Article Text

Abstract
BACKGROUND AND AIMS Whether healthcare workers have an increased prevalence of hepatitis C virus infection as a result of exposure to patient's blood and body fluids is controversial. This study assesses the prevalence of hepatitis C virus infection in healthcare workers, and its relation to the performance of exposure prone procedures and duration of occupational exposure, allowing an estimate to be made of the incidence of occupationally acquired hepatitis C infection among medical staff.
METHODS In this anonymous retrospective cohort study, we estimated the prevalence of hepatitis C infection in 10 654 healthcare workers. ELISA-3 testing was performed on pools of five sera collected during immunisation against hepatitis B. Healthcare workers were arranged into five occupational groups, according to the degree of patient exposure, and three age bands (<30 years, 30–39 years, >40 years).
RESULTS Prevalence of antibodies to hepatitis C was 0.28% (30/10 654), comparable in all occupational groups (p=0.34) and unrelated to duration of potential exposure. Assuming that all detected infections had been occupationally acquired, the maximum estimated risk of hepatitis C infection in exposure prone medical staff was low: 1.4% for surgeons and 1.0% for physicians over a 35 year professional career.
CONCLUSIONS Hepatitis C infection is infrequent in healthcare workers in Glasgow. Those conducting exposure prone procedures do not seem to be at higher risk than other healthcare staff.
- hepatitis C virus
- epidemiology
- exposure prone procedures
- healthcare worker
Abbreviations used in this paper
- HCV
- hepatitis C virus
- HBV
- hepatitis B virus
- RT-PCR
- reverse transcriptase-polymerase chain reaction
Statistics from Altmetric.com
The hepatitis C virus (HCV) was first identified in 1989 but has been prevalent for many decades. In western countries, HCV is most commonly transmitted among injecting drug users who share injecting equipment. Once infected most patients develop chronic HCV infection, a disease with considerable morbidity and mortality.1 The incidence of HCV seroconversion after accidental needlestick exposure is uncertain, with reports ranging from 0 to 10%.2-5 Whether healthcare workers have a higher prevalence of hepatitis C virus infection than the general population through percutaneous occupational exposure is unclear.6-12 The aim of this study was to assess the prevalence of HCV antibodies in healthcare workers in Glasgow, a city where injecting drug use is common, and to analyse rates in relation to specific occupational groupings and duration of potential exposure to HCV. The study focused in particular on staff performing exposure prone procedures, where injury to the worker may result in the exposure of the patient's open tissues to the blood of the worker. These rates were then compared with existing prevalence data in other local populations to determine if certain health care workers may be at increased risk of occupationally acquired HCV.
Methods
SETTING
This study was performed in the Greater Glasgow Health Board area, which incorporates the largest city in Scotland with a population of 909 000 in 1996. It is estimated that approximately 80% of Glasgow's large injecting drug user population have been infected with HCV.13 ,14 Glasgow is served by eight NHS hospital trusts providing a full range of clinical services, a single diagnostic virology laboratory service (Regional Virus Laboratory), and a coordinated occupational health service integrated into each NHS trust.
STUDY POPULATION
All healthcare workers in Glasgow who presented for hepatitis B virus (HBV) immunisation between October 1994 and October 1997 and had serum samples stored for anti-HBs assay were identified. Employees from one NHS trust, which denied ethics approval, were excluded.
Of the 24 077 serum samples received by the Regional Virus Laboratory from healthcare staff, there were 11 577 individuals that had occupational health case notes available after duplicate samples had been removed. Samples from 10 654 (92%) of these healthcare workers were located in the virology serum archive. According to 1997 Scottish Health Statistics payroll data, this sample represents 44% of the 24 150 healthcare workers employed in the seven Glasgow NHS hospital trusts studied (personal communication). Included are: 1430 of 1972 (73%) hospital medical staff, 203 of 547 (37%) dentists, 5913 of 11 803 (50%) nursing and midwifery staff, and 3108 of 9828 (32%) others.
STUDY PROCEDURE
This study was necessarily performed in an anonymous manner. Serum samples were initially linked to the corresponding employee's immunisation records at the occupational health clinics using a database consisting of employee's name, sex, date of birth, location of employment, and occupational group. When data collection was complete, the age of each employee at the time of sample collection was derived. Individuals were then grouped into one of five occupational categories by their degree of patient exposure and into three age bands (table 1) to ensure that any combination of the two contained more than 50 individuals, thus protecting any infected individual against identification. All employee identifiers were then deleted from the database leaving only non-identifying details of occupational category and age band, linked to the stored serum laboratory number.
Occupational categories and age bands of healthcare workers tested for antibodies to hepatitis C
A unique non-identifying code was generated for each database entry and printed on labels adjacent to the corresponding laboratory serum number. The appropriate sera were then labelled with their unique code and transferred to a separate laboratory for testing. By then deleting the laboratory serum numbers from the database, the HCV antibody results could only be linked with the anonymous data (occupational category and age band) via the unique non-identifying code.
SAMPLES FOR TESTING
Sera were initially stored by sequential laboratory number at either 4°C or −20°C on the day of collection in the virology department. The study sera were then identified, aliquoted into 2.5 ml Sarstedt vials, labelled with the unique non-identifying code, and stored at −20°C for testing.
HEPATITIS C TESTS
Sera were screened for antibodies to HCV by ELISA-3 (Ortho Diagnostics, Raritan, New Jersey, USA). Reactive samples were only considered positive if they were confirmed by RIBA-3 testing (Ortho Diagnostics). All samples confirmed positive were further tested for the presence of HCV RNA by reverse transcriptase-polymerase chain reaction (RT-PCR) using an inhouse method.15 RT-PCR positive samples were genotyped by restriction fragment length polymorphism.16
In view of the large number of sera to be tested, a pooling protocol was developed. Pools of five sera were tested by third generation ELISA. Twenty microlitres of each of the five sera to be tested were pooled and mixed thoroughly. A sample of this pool (50 μl) was transferred into the test plate (the equivalent of 10 μl of each serum), diluent was added to a total volume of 200 μl, and thereafter testing followed the Ortho ELISA-3 protocol. The final dilution of each individual serum in the pool was 1 in 20 compared with individual testing with a 1 in 11 dilution. The five sera in any reactive pool were then tested individually by ELISA-3 to identify the reactive samples requiring confirmatory testing by RIBA-3.
STATISTICS
Data were analysed for the prevalence of antibodies to HCV in each age band and occupational group. The prevalence in each of these categories was compared using the χ2 test or Fisher's exact test.
By assuming that 24 years is the median age at which doctors qualify in the UK, the probability of acquiring HCV per 100 person-years of occupational exposure for the medical staff was estimated to be:
Probability of HCV infection /100 person-years exposure=(Number positive for HCV antibodies×100/Number tested × (median age in occupational group−24))
This estimate is a maximum because it is possible that infections among HCV antibody positive individuals were acquired before healthcare work was commenced or through a non-occupational route. The median age for each occupational group was available from the dates of birth on the original database.
ETHICS
Ethics approval for this study was obtained from seven of the eight NHS trust research ethics committees in Glasgow. Employees of Yorkhill NHS University Trust, which did not grant approval, were excluded.
Results
EVALUATION OF POOLING
The pooling method was evaluated on the first 2190 serum samples from employees in exposure prone occupations. They were initially tested individually and then arranged into 438 pools and tested by a single operator blinded to the location of the known positive samples (table 2). Nine of these pools contained a single serum sample known to be reactive when tested individually by ELISA-3. On pooled testing, all five sera confirmed positive by RIBA-3 individual testing and one serum considered indeterminate by RIBA-3 testing (C33 2+ band only) were detected. Two pools were reactive when individual ELISA-3 and RIBA-3 testing confirmed all 10 sera to be unreactive (false positive pools). Three pools containing sera known to be reactive by individual ELISA-3 testing were unreactive. Two of these pools contained single samples which were RIBA-3 negative and considered false positives for antibodies to HCV and one was of indeterminate RIBA-3 reactivity (C33 2+ band only) and hence of doubtful significance. With confirmatory testing by RIBA-3, our method of pooling had a sensitivity of 100% (5/5) and specificity of 100% (433/433) for samples that were confirmed positive for antibodies to HCV.
Comparison of ELISA-3 hepatitis C virus (HCV) antibody test on individual and pooled sera from 2190 healthcare workers who conduct exposure prone procedures
HCV PREVALENCE
Thirty eight (1.8%) of the 2131 pools tested were reactive by ELISA-3 and individual sera were analysed further (fig 1). The overall prevalence of HCV antibodies was 0.28% (30/10 654, 95% confidence interval 0.19−0.41%). Occupational category and age band of employees tested are summarised in table 1. There was no statistically significant difference in the prevalence of HCV antibodies between the five occupational categories (p=0.34) or between exposure prone staff and all non-exposure prone staff (0.23% v0.30%; p=0.59). The prevalence of antibodies to HCV was significantly higher in the 30–39 year age band (p=0.012).

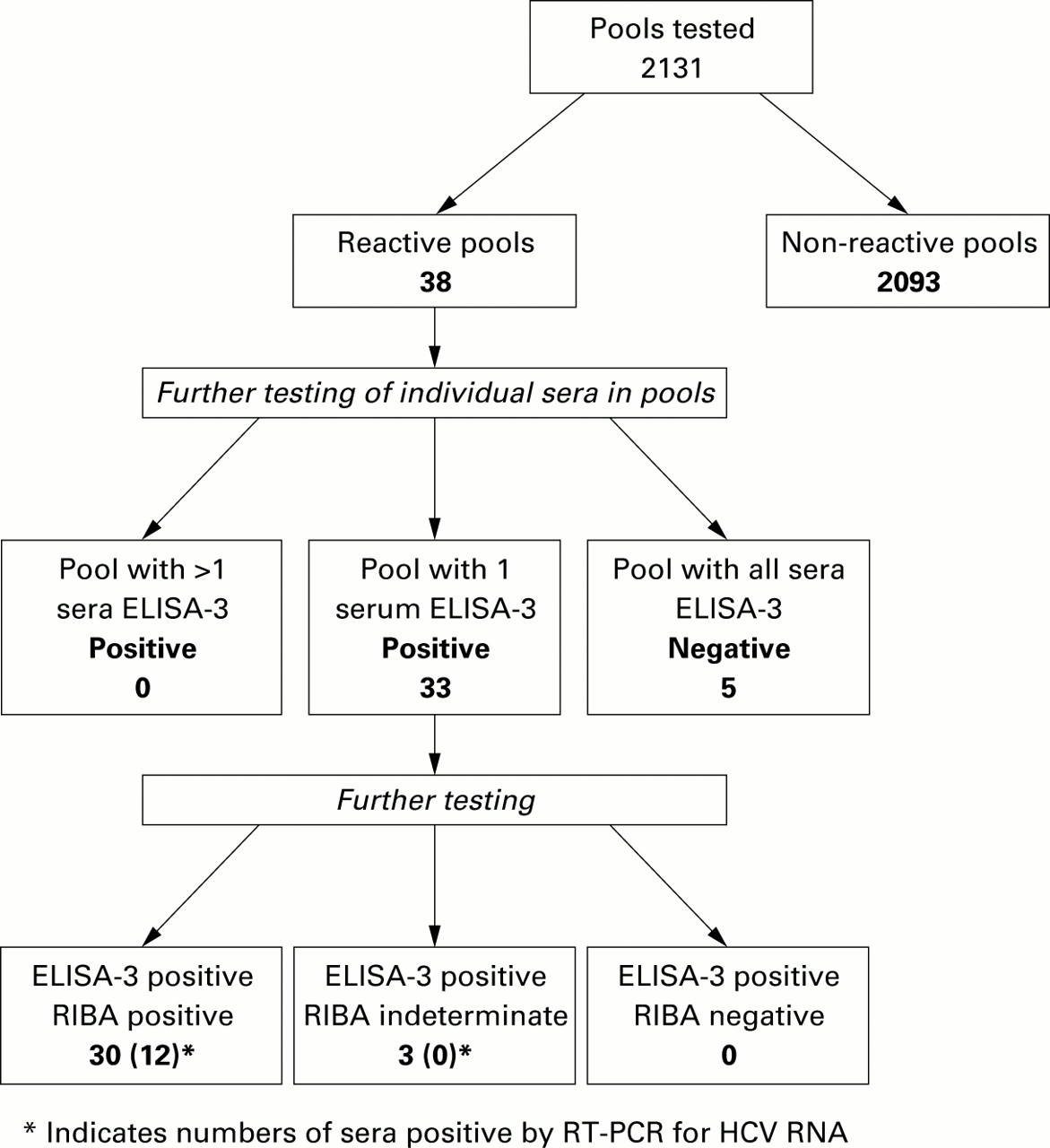{kind=link}
Results of testing sera from 10 654 healthcare workers for antibodies to hepatitis C virus (HCV) by ELISA-3 in pools of five.
Twelve (40%) of the 30 sera confirmed to contain antibodies to HCV had viral RNA detectable in serum by RT-PCR. These were typed as follows: six type 1, four type 3, one type 5, and one could not be typed.
PROBABILITY OF HCV INFECTION
Within the exposure prone category, median age and age ranges for each occupational group were: surgeons 30 years (22–62 years); physicians 34 years (22–63 years); dental staff 29 years (16–72 years); and nurses 34 years (17–64 years).
The maximum estimated probability of occupationally acquired HCV infection per 100 person-years in the exposure prone group was 0.04 for surgeons and 0.03 for physicians, which would equate to a 1.4% and 1% risk, respectively, over a professional career of 35 years.
Discussion
Hepatitis C is a blood borne virus transmitted by the parenteral route. Infection frequently results in a chronic asymptomatic carrier state for many years before the development of symptomatic liver disease. HCV infected healthcare workers may therefore be unaware of their condition and their potential to infect patients. Healthcare workers, who perform exposure prone procedures, where injury to the worker may result in exposure of the patient's open tissues to the blood of the worker, are theoretically at increased risk of infection with blood borne viruses. According to UK health department guidelines, these occupations include surgeons, interventional physicians, and intensive care unit and accident and emergency staff. If occupational transmission of HCV was common, staff performing exposure prone procedures might be expected to have a higher prevalence of hepatitis C antibodies compared with staff in less exposed occupations. Our results revealed that the overall prevalence of hepatitis C antibodies in healthcare workers in Glasgow was low (0.28%) and comparable with those reported in two smaller studies from England.5 ,6The data indicate that the performance of exposure prone procedures does not frequently result in the acquisition of HCV by healthcare workers (exposure prone 0.23% vnon-exposure prone 0.30%; p=0.59). The prevalence of HCV antibodies among surgeons (only one (0.23%) of 438 tested), the group perceived to be at greatest risk of occupational exposure, was comparable with that observed among healthcare workers who have had little or no patient contact, including student nurses. However, the similar prevalence may not reflect similar routes of infection and we were unable to explore the presence of other risk factors for HCV transmission with this study design. Needlestick injuries to surgeons in operating theatres are common (15.5 per operator per 1000 operations).17 Even if we assume that all infections in exposure prone staff were occupationally acquired, the estimated maximum probability of occupationally acquired HCV infection in surgeons is 1.4% (1 in 70) over a surgical career of 35 years (0.04 per 100 person years). This value agrees with a model based estimate of professional lifetime risk of HCV infection for a French surgeon of 0.3–3.1%18.
Studies have reported a higher prevalence of antibodies to HCV in healthcare workers compared with blood donors but they are non-representative self selected group and persons with high risk behaviour are excluded.6 ,7 The prevalence of antibodies to HCV in the Glasgow population is unknown. From 1991 to 1997, 2161 individuals tested positive for HCV in the Greater Glasgow Health Board catchment area (prevalence 0.24% (2161/ 905 100)).19This is likely to be an underestimate of the true population prevalence but is comparable with the prevalence recorded in healthcare workers in this study (0.28% v 0.24%; p=0.42). A mixed population of hospital attenders (male outpatients or inpatients, aged 16–49 years) at two of the general hospitals in our study were screened for HCV antibodies from July to December 1997 using the same pooling protocol (manuscript in preparation). The prevalence of antibodies to HCV in this population was 4.0% (107/2702 individuals tested), significantly higher than the healthcare worker population prevalence (0.28% v 4.0%; p<0.0001). Thus healthcare workers, including those performing exposure prone procedures, have an estimated prevalence of antibodies to HCV which does not exceed that already known in the local population and is less than that in a cohort of their male hospital patients.
Pooling of sera allowed us to increase the number of third generation ELISA tests performed without loosing sensitivity or generating an unacceptable number of false positives requiring further testing. This is in keeping with earlier reports using similar pooling methods with second generation ELISA kits for epidemiological studies in low prevalence populations.20 ,21 Of the 30 healthcare workers with antibodies to HCV, only 12 were found to be viraemic. This may reflect the suboptimal storage conditions of sera for RNA analysis. Alternatively, it may reflect the high rate of clearance of HCV RNA from serum of healthy individuals exposed to HCV many years previously.22 Most viraemic patients were infected with genotype 1 (six, 50%) or genotype 3 (four, 33%), similar to our local clinic population where genotypes 1 and 3 occur with equal frequency. One individual was infected with genotype 5, suggesting acquisition of infection abroad.
The risk posed to patients by a HCV infected healthcare worker is not known and there are no guidelines to assist in their management. There have been reports of HCV transmission to patients as a consequence of inadequate infection control procedures and by negligent medical practices.23 ,24 There has been only a single published report of HCV transmission from an infected cardiac surgeon to five patients despite universal precautions having been observed.25 Provided that appropriate infection control policies are followed, patients and healthcare managers should be reassured by the low reported prevalence of HCV infected healthcare workers in the health service.
Healthcare personnel and patients can both be reassured that the reservoir of healthcare personnel in the West of Scotland who are infected with HCV is extremely small (2.8 per 1000). It appears that working in the healthcare environment and performing exposure prone procedures, in an area with a large HCV infected injecting drug using population, only rarely leads to acquisition of HCV by healthcare workers. The risk that a patient may become infected by contact with the health service is probably low. However, these findings should not lead to any complacency in the implementation of universal precautions and the reporting and follow up of needlestick injuries.
Acknowledgments
The authors would like to thank Dr A Speekenbrink and Mr Graeme Gillespie for assistance in managing the Regional Virus Laboratory database and the support of Mr William Smyth and Mr Glenn Codere in programming and managing the study database. We would also like to acknowledge the help of Mrs Linda McDonald and Mrs Elaine Murray for pooling and ELISA testing the sera and Ms Parvez Murad for PCR testing and genotyping the ELISA reactive samples. Finally, we thank all of the staff of the occupational health departments in Glasgow for their assistance and cooperation over the duration of this study. The study was funded by the Department of Health at the Scottish Office (project number K/OPR/2/2/D321).
Abbreviations used in this paper
- HCV
- hepatitis C virus
- HBV
- hepatitis B virus
- RT-PCR
- reverse transcriptase-polymerase chain reaction