Article Text

Abstract
BACKGROUND AND AIMS The subtype and species related heterogeneity of β adrenoceptors prompted a functional reappraisal of these molecular targets of motility inhibition in the human colon.
METHODS Relaxation of muscle strips was measured in vitro.
RESULTS The following agonists had decreasing relaxing potency (effective concentration range 10−8–10−4 mol/l): (−)isoprenaline (non-selective), terbutaline (β2 selective), CGP 12177 (β3 selective, also β1, β2antagonist), and SR 58611A (β3 selective). Isoprenaline and terbutaline were more potent on circular than taenia strips; CGP 12177 and SR 58611A weakly and partially relaxed taenia but had little effect on circular strips. The potency of isoprenaline on circular strips was greatly reduced by the β1 selective antagonist CGP 20712 (10−7 mol/l), and less so by ICI 118551 (10−7 mol/l, β2 selective). CGP 20712 and ICI 118551 together (both 3×10-6 mol/l) had no effect on taenia relaxation by SR 58611A and rendered isoprenaline and terbutaline virtually inactive on circular strips, although not on taenia, which was relaxed at higher than control concentrations and maximally by isoprenaline. Propranolol, a β1, β2 non-selective antagonist, at high concentrations (10-5 mol/l) prevented taenia relaxation by CGP 12177 and SR 58611A; its quantitative antagonism of isoprenaline (in common with that of CGP 12177 used as an antagonist) was competitive in circular strips but not on taenia.
CONCLUSIONS β1, β2, and β3 adrenoceptors are functionally detectable in the human colon; agonist stimulation of any one type relaxed taenia but only isoprenaline was fully effective at the β3 subtype.
- β adrenoceptor subtypes
- human colon
- smooth muscle
- taenia coli
Abbreviations used in this paper
- IC50
- concentration producing 50% maximal response
Statistics from Altmetric.com
As early as 1892 secretions from the adrenals were reported to reduce the motility and tone of the gastrointestinal tract of dogs.1 This may in fact have suggested the pharmacological control of gut motor function through local adrenergic mechanisms. Ample animal and clinical evidence have shown that these play a primary inhibitory role in non-sphincteric smooth muscle contractions throughout the digestive system.2 ,3
More recent developments, such as the breakthrough discovery of α and β adrenoceptors4 and the latter's first two subtypes5 promptly resulted in life saving cardiovascular drugs (β blockers) and the widely appreciated agents for the management of obstructive lung disease (β2 selective adrenoceptor agonists). However, the major therapeutic advances resulting from our growing understanding of the fundamental aspects of adrenergic pharmacology have to date not been applicable to gastroenterology.
Observations in healthy humans and patients suffering from various gastrointestinal conditions suggest the potential of sympathomimetic and adrenergic blocking agents for therapeutic control of intestinal motility,6-11 but involvement of the sympathetic nervous system in homeostatic regulation of so many functions is a serious drawback for achieving selectivity. As an example, clinically acknowledged abnormally enhanced rectosigmoid motility reportedly improves after pharmacological β adrenoceptor stimulation but even the best tolerated β2 selective agonists have not proved adequate for standard treatment because of their significant cardiovascular effects.9
The recent undisputed recognition of a third β adrenoceptor subtype, β3,12 whose abundance and functional relevance in the intestine has been established in animal studies,3 raises fresh hopes and clinical interest in the adrenergic modulation of bowel movement.
In the light of growing awareness of substantial species related differences in the β3 adrenoceptor,3 ,12 we performed a series of in vitro tests, rating the mechanical responses of human colonic smooth muscle, with a view to functionally reassessing the β adrenoceptor subtypes therein.
Materials and methods
This study was approved by the ethics committee of the San Raffaele Hospital, Milan.
TISSUE PREPARATION
Specimens of human transverse or distal colon were obtained from patients (15 males and 11 females, aged 56–77 years) undergoing surgery for colonic cancer (80% rectum, 20% transverse) at the San Raffaele Hospital, Milan. Patients did not receive radiotherapy and had not been treated chronically with steroids or chemotherapeutic agents. However, two were receiving antihypertensive therapy with enalapril, one a calcium antagonist, and two the histamine H2 receptor antagonist ranitidine. Their otherwise uncontrolled medication history, standard anaesthesia, and other possible sources of variability had no influence on the isoprenaline response of the colon.
Specimens were available at the operating theatre, each consisting of a whole colon segment from a macroscopically normal region; they were washed in saline and immediately placed in a cold (4°C) pre-aerated (95% O2, 5% CO2) Krebs' solution (composition (mmol/l): Na Cl 118.4, KCl 4.7, CaCl2 2.5, KH2PO4 1.2, MgSO4 1.2, NaHCO3 25, glucose 11.7) and transported to Sanofi laboratories within approximately 30 minutes. Mucosa and submucosa were gently removed; circular and longitudinal (taenia coli) smooth muscle were cleaned of surrounding fat and connective tissue; and muscle regions were cut into strips approximately 3 mm wide along the longitudinal (taenia) or circular axis (total length of each preparation about 2 cm).
EXPERIMENTAL CONDITIONS
Strips (18–24) were dissected from each specimen, allowing direct comparison of agonist and antagonist activities. A few responses were tested in duplicate, in which case the results were always averaged and considered as from the same specimen.
Colonic strips were immediately mounted in a 20 ml organ bath containing warm (37°C) aerated (95% O2, 5% CO2) Krebs' solution containing 10−5 mol/l phentolamine, 5×10−7 mol/l desmethylimipramine, and 3×10−5 mol/l hydrocortisone (the latter two for preventing intraneuronal and extraneuronal uptake of catecholamines, respectively). The strips were stretched with 1–1.5 g, washed five times, and allowed to develop stable spontaneous tone. Muscle tension was recorded isotonically with a Gemini polygraph (Basile, Varese, Italy).
After a three hour equilibration period, cumulative agonist concentration-response curves were plotted for each preparation: isoprenaline and terbutaline, 10–20 minutes contact for each concentration; and CGP 12177 and SR 58611A, 60 minutes contact for each concentration. Agonists were tested with or without several β adrenergic antagonists: propranolol, CGP 12177, CGP 20172, and ICI 118551. Relaxation induced by agonists was expressed as a percentage of the maximal effect of papaverine (10−4mol/l) added at the end of each experiment. To test individual strip β adrenergic responsiveness, a maximal dose of isoprenaline (10−4mol/l) was added before papaverine which did not produce any further substantial relaxation except in about 30% of specimens, not included in this study, which had given inconsistent responses to isoprenaline. Antagonists were incubated for 60 minutes before the agonist cumulative concentration-response curves were plotted.
CALCULATIONS AND STATISTICAL ANALYSIS
The agonist concentration producing 50% maximal response (IC50) was calculated using a four parameter logistic model13 and adjustment was made by non-linear regression using the Levenberg-Marquard algorithm in RS/1 software.
The pA2 value for antagonists, as defined by Arunlakshana and Schild,14 was obtained from linear regression of mean log values (Dr−1) against the negative log of the antagonist concentration. Computer analysis was performed according to Tallarida and Murray.15
CHEMICALS
SR 58611A was synthetised in the chemistry department of Sanofi Midy Research Centre.16 Other chemicals were purchased from commercial sources as indicated: desmethylimipramine HCl, CGP 20712 HCl, CGP 12177 HCl, ICI 118551 HCl, (−)isoprenaline HCl, papaverine HCl, phentolamine HCl, propranolol HCl, terbutaline HCl (Sigma Corp., St Louis, Missouri, USA); hydrocortisone sodium, hemisuccinate (Flebocortid ampoules) (Richter-Lepetit, Milan, Italy).
Results
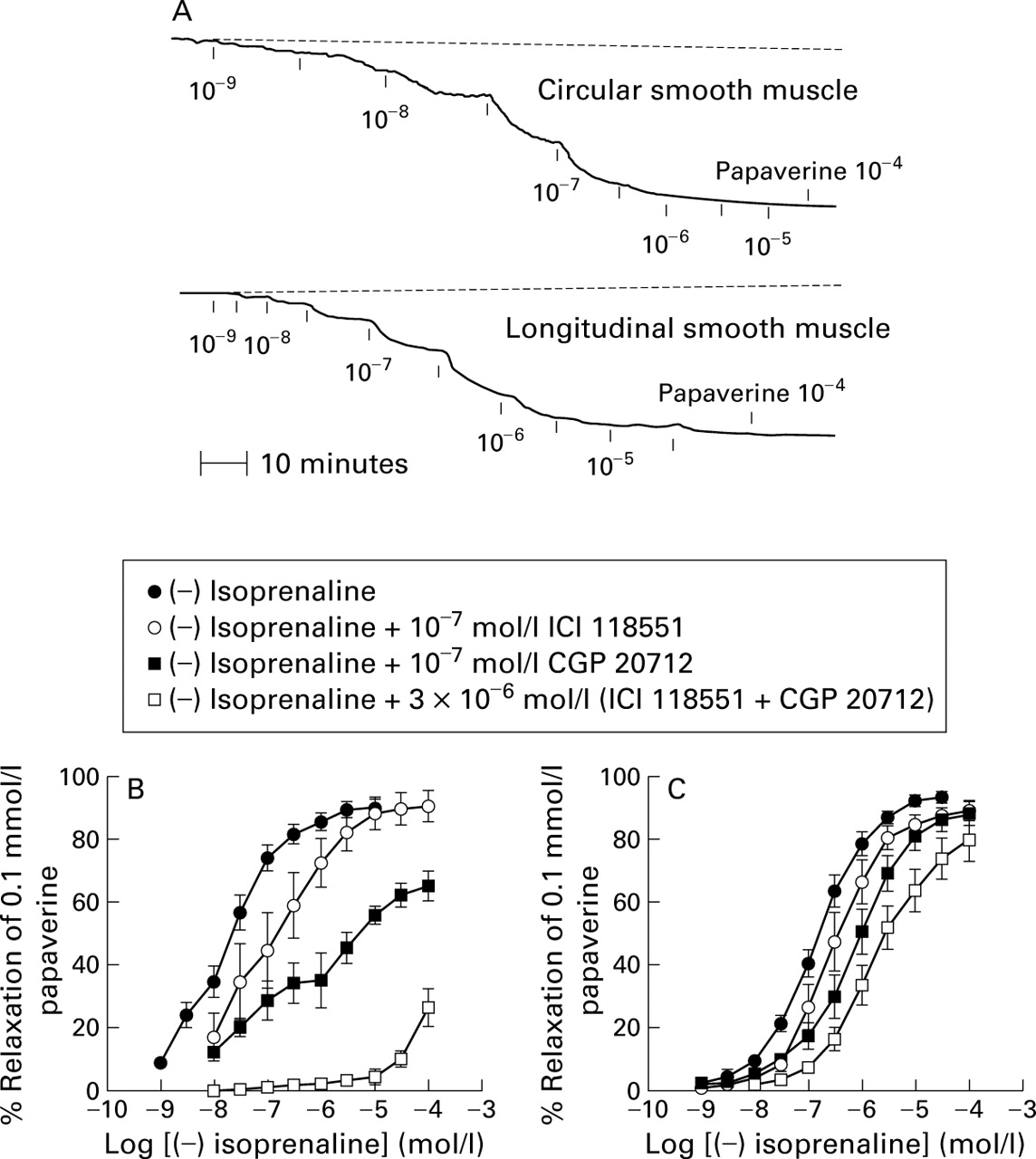
Adding β adrenoceptor agonist to the incubation medium resulted in concentration dependent relaxation of colonic smooth muscle strips from the circular and longitudinal layers; representative tracings with isoprenaline are shown in fig 1A. However, the potency and relaxing action of the agonist—rated as a percentage of the maximal effect of the musculotropic agent papaverine—as well as susceptibility to specific antagonists varied considerably in the two layers. Except for CGP 12177, none of the antagonists alone had an effect on muscle strip tone.
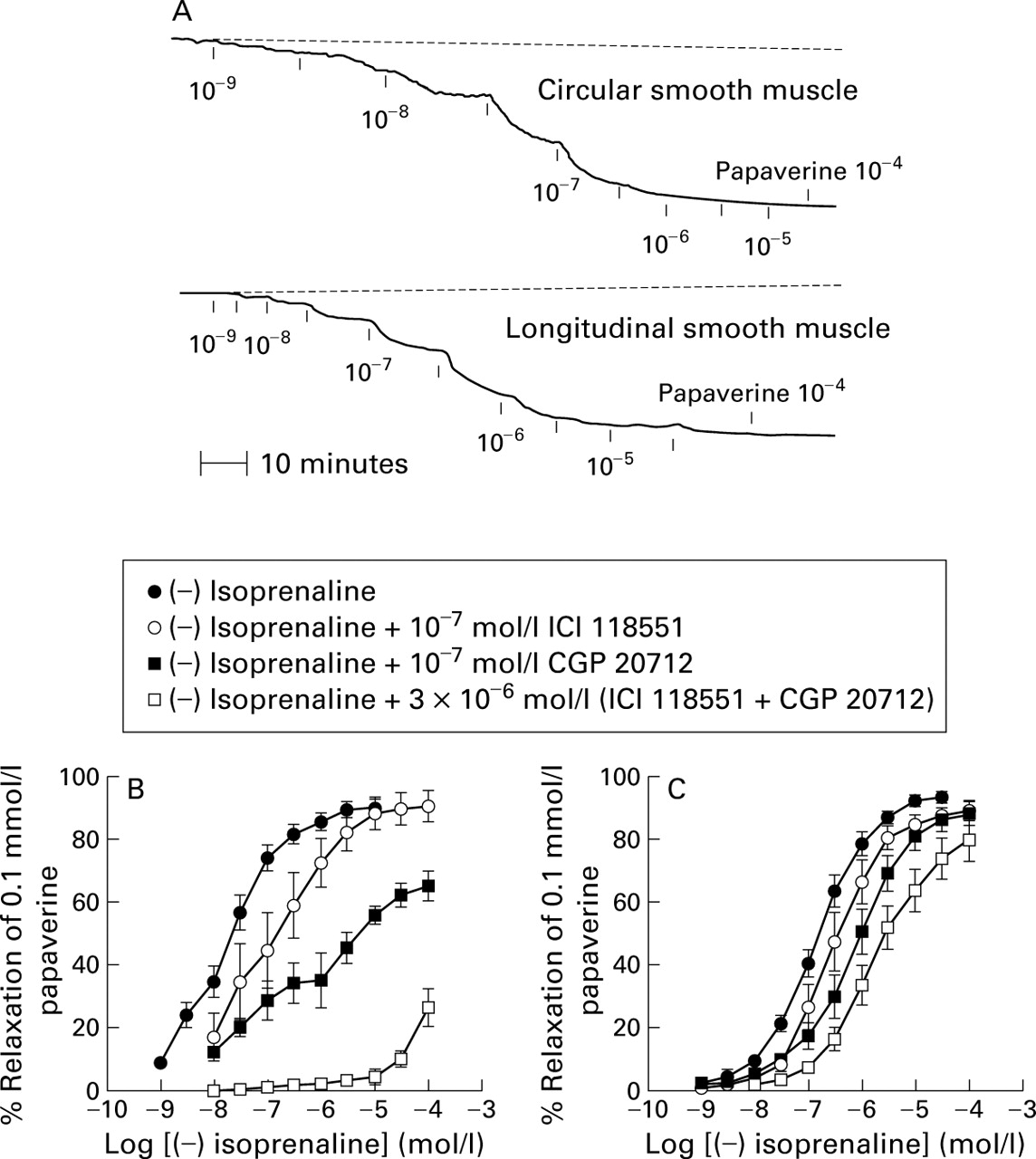
Concentration dependent relaxation of human colon by isoprenaline. (A) Representative tracings; values are mol/l of isoprenaline. (B) Concentration-response curves in circular smooth muscle with and without added β adrenoceptor antagonists; values are mean (SEM) of 5–10 preparations from different patients. (C) Concentration-response curves in longitudinal smooth muscle with and without added β adrenoceptor antagonists; values are mean (SEM) of 5–10 preparations from different patients.
CIRCULAR MUSCLE
In circular muscle, isoprenaline displayed the greatest agonist potency and was the only full agonist (that is, causing maximal relaxation), similar to papaverine; it was more potent than on taenia strips (table 1). Terbutaline had substantially lower potency than isoprenaline on circular strips and its maximal relaxing effect reached about 60% of that of papaverine (table 1, fig 2); CGP 12177 and SR 58611A had little effect (table 1, fig 3).
Potencies of agonists in relaxing human circular and longitudinal (taenia) smooth muscle preparations

Concentration-response curves to terbutaline in human colon circular smooth muscle and taenia coli with and without added β adrenoceptor antagonists. Results are mean (SEM) of 4–6 preparations from different patients.

{kind=link}
{kind=link}
{kind=link}
Concentration-response curves to CGP 12177 and SR 58611A in human colon circular smooth muscle and taenia coli with and without added β adrenoceptor antagonists. Results are mean (SEM) of 4–6 preparations from different patients.
The potency of isoprenaline in relaxing circular strips was reduced slightly by 10−7 mol/l ICI 118551, which presumably selectively blocks only β2 adrenoceptors, and markedly reduced after selective blockade of the β1 adrenoceptor with 10−7 mol/l CGP 20712, which in addition reduced maximal relaxation by isoprenaline. The latter's biphasic concentration-response curve, in the lower concentration range, presumably reflects the β2 adrenoceptor component. The combination of ICI 118551 and CGP 20712 (both 3×10−6mol/l) almost abolished the response to isoprenaline (fig 1B) and similarly rendered terbutaline almost inactive (fig 2).
Extensive tests on quantitative antagonism of isoprenaline relaxation of circular muscle by CGP 12177 and propranolol indicated the former's greater potency and the competitive nature of the antagonism, irrespective of the different potencies of the antagonists (table 2).
Quantitative antagonism of isoprenaline relaxation of human circular and longitudinal (taenia) smooth muscle preparations by propranolol and CGP 12177
LONGITUDINAL MUSCLE (TAENIA COLI)
Isoprenaline and terbutaline were less potent in relaxing colonic longitudinal muscle compared with their effects on circular muscle, although isoprenaline produced full relaxation and was the most potent of the agonists tested, as was the case in circular muscle (table 1). Terbutaline, CGP 12177, and SR 58611A were partial agonists in longitudinal muscle. However, maximal relaxation by terbutaline was about twice that of CGP 12177 and SR 58611A although these were more potent on the basis of their respective 50% effective concentrations which were well below that of terbutaline (table 1; figs 2, 3).
Relaxation of taenia by isoprenaline was less susceptible than circular muscle to ICI 118551 and CGP 20712, either alone or in combination, and even in the presence of both of these antagonists the maximal effect of isoprenaline was not significantly lower than controls, although it required agonist concentrations one order of magnitude higher (fig 1C).
ICI 118551 and CGP 20712 in combination rendered terbutaline less effective on taenia but terbutaline still produced relaxation although concentrations well above control levels were needed (fig 2). ICI 118551 and CGP 20712 did not impair the ability of SR 58611A to relax taenia although this, and the effect of CGP 12177, were prevented by higher concentrations of propranolol (10−5 mol/l) than those effective at β1 and/or β2adrenoceptors (fig 3). The kinetics of quantitative antagonism of isoprenaline relaxation of taenia coli by CGP 12177 and propranolol highlighted its non-competitive nature (Schild plot slopes different from one), unlike the case for circular strips. The potencies of the antagonists versus isoprenaline (based on their respective pA2 values) were comparable in taenia and circular muscle, propranolol being less potent than CGP 12177 (table 2).
Discussion
The extensive functional tests summarised in the present report provide complementary data on the in vitro reduction of intestinal smooth muscle tone by several agonists, with and without appropriate antagonists added, indicating that all three currently recognised β adrenoceptor subtypes variably account for relaxation of the human colon evoked by exogenous agonists, depending on the agonist and muscular layer.
In the circular layer, stimulation of the β1 subtype was the most effective, even achieving full relaxation; this occurred to a substantially lesser extent when only the β2 subtype was stimulated. Reduction of muscular tone ascribable to the β3 subtype was minimal. In taenia, full relaxation was obtained by stimulating virtually any β adrenoceptor subtype, providing that isoprenaline was the agonist; however, its potency differed, being about 10 times higher on β1 than on β3, and intermediate on β2 adrenoceptors.
In the circular muscle layer, relaxation by the non-selective β adrenergic agonist isoprenaline was primarily related to β1 adrenoceptor activation as unequivocally shown by the fact that it almost lost its ability to produce a maximal effect (comparable with that of papaverine) when the receptors were selectively blocked with the antagonist CGP 20712. Conversely, selective blockade of β2 adrenoceptors with ICI 118551 had little effect on the potency of isoprenaline in relaxing circular muscle, suggesting β2 adrenoceptors are less important in this tissue; this was further suggested by the inability of the β2 selective agonist terbutaline to produce full relaxation. Finally, stimulation of β3 adrenoceptors appeared to have almost no effect in circular muscle; neither isoprenaline nor terbutaline significantly relaxed this preparation in the presence of the β1 and β2 antagonists, whose combined action did not prevent β3 agonist responses (as shown by failure to affect taenia relaxation by SR 58611A). The selective β3 agonists CGP 12177 and SR 58611A had minimal effects on circular strips.
The limited functional role of β3 adrenoceptors in the human colon circular muscle layer is borne out by results of the comprehensive tests for quantitative antagonism of isoprenaline relaxation by CGP 12177 and propranolol: antagonism was competitive, which is not compatible with a substantial agonist component ascribable to a receptor population (β3) with lower affinity than the β1 and β2 receptors for the antagonists.
Unlike circular muscle, in taenia, tests for quantitative antagonism of isoprenaline using propranolol or CGP 12177 unequivocally highlighted its non-competitive nature, implying that a non-negligible lower affinity site (β3) very likely accounts for the ability of the agonist to relax the preparation. This was confirmed by full relaxation of taenia strips by isoprenaline in the presence of both CGP 20712 and ICI 118551, which prevented isoprenaline acting at β1 and β2 adrenoceptors. β3adrenoceptor mediated relaxation in taenia coli was further illustrated by its concentration dependent relaxation by the selective agonists CGP 12177 and SR 58611A (whose actions were prevented by high concentrations of propranolol). However, both were less effective than isoprenaline (that is, their effects did not exceed 40% of those of papaverine even at the highest concentrations tested).
Functional effects, apparently elicited by stimulation of β3 adrenoceptors in animal tissues, have been widely reported but there is only scant and conflicting information on human specimens, as recently discussed by Sennitt and colleagues.17 Reports on the motor responses of different human large intestine in vitro preparations to catecholamines, phenylethylamines, and CGP 12177—a non-selective β1, β2 adrenoceptor antagonist with β3 agonist action at concentrations three orders of magnitude higher that we used successfully as a β3 antagonist in view of its partial agonist action—generally agree that there is a β3adrenoceptor mediated component, similar to the one we discovered on similar grounds.18-22
However, before this study, no serious attempt was made to assess the importance of this component by comparison with responses caused by selective stimulation of β1 or β2adrenoceptors, and the information available to date, including from our study, has some inconsistencies regarding these responses. Thus although there is general agreement on the primary involvement of β1 adrenoceptors in the inhibitory motor responses of human colonic tissues evoked by appropriate agonists, none of the researchers who studied β adrenoceptors in the human colon found unequivocal evidence of a functional role for β2adrenoceptors. None the less, our coherent findings with agonists and antagonists of pronounced (circular) and even maximal (taenia) in vitro relaxation of colon strips, after stimulation of β2adrenoceptors only, are consistent with molecular (messenger RNA) evidence of this receptor subtype in both muscular layers21 and with the clinical observation that rectosigmoid motility is reduced in patients given the selective β2 adrenoceptor agonist terbutaline.9
The only inconsistency on the involvement of β2adrenoceptors in human colon smooth muscle responses comes from comparing our extensive results supporting this claim with limited negative findings from the one other laboratory that specifically addressed this aspect: salbutamol did not affect spontaneous activity and ICI 118,551 did not prevent its inhibition by isoprenaline, both tested only on circular muscle.19
The most recently published functional study on the atypical nature of the β adrenoceptors in taenia coli20 reluctantly admitted a component complying with the β3 subtype and speculated on the possibility of yet another subtype (β4). The authors argued about the possible lack of specificity of taenia relaxation by CGP 12177 that was refractory to high concentrations (100 μM) of the β blocker nadolol; they cast doubt on any such action of isoprenaline because it had no effect on the response elicited by CGP 12177. The latter finding, however, is consistent with isoprenaline acting at β3 adrenoceptors, as we have unequivocally shown that CGP 12177 is also a potent β3 antagonist in taenia coli. Moreover, the non-competitive nature of isoprenaline antagonism that we demonstrated in taenia with propranolol or CGP 12177 also indicates a non-β1, non-β2 component to its action at β adrenoceptors therein. Finally, by using a β blocker different from nadolol (that is, propranolol) at a concentration higher than that needed for β1 and β2 adrenoceptor antagonism, we observed displacement of the concentration-response curves for both CGP 12177 and SR 58611A, thus attesting to the specificity of their relaxation of taenia.
A major shortcoming in assessing the relative functional roles of β3 adrenoceptors in smooth muscle of the human large intestine, or other human tissues, is the lack of available β3 selective agonists. Compounds such as BRL 37344, SR 58611A, and CL 316243, when tested in vitro and in vivo on different intestinal segments of several animal species, proved even more powerful or as effective as the non-selective agonist isoprenaline, which acts on all three β adrenoceptor subtypes.3 Yet BRL 37344 was either inactive18-20 or had little effect and low potency21 ,22 in vitro on human colon muscle strips; this also applies to SR 58611A, as shown in our study. Adipocytes are reportedly the only human specimens challenged to date with CL 316243 that produced either a weak23 on no response,24 putatively mediated by β3adrenoceptors. However, non-selective β adrenoceptor agonists such as isoprenaline are substantially more potent and effective on the β3 subtype in human tissues than the above compounds originally designed based on animal assays. Thus “blurring” the responses of the β1 and β2 adrenoceptors with suitable antagonists, as performed by several investigators including ourselves, makes it possible to isolate the isoprenaline response component presumably due to activation of the β3subtype only, which can then be assessed in comparison with the same components for the other two subtypes.
Our comprehensive functional tests, in common with other similar but less extensive observations19 ,21 on the mechanical responses elicited in human intestine, indicate a major role for β3 adrenoceptors in taenia coli, but only a limited component, if any, in circular strips. Recent immunohistological25 and molecular biology (messenger RNA)21 studies showed more β3 adrenoceptors in taenia coli than in the circular muscular layer. However, De Ponti and colleagues18 found that isoprenaline fully relaxed human colonic circular smooth muscle in the presence of β1 and β2 adrenoceptor antagonists; this finding, unlike those discussed above, supports the considerable functional importance of β3 adrenoceptors in the circular layer also.
Different experimental conditions may account for the differences between the results from laboratories which have reinvestigated the functional role of β adrenoceptor mediated motor responses of isolated human colonic smooth muscle in the light of the recently discovered β3 subtype. As indicated by other investigators,19 uncontrolled variability from in vitro assays on human colon specimens obtained from surgery arise from: medication of the patient for disease or as needed for operative procedures; the assumption that the tissue proximal to a lesion is normal; handling of the tissue during surgical procedures (air exposure, ischaemia by clamping the blood supply); and the heterogeneity of patients. Additional differences in experimental conditions concern the end points such as relaxation of basal18 ,20 (similar to the present study) or chemically induced (KCl, carbachol) smooth muscle tone,19-21 and inhibition of spontaneous contractions.19 ,22
Regardless of these difference, complementary in vitro evidence strongly supports the presence and functional importance of β3 adrenoceptors in human colonic smooth muscle. Our findings suggest they do not play a secondary role in taenia coli, in association with the β1 and β2 subtypes whose relevance to gastrointestinal motility has been clinically established. The notion that β3 adrenoceptors may also be clinically important in gastroenterology suggests two important potential developments: (a) their susceptibility to endogenous catecholamines19 ,20 may be altered in functional gut motility disorders whose nature is currently unclear; (b) should β3 adrenoceptors have no substantial role in the human cardiovascular system, as in several animal species,3β3 adrenoceptor selective pharmacological agents may provide a new tool for therapeutically aimed pharmacological control of gut motility.3
Clinical trials with currently available β3 selective adrenoceptor agonists have been disappointing, not surprisingly in view of their low potency and effectiveness in human specimens in vitro. Yet persistence of some metabolic effects of isoprenaline when infused to healthy volunteers given a β adrenoceptor blocking agent preventing its cardiovascular actions (β1 and β2 adrenoceptor mediated) has been attributed to stimulation of β3 adrenoceptors only.26
Progress in understanding the clinical relevance of β3adrenoceptors in the intestine and elsewhere now awaits the results of research with new chemical agents with high potency and selectivity for the human receptor.
Abbreviations used in this paper
- IC50
- concentration producing 50% maximal response