Article Text

Abstract
BACKGROUND Perinuclear antineutrophil cytoplasmic antibodies (pANCA) have been detected in a clinically distinct Crohn's disease subpopulation. Antibodies toSaccharomyces cerevisiae (ASCA) have been demonstrated in the majority of patients with Crohn's disease.
AIMS To examine the relationship between selective marker antibody expression in Crohn's disease and disease onset, location, and clinical behaviour patterns.
METHODS Sera from 156 consecutive patients with established Crohn's disease were evaluated in a blinded fashion for the presence of ASCA and ANCA. Clinical profiles were generated by investigators blinded to immune marker status.
RESULTS Using multiple regression analyses, higher ASCA levels were shown to be independently associated with early age of disease onset as well as both fibrostenosing and internal penetrating disease behaviours. Higher ANCA levels were associated with later age of onset and ulcerative colitis-like behaviour. Substratification of the Crohn's disease population using selective ANCA and ASCA expression (high levels of a single marker antibody): (1) distinguished homogeneous subgroups that manifested similar disease location and behaviours; and (2) identified patients with more aggressive small bowel disease.
CONCLUSIONS The findings suggest that by taking into account the magnitude of the host immune response, Crohn's disease can now be stratified on an immunological basis into more homogeneous clinically distinct subgroups, characterised by greater uniformity among anatomical distribution of disease and disease behaviour.
- antineutrophil cytoplasmic antibody
- anti-Saccharomyces cerevisiae antibody
- Crohn's disease
- inflammatory bowel disease
- ulcerative colitis
Abbreviations used in this paper
- ASCA
- anti-Saccharomyces cerevisiae antibody
- CD
- Crohn's disease
- ELISA
- enzyme linked immunosorbent assay
- EU
- ELISA units
- IIF
- indirect immunofluorescent
- IBD
- inflammatory bowel disease
- pANCA
- perinuclear antineutrophil cytoplasmic antibodies
- UC
- ulcerative colitis
- TNF
- tumour necrosis factor
- PNPP
- p-nitrophenol phosphate
- Ig
- immunoglobulin
Statistics from Altmetric.com
- antineutrophil cytoplasmic antibody
- anti-Saccharomyces cerevisiae antibody
- Crohn's disease
- inflammatory bowel disease
- ulcerative colitis
Many variations in the clinical presentation and natural history of Crohn's disease (CD) have been recognised since the original descriptions in the early part of this century.1What is classically termed “Crohn's disease” may actually represent a heterogeneous group of diseases manifesting similar features.2-5 Numerous attempts have been made to characterise CD patients into uniform subgroups to better understand and predict clinical courses and responses to medical and surgical interventions. To date, most stratification analyses have focused on the anatomical distribution of inflammation and fibrostenosing or perforating/fistulising behaviour patterns. Such classifications are descriptive and have not been shown to reflect specific pathogenic mechanisms.
Serum immune markers have been used to characterise subgroups of patients with ulcerative colitis (UC) and CD. Antineutrophil cytoplasmic antibodies (ANCA), autoantibodies directed against intracellular components of neutrophils, are present in the majority of UC patients and in a clinically distinct CD subpopulation.6 ANCA expression in UC permits stratification at the mucosal, clinical, and genetic levels, and has been associated with distinct disease subgroups.7-14 UC associated ANCA exhibit perinuclear highlighting (pANCA) on indirect immunofluorescent (IIF) microscopy. The pANCA of UC loses the characteristic perinuclear IIF staining pattern when pretreated with DNase.15 Serum pANCA is thought to reflect mucosal pANCA production, and studies have shown that B cell priming and pANCA production take place in the colonic mucosa. These findings imply that recognition of mucosal antigen(s) leads to local production of pANCA.7 In relatively small studies, pANCA in UC has been associated with the clinical features of: (1) treatment resistant left sided disease8; (2) aggressive disease course9 ,10; (3) surgery early in the disease course11; and (4) development of pouchitis following ileal pouch-anal anastomosis.12-14 Genetic studies have suggested that subpopulations of UC can be defined by ANCA expression in association with specific HLA markers.16-18 In UC, pANCA production may reflect a distinct mucosal inflammatory process and thereby represents immunologically distinct subpopulations.
pANCA expression in CD provides additional evidence that pANCA is a marker of a distinct mucosal inflammatory process. CD patients expressing pANCA have clinical features of left sided colitisand endoscopic and/or histopathological features typical of UC.6 This “UC-like” phenotype has been confirmed in several studies.18-20 Additionally, the serum immunoglobulin G (IgG) subclass profile of pANCA+ CD is similar to that of UC.21 Thus in CD the presence of serum pANCA suggests a mucosal inflammatory process in common with the UC pANCA subgroup.
Antibodies to Saccharomyces cerevisiae(ASCA) have been detected in up to 79% of CD patients.22Expression of this marker antibody may also reflect a specific mucosal immune mediated response. Sendid et aldemonstrated that yeast cell wall phosphopeptidomannans were the epitopes responsible for the antigenic reactivity in ASCA+CD sera.23 Mannans are believed to be the major antigenic component of yeast cell walls and are an important antigenic constituent of mycobacteria and other microorganisms.24The clinical significance of ASCA expression in CD is not well defined. However, Darroch et al demonstrated that soluble preparations of S cerevisiae can induce a lymphoproliferative response in vitro, similar to that of known recall antigens.25 Taylor et al described the association of ASCA with the tumour necrosis factor (TNF) microsatellite haplotype a11b4c1d3e3 in patients with inflammatory bowel disease (IBD).26 These findings suggest that a gene related to ASCA expression resides on chromosome 6 within the major histocompatibility complex in the vicinity of this haplotype. A mutation located on the haplotype may be contributing to ASCA expression. Taken together, these findings raise the possibility that ASCA expression, in common with pANCA, may reflect specific mucosal immune mechanisms.
Selective marker antibody expression has been used to differentiate between UC and CD, but ASCA and ANCA have not been used to stratify CD subgroups.17 ,27 The aim of this study was to examine the association between clinical characteristics and ASCA and/or pANCA expression in CD patients. The results demonstrated that in this referral centre cohort, higher ASCA levels were associated with earlier age of disease onset of CD and both fibrostenosing and internal penetrating disease behaviours. In contrast, higher ANCA levels were associated with an older age of disease onset and a UC-like inflammatory response. Therefore, subgroups of CD patients stratified based on age of onset and clinical characteristics may represent immunologically distinct groups.
Methods
STUDY POPULATION
The study population consisted of 156 consecutive patients with an established diagnosis of CD evaluated at the CSMC IBD Center, who consented to donate serum for research purposes. This study was reviewed and approved for human subject participation by the Cedars-Sinai Institutional Review Board. Patients with primary sclerosing cholangitis, autoimmune hepatitis, and those with chronically elevated transaminases or alkaline phosphatase were excluded to avoid confusion with non-IBD ANCA.28 ,29Diagnosis of CD was defined by the presence of a combination of established features from at least two of the following categories: (1)clinical—perforating or fistulising disease, obstructive symptoms secondary to small bowel stenosis or stricture; (2) endoscopic—deep linear or serpiginous ulcerations, discrete ulcers in normal appearing mucosa, cobblestoning, discontinuous or asymmetric inflammation; (3)radiographic—segmental disease (skip lesions), small bowel or colon strictures, stenosis, or fistula; and/or (4) histopathological—submucosal or transmural inflammation, multiple granulomas, marked focal cryptitis or focal chronic inflammatory infiltration within and between biopsies, or skip lesions including rectal sparing in the absence of local therapy.
ASSESSMENT OF CLINICAL CHARACTERISTICS
Clinical assessment and serum immune marker evaluations were performed independently and before data analysis. Clinical information was collected by chart review and patient interview by clinical investigators blinded to individual patient ANCA and ASCA status. Detailed patient profiles were generated using the database intake forms currently in use at the CSMC IBD Center. Epidemiological data included: age, age of IBD symptom onset, disease duration, sex, ethnicity, and family history of CD or UC. Signs and symptoms associated with active CD were noted, including: obstructive symptoms, diarrhoea, bleeding and mucus discharge, urgency, tenesmus, aphthous ulcerations, perianal abscesses or fistulae, anal fissures or strictures, as well as extraintestinal manifestations of IBD. For each patient, the specific anatomical location of all documented areas of endoscopic, surgical, histopathological, or radiographic inflammation, stricturing, fistulisation, perforation, or abscess formation were recorded. Location of disease was further grouped into the standard categories of “small bowel disease only,” “small bowel and colonic disease,” and “colonic involvement only.” Clinical behaviour patterns were characterised as fibrostenotic, penetrating, and/or “UC-like.” To be classified as having “fibrostenotic disease” patients needed appropriate radiographic, endoscopic, surgical, or histopathological documentation. Patients with CD related fistulae, abscesses, or perforations were described as having “penetrating disease” and were further substratified into “internal” or “perianal” penetrating disease. CD related fistulae to the urinary tract and to the skin (other than perianal) were considered internal. Vaginal fistulae communicating with the rectum were grouped with perianal fistulae. Fistulae, abscesses, or perforations resulting from surgical complications were not included as “penetrating disease.” CD patients were considered “UC-like” if they exhibited clinical features of left sided colonic disease and endoscopic and/or histopathological features of UC as previously described.6 Because it is recognised that CD behaviour patterns are not mutually exclusive and can coexist within a given individual, a single patient may thus be represented in more than one behaviour analysis. The number, types, and reason for all IBD related surgeries were recorded. Pharmacological interventions were grouped to reflect the use of sulfasalazine or oral 5-aminosalicylic acid derivatives, immunomodulatory agents (6-mercaptopurine, azathioprine, methotrexate, mycophenolate, cyclosporin, FK506, anti-TNF-α, interleukin-10), IBD directed antibiotic therapy, and topical therapies for distal colonic disease (enemas, foams, or suppositories).
SERUM ANCA DETERMINATION AND ANCA SUBTYPE CHARACTERISATION
Serum ANCA expression and ANCA subtype characterisation were performed in a blinded fashion by Prometheus Laboratories (San Diego, California, USA). ANCA presence was determined by fixed neutrophil enzyme linked immunosorbent assay (ELISA) as previously described.30 Polystyrene microtitre plates were coated with 2.5×105 normal human donor whole peripheral blood neutrophils per well, which were fixed with 100% methanol. Cells were incubated with bovine serum albumin (0.25%) in phosphate buffered saline to block non-specific antibody binding. Next, control and coded sera were added at a 1:100 dilution. Following incubation and washing, goat F(ab′)2 antihuman immunoglobulin G (γ chain specific) antibody (Jackson Immunoresearch Labs, Inc., West Grove, Pennsylvania, USA) conjugated to alkaline phosphatase was added at a 1:1000 dilution to label neutrophil bound antibody. Substrate solution containing p-nitrophenol phosphate (PNPP) was then added. Colour development was allowed to proceed until absorbance at 405 nm in the positive control wells was 0.8–1.0 optical density units greater than that in blank wells, using a reference wavelength of 650 nm on a Molecular Devices (Menlo Park, California, USA) E-Max microtitre plate reader. Levels were determined relative to a Prometheus laboratory standard consisting of pooled sera obtained from well characterised pANCA+ UC patients. Results were expressed as ELISA units (EU/ml). Sera with circulating antineutrophil cytoplasmic IgG antibody exceeding the normal reference range value were termed “ANCA+.” Numeric values below the normal reference range were termed “ANCA−”.
ANCA+ sera were further subtyped via IIF staining to determine the ANCA neutrophil binding pattern. Glass slides containing approximately 105 normal human donor whole peripheral blood neutrophils per slide were prepared by cytocentrifugation (Shandon Cytospin, Cheshire, UK). Cells were fixed in 100% methanol, air dried, and stored at −20°C. The coded patient sera were diluted (1:20) and then layered over the fixed neutrophils, incubated at 37°C, and washed. Fluorescein labelled F(ab′)2 γ chain specific goat antihuman antibody was added and incubated and washed, as previously described.30 The sections were examined by fluorescence microscopy using an epifluorescence equipped Nikon microscope (Garden City, New Jersey, USA). Sera exhibiting the characteristic perinuclear highlighting that then lost this characteristic staining pattern when first treated with DNase were termed “pANCA+”.15
DETERMINATION AND CHARACTERISATION OF SERUM ASCA
Sera were analysed for ASCA expression in a blinded manner by Prometheus Laboratories using a fixed ELISA assay. High binding polystyrene microtitre plates were coated with purified phosphopeptidomannans extracted from yeastSaccharomyces uvarum, a subspecies of S cerevisiae. Coded patient sera were diluted and added to the wells. Following incubation and washing, alkaline phosphatase conjugated goat antihuman F(ab′) fragment specific IgG (Pierce, Rockford, Illinois, USA) or alpha chain specific IgA (Jackson) was added. After incubation, wells were washed, and PNPP substrate was added. Colour development was proportional to concentrations of antibody present in sera. Samples were read at 405 nm with a reference wavelength of 650 nm on a Molecular Devices E-Max microtitre plate reader. Levels were determined and results expressed as ELISA units (EU/ml) relative to a Prometheus laboratory standard which was derived from a pool of patient sera with well characterised CD found to have reactivity to this antigen. Sera exhibiting ASCA reactivity (IgG and/or IgA) exceeding the normal reference range were termed “ASCA positive” (ASCA+).
STATISTICAL ANALYSIS
Statistical analyses were performed using SAS computer software (Release 6.10; SAS Institute, Inc., Cary, North Carolina, USA, 1994). Both quantitative ASCA and ANCA—that is, antibody levels—and qualitative ASCA and ANCA—that is, antibody positivity and ANCA pattern—were used in analyses. Logarithmic transformation was performed for ASCA and ANCA levels (including those below the reference range) to obtain a more ready normal distribution before correlation was computed and statistical tests performed. Actual numeric values were used when analysing serum immune marker levels as quantitative variables. In practice, ASCA positivity was determined by either IgG or IgA being positive. Similarly, to obtain one measure for a quantitative ASCA level, we used both IgG and IgA values by selecting the larger one of the two standardised values (IgG' or IgA'), where IgG'=[lnIgG–mean(lnIgG)]/SD(lnIgG) and IgA'=[lnIgA–mean(lnIgA)]/SD(lnIgA). Correlations between normalised variables were evaluated by Pearson correlation coefficients and corresponding p values. To evaluate the relationship between serum ANCA and ASCA and clinical features, linear multiple regression analysis was performed by specifying antibody levels as dependent variables and clinical characteristics as independent variables using a stepwise procedure. To further corroborate the independent variables identified as significant by multiple regression analysis, an additional analysis was performed examining those populations expressing high levels of a single marker antibody. Because there was a significant overlap of ANCA and ASCA, levels⩾50 EU/ml were chosen for ASCA and levels⩾40 EU/ml for ANCA to allow for a sufficient number of patients for analysis while eliminating patients expressing only low levels of this marker. To test mean differences in normalised quantitative variables between any two groups, the Student'st test was used; between multiple groups, one way ANOVA was used followed by pairwise Fisher's least significant difference test for means. p values for such pairwise tests were adjusted for multiple comparisons. The non-parametric Kruskal-Wallis test was used to compare numbers of small bowel surgeries between groups.
Results
ANCA EXPRESSION AND IMMUNOFLUORESCENCE STAINING PATTERNS IN CD PATIENTS
In this study, using a well defined CD population and optimised technology, ELISA screening detected serum ANCA above the reference range in 56% (87/156) of patients. Forty one per cent (36/87) of CD patients expressing ANCA exhibited a perinuclear highlighting pattern (pANCA) on IIF staining. To further characterise the pANCA of CD patients, all pANCA+ CD sera were analysed by pretreatment of neutrophils with DNase and reassessed for the resulting ANCA IIF staining pattern. Complete loss of antigen recognition following treatment with DNase (P→Ø) was observed in 78% (28/36) of pANCA+ samples. Fourteen per cent (5/36) converted to a homogeneous cytoplasmic staining pattern (P→C). Three of 36 (8%) retained the perinuclear highlighting pattern (P→P). The proportion of DNase sensitive pANCA CD serum samples converting from P→Ø and from P→C was similar to that seen in the pANCA+ UC population (70% and 30%),15 and provides evidence that pANCA of CD is the same as pANCA of UC.
The reported prevalence of ANCA expression in CD has varied greatly due to differences in study populations and detection methodology. In most other reports of ANCA in IBD, ANCA expression was detected by IIF alone. In this study, ANCA expression was determined by ELISA, with assessment of neutrophil staining pattern by IIF, and finally confirmation by DNase digestion of neutrophils. Therefore, in this paper all subsequent references to “pANCA” should be interpreted as DNase sensitive pANCA with loss of antigen recognition following pretreatment with DNase (P→Ø or P→C). ELISA levels of ANCA were highest in the pANCA+ subgroup (mean (SEM): 72 (10) EU/ml) compared with the non-pANCA+ subgroup (25 (2) EU/ml), and those that were ANCA− (10 (1) EU/ml) (pχ2 for trend < 0.0001).
IgG AND/OR IgA ASCA EXPRESSION DISTINGUISHES CD SUBGROUPS
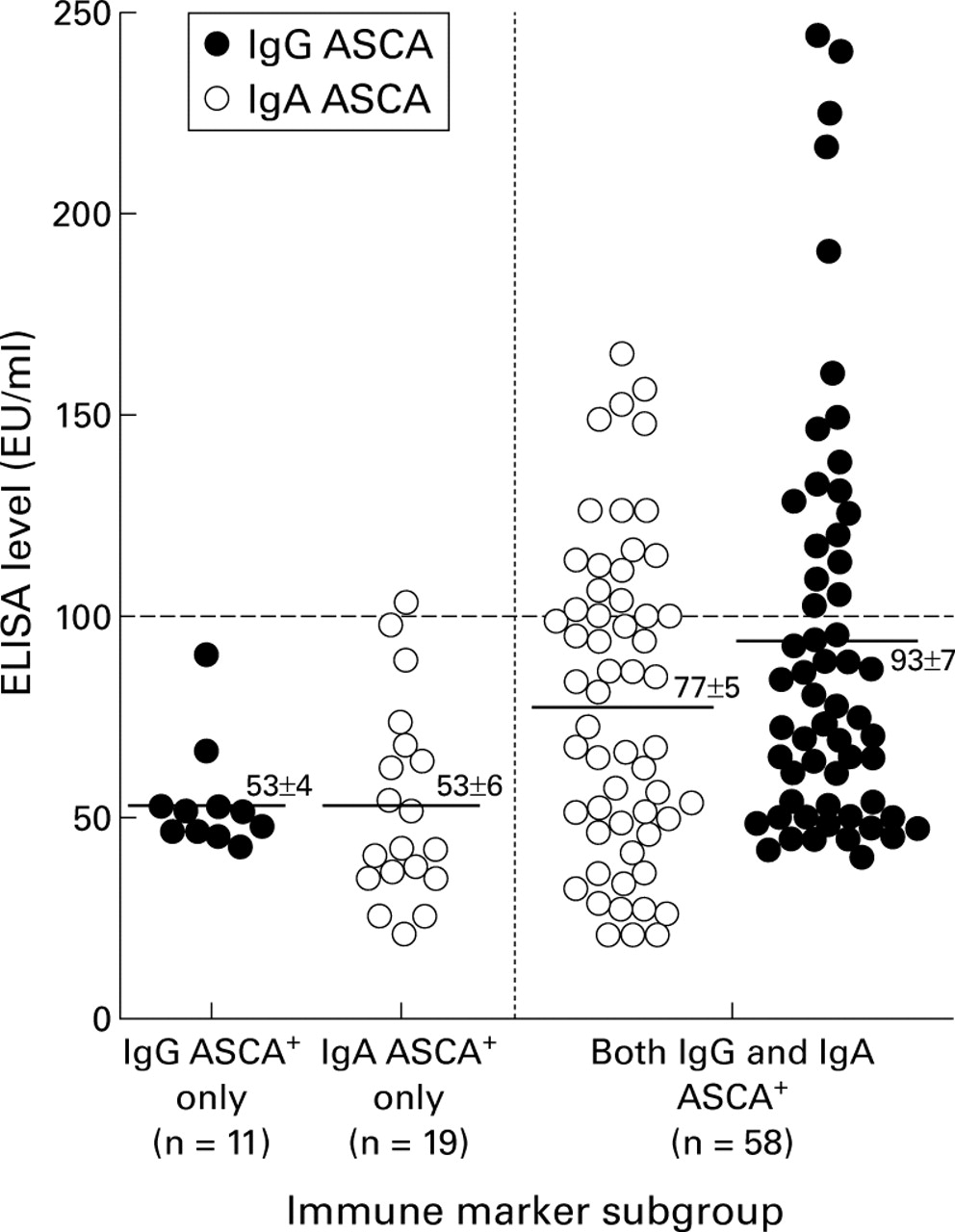
Using a purified antigen preparation and an ELISA optimised for antibody detection, IgG and IgA serum antibodies toSaccharomyces cerevisiae (ASCA) were detected above the reference range in 56% (88/156) of the CD study population. Of the ASCA+ patients, 13% (11/88) expressed IgG ASCA alone, 22% (19/88) expressed IgA ASCA alone, and 66% (58/88) expressed IgG and IgA ASCA. Patients with both IgG and IgA ASCA had higher mean (SEM) quantitative levels (IgG ASCA 93 (7) EU/ml; IgA ASCA 77 (5) EU/ml) than patients expressing exclusively IgG ASCA (53 (4) EU/ml) (p=0.039) or IgA ASCA (53 (6) EU/ml) (p=0.10) (fig 1). Figure 1 also illustrates that almost all patients (25/26) expressing the highest levels of either IgG or IgA ASCA (⩾100 EU/ml) were part of the CD subgroup expressing both IgG and IgA ASCA.
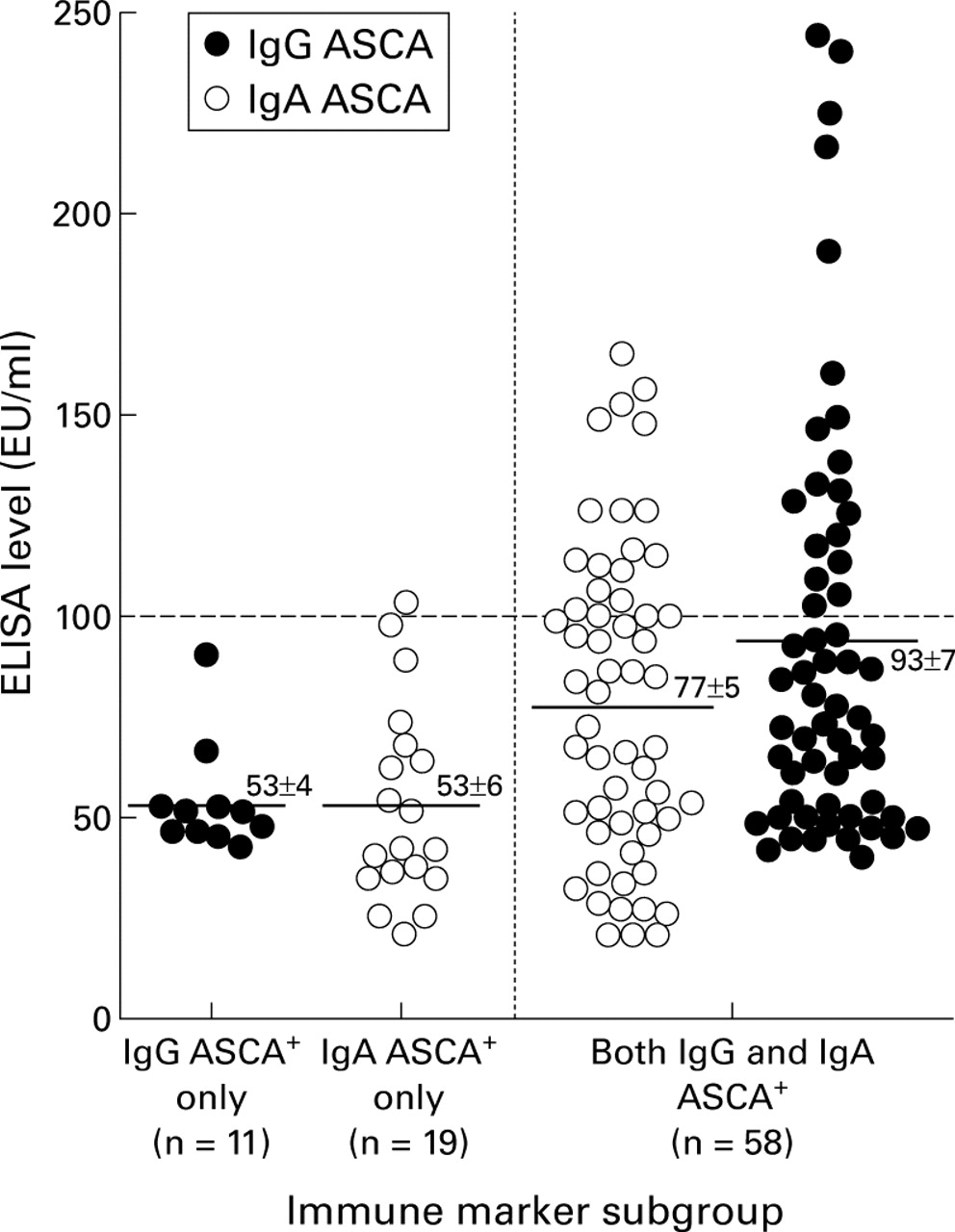
Levels of anti-Saccharomyces cerevisiae antibody(ASCA) positive sera from the Crohn's disease (CD) population. The solid line in each group represents the mean of the subgroup. Almost all patients (25/26) expressing the highest levels of either IgG or IgA ASCA (⩾100 EU/ml, values above the broken line) were part of the CD subgroup expressing both IgG and IgA ASCA.
RELATIONSHIP AMONG MARKER ANTIBODY LEVELS
As there was great variation in levels of marker antibody expression among CD patients, we examined the relationship between levels of marker antibody expression. There was a significant positive correlation between IgG ASCA and IgA ASCA levels (r=0.72, p=0.0001) and a negative correlation between IgA ASCA and ANCA levels (r=−0.21, p=0.009). The correlation between IgG ASCA and ANCA levels was also negative (r=−0.13) but did not attain statistical significance (p=0.11). Thus an inverse relationship between ANCA and ASCA levels within this CD patient cohort was suggested (that is, the higher the ASCA level, the lower the ANCA level). This inverse relationship suggests that the presence and levels of a specific marker antibody could reflect distinct immunological reactivity leading to differences in clinical expression among CD patients.
RELATIONSHIP BETWEEN MARKER ANTIBODY EXPRESSION AND LEVEL AND DEMOGRAPHIC CHARACTERISTICS WITHIN CD PATIENTS
Multiple investigations have demonstrated that serum and genetic markers can be correlated with identifiable CD phenotypes.6 ,18-20 ,27 ,31-35 The demographic variables of sex, current age, Jewish ancestry, and family history of CD, UC, or IBD in general, were compared between antibody marker subgroups (table1). Except for age, there were no significant differences either between ASCA+ and ASCA− subgroups or among pANCA+, other ANCA+, and ANCA− subgroups. Although more ASCA+ patients (88%) had been treated with immunosuppressive therapies than those that were ASCA− (72%) (p<0.0001), this referral centre cohort as a whole had severe disease, as reflected by the use of immunosuppressive interventions in 81% of patients overall.
Demographic features of the Crohn's disease study population stratified by ANCA and ASCA expression
Age of onset
The majority of epidemiological studies examining age of presentation suggest a bimodal age distribution in CD.36-39 To begin to assess whether clinical differences between childhood and adult onset CD in disease distribution and clinical course40-47 may be associated with different immune responses, we examined the relationship between age of onset of CD and expression of these immune markers. Patients in whom ASCA was detected experienced onset of IBD symptoms significantly earlier in life than patients not expressing ASCA (mean (SEM) 22 (1)v 29 (2) years, respectively) (p<0.0001) (table 1), corroborating previous observations by Quinton and colleagues.27 In fact in a multivariate analysis of ASCA levels (see methods) there was a significant correlation with early age of onset (p<0.005). As current age is not independent of patient's age at disease onset and/or duration of disease, we examined these three age related factors together using multiple regression analysis to evaluate which factor had the primary association with levels of IgG or IgA ASCA. Age of onset was shown to be independently associated with levels of both IgG and IgA ASCA but not current age or duration of disease. The negative correlation between IgG and IgA ASCA levels and age of onset of CD (IgG r=−0.33, p=0.0001; IgA r=−0.30, p=0.0002) provides further evidence for the association of this immune response with younger age of onset. The effect of age of onset on expression of ASCA, and ANCA expression and levels in patients with pre-teenage (age <13 years) onset of CD was compared with marker expression in patients with late adult onset (age >40 years) CD (age >40 has been described as the start of the second peak age for onset of CD).36-39 As depicted in table 2, 73% (16/22) of patients with pre-teenage onset of CD were ASCA+ compared with 59% (65/110) of patients with onset between 13 and 40 years, and only 29% (7/24) of patients with disease onset after age 40 years (pχ2 for trend<0.003). Although the per cent of CD patients expressing pANCA did not vary significantly with age of onset, there was a tendency towards higher levels of ANCA expression with increasing age of onset (p=0.019). Early and late onset CD may have distinct immunological responses.
Age at onset of Crohn's disease stratified by ANCA and ASCA expression
RELATIONSHIP BETWEEN MAGNITUDE OF MARKER ANTIBODY EXPRESSION AND CLINICAL FEATURES OF CD
The variability of levels of ASCA (fig 1) and ANCA expression and the inverse relationship of these marker antibodies within this cohort led to analysis of the relationship between levels and clinical features. ASCA (IgG or IgA) and ANCA were measured as a continuous trait (that is, levels). To increase the statistical power and evaluate the relationship between antibody expression and clinical features of CD in an objective manner, we first conducted a multiple regression analysis using the quantitative ASCA or ANCA level as a dependent variable and all clinical features as independent variables, including anatomical distribution of disease and disease behaviours (fibrostenosing, internal penetrating, perianal penetrating, and UC-like).
Table 3 lists the clinical features that showed significant association with either ASCA or ANCA. As overall ASCA positivity was determined by the presence of either the IgG or IgA ASCA isotype, we used both IgG and IgA values by selecting the larger one of the two standardised values (as described in methods). Higher levels of ASCA were associated with fibrostenosing disease, internal penetrating disease, and less often UC-like features (table 3). In contrast, higher levels of ANCA levels were associated with UC-like features only (table3).
Clinical features: results of multivariate analysis
The presence of each of these serum immune markers has been associated with disease location.6 ,18 ,19 ,27 ,31 ,32 In this cohort, the presence of pANCA was associated with colonic involvement (88%; 29/33) and ASCA with small bowel involvement (alone or in combination with colonic disease) (90%; 79/88). Ileal involvement was seen in all 79 patients; 93% (64/69) and 90% (69/77) of IgG ASCA+ and IgA ASCA+, respectively. However, whenlevels of these serum immune markers were analysed with respect to disease location, there was no independent association.
SUBSTRATIFICATION USING SELECTED EXPRESSION OF IMMUNE MARKERS FURTHER CHARACTERISES DISTINCT CLINICAL PHENOTYPES IN CD
In this study the associations with behavioural manifestations in CD became more evident at higher levels of both marker antibodies. Higher levels of ASCA expression were associated with the traditional “classic” fibrostenosing and internal fistulising features of CD, while higher levels of ANCA were associated with UC-like features. This demonstrates that not only the type, but also the magnitude of the immune marker expression (as measured by level of host marker antibody production) may reflect divergent immune responses that manifest as specific disease behaviours (phenotypes) in these subsets of CD patients.
To further evaluate this hypothesis, we examined those populations expressing high levels of a single marker antibody, that is: (1) high levels of ASCA without ANCA (IgA and IgG ASCA+ ⩾50 EU/ml and ANCA− ); and (2) high levels of pANCA without ASCA (pANCA+ ⩾40 EU/ml and ASCA−). Because there was a significant overlap of ANCA and ASCA, levels⩾50 EU/ml were chosen for ASCA to allow for a sufficient number of patients to be analysed while eliminating patients expressing only low levels of this marker. As illustrated in fig 2, all patients with IgA and IgG ASCA+⩾50 EU/ml and the ANCA−immune marker subprofile had developed fibrostenosis (14/14; 100%). Most experienced internal penetrating complications (11/14; 79%); only 14% (2/14) had UC-like features. In contrast, 86% (12/14) of pANCA+ ⩾40 EU/ml and ASCA− CD patients exhibited UC-like features while only 14% (2/14) of patients in this subgroup had fibrostenotic disease and 29% (4/14) had internal penetrating disease. Fibrostenosing and internal penetrating behaviours have been considered by some to be indicators of a more aggressive form of small bowel CD.48-54
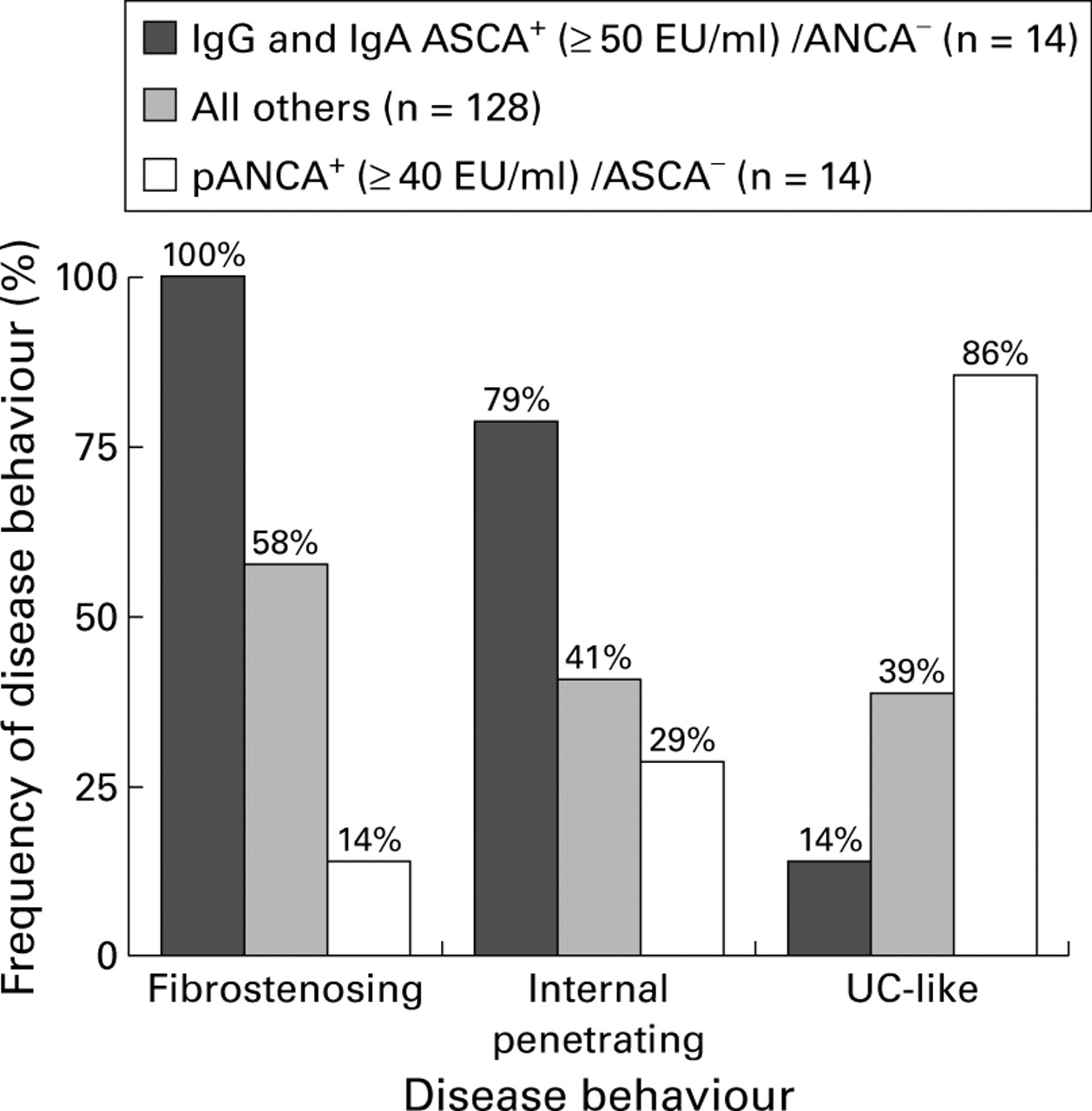
Substratification using selected expression of immune markers. Disease behaviour characteristics were examined in more immunologically homogeneous subgroups of patients with Crohn's disease (CD) (those expressing high levels of a single marker antibody) and compared with all other CD study patients. Overall differences in proportions were evaluated using the χ2 test for trend (p<0.001 for each of the disease behaviour characteristics).
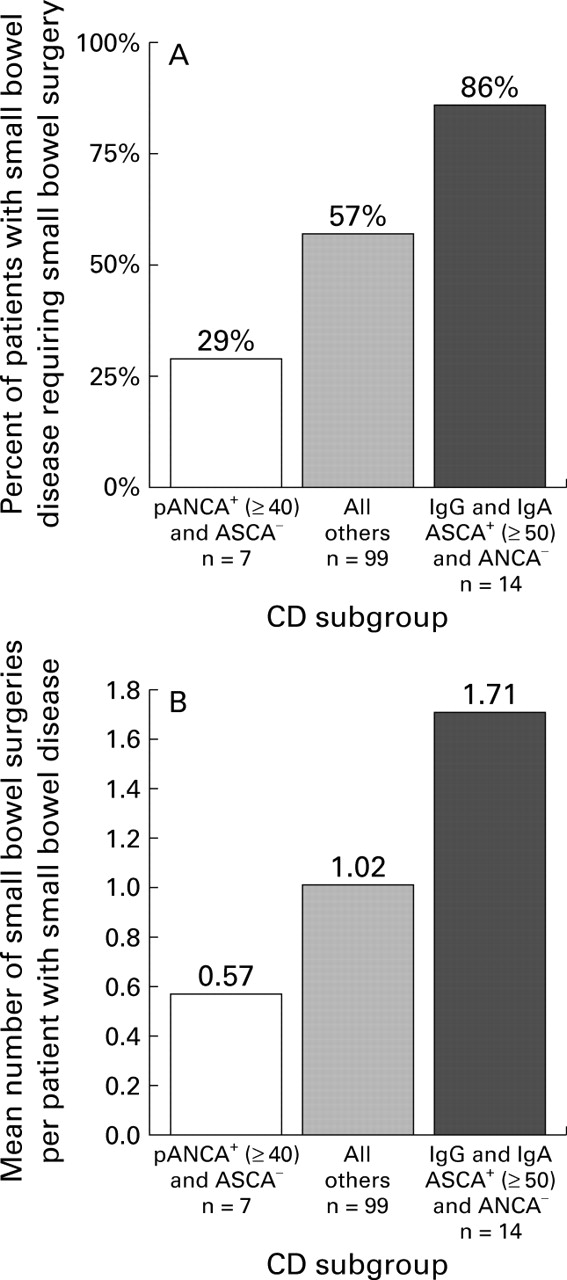
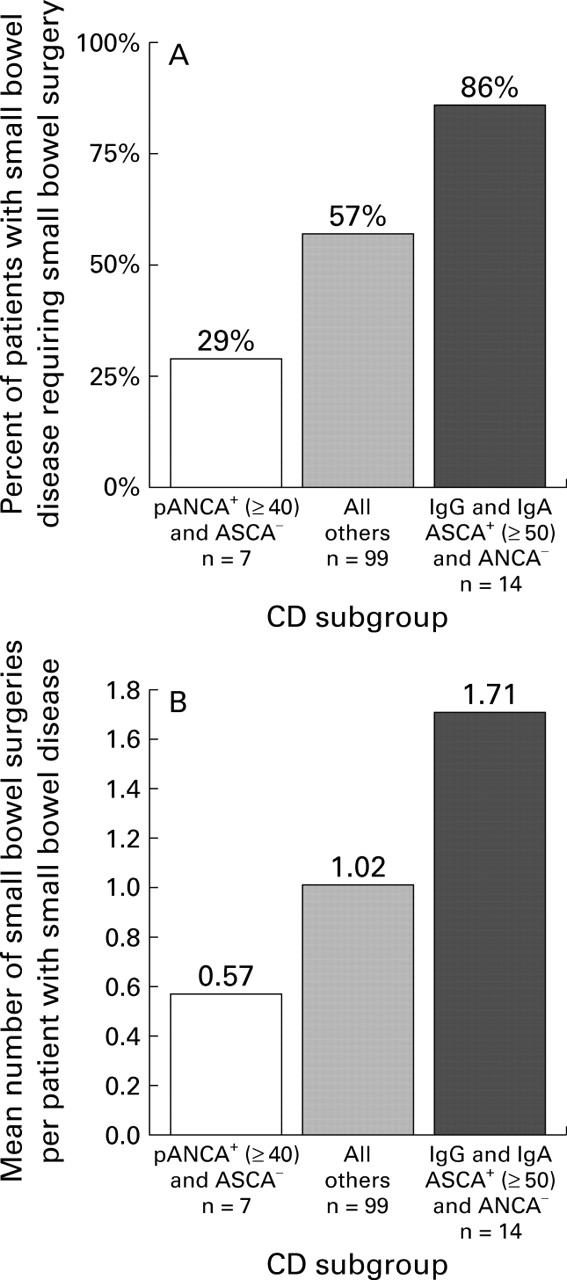
The need for small bowel surgery or recurrent surgeries has been suggested as a further measure of disease severity. To take into account the observation that the incidence of small bowel disease varied between immune marker subgroups, we examined prevalence and numbers of surgeries per patient among those with small bowel involvement (alone or in combination with colonic disease). Analysis revealed that small bowel surgery was required by 86% (12/14) of the IgA and IgG ASCA+ ⩾50 EU/ml and ANCA−subgroup (fig 3A). This was significantly more than the pANCA+ ⩾40 EU/ml and ASCA− group (2/7; 29%) and the remainder of the study patients with small bowel involvement (56/99; 57%) (p=0.0001). Additionally, the mean number of small bowel surgeries per patient with small bowel disease was higher in the IgA and IgG ASCA+ ⩾50 EU/ml and ANCA− (1.71/patient) subgroup than in the pANCA+ ⩾40 EU/ml and ASCA−subgroup (0.57/patient) and all others (1.02/patient) (p=0.0054) (fig3B). Therefore, higher levels of ASCA without ANCA may reflect more aggressive small intestinal disease.
{kind=link}
{kind=link}
{kind=link}
Surgery as a measure of disease aggressiveness. Substratification of the subset of patients with small bowel disease (Crohn's disease (CD) involving the small bowel alone or in combination with the colon) using selective immune marker expression. (A) Percentage of patients requiring small bowel surgery and (B) total number of small bowel surgeries per patient with small bowel involvement. Overall differences in proportions were evaluated using the χ2 test for trend. (A: p<0.0001; B: p<0.005).
Discussion
We have demonstrated that serum ASCA and ANCA status are criteria by which patients with CD can be stratified into distinct clinical subgroups. Levels of ASCA were independently associated with earlier age of onset of CD and a tendency towards developing classic fibrostenosing and internal penetrating small bowel complications (table 3). In contrast, higher levels of pANCA were associated with later age of onset and a UC-like inflammatory response, as well as a relative lack of fibrostenosis and penetrating disease (table 3). Finally, the concept of substratifying the CD population using selective ANCA and ASCA expression was demonstrated as a complementary approach for identification of immunologically and clinically homogeneous subgroups (fig 2), including a group with a more aggressive disease course (figs 2, 3A, 3B). Most studies that have examined expression of marker antibodies in IBD have focused on the presence or absence of the particular antibody and the presence or absence of what we currently term “UC” or “CD”.6 ,18 ,19 ,23 ,27 ,30 Our study revealed that the presence of these marker antibodies and the magnitude of the host immune response correlated with distinct, and indeed divergent, clinical characteristics, and suggests that ASCA and pANCA are serum markers for different mucosal inflammatory mechanisms that influence disease expression.
Of the patient characteristics evaluated, age of disease onset correlated strongly with disease behaviour and anatomical location. It has been observed that childhood onset CD is characterised by a greater prevalence of small bowel disease and stricturing/penetrating complications compared with late onset which is associated with more colonic disease and a lower incidence of fistula formation.44 Other studies suggest that childhood onset CD has a more aggressive course40 ,41 while older onset is associated with a comparatively favourable prognosis, better response to medical therapies, and lower risk of recurrence in the minority requiring surgery.39 ,45-47 The results of our study corroborate these clinical observations. In this CD cohort early disease onset was associated with increased incidence of small bowel involvement and fibrostenotic, as well as internal perforating complications (data not shown). In contrast, CD limited to the colon and UC-like features were more frequent in late onset CD, with the disease course less often complicated by fibrostenosis or internal perforating complications (data not shown). These differences in disease location and behaviour pattern tendencies suggest that paediatric and later adult onset CD represent pathogenetically distinct forms of the disease.
The underlying pathogenetic mechanisms for these clinical differences observed between adult versus childhood onset CD remain unclear. Although familial clustering supports the role of genetic factors in the pathogenesis of paediatric and adult onset CD, additional factors must also be involved to account for the observed differences.55-60 It has been hypothesised that young children may be more immunologically reactive than older children or adults.61-63 Age dependent immune influences have been described in other immune mediated disorders.64-67 The results of this study provide evidence that age of onset associated with host dependent immune responses may influence intestinal location, phenotypic expression, and CD behaviour.
Disease location is another variable previously found to positively correlate with immunological markers such as ASCA and ANCA expression. Giaffer et al observed that patients with isolated small bowel involvement had significantly higher ASCA IgG titres against two strains of S cerevisiaethan those with colonic disease.31 In a study examining ASCA expression in monozygotic twins, Lindberg et al found higher IgG ASCA levels (to whole yeast) in patients with CD limited to the small bowel compared with those with both small bowel and colonic involvement.32 In contrast, several investigators have suggested that pANCA expression in CD is related to colonic disease which at minimum is left sided.6 ,18 ,19In the present study, we extended this observation, describing the importance of considering both pattern andquantitative levels of marker antibody expression when defining this association. Although the majority of ASCA+ patients had CD involving the small bowel and most pANCA+ patients had colonic involvement, levels of the serum immune markers were not independently associated with disease location.
Stratification based on CD behaviour has been widely studied and reported, often including an “inflammatory” behaviour in the analysis. All CD related behaviours are the result of inflammation, and therefore this variable was not included separately in the stratification analysis in this study. Higher levels of ASCA expression are associated with the well characterised subgroups of patients with the classic complications of fibrostenosing and internal penetrating disease. While perforating and non-perforating behaviours are clinically (and likely in some ways immunologically) distinct also, the observation that higher levels of ASCA expression are associated with both of these traditional “classic” fibrostenosing and internal penetrating features of CD suggests an overlapping mucosal mechanism rather than distinct mechanisms. In contrast, CD patients with higher ANCA levels experience these complications less frequently. Furthermore, with internal penetrating disease, no significant correlation was seen with these markers and perianal fistulising disease. This suggests that these two penetrating forms of CD involve different immunological mechanisms and may be considered not only clinically but immunologically distinct.
UC-like behavioural attributes were recently described as the predominant behaviour pattern common to the subgroup of CD patients expressing serum pANCA.6 ,18 ,19 This study extends previously reported observations. The incidence of UC-like behaviour was greatest at higher ELISA levels of pANCA expression and by exclusion of ASCA expression. The frequency of UC-like features in low level expression of pANCA was no different than in the overall population, emphasising the importance of taking into account the magnitude of the immune response. In this study sera were screened at 1:100 dilution, which may further explain why some studies that included low level pANCA expression have found less pronounced associations. These data strengthen the assertion that CD and UC pANCA subgroups share a similar mucosal immune response.
Based on our multiple regression analysis that defined the independently associated variables, ASCA and pANCA expression defined different host immune responses, each of which was associated with a different disease behaviour. Thus stratifying patients by expression of only one or the other marker antibody might better define specific clinical phenotypes. Furthermore, stratification by expression of pANCA or ASCA with the added variable of the magnitude of expression may better define subgroups of CD patients into more homogeneous clinical subsets. The use of this approach was demonstrated in this study. We found that the subset of CD patients that expressed higher levels of both IgG and IgA ASCA and not ANCA experienced a more aggressive course of disease. A precedent has been set in UC, where pANCA expression is associated with a more resistant disease course.8-14 The subset of patients that expressed higher levels of both IgG and IgA ASCA and not ANCA may have a more aggressive form of small bowel CD. Evidence in support of this characterisation include: (1) universal occurrence of fibrostenosis; (2) frequent development of internal penetrating complications; (3) observation that within the subset of all patients with small bowel disease a higher percentage of patients required small bowel surgery; and, (4) number of small bowel surgeries was three times higher in the IgA and IgG ASCA+ ⩾50 EU/ml and ANCA− subgroup than the pANCA+ ⩾40 EU/ml and ASCA− subgroup.
Conclusions
Our results demonstrate that Crohn's diseases can now begin to be stratified into distinct subgroups by pairing clinical features with the presence and levels of serum antibody markers. The study demonstrated the significance of taking into account the magnitude of the host immune response—that is, higher levels of ASCA and pANCA expression to identify CD subgroups that are immunologically and clinically more homogeneous. To approach the underlying mechanisms involved in the various forms of CD, clinical and genetic studies of CD must rely on homogeneous patient subgroups.52The use of ASCA and pANCA allows for identification of more homogeneous subgroups of patients with common subclinical and clinical characteristics, based on immune mechanisms of disease. Further corroboration of these results is warranted. In particular, the value of marker antibody determination performed at the time of diagnosis of IBD as a predictor of future disease behaviour expression needs to be evaluated in a prospective fashion. None the less, the immunological responses in IBD, as measured by marker antibody production, may well reflect different host genetic profiles.
Stratification of Crohn's diseases into more uniform subgroups using these and other immune markers may permit better characterisation and prediction of natural history. If these findings are reproduced in a clinically less severe population prospectively, this information could potentially allow for earlier and more aggressive treatment to avoid predictable complications in selected patients, without unnecessarily exposing others to potential adverse side effects of overaggressive therapeutic regimens. In addition, stratification based on markers will filter out the “background noise” inherent in studies of a heterogeneous group of diseases with similar characteristics. Stratified populations will facilitate the identification of pathogenically more homogeneous subsets of patients and perhaps identify “at risk individuals” in a group of diseases with complex genetic influences, including reduced penetrance or variable expression of disease.
Acknowledgments
The authors would like to acknowledge Rachel Kramer for data collection and interpretation. The study was supported by USPHS Program Project Grant DK46763, the Cedars-Sinai Inflammatory Bowel Disease Research Education Fund, the Feintech Family Chair in Inflammatory Bowel Disease, and the Cedars-Sinai Board of Governors' Chair in Medical Genetics.
Conflict of interest: Dr Stephan R Targan is a cofounder and current equity holder of Prometheus Laboratories (San Diego, California, USA)
Abbreviations used in this paper
- ASCA
- anti-Saccharomyces cerevisiae antibody
- CD
- Crohn's disease
- ELISA
- enzyme linked immunosorbent assay
- EU
- ELISA units
- IIF
- indirect immunofluorescent
- IBD
- inflammatory bowel disease
- pANCA
- perinuclear antineutrophil cytoplasmic antibodies
- UC
- ulcerative colitis
- TNF
- tumour necrosis factor
- PNPP
- p-nitrophenol phosphate
- Ig
- immunoglobulin