated with angiotensin II concentration and PPG and the change in UNaV correlated with the PPG.
CONCLUSIONS Results suggest that patients with advanced liver disease and low portal pressure handle sodium as well as patients with compensated liver disease and high portal pressure. These results are consistent with the notion that in addition to peripheral vasodilatation and severity of liver disease, the severity of portal hypertension contributes to the abnormalities of sodium retention in cirrhosis.
- cirrhosis
- transjugular intrahepatic portosystemic stent shunt
- TIPSS
- angiotensin
- sodium handling
- peripheral vasodilatation
Statistics from Altmetric.com
- cirrhosis
- transjugular intrahepatic portosystemic stent shunt
- TIPSS
- angiotensin
- sodium handling
- peripheral vasodilatation
Liver cirrhosis is characterised by hyperdynamic circulatory changes including high cardiac output and decreased peripheral vascular resistance.1-3 These changes worsen with disease progression.4 Compensatory activation of the renin–angiotensin,5-10 sympathetic,11-13and vasopressin14-17 systems contributes to the maintenance of vascular tone in these patients. The mechanism of retention of sodium in cirrhosis is unclear. Although several theories regarding the initiation of sodium retention in cirrhosis have been proposed,18 19 the most popular is the peripheral vasodilatation hypothesis which proposes that splanchnic hyperaemia and portal hypertension is the result of accumulation of splanchnic vasodilators because of reduced hepatic clearance and portosystemic shunting. This causes relative underfilling of the vascular compartment, which reduces effective arterial blood volume and stimulates release of neurohumoral factors in an attempt to restore vascular tone; retention of sodium and water returns the effective arterial blood volume to normal.20
Transjugular intrahepatic portosystemic stent shunt (TIPSS) successfully reduces portal pressure and is a useful treatment for ascites. Clearance of ascites occurs following TIPSS insertion despite advanced liver function. The improvement in ascites is thought to result from deactivation of the neurohumoral system with reduction in circulating renin, aldosterone, and angiotensin II (ANGII), and increased cardiac output.21-24 Expansion of the effective arterial blood volume with saline infusion in preascitic cirrhotic patients has shown abnormalities in renal circulation and tubular sodium handling before a decrease in the effective arterial blood volume. This abnormality is closely related to the severity of underlying liver disease.25 A confounding variable that these studies do not address is the role of concomitant portal hypertension; the relative contributions of increased portal pressure and the degree of liver dysfunction in producing defects of sodium handling in patients with liver disease are unclear.
Therefore, the aim of this study was to examine whether patients with severe liver disease and low portal pressure handle sodium as well as patients with mild liver disease and high portal pressure when subjected to acute saline loading. This study was performed in patients who were previously ascitic but had no ascites following insertion of TIPSS, and in patients who had early cirrhosis and established portal hypertension but no ascites. Changes in renal function and neurohumoral factors were determined in the basal state and also after acute saline loading.
Methods
SUBJECTS
Studies were undertaken with the approval of the local research ethics committee and in accordance with the Declaration of Helsinki (1989) of the World Medical Association and after obtaining written informed consent from each subject. Patients in both groups were included if they had biopsy proven cirrhosis. Patients with alcoholic liver disease abstained from alcohol for at least one month prior to the study. Patients were excluded if they had ascites (demonstrable on ultrasonography examination), pitting peripheral oedema, hepatic encephalopathy, clinically evident cardiovascular disease, renal dysfunction (decreased renal size on ultrasonography, proteinuria, or creatinine greater than 100 μmol/l), or were receiving any diuretics or vasoactive medications. Patients were maintained on a diet with restriction of sodium intake to 150 mmol per day for one week prior to the study.
Two groups of patients were studied (table 1). Group 1 (n=10) comprised stable, preascitic cirrhotic patients with established portal hypertension who had bled from oesophageal varices a mean of 4.5 (1.1) months previously and were managed by variceal band ligation. Group 2 (n=10) comprised patients who had undergone a TIPSS for bleeding from oesophageal varices and had ascites at the time of TIPSS insertion. They were included in the study if they had a portal pressure gradient of less than 12 mm Hg. Mean time from insertion of TIPSS to the study was 3.6 (1.4) months.
Patient characteristics
STUDY DESIGN
Patients were studied after an overnight fast between 8 am and 1 pm. Patients maintained a supine posture throughout the study, adopting the erect posture for voiding. Prior to the study, two venous cannulae were inserted, one in each arm (one for infusions and the other for sampling). Cardiovascular monitoring, which included measurement of blood pressure (Dynamap, Critikon, Australia) and pulse was performed at half hour intervals throughout the study. A primed, continuous infusion of 3H-inulin andp-aminohippuric acid (PAH) was started as indicated and continued throughout the study. After two hours of PAH and inulin infusion, one litre of 0.9% sodium chloride was infused over a one hour period. Figure 1 shows the timing of the infusions and various samples during the study.
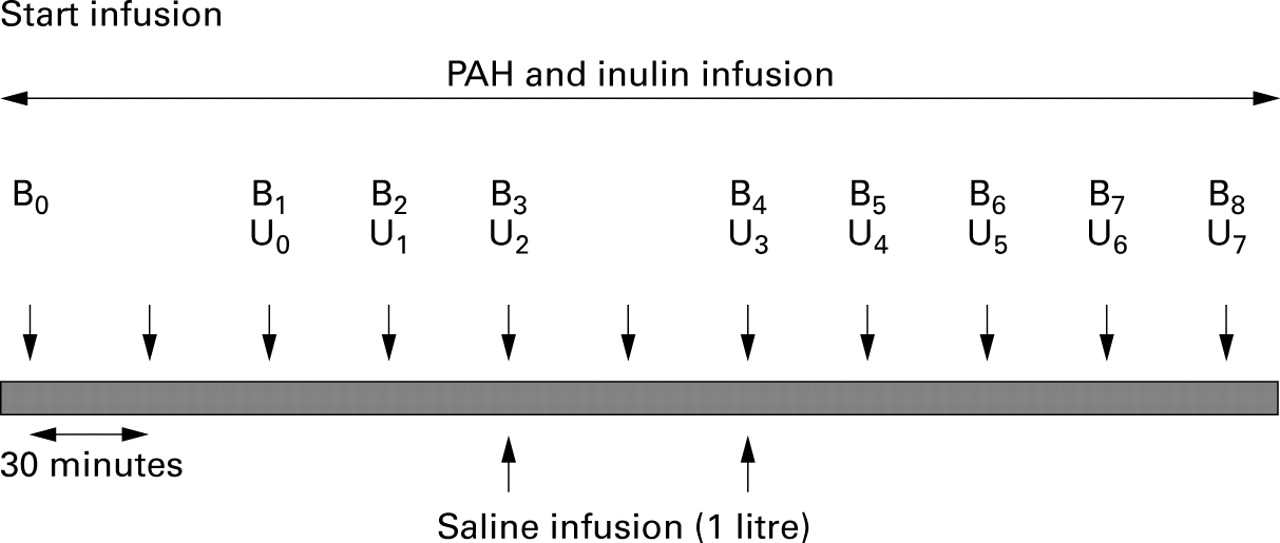
Study design. U1–U7, samples for urine volume, p-aminohippuric acid (PAH), inulin, sodium, and creatinine; B1–B7, blood samples for PAH, inulin, sodium, and creatinine; B3, B4 and B8, blood samples for plasma renin activity, angiotensin II, atrial natriuretic peptide, cyclic GMP, endothelin 1, and noradrenaline (norepinephrine). B0, B7, B3, B4, and B6, 250 ml water orally to ensure adequate urine flow.
MEASUREMENT OF PORTAL PRESSURE
In the TIPSS group, portal pressure gradient (portal pressure − inferior vena caval pressure) was determined the day after the study at routine portography. Hepatic venous pressure gradient (wedged hepatic venous pressure − inferior vena caval pressure) was measured in the patients in group 2 on the day after the study.
MEASUREMENTS
Blood (40 ml) was collected from a peripheral vein into precooled tubes. Plasma was separated and the samples stored at −70°C for analysis at a later date. Blood was also sampled from a peripheral vein in 10 healthy volunteers with a mean age of 49.6 (2.4) years (seven men and three women) for the measurement of neurohumoral factors.
Routine biochemistry
Plasma and urinary concentrations of sodium were measured using standard automated systems.
Measurement of glomerular filtration rate and estimated renal plasma flow
Glomerular filtration rate (GFR) and estimated renal plasma flow (ERPF) were determined during a constant infusion of3H-inulin (Amersham, International) and PAH (Merck, Sharpe and Dohme, Sydney, Australia) as described previously, and expressed per 1.73 m2 body surface area. Inulin concentration was measured using spectrophotometry, and PAH using high performance liquid chromatography.26
Measurement of plasma renin activity
The radioimmunoassay for measurement of plasma renin activity (PRA) was based on the principle that angiotensin I is generated by the action of renin on its substrate angiotensinogen. An in house antibody for angiotensin I was used. The coefficient of variation for the assay was 5.2%. The reference range for PRA was 1.6 (1.5) ng/ml/h.26
Measurement of angiotensin II
Samples of blood were obtained in ANGII inhibitor. ANGII values were measured by radioimmunoassay with an in house rabbit antibody R6B4. The coefficient of variation for the assay was 3.2%. The reference range for ANGII was 3.2 (1) fmol/ml.26
Measurement of atrial natriuretic peptide
The radioimmunoassay was performed using an antibody to human atrial natriuretic peptide (ANP) that had been raised in the rabbit following immunisations with human ANP. The coefficient of variation for the assay was 9.8%. The reference range for ANP was 62.1 (7.1) pg/ml.26
Measurement of cGMP
The dried samples were acetylated and plasma cGMP measured with an in house antibody (ED2–3). The coefficient of variation for the assay was 3.6%. The reference range of cGMP was 1.18 (0.34) nmol/l.26
Measurement of noradrenaline
Noradrenaline (NA; norepinephrine) was measured by an electrochemical method after separation by reverse phase high performance liquid chromatography. The coefficient of variation for the assay was 4.5%. The reference range of NA was 1.3 (0.34) pmol/ml.26
Measurement of endothelin 1
Following extraction using Bond Elut columns, endothelin 1 (ET-1) concentration was determined using a radioimmunoassay as described previously.27 The coefficient of variation for the assay was 5%. The reference range of ET-1 was 6.9 (1) fmol/l.
MEASUREMENT OF CARDIOVASCULAR HAEMODYNAMICS
On the morning of the study, haemodynamic parameters including heart rate, mean arterial pressure, stroke volume, and cardiac output were measured using a non-invasive bioimpedance method (BoMed NC-COM3, BoMed Medical manufacturer Ltd); the systemic vascular resistance and cardiac index were calculated using standard formulae.
CALCULATIONS
Using the inulin clearance as a marker of glomerular filtration rate (GFR), and PAH clearance as a marker of renal plasma flow, urinary sodium, and urinary volume, the following parameters were derived using the formulae as follows: urinary sodium excretion (UNaV, mmol/min): urinary sodium × urinary vol/min; filtered sodium load (FLNa, mmol/min): GFR × serum sodium; fractional excretion of sodium (FENa, %): (UNaV/FLNa) 100; sodium clearance (ClNa, ml/min): UNaV/plasma sodium.
DATA ANALYSIS
All results were expressed as mean (SEM). Repeated measures analysis of variance (ANOVA) was used to compare data within the same group and the unpaired t test was used to compare the difference between the two patient groups. Linear regression was used to test associations between renal, neurohumoral, and hepatic function parameters. Variables that reached statistical significance on the above analysis were entered into a multivariate analysis by stepwise logistic regression analysis.
Results
PATIENTS
The patients in both groups were well matched for age, sex, aetiology of liver disease, and duration since their first bleed. Patients in the TIPSS group had significantly more severe liver disease, manifested by lower albumin (p<0.001) and greater prothrombin time (<0.01), bilirubin (p<0.0001), and Pugh score (p<0.01). All the patients recruited into the study had normally functioning TIPSS and therefore a significantly lower portal pressure gradient (p<0.01). Mean arterial pressure and heart rate were not significantly different between the groups but the inferior vena caval pressure was significantly higher in the TIPSS group. Cardiac index was significantly higher (p<0.01) and the systemic vascular resistive index (p<0.01) was significantly lower in the TIPSS group. There was no significant change in heart rate or mean arterial pressure in either group following saline infusion.
RENAL HAEMODYNAMICS
Patients with TIPSS had significantly higher GFR (as measured by inulin clearance) and ERPF (as measured by PAH clearance) compared with preascitic cirrhotic patients (p<0.05). Following saline infusion both GFR and ERPF increased significantly (figs 2 and 3). Basal UNaV, FENa, and ClNa were similar in both groups but the filtered load of sodium was significantly greater in the TIPSS group. There was a significant increase in urinary sodium excretion (fig 4), fractional excretion of sodium, and sodium clearance in both patient groups. UNaV was significantly greater in patients in the TIPSS group, one hour after saline infusion.

Changes in glomerular filtration rate following saline infusion. *p<0.05 versus baseline; †p<0.05 between groups.

Changes in renal plasma flow following saline infusion. *p<0.05 versus baseline; **p<0.01 between groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in urinary sodium excretion following saline infusion. *p<0.05, **p<0.01 versus baseline; †p<0.03 between groups.
NEUROHUMORAL FACTORS
Table 2 summarises the changes in neurohumoral factors. PRA was significantly higher in both patient groups compared with healthy controls (p<0.05 for both groups). There was a significant reduction in PRA after acute saline loading in both groups (p<0.01). This reduction was not significantly different between groups. ANGII was significantly higher in the preascitic patients compared with healthy controls (p<0.05) and also compared with patients in the TIPSS group. There was no significant difference in ANGII between TIPSS patients and healthy volunteers. ANGII decreased significantly after saline infusion in both groups. ANP concentration was not significantly different between either group and healthy volunteers. There was no significant difference between the patient groups at baseline. There was a significantly greater increase in ANP after saline infusion in the TIPSS group. Cyclic GMP concentration was significantly higher in both patient groups compared with controls. There was no significant difference between groups and no significant change after saline infusion. Noradrenaline concentration was similar in both patient groups and controls and did not change significantly after saline infusion. ET-1 concentration was significantly higher in TIPSS groups compared with controls. ET-1 concentration was not significantly different between preascitic cirrhotic patients and healthy volunteers. ET-1 concentration was higher in patients in the TIPSS group but did not change significantly after saline infusion.
Changes in neurohumoral factors
RELATION BETWEEN VARIABLES
Basal UNaV correlated significantly with ANGII (r=−0.78, p<0.001), PRA (r=−0.6, p<0.001), and the portal pressure gradient (r=−0.6, p<0.001). Both ANGII and portal pressure gradient retained an independent relation with basal UNaV (r=−0.54, p<0.01; and r=−0.57, p<0.01 respectively). No significant correlation was detected between basal UNaV and noradrenaline, ANP, cGMP, ET-1 concentration, and Pugh score, albumin, bilirubin, or prothrombin time. No significant correlation was detected between the change in UNaV and the change in any of the measured neurohumoral factors. The change in UNaV correlated significantly with the portal pressure gradient (r=−0.55, p<0.01) on univariate analysis. No significant correlation was detected between GFR and ERPF, and any of the measured neurohumoral factors.
Discussion
Sodium retention is the cardinal manifestation of decompensated cirrhosis, but abnormalities in the handling of sodium are also evident in well compensated patients. Although there is a significant relation between abnormalities in sodium handling with severity of liver disease, the contribution of the severity of portal hypertension to this abnormality remains unknown.25 In this study, we have compared sodium handling following acute volume expansion by saline infusion in two groups of patients. Patients in group 1 had a significantly lower Pugh score and cardiac index, and significantly higher portal pressure and systemic vascular resistance compared with patients in group 2. Despite more advanced liver disease, patients in group 2 had significantly higher GFR and ERPF compared with group 1, although there was no significant difference in urinary sodium excretion. Following acute saline loading, GFR, ERPF, and sodium excretion improved significantly in both groups, suggesting that the improvement in UNaV following saline infusion is the result of an increase in renal blood flow and a reduction in renal vascular resistance (increased renal blood flow without any change in mean arterial pressure). Although we did not measure changes in systemic vascular resistance after saline infusion it is likely that the change in renal vascular resistance is caused by a reduction in systemic vascular resistance.28
Introduction of TIPSS in patients with refractory ascites reduces portal pressure and increases cardiac index, and urinary and fractional excretion of sodium. This improvement is caused by multiple factors related to expansion of the effective arterial blood volume and deactivation of vasopressor systems.21-24 In addition, the reduction in portal pressure gradient by the introduction of TIPSS may be envisaged to increase renal blood flow through the hepatorenal axis and therefore improve renal perfusion and sodium excretion. Langet al,29 in an animal model, showed an acute reduction in renal blood flow following infusion of glutamine into the portal vein. The effect of the infusion was to induce acute hepatocyte swelling and portal hypertension. This was abolished following section of the hepatic vagal fibres and renal denervation. They proposed the existence of a hepatorenal axis controlled by a reflex arc, the afferent limb of which was the hepatic vagal innervation and the efferent limb the renal sympathetic system. Stimulation of the sympathetic system produces an increase in renal vascular resistance, thereby reducing renal blood flow.30Acute increase in portal pressure produces a significant reduction in renal blood flow and an increase in renal resistance, suggesting the existence of a signalling mechanism between the liver and the kidney.31 The higher GFR and ERPF in the TIPSS group, observed in this study, may be the result of modulation of renal blood flow through the hepatorenal reflex. The significant correlation between the portal pressure gradient and UNaV, both in the basal state and with acute saline loading, confirms the existence of a hepatorenal axis.
Despite the absence of ascites, the PRA and ANGII concentrations were significantly higher in the preascitic cirrhotic patients compared with healthy volunteers; this is at variance with previous data and reflects the fact that the effective arterial blood volume in these patients was low.32 33 These differences may reflect different populations under study or a selection process. The mechanism of this activated basal renin–aldosterone–angiotensin system is not clear but may be caused by the following factors. As the preascitic cirrhotic patients in this study had established portal hypertension, the increased ANGII may reflect circulatory compensation. On the other hand, ANGII concentration was normal in patients with TIPSS, which argues for an expanded circulatory volume evidenced by significantly higher cardiac index. Studies in the isolated forearm to assess regulation of vascular tone in patients with preascitic cirrhosis has shown significant hyporesponsiveness to infusion of ANGII compared with controls.34 This observation suggests that ANGII hyporesponsiveness may be the stimulus for further activation of the renin–aldosterone–angiotensin system. The increase in UNaV with concomitant reduction in PRA and ANGII following saline infusion reflects deactivation of this system with volume expansion. Further evidence for the role of ANGII in mediating sodium handling is evident from a preliminary report suggesting an improvement in urinary sodium excretion following administration of the angiotensin I receptor blocker losartan. However, the action of this drug may be modulated through its effects on reduction of the portal pressure gradient.35
The increased concentration of ET-1 shown in this study is probably the result of excessive production rather than reduced clearance.36 37 It is most likely the result of injury to the sinusoidal cells, and the higher concentration observed in patients with more advanced liver disease is consistent with previous reports. The absence of any significant change in ET-1 concentration following volume expansion suggests that the reason for this excessive production is unlikely to result from the relative hypovolaemia of cirrhosis.38 39 Normal concentrations of noradrenaline at baseline and no significant change following volume expansion suggest that activation of the adrenergic system probably follows the development of ascites, and is consistent with the work of Wonget al who failed to show activation of the sympathetic system in preascitic cirrhosis and normal vascular responses to administration of noradrenaline in isolated forearm circulation.40 The significant increase in ANP following acute saline loading probably reflects the poorly compliant circulation following insertion of TIPSS and may have contributed in part to the enhanced urinary sodium excretion observed in the TIPSS group. cGMP measurements in this study are likely to reflect the activity of other unmeasured natriuretic factors and probably nitric oxide activity. cGMP concentration was increased in both patient groups as has been observed previously in cirrhosis. Administration of nitric oxide synthase inhibitors to cirrhotic rats was shown to improve both the haemodynamic state and also sodium handling.41-43 However, in this study the changes in renal sodium handling following acute saline loading did not seem to be related to changes in cGMP.
The results of this study suggest that the severity of portal hypertension is an important determinant of sodium retention in patients with cirrhosis and proposes the role of the hepatorenal reflex. It is likely that there are three concurrent factors which are responsible for the sodium retention of cirrhosis. Firstly, the deranged sodium handling observed in the two patient groups with activated neurohumoral systems is consistent with the original peripheral vasodilatation hypothesis which proposes the activation of vasopressor systems to counteract the effects of vasodilators on regional vascular beds as suggested by Schrier et al.20 Secondly, severity of liver disease is an important determinant of sodium homoeostasis in cirrhosis.25 Finally, this study highlighted the role of portal pressure. The chronology of these derangements and the role of intrarenal factors in producing sodium retention of cirrhosis and ascites remains to be defined and requires longitudinal studies in patients with cirrhosis.
Acknowledgments
We gratefully acknowledge the help of Sister G Wilkie for help with the study and Mr N Johnstone for assays of the neurohumoral factors. This study was presented in an abstract form at the meeting of the American Association for Study of Liver Diseases in Chicago, 1998 (Jalan R, Hayes PC. Renal and neurohumoral response to saline loading in pre-ascitic cirrhotics and in ascitic patients with TIPSS.Hepatology1998;28:555A).
References
Footnotes
- Abbreviations used in this paper:
- ANGII
- angiotensin II
- ANP
- atrial natriuretic peptide
- cGMP
- cyclic guanosine monophosphate
- ClNa
- sodium clearance
- ET-1
- endothelin 1
- FENa
- fractional excretion of sodium
- FLNa
- filtered load of sodium
- GFR
- glomerular filtration rate
- NA
- noradrenaline (norepinephrine)
- PAH
- p-aminohippuric acid
- PPG
- portal pressure gradient
- PRA
- plasma renin activity
- RPF
- renal plasma flow
- TIPSS
- transjugular intrahepatic portosystemic stent shunt
- UNaV
- urinary sodium excretion