Article Text

Abstract
BACKGROUND Cancer of the ampulla of Vater kills 60% of affected patients. Local spread of the tumour (T stage) is the only reliable prognostic factor. Nevertheless, any cancer stage includes long term survivors and patients dying from the disease. The molecular anomalies involved in this process have the potential to serve as additional prognostic markers.
AIM To evaluate if allelic losses (LOH) of chromosomes 17p and 18q may be of prognostic value in multivariate survival analysis.
METHODS We examined 53 ampullary cancers for chromosome 17p and 18q LOH using microsatellite markers and DNA from paraffin embedded tumours. All patients were treated by surgery alone (pancreaticoduodenectomy). Multivariate survival analysis included age, sex, tumour size, macroscopic appearance, grade of differentiation, T stage, lymph node metastasis, and chromosome 17p and 18q status.
RESULTS Chromosome 17p and 18q LOH were detected in 28 (53%) and 18 (34%) cancers, respectively. Multivariate survival analysis indicated chromosome 17p status as an independent prognostic factor together with T stage. The five year survival for chromosome 17p retention and 17p loss was 80% and 7%, respectively. The risk of death from cancer within the five year follow up period for patients with cancers harbouring chromosome 17p LOH was 11 times higher than that of patients with cancers retaining chromosome 17p (p<0.0001), regardless of the tumour stage at diagnosis.
CONCLUSIONS Chromosome 17p status is an independent prognostic factor among ampullary cancers at the same stage. The combined use of T stage and chromosome 17p status may help in deciding whether ampullary cancer patients require additional therapy other than surgery alone.
- ampulla of Vater
- cancer
- loss of heterozygosity
- microsatellites
- allelotyping
- microsatellite instability
Statistics from Altmetric.com
Patients with cancer of the ampulla of Vater account for up to 36% of those undergoing surgery for pancreaticoduodenal malignancies and are the only patients among those affected by cancers of biliopancreatic origin who have up to a 50% chance of being cured by surgery alone.1-8 There is general agreement that local spread of the tumour (T stage) is the only significant and independent prognostic factor for this cancer whereas the predictive value of tumour grade and lymph node metastases is controversial.1-8 Nevertheless, as any cancer stage includes both long term survivors and patients dying from the disease, the decision of whether therapy for ampullary cancer patients should be limited to surgery or include adjuvant therapies is subjective. There is undoubtedly a need for additional prognostic markers, and the molecular anomalies involved in this process6 9-12 have the potential to serve such a purpose.
As part of our continuing efforts designed to clarify the molecular pathogenesis of cancers of the ampulla of Vater, we have performed a genome wide survey of allelic losses (LOH) on a limited number of cases for which DNA extracted from frozen tissues was available using site specific microsatellite markers on each chromosome.13 14Microsatellites are short repeat DNA sequences located throughout the genome15 which may be readily assayed by polymerase chain reaction (PCR) amplification and gel electrophoresis.13 14 The two allelic forms of the microsatellites in normal cells, one inherited from each parent, migrate on gel electrophoresis as two bands of nearly equal intensity but different sizes. Loss of a chromosome in tumour tissue causes loss of one of the two PCR products (see fig 1). During these studies we noticed that allelic losses of the short arm (p) of chromosome 17 and of the long arm (q) of chromosome 18, at sites including or closely linked to p53 andDCC/DPC4 (deleted in colon cancer/deleted in pancreatic cancer) genes, respectively, seemed to be associated with advanced stage cancers and poor outcome. This observation prompted us to evaluate if these chromosomal anomalies might be of prognostic value in a larger series of patients for which only archival formalin fixed, paraffin embedded samples were available.
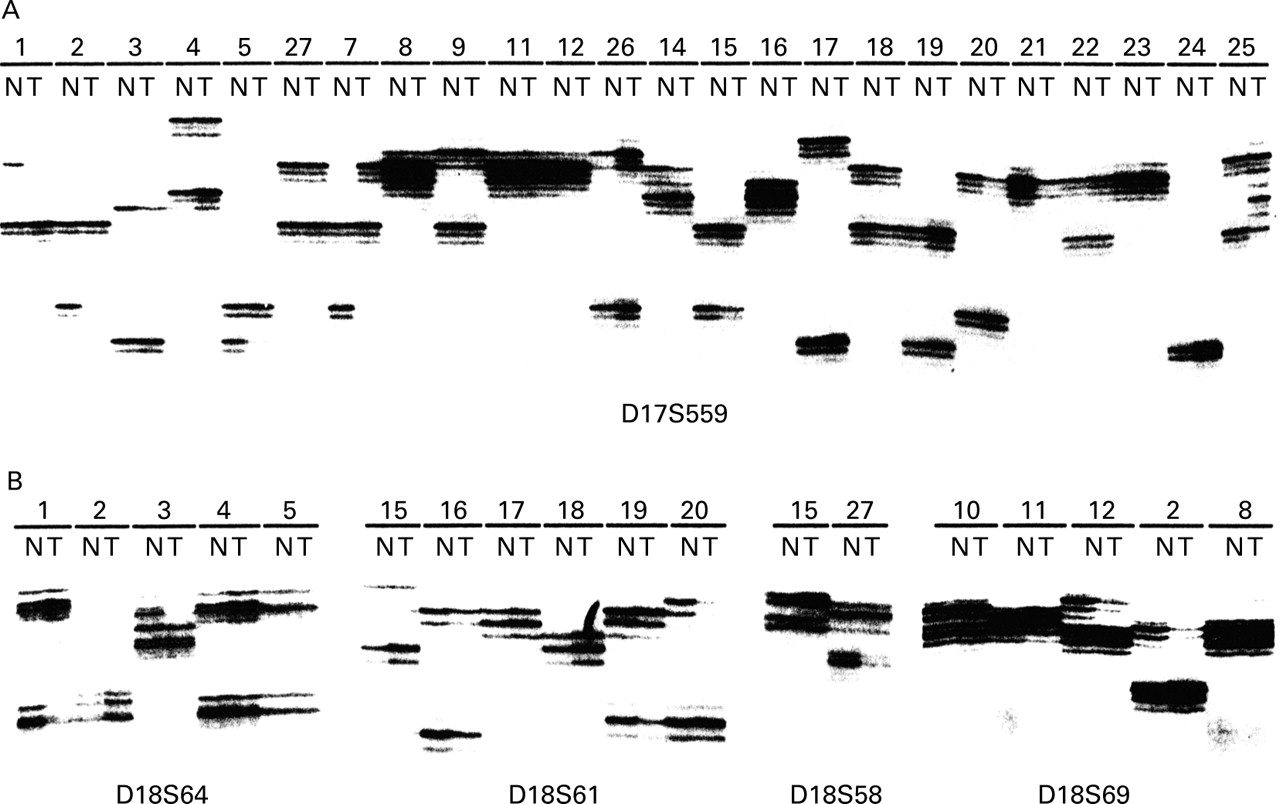
(A) Analysis of polymerase chain reaction (PCR) amplified microsatellite locus D17S559, localised at chromosome 17p13, using high molecular weight DNA from frozen tissues. Case numbers are indicated at the top of each lane and correspond to those of table 1. T, tumour; N, matched normal tissue DNA. The upper allele is lost in cancers 1, 3, 14, and 20 whereas loss of the lower allele is evident in cancers 2, 5, and 15. Case Nos 4, 27, 9, 26, 17, 18, 19, and 22 show no losses. Case Nos 8, 11, 12, 16, 21, 23, and 24 were considered as non-informative. Cancers 7 and 25 are good examples of the possible findings in replication error (RER) positive neoplasms, showing the disappearance of one allele with the appearance of a new one, the presence of additional longer or shorter fragments, or a combination of these phenomena. Case Nos 9, 11, and 21 are three adenomas, two of which have been described previously.9 11 (B) Analysis of PCR amplified microsatellite loci of chromosome 18q, using DNA from formalin fixed, paraffin embedded tissues. Microsatellite loci are indicated at the bottom of each panel. Allelic losses occurred in cancers 1, 3, 19, 20, 27, 12, and 2. Case No 15 is an example of allelic imbalance due to the increased intensity of one allele in the absence of a decrease in intensity of the other. This case was considered as not having allelic loss as such a pattern may well be attributable to partial or total chromosomal gains (for example trisomies). Case No 11 is a previously described adenoma.9
Materials and methods
SELECTION OF CASES
Fifty three cancers of the ampulla of Vater, observed at the Verona University Hospital (Italy) between 1986–1994, were selected by applying the following criteria: (a) unequivocal establishment of their origin from the anatomical structures forming the ampulla of Vater6 9-11; (b) treatment of patients with curative intent by surgery alone, consisting of pancreaticoduodenectomy; (c) availability of follow up through direct contact at least once a year with the patient or his/her physician.
PATIENTS AND TUMOURS
The clinicopathological characteristics of the 53 cases are reported in table 1. The patients comprised 37 males (70%) and 16 females (30%), with a mean age of 57 years (range 33–73). The tumour stage was based on pathological and clinical evaluation, which included preoperative radiography, computed tomography, and abdominal exploration at laparotomy. The staging system used was that of Yamaguchi and Enjoji16: T stage I, tumour restricted to within the muscle of Oddi; T stage II, infiltration of duodenal submucosa; T stage III, involvement of duodenal muscularis propria; T stage IV, infiltration of periduodenal fat and pancreas; N, nodal metastases; and M, blood borne metastases. All but three cancers (two colloid and one small cell carcinoma) were graded according to Achille and colleagues.6 Three cancers were well (6%), 21 moderately (42%), and 26 poorly (52%) differentiated. The average number of lymph nodes isolated from the surgical specimens was 11 (range 5–32) and nodal metastases were present in 23 (43%) cancers.
Clinicopathological data and results of genotypic studies according to disease stage and outcome at follow up
TISSUE AND DNA PREPARATION
Thick tissue sections (6 μm) from formalin fixed, paraffin embedded surgical specimens were stained with haematoxylin and dried without a cover glass. They were soaked for five minutes in TE (10 mM Tris HCl, pH 8.0, 1 mM EDTA) containing 1% glycerol. Regions containing at least 70% cancer cells and matched normal mucosa were microdissected using a 27 gauge sterile needle and collected in 20 μl of TE, 1% Tween 20, and 200 μg/ml proteinase K. Samples were incubated overnight at 37°C. After boiling for 10 minutes, 4 μl aliquots were used for PCR amplification.
LOSS OF HETEROZYGOSITY AT 17p AND 18q CHROMOSOMAL ARMS
Twenty one previously reported cases,6 for which high quality DNA from frozen tissue was available, were analysed and compared with results obtained with the partially degraded DNA extracted from paraffin sections of the same cases. As the results correlated totally, we extended the study to the additional 32 cases for which only paraffin embedded tissue was available.
Allelic losses at chromosomes 17p and 18q were examined by PCR amplification of matched normal and cancer DNAs using four microsatellite markers for each chromosome: D17S513, D17S1176, D17S525, and D17S559 for chromosome 17p13, and microsatellites D18S61, D18S58, D18S64, and D18S69 for chromosome 18q21. All primers were from the MapPairs collection (Research Genetics, Huntsville, Alabama, USA). All cases were tested for D17S559, D17S1176, D18S69, and D18S64. Non-informative and negative scoring cases were subsequently tested for D17S513, D17S525, D18S61, and D18S58. The PCR reactions (10 μl) were performed as previously described,11 14 with modification for DNA from paraffin embedded tissues consisting of addition of five extra PCR cycles and an annealing temperature 5°C lower than that indicated by the primers' manufacturer. The radioactively labelled PCR products were analysed by polyacrylamide gel electrophoresis.14
Allelic losses were determined as previously detailed.14Briefly, LOH was scored only when there was loss or diminished intensity of at least 60% of the bands representing one allele in the tumour sample with respect to the matched allele from normal tissue. Tumours yielding PCR products of abnormal sizes with four or more microsatellite markers were considered to belong to the replication error (RER) subclass.6 17-20
MUTATION OF THE p53 GENE
The 21 cases for which DNA from frozen tissues was available had been previously characterised for p53mutations by PCR-single strand conformational polymorphism and direct DNA sequencing.6 9 11 However, these methods are difficult to apply to the partially degraded DNA from paraffin embedded tissues. Therefore, we used immunocytochemistry with pAb1801 and DO7 anti-p53 monoclonal antibodies to assess the p53 mutational status in the 32 additional cases for which only paraffin embedded tissue was available. The rationale for this is that mutant proteins show a prolonged half life and it has been demonstrated that detection of p53 protein accumulation in cell nuclei serves as a surrogate for detection of p53 gene mutations in gastrointestinal cancers.9 21 In particular, it recognises about 80% ofp53 gene mutated ampullary cancers.6 9 11 Specifically, when the threshold for positivity is set to staining over 30% of cancer cells, all cases showing immunohistochemical positivity had a mutation confirmed by direct sequencing.6 9 11 However, it should be recognised that false negative results occur in up to 20% of cases (see table 1, column p53 IHC).
FOLLOW UP AND STATISTICAL ANALYSIS
The primary statistical outcome in this study was overall survival measured from the date of surgery. Death from cancer was the end point. No case was lost at follow up, which was updated to May 1998. Overall survival distribution was calculated by the product-limit method and analysed using the Mantel-Cox test.22 Multivariate survival analysis was performed using the Cox's proportional-hazard model.23 To select the more stringent model, we used a backward elimination procedure, including all conventional factors (age, sex, macroscopic features, size, grade, stage, and nodal metastases), p53 mutation status, and chromosome 17p and 18q LOH status. The final model included only the factors consistently retaining significant p (<0.05) values. BMDP (BMDP Inc., Los Angeles, California, USA) and SPSS (SPSS Inc., Chicago, Illinois, USA) statistical programs were used.
Results
At diagnosis, 35 (66%) cancers had extraduodenal local invasion (T stage IV) or nodal metastases, and 18 (34%) were confined to the duodenal wall (T stages II and III) (see table 1). Twenty one of the 53 patients (40%) were alive and well after a period ranging from 48 to 203 months, including 11 whose cancer was confined to the duodenal wall and 10 with advanced stage disease. All of the remaining 32 patients, suffering from either low or advanced stage cancers, died after a median period of 20 months (mean 18 months; range 4–74) following surgery.
LOSS OF HETEROZYGOSITY ANALYSIS
The results of the molecular study are summarised in table 1 and a representative analysis is shown in fig 1 where examples of interpretation are also detailed.
Chromosome 17p and 18q LOH were detected in 28 (53%) and 18 (34%) cancers, respectively. In 15 of these cases both allelic losses coexisted, and this association correlated with the cancer stage; it was found in 17% (3/18) low stage and in 34% (12/35) advanced stage cancers. The majority of patients whose cancer harboured chromosome 17p LOH (11/13) or 18q LOH (2/3) alone died from the disease. All 15 patients whose cancer showed coexistent chromosome 17p and 18q allelic losses died.
Eight tumours showed microsatellite instability (fig 1) in 4–6 of the eight loci analysed and were classified as RER positive.6The analysis of informative microsatellites not showing instability demonstrated that four of the eight RER positive ampullary tumours (AT7, AT23, AT26, ATp33) had retained both chromosome 17p alleles and four cases had retained both chromosome 18q copies (AT23, AT26, AT28, ATp35) (table 2). The five cases for which high molecular weight DNA was available were assessed for allelic losses at chromosome 17p by Southern blot analysis using the pYZ22 probe and MspI digestion. Only one case was informative (AT23) and the absence of 17p loss was confirmed in this case (data not shown). Finally, ATp35 showed no allelic loss by single strand conformation polymorphism analysis of the exon 6 polymorphic sequence of the p53 gene (codon 213, CGG, or CGA)9 11 (data not shown). No additional case was informative for the twop53 polymorphisms in intron 7 (C to T and T to G at 71 bp and 91 bp downstream of exon 7, respectively). In summary, we demonstrated that no chromosome 17p and 18q losses were found in five and four of the eight RER positive cases, respectively. Based on these results, and in accordance with Jen and colleagues,13 carcinomas of the RER type were included among the tumours with no loss of chromosomes 17p and 18q in the survival statistical analysis.
Detailed results of microsatellite markers analysis in the eight RER positive cancers
p53 IMMUNOHISTOCHEMISTRY
Abnormal accumulation of p53 protein was found in 25 cancers (47%), all showing immunostaining in the majority of cancer cell nuclei and therefore suggestive of p53 gene mutation (see materials and methods and table 1). There was no difference in the proportion of p53 mutated cases between cancers confined to the duodenal wall (8/18, 44% of T stages II–III cases) and advanced stage diseases (17/35, 48% of T stage IV or N+ cases) (p=0.17). Sixteen of the 25 cancers showingp53 mutations, as assessed by immunostaining, had complete loss of p53 function due to the concomitant loss of the normal p53 allele on chromosome 17p. All of these 16 cancers caused the death of the patients, including two of 18 with early stage disease and 14 of 35 with advanced disease.
SURVIVAL ANALYSIS
The results of multivariate analysis are summarised in tables 3and 4 and Kaplan-Meier survival curves are shown in fig 2. We first performed multivariate analysis using Cox's multiple regression model with inclusion of all conventional factors (age, sex, tumour size, macroscopic features, grade of differentiation, and lymph node metastasis), p53 mutation, and chromosome 17p and 18q LOH status. In this analysis we included the RER positive cancers among those retaining both copies of chromosomes 17p and 18q (table 3). Only T stage and 17p status emerged as independent prognostic factors. The estimated risk of death from cancer within the five year follow up period for patients with extraduodenal local extension of disease (T stage IV) was 4.78 times higher than that of patients with their disease confined to the duodenal wall (T stages II–III) (95% CI 2.20–10.38; p<0.0001). The relative risk of death for patients with cancers showing chromosome 17p LOH was 11.3 times higher than that of patients with cancers retaining chromosome 17p (95% CI 4.24–30.11; p<0.0001). The median actuarial survival time was 16 months (95% CI 13–19) for T stage IV and over 74 months for T stages II–III cases. The median actuarial survival time was 20 months (95% CI 14–26) and 19 months (95% CI 13–25) for cases with chromosome 17p and chromosome 18q allelic loss, respectively, whereas it was not measurable for cases retaining both copies of each of chromosome 17p or 18q.
Multivariate statistical analysis (Cox's model)
Multivariate statistical analysis (Cox's model) excluding eight RER positive patients (45 patients)

Survival curves obtained by the product-limit method. Better survival was associated with no loss of chromosome 17p (p<0.0001) or 18q (p<0.0001) (A, B) and T stages II–III compared with stage IV (p<0.0001) (C). (D) Overall survival of patients according to both T stage and chromosome 17p status. Numbers in parentheses indicate the number of subjects at risk at different time intervals. Vertical lines indicate 95% confidence intervals.
Both multivariate and univariate analysis showed no significant difference between survivors and non-survivors for age, sex, tumour size, macroscopic features, grade of differentiation, lymph node metastasis, or p53 gene mutations.
Exclusion of the eight RER positive cancers from the multivariate survival analysis did not alter the general results or the prognostic significance of chromosome 17p loss (table 4).
Discussion
Ampullary cancers are usually diagnosed when the tumour mass reaches about 2.5 cm in diameter.7 16 However, despite having a comparable tumour mass, they include neoplasms at different stages of evolution and with different levels of biological aggressiveness, which might be described by the associated genetic abnormalities. A schematic representation of the molecular pathogenesis of ampullary cancer is depicted in fig 3 which is based on the present data and on our previous published work with Ki-ras, p53, and adenomatous polyposis coli (APC) gene mutations, chromosome 5 allelic losses, and identification of a subset of ampullary cancers with widespread genomic alterations of the type seen in replication error phenotype (RER+) gastrointestinal cancers and good prognosis.6 9-12

{kind=link}
{kind=link}
{kind=link}
Molecular pathogenesis and prognosis of cancers of the ampulla of Vater. Ampulla of Vater cancers have similar molecular pathogenetic pathways as gastric and colorectal cancers. The majority of cases (85%) show frequent chromosomal changes (CIN, chromosomal instability), while a subgroup (15%) shows subtle widespread DNA alterations (MIN, microsatellite instability). In CIN type ampullary cancers, the early genetic events include mutation of the adenomatous polyposis coli (APC) and Ki-ras genes in 17% and 37% of cases, respectively, together with chromosome 5q loss (50%).9-12 Mutation of the p53 gene occurs in about 50% of cases at the time of adenoma-carcinoma transition.6 9 11 Allelic losses at chromosomes 17p (51%) and 18q (33%) are associated with progression of malignancy. MIN type ampullary cancers rarely show chromosomal losses. The two molecular pathways identify different prognostic categories. MIN ampullary cancers have a low aggressive potential,6similar to that of CIN cancers, retaining both copies of chromosome 17p. Chromosome 17p loss is associated with a high risk of death from cancer within two years following surgery.
Our study demonstrates that the allelic loss of chromosome 17p is an important prognostic marker in patients with cancer of the ampulla of Vater. The subgroup of patients whose tumour had retained both alleles of chromosome 17p (44% of patients) had a very good outcome (five year survival of 80%) whereas survival in patients whose tumour had lost one allele of chromosome 17p was poor (five year survival of 7%). The estimated risk of death from cancer within the five year follow up period for patients with cancers showing chromosome 17p loss was 11 times higher than that for patients with cancers retaining both alleles. Univariate statistics suggested that chromosome 18q status was also a prognostic indicator. However, multivariate survival analysis showed that its content of information was lower than that of chromosome 17p status.
Mutation of the p53 gene, as assessed by immunohistochemical analysis, was not useful for determining prognosis in our series. Fourteen patients, who all died of disease, showed complete inactivation of p53 function by mutation of one allele and deletion of the chromosomal 17p locus containing the other. Inactivating mutation of one p53 allele is likely to occur at the time of the adenoma-carcinoma transition in ampullary cancers6 9 whereas loss of the remaining normalp53 allele on chromosome 17p is associated with advanced stage cancers. It is likely that the prognostic information of 17p LOH resides in the identification of cancers with complete loss of p53 function—that is, of its gatekeeper function for cell proliferation.24
Our data suggest that chromosome 18q loss occurs at a later stage than chromosome 17p loss in ampullary cancers. This chromosomal loss is a frequent finding in duodenal, colorectal, and pancreatic cancer.13 25-27 More than one candidate gene for this loss resides on 18q. DPC4 has been suggested as a main target in pancreatic cancer.27 28 In colon cancer either DCC,DPC4, and/or MAD(mothers against decapentaplegic) related 2 gene have been suggested to be the targets of deletion (see Martinez-Lopez and colleagues26). There is no information as yet on the candidate gene on chromosome 18q in ampullary cancer.
In addition to the status of chromosome 17p, only the T stage—that is, the local invasiveness of the tumour—had an independent prognostic value among the conventional factors considered here. The estimated risk of death from cancer within the five year follow up period for extraduodenal diseases (T stage IV) was almost five times higher than that for cancers confined to the duodenal wall (T stages II–III). Our finding that local invasion describes the clinical aggressiveness of ampullary cancers better than any other conventional factor is in line with five other studies.1-4 6 Previous studies suggesting a prognostic value for lymph node metastases used either univariate statistics alone or evaluated only the size and not the local aggressiveness of the tumour (T stage).3 7 29 The use of cancer grading as an additional prognostic factor has led to inconsistent results1-4 6 7 which may be attributed to both lack of clear cut criteria and the subjectivity involved in the definition of grading categories.
The clinical importance of the assessment of both T stage and chromosome 17p status in cancers of the ampulla of Vater resides in the capacity of the latter to discriminate between patients with good and poor prognosis within the same stage. Patients with the disease confined to the duodenal wall (T stages II–III) and retention of both chromosome 17p alleles had a much better outcome (100% five year survival) than those with chromosome 17p allelic loss (18% five year survival). Similarly, patients with extraduodenal cancers (T stage IV) retaining chromosome 17p alleles had a five year survival of 60% whereas none of those with chromosome 17p allelic loss survived the second year following surgery.
Eight tumours in the present series were classified as RER positive as they showed widespread microsatellite instability and were associated with an excellent five year survival as those early stage cancers retaining chromosome 17p (100%). This finding confirms and extends our previous report on the good prognosis associated with RER positive tumours.6 It is difficult to assess the chromosomal losses in RER positive tumours. However, we demonstrated that both copies of chromosomes 17p and 18q were retained in five and four of the eight RER positive cases, respectively. Other studies have shown that gastrointestinal RER positive tumours, including gastric, duodenal, and colorectal cancers rarely have chromosomal losses.13 18 19 25 It is tempting to speculate that the better outcome in patients with RER positive tumours is a result of retention of both chromosome 17p and 18q alleles. At any rate, exclusion of these eight RER positive cancers from the univariate and multivariate analysis did not alter the results of survival analysis, including the prognostic significance of chromosome 17p loss.
In conclusion, allelic losses at chromosomes 17p and 18q are frequent alterations involved in ampullary cancers and are associated with shortened patient survival. Chromosome 17p status is useful in predicting prognosis among cancers at the same stage. The combined use of T stage and chromosome 17p status may be useful in deciding whether or not ampullary cancer patients may require therapy in addition to surgery.
Acknowledgments
This study was supported by grants from Associazione Italiana Ricerca sul Cancro (AIRC), Milan, Italy; Consorzio per gli Studi Universitari, Verona, Italy; Banca Popolare di Verona, Italy; by a co-financed grant from Verona University and Ministero Università e Ricerca Scientifica e Tecnologica (MURST), Rome, Italy; and European Community grant Biomed-2 CE-Contract No BMH4-CT98–3805.
Footnotes
- Abbreviations used in this paper:
- LOH
- loss of heterozygosity
- PCR
- polymerase chain reaction
- RER
- replication error