Article Text

Abstract
BACKGROUND AND AIMS Treatment of functional dyspepsia with acid inhibitors is controversial and it is not known if the presence ofHelicobacter pylori infection influences the response.
METHODS After a complete diagnostic workup, 792 patients with functional dyspepsia unresponsive to one week of low dose antacid treatment were randomised to two weeks of treatment with placebo, ranitidine 150 mg, omeprazole 10 mg, or omeprazole 20 mg daily. Individual dyspeptic and other abdominal symptoms were evaluated before and after treatment according to H pylori status.
RESULTS The proportions of patients considered to be in remission (intention to treat) at the end of treatment with placebo, ranitidine 150 mg, omeprazole 10 mg, and omeprazole 20 mg were, respectively, 42%, 50%, 48%, and 59% in the H pylori positive group and 66%, 73%, 64%, and 71% in the H pylori negative group. In H pyloripositive patients, the therapeutic gain over placebo was significant for omeprazole 20 mg (17.6%, 95% confidence intervals (CI) 4.2–31.0; p<0.014 using the Bonferroni-adjusted p level of 0.017) but not for omeprazole 10 mg (6.8%, 95% CI −6.7–20.4) or ranitidine 150 mg (8.9%, 95% CI −4.2–21.9). There was no significant therapeutic gain from active treatment over placebo in H pylori negative patients. Complete disappearance of symptoms and improvement in quality of life also occurred most frequently with omeprazole 20 mg and was significant in both H pylori positive and H pylori negative groups. The six month relapse rate of symptoms requiring treatment was low (<20%) in all groups.
CONCLUSIONS Omeprazole 20 mg per day had a small but significant favourable effect on outcome in H pylori positive patients. The differential response in these patients may be explained by an enhanced antisecretory response in the presence of H pylori. The effect of weaker acid inhibition was unsatisfactory.
- functional dyspepsia
- omeprazole
- ranitidine
- Helicobacter pylori
- randomised controlled trial
- quality of life
Abbreviations used in this paper
- QoL
- quality of life
- ITT
- intention to treat
- PP
- per protocol
Statistics from Altmetric.com
- functional dyspepsia
- omeprazole
- ranitidine
- Helicobacter pylori
- randomised controlled trial
- quality of life
There is still no adequate treatment for functional dyspepsia. In particular, the evidence for treatment of functional dyspepsia with acid pump blockers and other antisecretory agents is contradictory. Recently, two large controlled clinical trials conducted in parallel yielded conflicting results; in one trial, pump blockers appeared to be effective and in the other they were completely ineffective, although the protocols of the two trials were similar.1 In another study, only certain subgroups with a posteriori defined symptoms appeared to respond to omeprazole treatment.2 The question of whether omeprazole treatment is effective is all the more important as other treatment alternatives lack promise.3 There is increasing evidence, for example, thatHelicobacter treatment of functional dyspepsia does not improve dyspeptic symptoms.
Therefore, we conducted a large controlled clinical trial in which we tested the effectiveness of two antisecretory agents, omeprazole and ranitidine. Ranitidine was given at the dose presently recommended for over the counter treatment.4 We intended to conduct the trial in a manner which most closely resembled routine clinical practice. Thus we chose as a main outcome criterion the disappearance of dyspeptic symptoms requiring further treatment, instead of complete disappearance of peptic symptoms. Additionally, we decided not to blind the investigators to Helicobacter pyloristatus. In Germany, where this trial was conducted, a large proportion of dyspeptic patients already know theirH pylori status. Excluding those patients would have led to selection bias. In addition, it is still common clinical practice to give antibiotics to those patients who have adequately responded to symptomatic treatment.5 We tested the validity of this attitude in a second trial including those patients who did not adequately respond in the present study. The results of that trial will be reported elsewhere. Thus in the present study the effectiveness of antisecretory treatment was assessed separately in H pylori positive and negative subjects with functional dyspepsia. This is of particular interest as it has previously been shown that antisecretory agents, in particular proton pump inhibitors, are more effective in H pylori positive than in H pylorinegative subjects.6
Patients and methods
STUDY PROTOCOL
A multicentre, double blind, double dummy, randomised clinical trial with parallel groups was conducted according to Good Clinical Practice and the revised Declaration of Helsinki. The ethics committee at each centre approved the protocol and all patients gave written informed consent.
SELECTION OF PATIENTS
Recruitment took place between August 1994 and July 1996 and included 801 ambulatory patients of both sexes from 71 private gastroenterological practices in Germany, aged ⩾18 years, with chronic functional dyspepsia, with or without gastritis due toH pylori. Chronic functional dyspepsia was defined as epigastric symptoms in the absence of organic disease known to produce epigastric symptoms. Initial symptoms had to be severe enough to require treatment. Dyspeptic symptoms necessitating treatment had to be present for at least four weeks and be severe on at least three days of the seven day run in screening period.
We excluded patients with heartburn/acid regurgitation without concomitant epigastric symptoms and also those with symptoms suggesting irritable bowel syndrome (pain in the lower abdomen, flatulence, diarrhoea, or constipation) which were severe enough to require treatment or diagnostic tests. In addition, patients with any of the following were excluded: current or previously documented erosive or ulcerative oesophagitis, peptic ulcer, or previous abdominal surgery (except for inguinal hernia, appendicectomy, hysterectomy, or Caesarean section); treatment with proton pump inhibitors and/or antibiotic treatment within one month prior to screening or regular treatment within the previous week with other drugs which might interfere with the study outcome; symptoms indicative of serious disease (for example, unintended weight loss, haematemesis) during the previous three months; and conditions associated with poor study compliance (for example, drug addiction or alcoholism).
BASELINE INVESTIGATIONS
At baseline, a complete medical history was taken followed by physical examination, abdominal sonography, and gastroscopy with biopsy (only axial hernia, less than 10 gastric erosions and endoscopic signs attributed to H pylori induced gastritis were permitted at gastroscopy). Biopsy specimens were taken from the corpus (greater curvature) and from the antrum (3 cm proximal to the pylorus) for histological examination using the Sydney criteria7 for assessment of H pylori and gastritis. Rapid urease tests8 (HUT, Astra Chemicals, Wedel, Germany) were also performed and these were considered positive for H pylori if at least one sample of the gastric corpus or antrum caused red discolouration within 24 hours. A validated 13C urea breath test was also performed.8 H pylori infection was diagnosed when, in addition to a positive HUT test, histological examination showed Helicobacter-like organisms in the corpus and/or antrum. The investigators were aware of the HUT test results but were blinded to the histological results throughout the study. Blood samples were taken at entry for routine assessment of haematology and clinical chemistry (one minor transitory abnormality was permitted) and these were repeated after the two week double blind treatment. Additional investigations, for example colonoscopy or CT scan, were done at the investigator's discretion if clinically justified and all findings had to be normal for inclusion in the study.
STUDY TREATMENTS
Patients were given antacid tablets which could be taken up to three times a day during the seven day run in screening period. These were Maaloxan tablets (Rhône-Poulenc-Rorer, Germany) which contained 200 mg of aluminium hydroxide and 200 mg of magnesium hydroxide, with an acid binding capacity of 11 mmol HCl per tablet. Those patients who had severe dyspeptic symptoms on ⩾3 days during the run in screening period were eligible for study treatment. They were randomised and received omeprazole (Losec, Astra Pharmaceuticals Production AB, Sweden) capsules 10 mg (OM10) or 20 mg before breakfast (OM20), ranitidine (Zantac, Glaxo SpA, Italy) tablets 150 mg in the evening before retiring, or placebo tablets and capsules (matched for appearance, taste, and smell) for 14 days. A visit with assessment of symptoms (see below) was carried out at the end of this treatment and if no further management was required (that is, medical treatment other than liquid antacids and/or diagnostic procedures such as endoscopy), patients entered a follow up period of up to six months. With their consent, H pylori positive patients with symptoms requiring further treatment entered a second study evaluatingH pylori treatment (fig 1). ForH pylori negative patients with persistent symptoms at two weeks, the study was terminated, except for a personal visit or a telephone interview six months later.
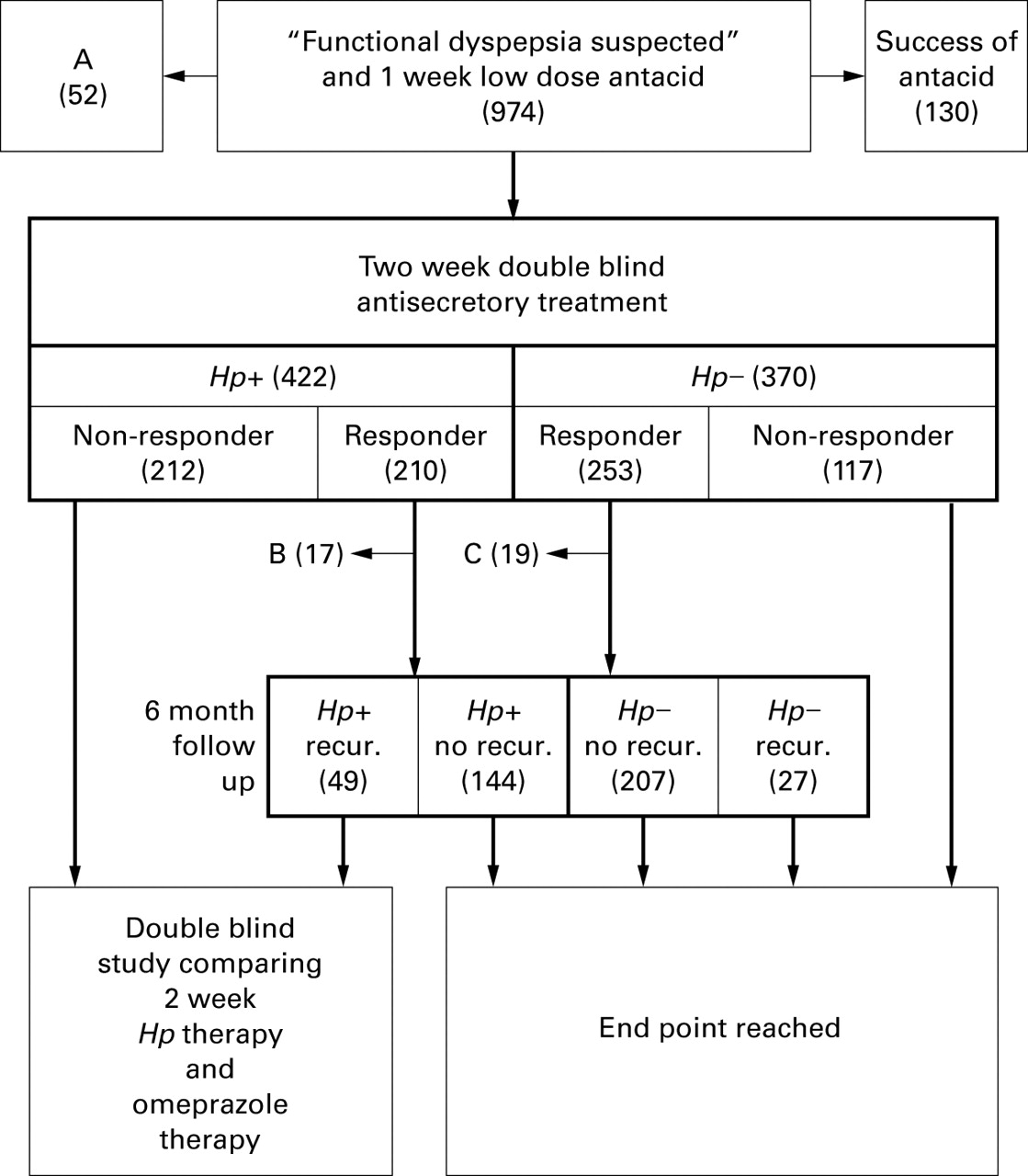
Flow chart of the 974 dyspeptic patients who entered the run in week with low dose antacid treatment. A=not randomized after run in period for reasons other than response to antacid treatment (n=52). B=H pylori positive responders not entering follow up (n=17). C=H pylori negative responders not entering follow up (n=19). Responder=no dyspeptic symptoms requiring further management after the two week double blind treatment (main outcome criterion). Hp, Helicobacter pylori; recur.,recurrence of dyspeptic symptoms requiring management
FOLLOW UP PERIOD
Follow up of patients without symptoms requiring further treatment lasted for six months or until relapse of dyspepsia. During this period, no treatment for dyspepsia other than an antacid suspension (10 ml bags containing 3.13 g of aluminium hydroxide gel, 0.27 g of magnesium oxide, and 0.63 g of magnesium carbonate, with an acid binding capacity of 33 mmol/ml) for occasional dyspeptic symptoms was allowed. Unscheduled visits were encouraged at any time during the six month follow up period when dyspeptic symptoms recurred, when antacid treatment was needed for more than four consecutive days, and/or when antacid consumption exceeded 30 ml per day. Relapse was defined as reappearance of symptoms requiring management (treatment other than liquid antacid and/or diagnostic tests such as endoscopy).
OUTCOME CRITERIA
The main outcome criterion, tested at two weeks, was lack of dyspeptic symptoms requiring further management (as defined above). In addition, the severity of individual dyspeptic and other abdominal symptoms (specifically epigastric pain/burning, epigastric pressure/fullness, heartburn, acid regurgitation, nausea, vomiting, pain in the lower abdomen, flatulence, diarrhoea, and constipation) during the previous week was graded according to a four point scale (0=no complaints, 1=complaints not interfering with daily activities and not requiring treatment, 2=complaints requiring treatment but not interfering with daily activities, and 3=complaints interfering with daily activities and requiring treatment). Patients answered the question “How were your symptoms in the area of the oesophagus and stomach” and “How was your general condition during the last seven days” by making a mark on a 10 cm visual analogue scale (10 cm, best possible condition; 0 cm, worst condition). Quality of life (QoL) during the previous week was assessed using a validated questionnaire adapted to German lifestyles.9 It contained 40 general items relating to physical strength, ability to enjoy and relax, positive mood, absence of negative mood, social contacts, and social well being. In addition, nine questions validated in Germany, relating to impairment of QoL by dyspeptic symptoms,10 were asked. They assessed the effect of dyspeptic symptoms on eating, other daily activities, social contacts, sleep, and fears of serious disease. Finally, the patient's time spent off work and/or in hospital was recorded.
DATA MANAGEMENT AND STATISTICS
Data management was performed according to Good Clinical Practice and data were transferred to an independent statistical institute (Institut für numerische Statistik, Cologne, Germany). The treatment code was broken after decisions on the allocation of individual patients to intention to treat (ITT) and per protocol (PP) analyses. All analyses were based on SAS11 and SPSS7.5 (for Windows).
The response rate based on the primary outcome variable was estimated to be 60% after placebo and 80% after omeprazole therapy. Thus accepting a β error of 0.20, the necessary number of patients per group in an ITT analysis would be 75 (Fisher's exact test, two sided), with an α error adjusted to 0.017 according to Bonferroni to compensate for comparisons between the three active treatment groups and placebo. This number was increased to 90 per group to provide for a valid PP analysis. The primary response rate was tested for centre effects using the Breslow-Day test.
Secondary outcome measures included effects of treatment on gastrointestinal symptoms and on QoL. These analyses were exploratory and used standard significance levels (p<0.05). A life table analysis of relapses during the six month follow up period was performed.
POSSIBLE PROGNOSTIC FACTORS
The following factors were included in a logistic regression analysis using the main outcome criterion as the dependent variable: treatment, age, gender, smoking, alcohol consumption, dyspepsia, gastric erosions present, and positive urea breath test.
Results
PATIENTS
A flow chart showing the fate of the 974 patients entering the one week run in period is shown in fig 1. The response rate to low dose antacid was 13% and was independent of the predominant symptom recorded at entry. Patients who were found to have a cause for their symptoms other than functional dyspepsia were excluded. The remaining 792 patients were symptomatic for at least three days of the run in week and were considered to require treatment. H pylori positive and negative patients (422 and 370, respectively) were randomised to study treatments and data from those patients were included in an ITT analysis. PP analysis was performed on data from 354 and 315 patients (reasons for exclusion of 123 patients are summarised in table 1). There was a similar distribution of patient characteristics across the four treatment groups in bothH pylori positive and negative cohorts (table 2). Comparing the cohorts, H pyloripositive patients were older and more frequently male thanH pylori negative patients.
Reasons for exclusion of patients in the placebo, ranitidine 150 mg, omeprazole 10 mg (OM10), and omeprazole 20 mg (OM20) groups from per protocol (PP) analyses
Pretreatment patient characteristics (intention to treat analysis) in the placebo, ranitidine 150 mg, omeprazole 10 mg (OM10), and omeprazole 20 mg (OM20) groups
EFFECT OF TWO WEEK ANTISECRETORY TREATMENT
Patient response rates (ITT) at the end of two weeks of active or placebo treatment are illustrated in fig 2 for the two outcomes: “no need for management” and “no dyspeptic symptoms”. For comparisons, Fisher's exact test was used. Compared with placebo, a significant therapeutic gain was obtained only with OM20, the beneficial effect being both in terms of management (17.6%; p=0.014 using the Bonferroni adjusted p level of 0.017) and abolition of symptoms (19.6%; p=0.0005) in the H pylori positive group. In the H pylori negative group, there were no significant changes in the primary response (need for management) compared with placebo but in significantly more patients symptoms were abolished after OM20 compared with placebo (16.7%; p=0.023). All changes (compared with placebo) are presented in table 3 and indicate that treatment with OM20 produced the greatest therapeutic benefit, especially in the H pylori positive group. All treatments were more effective at reducing the intensity of dyspeptic symptoms below the “need for treatment” threshold than in abolishing symptoms altogether (fig 2). The results of the ITT analysis for the primary variable were confirmed using a PP approach.
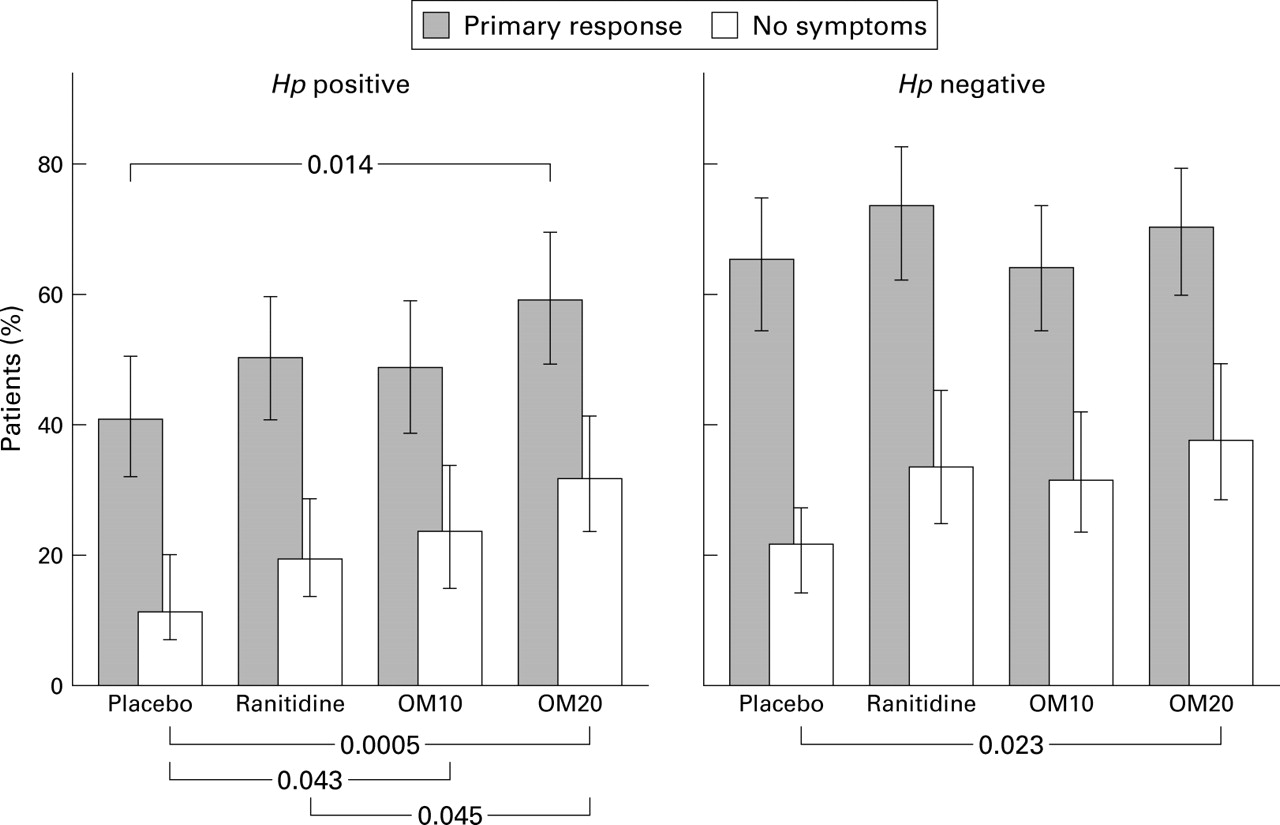
Effect of two week treatment with placebo, ranitidine, omeprazole 10 mg (OM10), or omeprazole 20 mg (OM20) on dyspeptic symptoms according to percentage of patients who became completely symptom free (no symptoms) and those with no need for further management (main outcome criterion) (means and 95% two sided confidence intervals; exact test). For assessment of significance levels, see text. The number of patients per group is given in table 1. Hp, Helicobacter pylori.
Differences in response rates (per cent of patients with 95% confidence intervals) at the end of the two week treatment period compared with placebo (therapeutic gain) in the ranitidine 150 mg, omeprazole 10 mg (OM10), and omeprazole 20 mg (OM20) groups. “Primary response” indicates no need for management of dyspepsia; “No symptoms” indicates disappearance of all dyspeptic symptoms (intention to treat analysis)
Figure 3 shows the proportions of H pyloripositive and negative patients with symptoms of epigastric pain/burning, epigastric pressure/fullness, or heartburn before and after treatment. Placebo treatment caused disappearance of symptoms in approximately one third of patients in each group. OM20 significantly reduced all three symptoms compared with placebo in theH pylori positive patients but only epigastric pressure/fullness was significantly reduced inH pylori negative patients by all three active treatments.

Effect of treatment with placebo, ranitidine, omeprazole 10 mg (OM10), or omeprazole 20 mg (OM20) on individual dyspeptic symptoms. The horizontal bars show the percentages of patients with each individual symptom before and after each two week double blind treatment. *p<0.05; **p<0.025, ***p<0.001 compared with placebo in the same Helicobacter pylori (HP) group.
QoL parameters and impairment caused by dyspepsia were analysed inH pylori positive and negative cohorts before and after treatment. Baseline QoL was similar across the treatment groups for both H pylori positive and negative cohorts and there was significant improvement within all groups (including placebo) following treatment (Wilcoxon signed rank test). However, when improvement was compared between treatments, OM20 improved QoL to a significantly greater extent than placebo on seven out of nine parameters measured in H pyloripositive patients (Wilcoxon rank sum test). In H pylori negative patients, OM20 was significantly better than placebo on only one of nine items of the QoL. With the other treatments, no significant differences from placebo were found for either H pylori positive or negative patients.
ADVERSE EVENTS
The adverse events noted during the study are described below for the four treatment groups and numbers in parentheses refer toH pylori positive and H pylori negative status, respectively. Eight patients (placebo 3 (2/1); ranitidine 4 (3/1); OM10 1 (0/1)) stopped treatment early because of worsening symptoms (they were included in the PP analyses as “treatment failures”) and three patients because of other adverse events: ranitidine 1 (1/0) vascular disorder; OM10 1 (1/0) taste disorder; OM20 1 (1/0) scarlet fever (these three patients were excluded from PP analyses). One OM20 (1/0) patient who developed borreliosis completed the study. All other adverse events (placebo 21 (11/10); ranitidine 28 (14/14); OM10 28 (12/16); OM20 26 (14/11)) were not serious and had no effect on the course of the study or analyses.
LOGISTIC REGRESSION ANALYSIS OF FACTORS AFFECTING THE PRIMARY OUTCOME RESPONSE
In a logistic regression analysis of data from all patients (n=792) using the factors previously described, antisecretory treatment and H pylori infection had a statistically significant influence on treatment outcome. The odds ratios for the two factors were 1.39 (95% CI 1.00–1.93) and 0.46 (95% CI 0.34–0.62), respectively. When, instead of “antisecretory treatment”, each of the four treatment groups was entered separately into the logistic regression analysis, the only statistically significant factor wasH pylori infection. WhenH pylori positive and negative patients were analysed separately, excluding H pyloristatus from the analysis, a significant influence of antisecretory treatment was observed only in H pylori infected patients (odds ratio 1.57, 95% CI 1.01–2.42). No other factors proved to be significant in either group.
RESULTS OF FOLLOW UP
A total of 427 patients (placebo n=97, ranitidine n=108, OM10 n=106, OM20 n=116) entered follow up. Forty nine per cent of patients remained symptom free and 34% had minor symptoms below the need for treatment threshold during the six month follow up period. Only 18% of patients (25% of the H pylori positive group and 12% of the H pylori negative group) had a relapse as defined by the protocol—that is, reappearance of symptoms requiring management. Thirty four patients (total followed by H pylori positive/H pylori negative: placebo 6 (6/0); ranitidine 10 (8/2); OM10 7 (5/2); and OM20 11 (7/4)) were re-endoscoped. Two (2/0) ranitidine patients had erosive duodenitis; all others had normal endoscopic findings. Life table analysis of symptomatic relapse is shown in fig 4. The symptom pattern of relapses closely resembled that observed on admission to the study. Interestingly, OM20 was the most effective treatment for the prevention of relapse in the H pylori positive group while relapse rates were similar with OM20 and ranitidine 150 mg (and not significantly different from placebo) in the H pylori negative group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Life table analysis of patients without sufficient symptoms to require specific active management after successful treatment in the four treatment groups (placebo, ranitidine, omeprazole 10 mg (OM10), or omeprazole 20 mg (OM20)). At time 0 the proportion of patients with successful two week treatment is given; these patients entered follow up. The number of patients per group is given in the text. Hp, Helicobacter pylori.
Discussion
In this large controlled clinical trial, the primary outcome criterion was disappearance of dyspeptic symptoms requiring further management after a two week treatment course. Using this main criterion, which reflects the treatment of dyspeptic patients in general practice, we observed a favourable effect of omeprazole, given at a dose of 20 mg per day, in the treatment of dyspeptic patients infected with H pylori. Conversely, no significant favourable effect was observed in non-infected dyspeptic patients. Using the same outcome criterion, a lower dose of omeprazole, 10 mg a day, and ranitidine given at a dose presently recommended for over the counter treatment of dyspeptic patients,4 were ineffective both in infected and non-infected patients. A favourable effect of omeprazole and ranitidine in non-infected patients cannot be totally excluded because a secondary outcome criterion (that is, complete disappearance of symptoms) appeared to be favourably affected by these two drugs. However, as the primary outcome criterion remained unchanged, this observation is of little importance.
The primary effect of omeprazole 20 mg, albeit statistically significant, was weak. The therapeutic gain over placebo observed inH pylori positive subjects was only 17% and was lower than the actual placebo response (42%) in the same group of patients. The therapeutic gain was similar (20%) when, instead of the primary outcome criterion, complete disappearance of dyspeptic symptoms was used. Even with 20 mg of omeprazole, only about one third of patients became asymptomatic during the two week treatment period.
The two week treatment period was chosen in the present study because in previous positive studies a favourable drug effect was observed within two weeks.11 We cannot exclude the possibility that prolongation of treatment may further improve the favourable effect of 20 mg of omeprazole. However, it may, in parallel, also increase the placebo effect, which appears to increase over time.11 In the present study, low dose antacid treatment, which in previous studies was not different from placebo treatment,11 was given for one week before double blind treatment was started and was successful in 13% of individuals treated. In subjects who did not respond to low dose antacids, the effectiveness of a two week placebo treatment was considerable. This placebo effect might be due in part to the relief of obtaining negative endoscopy results12 and also to the natural history of functional dyspepsia, which typically produces self-limiting symptomatic episodes followed by prolonged periods with little or no symptoms.13 This observation was confirmed during the follow up period of the present study (see fig 4).
The decision was taken not to blind the investigators toH pylori status because in Germany a large portion of dyspeptic patients already know their H pylori status. Furthermore, it was planned to give antibiotic treatment to H pylori positive patients who did not respond to antisecretory treatment. Again, this procedure was intended to resemble, as much as possible, rountine treatment of dyspeptic patients in clinical practice. The study investigators were instructed to include H pylori positive non-responders in a second double blind trial. This option, not available to H pylori negative subjects, could theoretically have led to some bias in the investigators, by making them more prone to recognise therapeutic failure inH pylori positive than inH pylori negative patients. This bias, rather than a more severe form of the disease, may have been responsible for the lower global responsiveness to treatment, including placebo, in H pylori positive than inH pylori negative subjects. However, due to the double blind administration of study treatment, such a bias cannot explain the finding that antisecretory treatment with OM20 had a significant beneficial effect in H pyloripositive patients while in general it was considerably less effective in H pylori negative subjects. Therefore, we conclude that OM20 is more effective in H pylori positive subjects.
The higher therapeutic gain in response to 20 mg of omeprazole inH pylori positive subjects compared with negative subjects might be due to the effect of omeprazole onH pylori.14 Omeprazole causes overall suppression of Helicobacter growth in the stomach and redistribution of inflammation, which improves in the antrum and increases in the corpus. Lower antral inflammation may theoretically normalise gastrin levels, antral motility, and visceral sensitivity, and thus improve functional dyspepsia.15However, more aggressive Helicobactertreatment hardly improved the symptoms of functional dyspeptics in several controlled clinical trials.16-19 Also, in ourH pylori positive patients,Helicobacter treatment did not have a favourable effect, either in those patients with an inadequate primary response to treatment or in those who first responded and later had a recurrence.20 Thus we conclude that neither suppression ofH pylori nor associated improvement of gastritis is responsible for the favourable effect of omeprazole. An alternative mechanism is improvement in pH control by omeprazole in the presence of concomitant H pyloriinfection6 which could, in turn, improve acid induced symptoms of dyspeptics.21 Finally, acid may play a more important role in infected subjects than in non-infected subjects; the infected mucosa could be more acid sensitive than the non-infected mucosa, or duodenal acid clearance could be slower in infected than in non-infected subjects.15 ,21 Functional dyspepsia provides yet another example of where a better clinical effect with proton pump inhibitors is found in H pylori infected subjects. Previous examples include treatment and prevention of recurrence of reflux oesophagitis22 as well as treatment of ulcers induced by non-steroidal anti-inflammatory drugs.23
It could be argued that the difference between H pylori positive and H pylori negative subjects was caused by an unequal distribution of the two collectives. In fact, as expected,24 infected dyspeptics were older than non-infected subjects in our study and were more frequently male. These two characteristics, age and sex, might be associated with a better response of acid symptoms to antisecretory drugs.25-27 To assess this possibility, we performed a logistic regression analysis using all possible confounders. We found that H pylori infection was the only factor associated with outcome when all dyspeptic patients were analysed together. In the group of subjects with H pyloriinfection, the only factor associated with outcome was antisecretory treatment, while in non-infected subjects no predictor was identified in our logistic regression analysis. Therefore, unequal distribution of age and sex cannot explain the different responses of infected and non-infected dyspeptics to antisecretory treatment.
In this study we included patients with heartburn provided they also had epigastric symptoms. We excluded patients with reflux symptoms alone. In these patients, reflux disease appeared to be likely while in patients admitted with heartburn and epigastric symptoms, it remained a possibility, in spite of a normal endoscopic appearance of the oesophagus.28 Oesophageal pHmetry, which is thought by some authors to represent the gold standard for the diagnosis of reflux disease,29 was not feasible in this large multicentre trial and may not in fact have been helpful as it may give abnormal results in asymptomatic subjects and in those with functional dyspepsia who do not complain of heartburn.30 Conversely, heartburn patients may have normal pHmetry.31 Patients with a sensitive oesophagus suffer from acid induced symptoms in spite of normal pHmetry.32 In others, the cause of heartburn is not clear as they have normal pHmetry and do not respond to high dose antisecretory treatment.33 We noted that patients with and without heartburn showed similar responses to treatment and omeprazole improved epigastric pain and pressure as well as heartburn. These observations make it highly unlikely that omeprazole has a favourable effect on functional dyspepsia simply because it improves reflux symptoms. Our study argues against excluding heartburn patients who also complain of epigastric symptoms from controlled clinical trials and from definitions of functional dyspepsia.
We were surprised by the low recurrence rate of dyspeptic symptoms during the six month follow up period. The higher recurrence rate inH pylori positive patients was probably a consequence of biased assessment by the investigators, as was the case for the higher placebo response. More importantly, there was no evidence of a higher recurrence rate after omeprazole in spite of reports of rebound acid secretion in H pylorinegative patients after omeprazole treatment.34
Recently, the question has been raised as to whether or notH pylori infection should be treated in functional dyspeptics.17 On the basis of this study, proton pump inhibitors may be less effective after cure of infection. However, this needs to be tested in another trial but for now it is yet another argument against H pylori treatment in functional dyspepsia.
In conclusion, omeprazole 20 mg per day improved dyspeptic symptoms in patients infected with H pylori to a greater extent than in those who were H pylorinegative. The effect was relatively weak however, and identification of those patients who are likely to respond requires additional studies.
Acknowledgments
We are grateful to Dr Madeline Frame for expert assistance with the manuscript preparation. Supported by Swiss Science Research Foundation, grant No 31-43240.95, and by Astra-Hässle, AB, Sweden.
FROSCH STUDY GROUP
Werner Abels (Nürnberg), Krikor Amdja (Wermelskirchen), Walter Armknecht (Worms), Amelie Arnold (Marburg), Herbert Bock (Frankfurt), Dibor Bojanovski (Hannover), Hilmar Böneke (Lienen), Hubert Brinkhoff (Stuhr), Burkhardt Cyrus (München), Axel Dettmer (München), Reinhard Diedrich (Marburg), Klaus Dietrich (Saarbrücken), Bernhard Dirr (Hechingen), Wolfgang Dübel (Berlin), Michael Dudek (Düsseldorf), Dieter Ebbinghaus (Lünen), Horst Feyerabend (Hagen), Wolfgang Fortelny (Waldsassen), Frank Fueting (Nassau), Meinolf Golsong (Oberhausen), Roland Graf (Leutkirch), Wolfgang Güttel (Rastatt), Hans-Jürgen Hagel (Schwabach), Bernt Hawickhorst (Wülfrath), Martin Hell (Salzgitter-Lebenstedt), Rüdiger Hildebrandt (Clausthal-Zellerfeld), Gert-Heintz Hirschmann (Berlin), Andreas Hoffmann (Magdeburg), Walter Hofmeister (Weiden), Hermann Hornstein (Pfullingen), G. Hornung (Essen), Wolfgang Huppertz (Essen), Harvey Juergens (Ölde), Bernhard Klesser (Ulm), Horst Klewer (Wetzlar), Michael Klöters (Spaichingen), Andreas Kocjan (Lüdenscheid), Justine Kosmowski (Frankfurt), Thomas Krummenerl (Münster), Joachim Labenz (Essen), Günter Leiber (Marburg), Christian Leischik (Köln), Helmut Lichti (Gladenbach), Albin Lütke (Koblenz), Andrei Mares (Frankfurt), Eckard Massmann (Münster), Peter Mayr (Stockach), Bernd Metscher (Berlin), Heinrich Miks (Hamm), Hubert Mönnikes (Marburg), Michael Müller (Delmenhorst), Claus Nolte (Mettmann), Paul-Peter Pech (Münster), Wilhelm Peters (Duisburg), Stefan Pfäffl (Nürnberg), Thomas Rachel (Rastatt), Axel Rambow (Frankfurt), Gerd Rosprich (Saarbrücken), Thomas Schädlich (Ellefeld), Jost Schattenberg (Wiesbaden), Dieter Schlauch (Ludwigshafen), Volker Schmid (Fürstenzell), Andreas Schober (Göttingen), Michael Schumacher (Wolmirstedt), Erich Schütz (Regensburg), Rainer Stroband (Münster), Gerard Tangerding (Wangen), Peter Tippmann (Esslingen), Huschang Toluipur (Schiffweiler), Rüdiger Vogt (Mannheim), Rainer Wack (Berlin), Hannelore Wiechmann (Potsdam), Günter Wilhelms (Goslar), Friedrich Winter (Burgebrach), Jürgen Zeus (Erlangen).
Abbreviations used in this paper
- QoL
- quality of life
- ITT
- intention to treat
- PP
- per protocol
References
Footnotes
↵† Details of the Frosch Study Group are given in the .
Linked Articles
- Commentary