Article Text

Abstract
BACKGROUND Serotonin 5-HT4 receptors are located on enteric cholinergic neurones and may regulate peristalsis. 5-HT4 receptors on primary afferent neurones have been postulated to modulate visceral sensation. While 5-HT4 agonists are used as prokinetic agents, the physiological role of 5-HT4 receptors in the human gut is unknown.
AIMS Our aim was to characterise the role of 5-HT4 receptors in regulating gastrointestinal motor and sensory function in healthy subjects under baseline and stimulated conditions with a 5-HT4 receptor antagonist.
METHODS Part A compared the effects of placebo to four doses of a 5-HT4receptor antagonist (SB-207266) on the cisapride mediated increase in plasma aldosterone (a 5-HT4 mediated response) and orocaecal transit in 18 subjects. In part B, 52 healthy subjects received placebo, or 0.05, 0.5, or 5 mg of SB-207266 for 10–12 days; gastric, small bowel, and colonic transit were measured by scintigraphy on days 7–9, and fasting and postprandial colonic motor function, compliance, and sensation during distensions were assessed on day 12.
RESULTS Part A: 0.5, 5, and 20 mg doses of SB-207266 had significant and quantitatively similar effects, antagonising the cisapride mediated increase in plasma aldosterone and acceleration of orocaecal transit. Part B: SB-207266 tended to delay colonic transit (geometric centre of isotope at 24 (p=0.06) and 48 hours (p=0.08)), but did not have dose related effects on transit, fasting or postprandial colonic motor activity, compliance, or sensation.
CONCLUSION 5-HT4receptors are involved in the regulation of cisapride stimulated orocaecal transit; SB 207266 tends to modulate colonic transit but not sensory functions or compliance in healthy human subjects.
- 5-HT4 receptors
- colon transit
- gastrointestinal motor function
- gastrointestinal sensory function
Abbreviations used in this paper
- AUC
- area under the plasma concentration curve
- Cmax
- maximal concentration
- GC
- geometric centre
- MI
- motility index
Statistics from Altmetric.com
The effects of serotonin on gastrointestinal motor and sensory function are mediated by a growing family of receptor subtypes.1 The role of 5-HT4 receptors in regulating normal gastrointestinal motor and sensory function in humans is unknown; to date, in vitro studies have provided conflicting evidence on this issue. In “flat” preparations using the three compartment model, mucosal stimulation is accompanied by release of the neurotransmitter 5-HT from enterochromaffin cells and activation of intrinsic primary afferents2; this activation may be associated with initiation of the peristaltic reflex. Thus experimental studies in the human jejunum, and guinea pig and rat colon using selective 5-HT4 antagonists suggest that 5-HT activates 5-HT4 receptors on sensory afferents to trigger the peristaltic reflex and aborad propagation of faecal pellets.2 In contrast, other authors suggest that 5-HT4 receptor antagonism does not affect peristalsis evoked by radial intraluminal distension in isolated small intestinal preparations.3 ,4 In the human colon, 5-HT4receptors are also located on smooth muscle and have been reported to mediate relaxation.5-7
In addition to their location on intrinsic sensory neurones,8 mRNA for 5-HT4 receptors has also been found in the dorsal root ganglion,9 laminae I and II of the spinal cord,10 neocortex, and hippocampus.11 5-HT4 antagonists may have visceral antinociceptive effects in some12 but not all13 rat models. However, 5-HT4 receptors have not been reported on gut extrinsic sensory afferents projecting centrally.
SB-207266 is a highly potent, orally active, long acting 5-HT4 antagonist with an approximately 1000-fold greater binding affinity for 5-HT4 than for other 5-HT and non-5-HT receptors.14 SB-207266 inhibited motor activity induced by serotonin in human ileal circular muscle and prevented 5-HT evoked inhibition of spontaneous activity in human colonic circular muscle strips.3 Preliminary data suggest that SB-207266 may improve symptoms in patients with irritable bowel syndrome, reducing both orocaecal transit time and patient reported symptoms.15
Thus our objectives were: (i) to demonstrate the efficacy of SB-207266 as a 5-HT4 receptor antagonist in healthy subjects receiving a 5-HT4 agonist, and (ii) to assess the contribution of 5-HT4 receptors in regulating gastrointestinal transit, colonic motor, and sensory functions in unstimulated healthy subjects. We used elevation in serum aldosterone and acceleration of orocaecal transit induced by cisapride as a model for testing the 5-HT4 antagonist properties of SB-207266. The stimulatory effect of cisapride on serum aldosterone is mediated by agonistic effects at the 5-HT4 receptor.16Cisapride is primarily a 5-HT4 receptor agonist with weak 5-HT3 antagonist properties. Acceleration of transit by cisapride is predominantly attributed to its 5-HT4 receptor agonist properties.
Methods
The studies in part A assessing the ability of SB-207266 to antagonise the 5-HT4 mediated effects of cisapride on aldosterone release and orocaecal transit were conducted in 18 healthy volunteers at the Clinical Pharmacology Unit, SmithKline Beecham Pharmaceuticals, Harlow, UK. Studies in part B assessing the effects of SB-207266 on gastrointestinal transit, colonic, motor, and sensory function were conducted in 52 healthy volunteers at the Gastroenterology Research Unit, Mayo Clinic, Rochester, Minnesota, USA.
HEALTHY VOLUNTEERS
Inclusion and exclusion criteria for parts A and B were similar. All participants were healthy subjects aged 18–51 years and were recruited by public advertisement. A clinical interview, physical examination, and laboratory tests (complete blood count, chemistry group, urinalysis, serum pregnancy test for women of childbearing potential, and ECG) were performed during a screening visit and after the study was completed. Subjects were within 25% of ideal weight for height. Subjects with a history of clinically significant cardiovascular, respiratory, neurological, psychiatric, or endocrine disease, previous abdominal surgery (other than appendicectomy and/or cholecystectomy) or clinically significant abnormalities on examination were excluded.
For part B, validated screening questionnaires (bowel disease questionnaire17 and the hospital anxiety and depression inventory18) were used to exclude subjects with irritable bowel syndrome or significant affective disorders, as well as to determine anxiety and depression scores prior to the study. Subjects were not receiving other medications on a regular basis with the exception of acetaminophen, oral contraceptives, or multivitamins, none of which interferes with the pharmacokinetic profile of SB-207266. In part B, three subjects were receiving l-thyroxine replacement therapy for hypothyroidism and were demonstrated to be euthyroid by clinical and biochemical criteria prior to the study. All participants gave written informed consent to participate in the studies which were approved by an independent ethics committee at SmithKline Beecham Pharmaceuticals, Harlow, UK and the institutional review board at Mayo Clinic for parts A and B, respectively.
MEDICATION PHARMACOKINETICS AND EXPERIMENTAL DESIGN
In previous single and repeat dose studies, peak plasma concentrations of SB-207266 occurred between two and six hours post-dose; half life was 17–27 hours and steady state was attained on or before day 7 of repeated oral administration. There was a linear relationship between dose and the pharmacokinetic parameters such as area under the plasma concentration curve (AUC) and maximal concentration (Cmax) over the dose range 0.125 –20 mg. After single dose administration, the variability in Cmax and AUC between subjects at each dose level was generally low and ranged from 1.5% to 35%.
STUDY DESIGN: PART A
The experimental design for part A is summarised in fig 1. This was a randomised, double blind, placebo controlled, five part crossover study in 18 healthy subjects. Each subject received placebo or one of four single doses of SB-207266 (that is, 0.05, 0.5, 5, or 20 mg), followed three hours later by a 10 mg dose of cisapride on each of the five dosing days. The dosing days were separated by a period of at least 14 days. On each study day, blood samples for plasma aldosterone were collected immediately prior to and at hourly intervals up to six hours post-cisapride. Plasma aldosterone concentrations were analysed by radioimmunoassay.19

Experimental design for part A. On each study day, volunteers received placebo or one of four doses of SB-207266. *Breath hydrogen samples were collected every 10 minutes until three consecutive samples with readings ⩾15 ppm above baseline were attained.
Method
Orocaecal transit was measured using the breath hydrogen technique. Before starting the test, a mouthwash was used to avoid oral bacterial metabolism of substrate, as shown by low baseline breath hydrogen readings (<5 ppm). A minimum of three baseline breath hydrogen samples were collected after cisapride and before the meal was administered until consistent values (that is, within 3 ppm of each other) were attained. Subsequent breath samples were collected at 10 minute intervals beginning 30 minutes after the breakfast meal until three consecutive samples with readings 15 ppm above baseline were recorded. The meal consisted of one glass of fruit juice, two slices of brown bread, 250 g of baked beans, and a cup of decaffeinated tea or coffee.
Data analysis
Orocaecal transit time was the interval from the start time or the time at which breakfast was begun to the end point, as described above.
STUDY DESIGN: PART B
In part B, 52 subjects were randomised to receive placebo or one of three doses of SB-207266 (that is, 0.05, 0.5, or 5 mg) in a randomised, double blind, parallel group study design. Each subject received a capsule one hour before or two hours after meals once daily for a minimum of 10 days and a maximum of 12 days to allow for intervening weekends. On days 1, 7, 8, 9, and 10, the capsule was administered under supervision. A whole gut scintigraphic gastrointestinal transit study was performed from days 7 to 9. The intubated colonic motility and sensation study was performed either on day 10 or, if day 10 fell on a weekend, on day 11 or 12. Medication was continued until the day of the intubated study.
Scintigraphic gastrointestinal transit study
Method
An adaptation of our established scintigraphic method was used to measure gastrointestinal and colonic transit.20 ,21 Briefly, 111In adsorbed on activated charcoal particles was delivered to the colon by means of a methacrylate coated delayed release capsule.4 ,5 Also,99mTc-sulphur colloid was used to label two scrambled eggs, which were ingested with one slice of whole wheat bread and one glass of whole milk (300 kcal) to facilitate measurement of gastric emptying and small bowel transit. The study medication was administered with the99mTc labelled meal. Subjects ingested standardised meals for lunch and dinner at four and eight hours after the radiolabelled meal. Abdominal images were obtained every 15 minutes for the first two hours, every 30 minutes for the following four hours, and at eight, 24, and 48 hours. A variable region of interest program was used to quantitate the counts in the stomach and each of four colonic regions: ascending, transverse, descending, and combined sigmoid and rectum. These counts were corrected for isotope decay, tissue attenuation, and cross talk (downscatter) of 111In counts in the99mTc window.
Data analysis
Summary parameters for comparison of transit profiles included gastric lag time (time for 10% emptying), gastric emptying at two (GE 2) and four (GE 4) hours, small bowel transit time (SBTT; t10%), and colonic geometric centre (GC) at four, eight, 24, and 48 hours. The geometric centre is the weighted average of counts in the different colonic regions (ascending (AC), transverse (TC), descending (DC), rectosigmoid (RS)) and stool. At any time, the proportion of colonic counts in each colonic region was multiplied by its weighting factor as follows:
(%AC×1+%TC×2+%DC×3+%RS×4+% stool×5)/100 = geometric centre.
Thus a high GC implies faster colonic transit; for example, a GC of 1 implied all isotope was in the ascending colon and a GC of 5 implied all isotope was in the stool.
We also calculated the t1/2 for proximal colonic emptying (combined ascending and transverse regions) by linear interpolation between the last value greater than 50% and the first value below 50%. If there was less than 50% emptied by 48 hours (that is, >50% still remained in the proximal colon), the last scan time used in this study (48 hours) was assigned a “censored” t1/2 value for proximal colonic emptying.
Colonic motor function
Method
After an overnight oral lavage with 2–5 litres of polyethylene glycol 3350 and electrolyte solution (Golytely, Abbott Laboratories, Chicago, Illinois, USA), a multilumen polyethylene balloon barostat-manometric assembly was positioned in the descending colon using flexible endoscopy and fluoroscopy.22 Tonic and phasic contractile activity of the colon were measured using an infinitely compliant 10 cm long balloon with a maximum volume of 600 cc (Hefty Baggies, Mobil Chemical Co., Pittsford, New York, USA) linked to an electronic barostat (Mayo rigid barostat, Mayo Foundation Engineering Department, Rochester, Minnesota, USA) which has a rigid piston. The manometric portion comprised six water perfused (0.4 ml/min) pneumohydraulic sensors, three in the descending colon (sensor numbers 1–3) and three in the sigmoid colon (sensor numbers 4–6). The manometric sensors were 5 cm apart, while the first and second sensors were 5 cm orad and caudad to the balloon, respectively. The barostat balloon “operating pressure” was set as described previously (median pressure 10 mm Hg (range 4–18)22). Intraballoon volumes and manometric pressure changes in response to wall contractions and relaxations were monitored continuously throughout the study. A pneumobelt was applied around the abdominal wall at the level of the lower costal margin to help exclude artefact during movement and coughing.
The entire experimental protocol is summarised in fig 2. Fasting colonic tone and phasic activity were recorded for 30 minutes. Thereafter, we consecutively measured colonic compliance, sensation, and response to a standard meal.
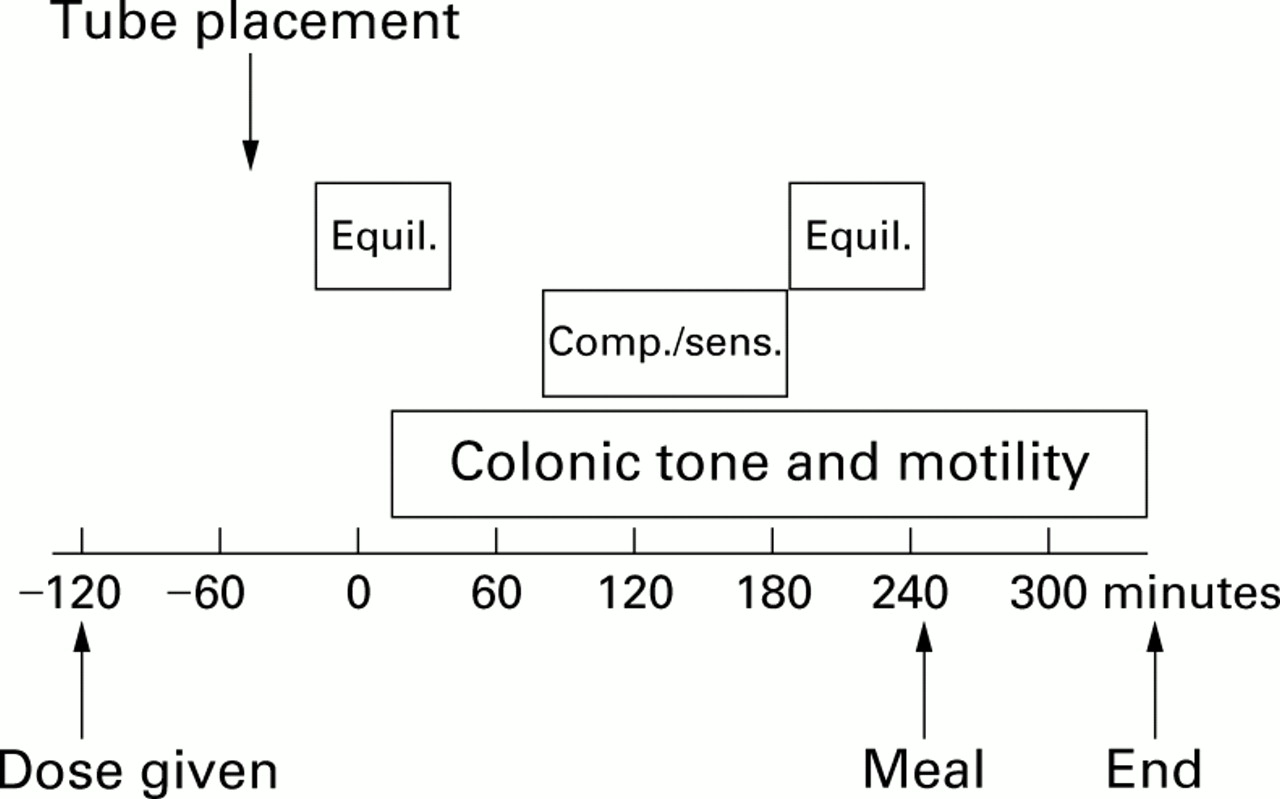
Experimental design for colonic barostat-manometric study. Equil., equilibration periods; Comp./sens., assessment of colonic compliance and sensation.
Data analysis
Colonic motor response (that is, tone and phasic activity) was quantified using methods identical to those in previous studies.22 Phasic pressure activity was expressed as motility index per hour (MI/h) for the descending colon (sensors 1–3) and sigmoid colon (sensors 4–6); MI/h was defined as ln ((number of contractions×amplitude of contractions)+1). For the barostat balloon volume data, the baseline balloon volume representing colonic tone was separated from phasic volume deflections >10 ml from baseline volume.
Colonic compliance
Method
Fifteen minutes after the initial conditioning distension (4 mm Hg steps, 60 second intervals; 4–44 mm Hg), we measured the colonic compliance curve by increasing intraballoon pressure in 4 mm Hg steps at 30 second intervals from 0 to 44 mm Hg. The intrinsic compliance of the rigid piston in the barostat used for this study is nearly zero.
Data analysis
For colonic compliance, the balloon volume was averaged for 30 seconds at each pressure increment. We have previously demonstrated that colonic pressure-volume relationships are not linear but sigmoid, approximating closely to a power exponential function.22 Similarly, in this study pressure-volume relationships were non-linear; a power exponential function fitted the actual data points closely (r 2=98.8 (93.7–99.6) median (range)). The proportionate volume (observed volume at each pressure divided by maximum observed volume) as a function of (reciprocal) pressure (RP) is specified by the following model:
pVol=r+exp{−(k×RP)β} where r=estimated limiting value of pVol at zero pressure (essentially the initial volume divided by maximum volume) and RP=1/pressure. The parameter β reflects the overall shape of the curve, while k is essentially the rate of change in pVol as a function of 1/pressure at any given point. The parameters, r, k, and β for the ascending portion (0–44 mm Hg) of the colonic compliance curve were estimated using the NLIN procedure in the SAS software package.23 The estimated parameters from each subject were used to calculate the pressure corresponding to half maximum volume (Prhalf).
Colonic sensation
Method
As described previously,24 ,25 colonic distension was performed as rapid, intermittent “phasic” increases in intraballoon pressure in four steps of 8, 16, 24, and 32 mm Hg greater than the operating pressure. The order of distensions was randomised; each phasic pressure increment was maintained for one minute with a one minute interval during which the intraballoon pressure was reduced to operating pressure. For rating sensory perception, participants were asked to mark two separate 100 mm visual analogue scales for abdominal pain and feelings of gas at a standardised time, 20 seconds after the distension had commenced. The 100 mm long visual analogue scales were anchored at the ends by the descriptions “unnoticeable” and “unbearable”. During assessment of sensations, verbal interaction between the subject and investigator was minimised.
Data analysis
Sensations scored on the visual analogue scale were evaluated with a number of covariates which were previously shown to influence sensation: balloon volume at standard distension levels, arousal, and stress levels. As balloon volume varies over time as the colonic segment accommodates to the pressure load, intraballoon volume was averaged over a 30 second period, beginning at 20 seconds after the distension had commenced. Levels of arousal and stress were determined immediately prior to assessment of colonic sensation. Two 100 mm linear analogue scales marked “tired-energetic” and “active-drowsy” were used to assess arousal levels, while stress levels were assessed using similar scales marked “peaceful-tense” and “worried-relaxed”.25
Colonic response to a meal
Method
As in previous studies,22 colonic tone and motility were assessed for 30 minutes before and 90 minutes after consuming a chocolate milkshake containing 1000 kcal (35% carbohydrate, 53% fat, and 12% protein).
Data analysis
The tonic and phasic colonic motor responses to meal ingestion were calculated as the change in log scale (that is, log (90 minutes post-meal average/30 minutes pre-meal average)) of balloon volumes and MI/h, respectively.
STATISTICAL ANALYSIS
Part A
Analysis of variance was used to estimate drug effects on two parameters—that is, plasma aldosterone and orocaecal transit after cisapride. For both parameters, differences between each dose of SB-207266 and placebo were estimated as percentage changes in mean and 95% confidence intervals from baseline at each time point.
Part B
The focus of the statistical analyses was to compare responses between placebo (A) and three different doses of SB-207266 (0.05 mg (B), 0.5 mg (C), and 5 mg (D)) on the primary end points of this study: geometric centre for colonic transit at 24 hours (GC24), colonic sensation of pain and gas during phasic balloon distension, and colonic motor response to a meal. Additional analyses also examined secondary end points, including regional transit (gastric emptying, small bowel transit, geometric centre for colonic transit at four hours (GC4)), proximal colonic emptying, fasting tone, and colonic compliance parameters (k, β, and Prhalf).
GC24, postprandial colonic motor responses, and colonic compliance parameters (k, β ratio, and Prhalf) were analysed using one way analysis of variance. A similar analysis for the transformed proportions emptied from the stomach at two and four hours was examined, and a non-parametric Kruskal-Wallis test was used to analyse small bowel transit data. Visual analogue scale (VAS) scores for pain and gas during colonic distension were analysed separately using a repeated measures analysis of variance fitting terms for groups (doses), pressure, and order (of pressure distensions). Interaction terms (for example, group by pressure, group by order, pressure by order, and group by pressure by order) as well as several potential covariates (for example, pain score and balloon volume at the operating pressure, stress, and arousal levels) were also included in these analyses. An unstructured variance-covariance matrix was used to accommodate within subject correlations.
Results
SUBJECT DISPOSITION AND DEMOGRAPHIC DATA (TABLE1)
SB-207266 was well tolerated by subjects in parts A and B. One subject participating in part B sustained a syncopal episode during the study that was considered unlikely to be related to the study medication. All subjects in part A completed the study; three of 52 subjects enrolled in part B did not tolerate the oral colonic cleansing solution. These three subjects and another subject in whom the polyethylene balloon leaked during the motility study were replaced without breaking the study randomisation code. Thus combined assessment of gastrointestinal transit and colonic motility was completed in a total of 48 subjects. In part B, the proportion of men (2/12) in the group randomised to receive 0.5 mg was lower (p=0.11; Fisher's exact test) compared with the placebo (6/14), 0.05 mg (6/11), and 5 mg (7/11) groups. Anxiety and depression ratings, and stress and arousal scores were similar in the four groups (data not shown).
Effect of SB-207266 on gastric emptying, small bowel transit, and proximal colonic emptying
EFFECT OF SB-207266 ON CISAPRIDE INDUCED INCREMENT IN PLASMA ALDOSTERONE
A plot of plasma aldosterone levels against time is shown in fig3. The 95% confidence intervals of mean aldosterone levels of the cisapride plus SB-207266 treatment groups did not overlap the data for cisapride with placebo, indicating a reduction in the cisapride associated increment in plasma aldosterone. Thus statistically significant reductions in the cisapride induced plasma aldosterone increment were evident for the 0.5, 5, and 20 mg doses of SB207266 compared with placebo (p<0.05 for each dose).

Effect of SB-207266 on cisapride induced increases in plasma aldosterone. SB-207266 (0.5, 5, and 20 mg) significantly inhibited the cisapride induced increase in plasma aldosterone levels.
EFFECT OF SB-207266 ON OROCAECAL TRANSIT AFTER CISAPRIDE
SB-207266 retarded orocaecal transit compared with placebo in subjects who had previously received cisapride (table 2). There was a statistically significant prolongation of orocaecal transit time for all doses compared with placebo. The mean differences for the comparisons of 0.5, 5, and 20 mg of SB-207266 with placebo were similar, suggesting that the 5 mg and 20 mg doses had similar effects as the 0.5 mg dose.
Effect of SB-207266 on cisapride induced acceleration of orocaecal transit
EFFECT OF SB-207266 ON GASTROINTESTINAL TRANSIT (PART B)
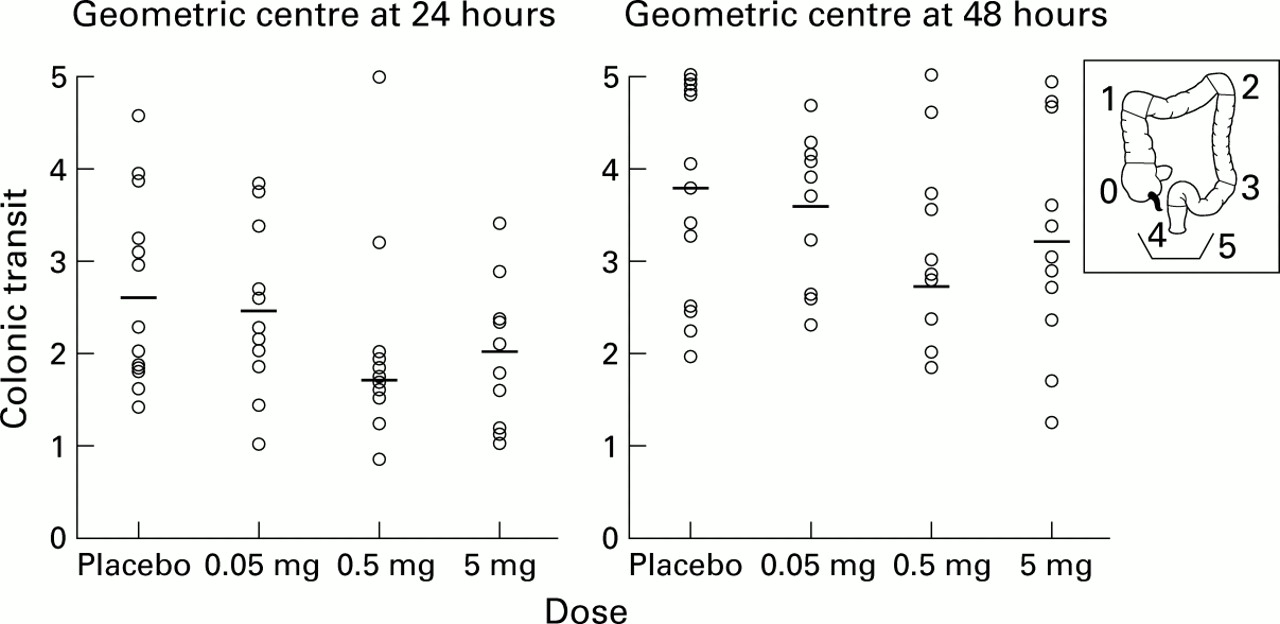
These studies were not preceded by administration of cisapride. SB-207266 did not affect gastric emptying lag time (data not shown), percentage isotope emptied from the stomach at two or four hours, or small bowel transit time (table 1). There was a non-significant trend (p=0.14) in favour of SB-207266 for slower emptying from the proximal colon, measured as time for 50% emptying of the isotope. Data also suggested slower overall colonic transit (GC24 (p=0.06) and GC48 (p=0.08)) (fig 4) with drug treatment. The 5 mg dose had similar effects as the 0.5 mg dose on colonic transit, but these effects were not statistically significant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of drugs on colonic transit expressed as the geometric centre of colonic transit at 24 (GC24) and 48 (GC48) hours. Main figure shows data for each subject with dose mean. Insert depicts anatomical location of GC 0–5.
EFFECT OF SB-207266 ON COLONIC TONE, PHASIC ACTIVITY, AND COMPLIANCE
SB-207266 did not significantly affect fasting or postprandial colonic tone, phasic activity (not shown), or colonic compliance (table3).
Effect of SB-207266 on colonic tone and compliance (mean(SEM))
EFFECT OF SB-207266 ON PERCEPTION OF COLONIC DISTENSION
Mean pain and gas scores increased overall with increasing pressure over all dose groups (p=0.0001), but not consistently for each dose group (p=0.03 for the pressure×group interaction) (table 4). There was no overall effect of SB-207266 on pain or gas scores compared with placebo. None of the covariates studied (that is, sex, VAS scores for stress and arousal, baseline sensation score, and baseline volume at operating pressure) significantly influenced sensation scores.
Effect of SB-207266 on perception of colonic distension (mean (SEM))
ASSESSMENT OF SAMPLE SIZE AND ACTUAL STUDY POWER
Using estimates of the coefficients of variation from previous studies, we calculated that a sample size of 12 subjects per group would provide at least 80% power of detecting a priori specified differences at an alpha level of 5% (type I error) (table 5). After the study was completed, we used the coefficient of variation observed in the placebo group to re-estimate the power of detecting differences between placebo and drug. Calculations were based on a two samplet test for comparison of placebo versus each dose group. These data showed that for all parameters except postprandial colonic motor response, the sample size was adequate and consistent with pre-study estimates.
Sample size estimates for detecting significant differences
Discussion
While 5-HT4 receptor agonists are known to enhance gut contractility in humans,26 the contribution of 5-HT4 receptors to regulating gastrointestinal motor and sensory function can only be assessed with a 5-HT4antagonist. In this respect, therefore, this is the first study to assess the contribution of 5-HT4 receptors on gastrointestinal motor and sensory function in vivo in normal humans. Our results demonstrated that a selective 5-HT4 antagonist, SB-207266, administered in doses sufficient to antagonise the effects of a 5-HT4 receptor agonist, tended to delay colonic transit without delaying gastric emptying or small bowel transit. Moreover, 5-HT4 antagonism did not influence fasting or postprandial colonic motor activity or perception of colonic balloon distension in healthy subjects. Despite the evidence supporting a role for 5-HT4 receptor modulation of peristalsis from in vitro studies,2 our results suggest that in healthy subjects 5-HT4 receptors play a relatively modest role in modulating colonic motor activity and sensation under basal physiological conditions.
Interestingly, the 0.5, 5, and 20 mg doses of SB 207266 prevented the effects of cisapride on orocaecal transit and plasma aldosterone to a similar degree, whereas 0.05 mg had no effect compared with placebo. These data suggest that the 0.5 mg dose may be close to the minimal effective SB-207266 dose in the “stimulated” state with a 5-HT4 agonist. In part B, the highest dose of SB-207266 was fivefold higher than the dose which inhibited cisapride stimulated elevation of plasma aldosterone levels by 90%. The broad range of dosages reduces the likelihood that a significant drug effect was missed in the “unstimulated” state, without a 5-HT4agonist.
Hence we considered four other potential factors that might explain the lack of efficacy of SB-207266 on intraluminal assessments of colonic motor and sensory function—that is, insensitivity of measurements or end points, insufficient power, lack of compliance with study drug, and true lack of biological effect of the drug. Interpretation of our data is limited by the inability to detect differences smaller than those specified in the power calculation; however, it is unlikely that a type II error would prevent identification of a drug effect on any of the parameters assessed in this study, except postprandial motility.
Our methods are sensitive in detecting pharmacological modulation of colonic sensorimotor functions in our laboratories and other centres. Previous studies with a barostat balloon within the descending colon have shown that the 5-HT3 receptor antagonist ondansetron significantly reduced tonic and phasic colonic motor responses to a meal27 while the 5-HT1a agonist buspirone28 and the 5-HT1D agonist sumatriptan29 reduced fasting colonic tone. Thus the barostat can detect colonic contraction and relaxation. We have used identical methods and a comparable number of healthy subjects to demonstrate alterations in perception during balloon distension resulting from psychogenic stress or pharmacological perturbations.22 ,30 ,31 Although pharmacokinetic studies were not performed, the medication was administered under supervision on days 1, 7–9 (transit study), and 10 (motility study). At the end of the study, pill counts were as expected, with the exception of two subjects who lost one pill each. Gastrointestinal transit and colonic motility studies were performed after allowing sufficient time for serum concentrations to achieve steady state, according to previously determined pharmacokinetics. Transit measurements allow detection of pharmacological retardation32 or acceleration33 of transit with agents active on 5-HT3 or 5-HT4 receptors.
Intraluminal assessments of colonic tone and phasic pressure activity do not explain the tendency towards delayed transit for the 0.5 mg dose of SB207266. Cook et al recently demonstrated that aborad propulsion of colonic contents occurred with both propagating and non-propagating pressure events.34However, propagating sequences were associated with significantly greater isotope movement. We observed no differences in low or high amplitude propagated contractions in the left colon between groups and hence cannot fully explain the trend towards delayed transit in one group.
The 0.5 mg dose group had a higher proportion of females than the other groups. It is unclear if sex differences contributed to the trend to delayed transit with this dose. For instance, it is conceivable that a 5-HT4 antagonist may be more effective in blocking endogenous 5-HT in females as the rate of 5-HT synthesis is lower in females than males.35 To date, this difference in synthesis between the sexes has been observed in the human brain but it is unclear if it also applies to the gut.
Previous studies evaluating 5-HT4 receptor contribution to gastrointestinal function have relied on the effects of 5-HT4 receptor agonists in humans and 5-HT4receptor antagonists in animals. These are notable for interspecies and interorgan variability,5 dependence on 5-HT induced sensitisation,3 ,4 and/or coexistent 5-HT3receptor antagonism.12 ,36 ,37 Cisapride, a 5-HT4 receptor agonist with weak 5-HT3antagonist effects, increases upper gut contractility in humans and colonic contractility in the guinea pig, mainly by stimulating 5-HT4 receptors on enteric neurones, leading to enhanced release of acetylcholine.26 In contrast, 5-HT acts on 5-HT4 receptors in colonic smooth muscle to reduce the amplitude and frequency of contractions, causing relaxation.5-7 Therefore, the effects of 5-HT4 receptor antagonism are presumably dependent on the balance between blocking excitatory effects on neurones and blocking inhibitory effects on smooth muscle. While 5-HT4 receptors are located on intrinsic primary afferents and in cerebral foci involved in sensory processing, SB-207266 did not influence perception of colonic balloon distension.
It is conceivable that selective 5-HT4 receptor antagonists may have more pronounced effects on colonic motor activity and sensation in the setting of serotonergic stimulation, as in carcinoid diarrhoea or in the presence of a 5-HT4 agonist, as shown with the combined trial with cisapride in part A. It is also known that SB-207266 and other related 5-HT4 receptor antagonists reduced faecal pellet output in mice only after pretreatment with 5-HTP3; in contrast, SB-207266 had no effect in the basal state. In the canine colon, another selective 5-HT4antagonist, SDZ 205–557, did not influence baseline contractile activity but inhibited the response to a 5-HT4 receptor agonist.38 Lastly, in some models, such as the guinea pig37 and rat36 colon, combined 5-HT3 and 5-HT4 receptor blockade was necessary to inhibit transit.
In summary, a selective 5-HT4 antagonist tended to delay colonic transit but did not affect intraluminal assessments of colonic motor activity or sensation in healthy subjects. The relatively mild effects on gastrointestinal transit and the absence of an effect on colonic fasting or postprandial motor activity contrast with the pronounced effects of the 5-HT4 antagonist on orocaecal transit in the presence of cisapride, a 5-HT4 agonist. Our data also re-emphasise the interspecies differences in the effects of 5-HT4 receptor blockade, highlight the importance of conducting studies in humans, and underscore the need to continue to refine experimental models and surrogate markers in humans when testing pharmacological agents.
Acknowledgments
This study was supported in part by General Clinical Research Center grant No RR00585 from the National Institutes of Health in support of the Physiology Laboratory and Patient Care Cores, by NIH R01 HD38666–01 (AEB), NIH R01 DK54681–01 (MC) and K24 DK02638–01 (MC), and by a grant from SmithKline Beecham Pharmaceuticals. Conflict of interest statement. This study was funded by SKB Pharmaceuticals. S Haydock, S Cooper, D Tompson, K Fitzpatrick, and R Higgins were employees of SKB Pharmaceuticals when this study was conducted.
Abbreviations used in this paper
- AUC
- area under the plasma concentration curve
- Cmax
- maximal concentration
- GC
- geometric centre
- MI
- motility index