Article Text

Abstract
BACKGROUND Changes in substance P content and a relationship between the degree of perineural inflammation and pain has been demonstrated in chronic pancreatitis. Whether a relationship exists between neural alteration and pancreatic inflammation (neurogenic inflammation) is not known.
AIMS In the present study we evaluated gene expression of preprotachykinin A (PPT-A), the gene encoding substance P, and interleukin 8, a proinflammatory and hyperalgesic mediator whose release is co-regulated by substance P.
PATIENTS Pancreatic tissue specimens obtained from 21 patients (16 male, five female) with chronic pancreatitis and 18 healthy organ donors (nine male, nine female) were analysed.
METHODS Gene expression of PPT-A and interleukin 8 was studied by northern blot analysis. Respective proteins were localised using immunohistochemistry.
RESULTS Northern blot analysis showed that PTT-A mRNA expression levels were present at comparable levels in normal and chronic pancreatitis tissue samples. In contrast, interleukin 8 mRNA was expressed at very low levels in normal controls but was increased 41-fold (p<0.001) in chronic pancreatitis tissue samples. Using immunohistochemistry, interleukin 8 protein was localised mainly in immune cells often found around enlarged pancreatic nerves. In addition, in chronic pancreatitis, intense interleukin 8 immunostaining was present in metaplastic ductal cells of the atrophic pancreatic parenchyma. In chronic pancreatitis samples there was a positive relationship between interleukin 8 mRNA levels and the presence of ductal metaplasia (r=0.795; p<0.001) and the inflammation score (r=0.713; p<0.001).
CONCLUSIONS Our data indicate that in chronic pancreatitis, the increase in substance P in enlarged pancreatic nerves is not caused by enhanced intrapancreatic PTT-A mRNA expression, suggesting that the location of substance P synthesis is outside of the pancreas. In addition, localisation of interleukin 8 positive immune cells around pancreatic nerves further supports the existence of neuroimmune interactions as a pathophysiological mechanism in chronic pancreatitis.
- chronic pancreatitis
- interleukin 8
- neurogenic inflammation
- preprotachykinin A
- substance P
- immunohistochemistry
Abbreviations used in this paper
- IL-8
- interleukin 8
- PPT-A
- preprotachykinin A
- CP
- chronic pancreatitis
- ENS
- enteric nervous system
- GAPDH
- glyceraldehyde-3-phosphate dehydrogenase
- TBS
- Tris buffered saline
- ir
- immunoreactive
- PMNL
- polymorphonuclear leucocytes
- TNF
- tumour necrosis factor
Statistics from Altmetric.com
- chronic pancreatitis
- interleukin 8
- neurogenic inflammation
- preprotachykinin A
- substance P
- immunohistochemistry
Chronic pancreatitis (CP) is characterised histologically by atrophy of the exocrine pancreatic tissue, an increase in local fibrosis, and alterations in nerves, especially in areas of inflammation.1 These histological changes are accompanied by chronic inflammation and recurrent or persistent upper abdominal pain. Nevertheless, the pathophysiology of chronic inflammation and pain generation in CP is not clear and is still under investigation. Current concepts in neurobiology indicate possible participation of the enteric nervous system (ENS) in pain generation and in the inflammatory process in CP.2-6
Recently, we supplied immunohistochemical evidence for neuronal activation in CP using GAP-43, a well-established marker of neuronal plasticity.7 Moreover, a relationship was found between the presence of GAP-43 in intrapancreatic nerves and abdominal pain.8 In addition, a previous study, using immunostaining, demonstrated that the pattern of pancreatic innervation is altered in CP, leading to increased immunoreactivity for different neuropeptide proteins, such as substance P, calcitonin gene related peptide, and vasoactive intestinal polypeptide, which are known to be proinflammatory and pronociceptive mediators.9 These findings, together with the observation of perineural accumulation of inflammatory cells, indicate the possibility of neuroimmunological interactions in the pathophysiology of CP.
Neuropeptides such as substance P are implicated in local immune responses. Substance P increases the proliferation of activated lymphocytes and immunoglobulin synthesis both in vivo and in vitro.10 Furthermore, cytokines, a class of glycoproteins with immunoregulatory functions, have been shown to interact with substance P in various paradigms for pain and inflammation.11 Interleukin 1 and substance P were shown to synergistically increase proliferation of the BALB/3T3 fibroblast cell line in a model of arthritis associated with inflammation,12 and substance P directly stimulates the release of interleukin 8 (IL-8) from macrophages. Substance P, a proinflammatory mediator mainly involved in acute inflammatory responses, stimulates and triggers the release of other cytokines and growth factors.13 ,13 Inasmuch as IL-8 release also generates hyperalgesia by stimulation of postganglion sympathetic neurones,10 these observations strongly suggest that neuropeptides and cytokines might be involved in the pathophysiology of inflammatory disorders and might contribute to the ongoing inflammation and destruction of the exocrine pancreas in CP.
To assess this hypothesis we used northern blot analysis and immunohistochemistry to evaluate expression of the preprotachykinin A (PPT-A) gene, which encodes substance P, and of IL-8 in CP and the normal human pancreas.
Materials and methods
PATIENTS AND TISSUE SAMPLING
CP tissue samples were obtained from 21 patients (five female, 16 male; median age 43.6 years; range 34–49 years) who underwent pancreatic resection. The aetiology of CP was alcohol overconsumption in all patients, and surgical procedures consisted of either a partial duodenopancreatectomy (Whipple operation, three patients) or a duodenum preserving pancreatic head resection. Normal human pancreatic tissue samples were obtained through an organ donor programme from 18 previously healthy individuals (nine female, nine male; median age 30.3 years; range 17–56 years) from whom other organs were taken for transplantation and no recipients for the pancreas were present. Histomorphological analysis of CP graded disease severity as moderate to severe in all patients. In all cases, freshly removed tissue samples were fixed in a paraformaldehyde solution for 12–24 hours, followed by paraffin embedding for histological analysis. In addition, part of the tissue samples destined for RNA extraction was snap frozen in liquid nitrogen immediately on surgical removal and maintained at −80°C until use. The studies were approved by the Human Subjects Committee of the University of Bern, Switzerland.
PROBE SYNTHESIS
The PPT-A cRNA probe consisted of a 457 base pair KspI/SacI fragment of human PPT-A cDNA corresponding to nucleotides 202–659.15 The IL-8 cDNA probe consisted of a 220 base pair NdeI/XhoI fragment of human IL-8 cDNA excised from pRSET-A plasmid (kind gift of Dr Sozzani, Istituto di Ricerche Farmacologiche Mario Negri, Milano, Italy). To verify equivalent RNA loading and RNA transfer in the northern blot analysis, a cDNA probe for glyceraldehyde-3-phosphate dehydrogenase (GAPDH) (ATCC, Rockville, Maryland, USA) was used. For northern blot analysis, cDNA probes (IL-8 and GAPDH) were labelled with [alpha-32P]dCTP (Du Pont International, Regensdorf, Switzerland) prepared by using a random primer labelling system (Boehringer-Mannheim, Mannheim, Germany). The PPT-A cRNA probe was radiolabelled with [alpha-32P]CTP (Du Pont International, Regensdorf, Switzerland).
IMMUNOHISTOCHEMISTRY
Paraffin embedded tissue sections 2–4 μm thick were subjected to immunostaining using the streptavidin-peroxidase technique. Tissue sections were submerged for 15 minutes in Tris buffered saline (TBS) (10 mM Tris HCI, 0.85% NaCI, pH 7.4) containing 0.1% (vol/vol) Triton X-100, and washed for five minutes in TBS solution, as previously reported.16-19 Endogenous peroxidase activity was quenched by incubating the slides in methanol and in methanol/0.6% hydrogen peroxide, followed by washings in methanol and TBS containing 0.1% bovine serum albumin. Following treatment with hyaluronidase (1 mg/ml in 100 mM sodium acetate, 0.85% NaCI), sections were incubated for 30 minutes at 23°C with 10% normal goat serum, and incubated overnight at 4°C with polyclonal antibodies against IL-8 (Endogen, Inc., Woburn, Massachusetts, USA) (1:25 dilution) and substance P (Serotec, Kidlington, Oxford, UK) (1:5000 dilution), or a monoclonal CD-68 antibody (DAKO Diagnostics AG, Zürich, Switzerland) (1:200 dilution) that labels human monocytes and macrophages. The antibodies were diluted in 5% normal goat serum. Bound antibody was detected with a biotinylated goat antirabbit or antimouse IgG secondary antibody and a streptavidin-peroxidase complex (Kirkegaard and Perry Laboratories, Inc., Gaithersburg, Maryland, USA), followed by incubation with diaminobenzidine tetrahydrochloride (0.05%) (brown colour reaction) as substrate and counterstaining with Mayer's haematoxylin.
To ensure antibody specificity, control slides were incubated in the absence of primary antibody or incubated with non-specific IgG antibody. In both cases no immunostaining was detected. All slides were analysed by two independent observers blinded to patient status, followed by resolution of any differences by joint review and consultation with a third observer.
NORTHERN BLOT ANALYSIS
Total RNA was extracted by the guanidine isothiocyanate method, size fractionated on 1.2% agarose/1.8 M formaldehyde gels, and stained with ethidium bromide for verification of RNA integrity and loading equivalency.16-18 ,20 RNA was electrotransferred onto nylon membranes (Gene Screen, Du Pont, Boston, Massachusetts, USA) and cross linked by UV irradiation. The filters were then prehybridised, hybridised, and washed under conditions appropriate for specific antisense cRNA riboprobes (PPT-A) or cDNA probes (IL-8 and GAPDH).
In the case of the antisense riboprobe, blots were prehybridised overnight at 65°C. The blots were then hybridised for 18 hours at 68°C in the presence of 1×106 cpm/ml of the [alpha-32P]CTP labelled antisense riboprobe, washed twice at 65°C in a solution containing 1×SSPE (150 mM NaCI, 10 mM NaH2PO4, and 1 mM EDTA) and 0.5% SDS, and washed twice at 65°C in a solution containing 0.1×SSPE and 0.5% SDS.16-18 ,20 In the case of the cDNA probes, blots were prehybridised overnight at 42°C. Hybridisation was carried out at 42°C for 18 hours with the [alpha-32P]dCTP labelled cDNA probe (1×106 cpm/ml for IL-8, 1×105cpm/ml for GAPDH) and then washed twice (50°C) in 2×SSC and three times at 55°C in 0.2×SSC and 2% SDS.16-18 ,20
Membranes were then exposed at −80°C to Fujix ray films with intensifying screens for 1–12 days. All membranes were rehybridised with the GAPDH cDNA probe to assess equivalent RNA loading. The autoradiograms were scanned and peak areas were measured for relative mRNA levels (IL-8/GAPDH and PPT-A/GAPDH) in the samples tested. Values were stored in spreadsheet software producing a graphic representation of the signals.
RELATIONSHIP BETWEEN IL-8 mRNA EXPRESSION AND HISTOPATHOLOGICAL ANALYSIS
IL-8 mRNA expression data obtained by northern blot analysis were correlated with histopathological parameters. In this analysis the inflammation score, presence of ductal metaplasia, and degree of fibrosis were included. To assess these parameters in the CP samples, haematoxylin and eosin stained tissue sections were analysed. The inflammation score (graded 0–3), presence of ductal metaplasia (graded 0–3), and percentage of fibrosis (graded 0–100%) were measured on five different tissue sections in each CP tissue sample and the mean value calculated, as previously reported.17 ,20
STATISTICAL ANALYSIS
Results are expressed as median and range or upper and lower quartiles. For statistical analysis the Mann-Whitney U test and Spearman's rank correlation test were used. Significance was defined as p< 0.05.
Results
NORTHERN BLOT ANALYSIS
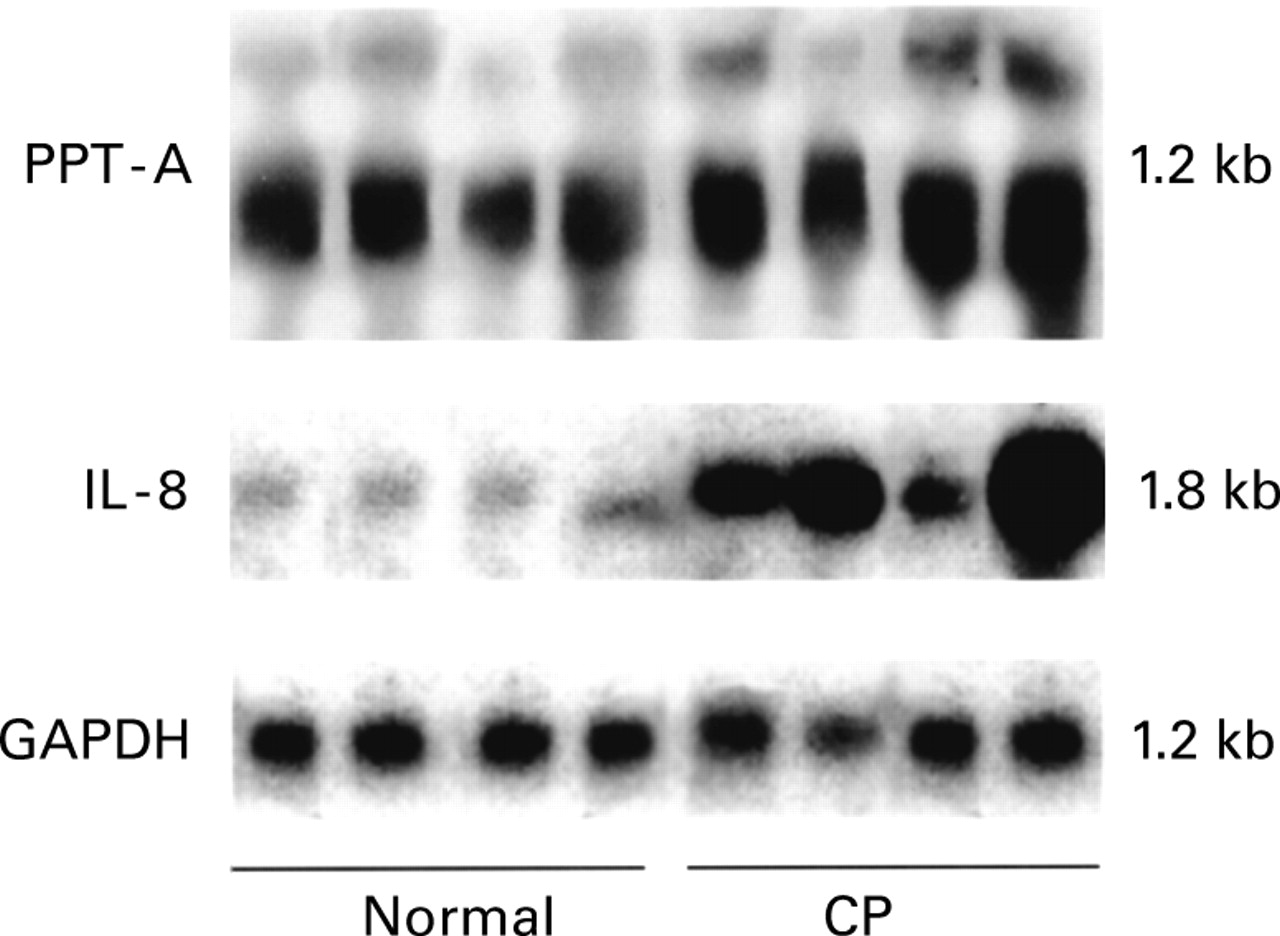
PPT-A mRNA signals (transcript size 1.2 kb) were detectable in both the normal pancreas and CP tissue samples (fig 1). Densitometric analysis of the northern blot signals revealed no significant differences between the normal and CP tissue samples (p>0.05) (fig 2). IL-8 mRNA expression (transcript size 1.8 kb) was only weakly visible on the original autoradiographs in the normal pancreatic tissue samples (fig 1). In contrast, 86% of the CP tissue samples exhibited markedly enhanced IL-8 mRNA levels (fig 1). Densitometric analysis of the northern blots indicated that IL-8 mRNA levels were 41-fold increased (p<0.001) in CP compared with normal controls (fig2).

Northern blot analysis. Preprotachykinin A (PPT-A) and interleukin 8 (IL-8) mRNA expression in the normal pancreas (first four lanes) and in tissue samples from patients with chronic pancreatitis (CP) (latter four lanes). PPT-A mRNA was detectable in comparable levels in normal and CP tissue samples. In contrast, enhanced levels of IL-8 mRNA were present in CP samples. The filters were rehybridised with glyceraldehyde-3-phosphate dehydrogenase (GAPDH) cDNA to verify equivalent RNA loading and RNA transfer. PPT-A mRNA migrates as a 1.2 kb band and IL-8 as a 1.8 kb band.

Densitometric analysis of northern blots. Preprotachykinin A (PPT-A), interleukin 8 (IL-8), and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) mRNA levels were analysed by laser densitometry in the normal pancreas and in chronic pancreatitis. The ratio of the optical density between PPT-A, IL-8, and the corresponding GAPDH signal was calculated. Bars represent the median with upper and lower quartiles. *p<0.001.
IMMUNOHISTOCHEMISTRY
In normal pancreatic tissue samples, substance P immunoreactive (ir) nerve fibres were regularly detected in the exocrine parenchyma, in vascular and perivascular nerves, in a few intrinsic nerve cell bodies, and in some inter- and intralobular nerves. IL-8 immunostaining in the normal human pancreas was absent (fig 3A).

{kind=link}
{kind=link}
{kind=link}
Immunohistochemical analysis. Interleukin 8 (IL-8) immunohistochemical analysis in the normal pancreas (A) and in chronic pancreatitis (CP) (B–D, F, H). In the normal pancreas (A), no IL-8 immunostaining was detectable. In contrast, in CP tissue sections (B–D, F, H), moderate to intense IL-8 immunoreactivity was found, mainly in the inflammatory cells (D, F, arrows) surrounding enlarged pancreatic nerves. In some cases those nerves were substance P immunoreactive (E). Panels (G) and (H) (arrowheads) show staining of consecutive tissue sections of CP for CD-68 (G) and IL-8 (H). The inserts in (G) and (H) show that IL-8 immunoreactive cells (H) are most probably also stained CD-68 positive (G). In addition, in CP tissue samples, moderate to strong IL-8 immunoreactivity was also found in metaplastic ductal cells (B, C, arrows). n=nerve; d=duct. (A) IL-8 immunostaining; (B– D, F, H) IL-8 immunostaining (patients Nos 14, 16, see table 1); (E) substance P immunostaining (patient No 14); (G) CD-68 immunostaining (patient No 16). Original magnification ×200.
In CP, enlarged nerve bundles were regularly detected. As described before, moderate to strong substance P immunoreactivity was observed in these enlarged nerves (fig 3E). The number of intrinsic neurones staining for substance P was higher than in organ donors, and the intensity of the immunohistochemical signals varied from weak to moderate. Nerve fibres exhibiting intense substance P ir were in some cases surrounded by inflammatory cells (fig 3D, E, arrows). In some regions, inflammatory cells often positively stained for substance P and infiltrated the nerve bundles and ganglia in which strong substance P immunostaining was present (fig 3E)
In addition, in the CP tissue samples, immune cells showed moderate to intense IL-8 immunocytochemical staining (fig 3D, F, arrows). IL-8 immunostaining was more evident, especially in those inflammatory cells surrounding the enlarged nerve bundles in the so-called “inflammatory foci” (fig 3D, F, arrows). These findings were more evident in the area of severe pancreatic damage where the parenchyma was almost completely replaced by fibrosis. In addition, intense IL-8 immunostaining was detected in the remaining acinar cells of the exocrine parenchyma, in metaplastic ductal cells, and in areas where the atrophic acinar cells appeared to dedifferentiate into tubular and duct-like structures (fig 3B, C, arrows). Moreover, consecutive CP tissue sections were stained with both IL-8 (fig 3H) and CD-68 antibodies (fig 3G), a specific marker of human monocytes and macrophages, thus indicating that most of the IL-8 immunopositive cells were also CD-68 immunoreactive (fig 3G, H, arrowheads).
CORRELATION BETWEEN NORTHERN BLOT RESULTS AND HISTOMORPHOLOGICAL ANALYSIS
CP tissue specimens were evaluated to determine if there exists a relationship between inflammation score, presence of ductal metaplasia or degree of fibrosis, and IL-8 mRNA expression levels (table 1). There was a significant positive relationship between the presence of ductal metaplasia and IL-8 mRNA expression levels (r=0.795; p<0.001) and between inflammation score (r=0.713; p<0.001) and IL-8 mRNA expression levels. However, no relationship between the degree of fibrosis and IL-8 mRNA expression levels (r=−0.269) was found.
Histopathological findings and interleukin 8 (IL-8) mRNA expression in patients with chronic pancreatitis (CP). Evaluation of the inflammation score, ductal metaplasia, fibrosis, and IL-8 mRNA levels are given in the methods section
Discussion
During the past decades much information has been accumulated on the occurrence and distribution of neuropeptides in the gastro-entero-pancreatic system. Additionally, alterations in the ENS in the regulation of gut functions have been postulated for a number of pathological conditions, including achalasia, Hirschsprung's disease, inflammatory bowel diseases, irritable bowel diseases, etc.19 ,21-23 In recent studies on pancreatic nerves in patients with CP, we used immunochemistry to demonstrate changes in peptidergic innervation. These findings led to the hypothesis that alterations in pancreatic nerves, possibly interrelated with the immunological response, could be involved in the pathogenesis of pain and also in the inflammation of the pancreas.7-9
In the present study, we confirmed our pervious findings of a significant increase in substance P immunoreactive nerve fibres in CP.9 However, there was no difference in PPT-A mRNA expression between normal and CP tissue samples, indicating that the increase in substance P ir nerve fibres in CP is not caused by enhanced intrapancreatic PPT-A mRNA expression. These observations led to the hypothesis that enhanced PPT-A mRNA synthesis might occur in extrapancreatic ganglia and that substance P synthesised in the nerve cell bodies of the spinal root ganglia is afterwards transported through the enlarged nerve fibres into the inflamed pancreas. These observations are supported by our clinical experience that often only resective surgery—such as the Whipple operation, the duodenum preserving pancreatic head resection with dissection of extrapancreatic nerve fibres entering the pancreatic head, or thoracoscopic splanchnicectomy by cutting of the sensitive nerve fibres—is successful in treating pain in CP.24 ,25
In addition, in the present study we found a significant increase in IL-8 mRNA expression in most of the CP tissue samples. Immunohistochemistry showed IL-8 present mainly in macrophages surrounding the enlarged pancreatic nerves but also in the remaining acinar cells of the exocrine parenchyma and often in the metaplastic ductal cells. Moreover, in CP we found a positive correlation between the inflammation score and IL-8 mRNA expression levels and between the presence of ductal metaplasia and IL-8 mRNA expression levels.
The proinflammatory cytokine IL-8 is a well known α chemokine involved in leucocyte recruitment and activation.26 It is increased in a broad range of acute inflammatory disorders27 and has chemotactic activity for T lymphocytes.28 IL-8 was originally isolated from stimulated monocytes29 but it is also secreted by a variety of cell types, including lymphocytes,30neutrophils,31 epithelial cells,32 vascular cells,33 and fibroblasts.34 Meanwhile, several studies have emphasised a possible link between neuropeptides and inflammatory mediators. Lotz and colleagues10demonstrated that substance P and related peptides are potent and specific stimulators of the production of cytokines such as IL-1, tumour necrosis factor α (TNF-α), and IL-6 by human blood monocytes, suggesting that immunological and inflammatory responses might be regulated by signals deriving from the nervous system. Moreover, substance P affects the functional responses of polymorphonuclear leucocytes (PMNL) by directly inducing IL-8 synthesis and release, and by enhancing IL-8 release from PMNL induced by other stimuli such as TNF.35 The reported findings on interaction of substance P and IL-8, in combination with our present data, indicate to us that mRNA expression of IL-8 in CP could be mediated in part by substance P released from sensory pancreatic nerves. In fact, in the present study, using immunohistochemistry, we demonstrated intense IL-8 immunoreactivity in those inflammatory cells, especially macrophages, present around the enlarged nerves in the so-called “inflammatory foci”. Thus induction of IL-8 in immune cells by substance P might contribute to amplification of the inflammatory process in CP. In addition, IL-8 was also present in the remaining exocrine pancreatic parenchyma, suggesting the possibility of intrinsic maintenance of the inflammatory response after the first damage to the pancreatic gland, thus sustaining disease progression and evolution.
In conclusion, our findings provide further evidence for a neuroimmune cross talk in CP, which might be a critical aspect in maintaining the inflammatory reaction in the pancreas.
Abbreviations used in this paper
- IL-8
- interleukin 8
- PPT-A
- preprotachykinin A
- CP
- chronic pancreatitis
- ENS
- enteric nervous system
- GAPDH
- glyceraldehyde-3-phosphate dehydrogenase
- TBS
- Tris buffered saline
- ir
- immunoreactive
- PMNL
- polymorphonuclear leucocytes
- TNF
- tumour necrosis factor