Article Text

Abstract
BACKGROUND AND AIMS Untreated coeliac disease in the mother is associated with lower birth weight. We examined the risk of adverse neonatal outcome when the infant's mother, father, or other relative suffered from known coeliac disease.
METHODS Mothers answered a questionnaire a few days after the birth of their infant. Of a total of 10597 single birth infants from Southeast Sweden, 53 infants had a mother with coeliac disease (father 27, sibling 70, other close relative 442). Adjusted odds ratios and adjusted differences for neonatal outcome were calculated.
RESULTS Infants whose father suffered from coeliac disease had a lower birth weight (95% adjusted confidence interval (CI) −459, −72 g), more often belonged to the low birth weight (LBW) category (LBW ⩽2499 g) (95% CI adjusted odds ratio (AOR) 1.48–17.18), and had a shorter pregnancy duration (95% adjusted CI −1.53, −0.08 weeks) than non-coeliac controls. They also weighed less than infants whose father suffered from other autoimmune diseases (95% CI −549, −93 g). Infants whose mother suffered from coeliac disease had a lower birth weight (95% adjusted CI −370, −74 g) and more often belonged to the LBW category (95% CI AOR 2.60–15.08) than non-coeliac controls. These infants were more often in the LBW category than infants whose mother suffered from non-diabetic autoimmune diseases (95% CI AOR 1.24–9.65). Coeliac disease in other relatives was not associated with any adverse effect on neonatal outcome.
CONCLUSIONS This study suggests that even treated coeliac disease, in either of the parents, has a negative effect on pregnancy, resulting in lower birth weight and perhaps shorter duration of pregnancy.
- coeliac disease
- mother
- father
- newborn
- birth weight
Abbreviations used in this paper
- CD
- coeliac disease
- MCD
- mother with coeliac disease
- FCD
- father with coeliac disease
- SCD
- sibling with coeliac disease
- RCD
- other close relative with coeliac disease (grandparents). MCD, FCD, SCD RCD infants, infants whose mother, father, sibling, or relative suffered from coeliac disease, respectively
- AOR
- adjusted odds ratio
- Ajd diff
- adjusted difference
- LBW
- low birth weight
Statistics from Altmetric.com
Low birth weight (LBW ⩽2499 g) is an independent risk factor for immediate and long term morbidity.1 It is also associated with chronic disease in adult life.2-5 Even small decreases in birth weight predispose for later cardiovascular disease,6 and combined with a high weight gain in the first year of life also increase the risk of type 1 diabetes.7
Coeliac disease (CD) is common in the fertile years, and women with untreated CD more often experience stillbirths and abortions.8-11 ,12 ,13 The live infants suffer an increased risk of intrauterine growth retardation.14 ,15
Nørgard et al compared both untreated coeliac mothers with control mothers, and treated coeliac mothers with control mothers, but could only show a relationship between untreated CD in the mother and LBW.14 Also, Ciacciet al have reported a significantly increased incidence of LBW in untreated coeliac women compared with treated coeliac women but this increase was based on 90% confidence intervals (95% confidence interval (CI) 0.8–44.2).16Recently, Martinelli et al described a high prevalence of CD in 845 screened pregnant women.13 The decrease in infant birth weight of the coeliac women in this study (2601 g v 3164 g in controls) just failed to reach significance.13 Intrauterine growth retardation associated with CD in the mother has also been noted by Gasbarriniet al 15; 6/39 women with intrauterine growth retardation had positive serology tests for CD compared with 0/50 controls.
Hence a gluten free diet is considered crucial for a normal birth in coeliac women.12 ,14 ,16 ,17 However, Ciacciet al suggested that malabsorption may not be the only important factor in the adverse outcome of pregnancy in coeliac mothers.16
It is well known that male gonadal function is reduced in CD18 but there are few data on the effect of CD in the father on neonatal outcome. Both parental genomes are needed for normal embryonic development, and placental development may be more dependent on paternal than maternal genes.19
We hypothesised that malnutrition in the coeliac mother was not the only factor affecting fetal growth and pregnancy duration but that genetic factors associated with CD may play a direct role.20 For this reason we studied neonatal outcome not only when the mother suffered from CD but also when the father, a sibling, or other close relative (grandmother/grandfather) had CD. Secondly, we compared neonatal outcome in infants with a coeliac mother/father with that in infants whose parents suffered from other autoimmune diseases.
The purpose of this study was to investigate the relationship between CD and neonatal outcome, adjusting for important confounding factors such as smoking.21 ,22
Methods
MATERIAL
All 21 700 babies born in Southeast Sweden between 1 October 1997 and 1 October 1999 were invited to participate in a screening programme for prediction of autoimmune diseases, including CD. This study was performed as part of the prospective cohort study ABIS (all babies in Southeast Sweden).
The parents of 15 800 children (72.8%) gave informed consent to participate (fig 1). A few days after birth, mothers answered a questionnaire, including questions on CD in the (child's) mother, father, sisters/brothers, and close relatives (for example, grandmother/grandfather). The multiple choice questionnaire consisted of 117 questions. The diagnosis of CD was based on the answers to these questions. In a sample of patients we compared the questionnaire answers and the clinical records and found a high correlation. The results of the study are based on the first 10 597 single birth questionnaires (fig 1).
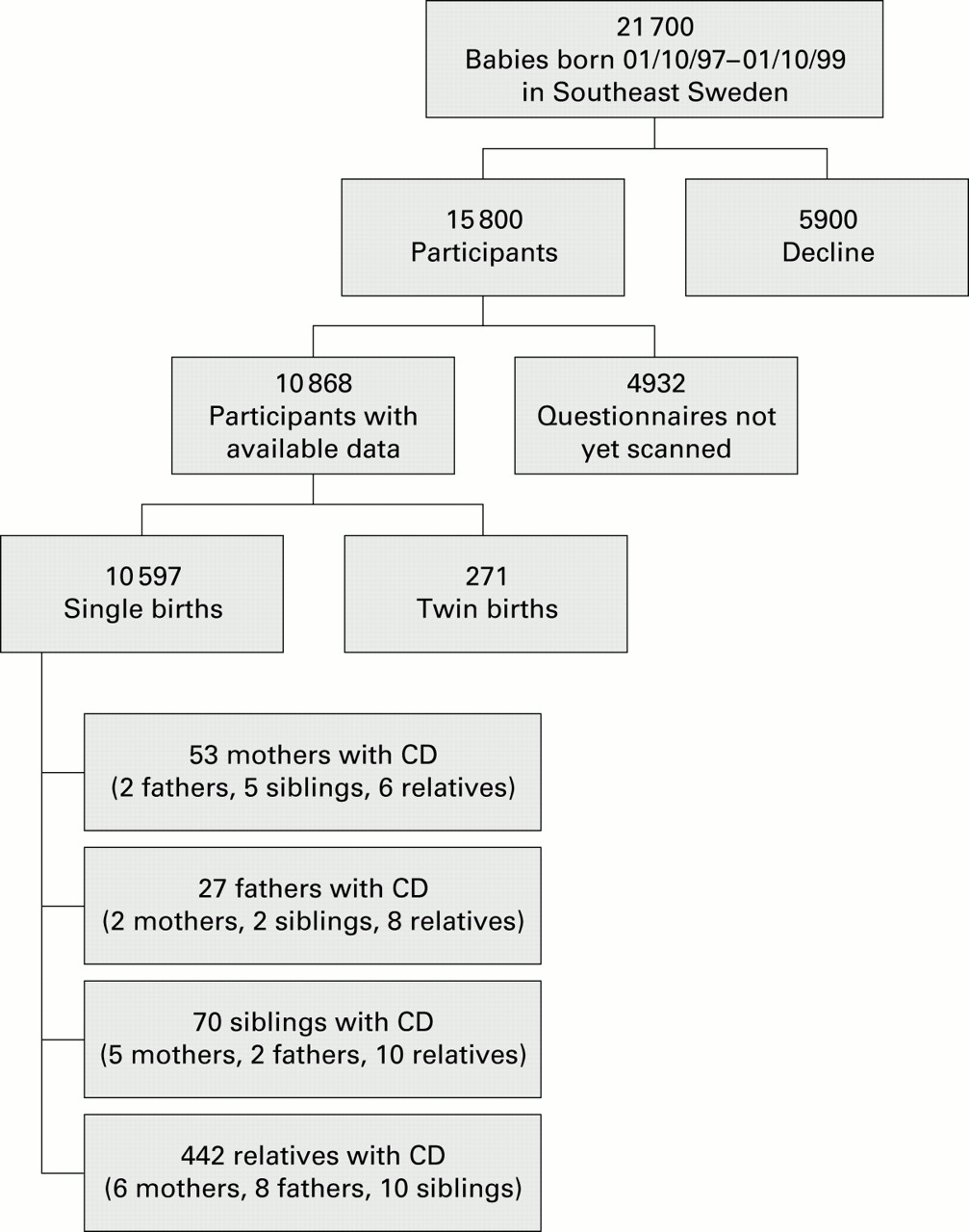
Flowchart of the ABIS study cohort. CD, coeliac disease. Number of infants with a positive history of other relative with CD are presented in parentheses (for example, of 53 infants whose mother had CD, two infants also had a coeliac father, five had coeliac siblings, and six had other close relatives with CD).
We used the following outcome variables: birth week (one week categories (for example, 37 or 38 weeks)), birth weight, birth length, preterm birth (<37 weeks), LBW (⩽2499 g), and neonatal hospital care. “Birth defects” in this paper refer to cases that demanded neonatal hospital care. Birth week, birth weight, and birth length were plotted and found to be normally distributed.
The ABIS study focused on children; we did not examine abortion rates or stillbirths.
INDEPENDENT VARIABLES
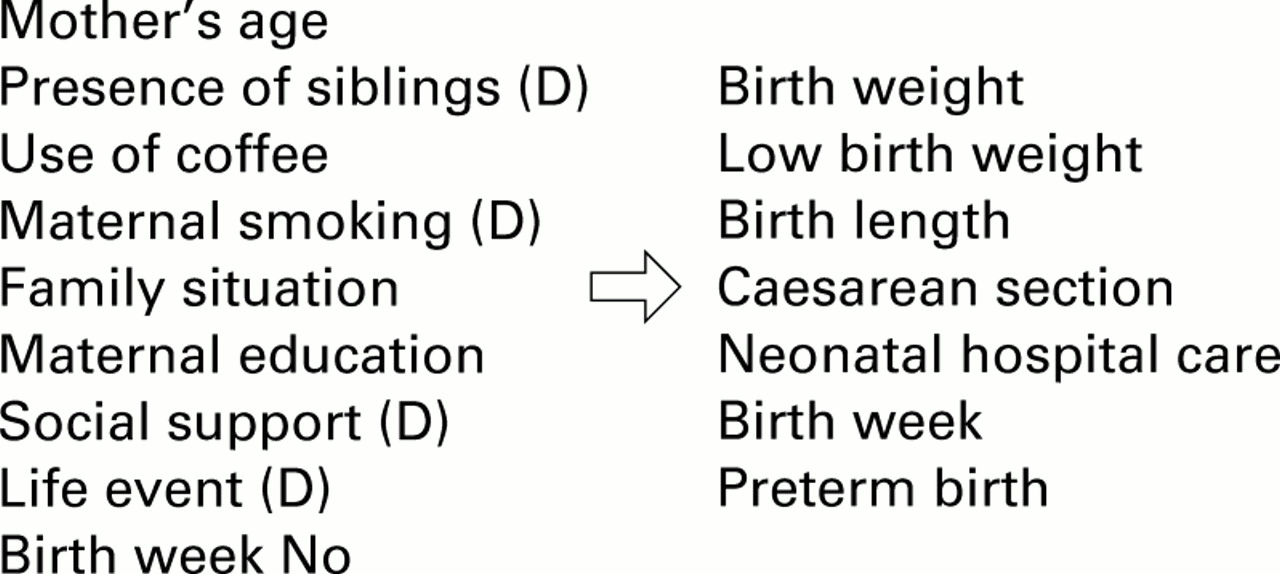
Independent variables are presented in fig 2. In the regression analysis, no more than 10 independent variables were included.

{kind=link}
{kind=link}
Variables in the regression analyses; independent variables, in addition to coeliac disease for either the mother, father, sibling, or other close relative. D, Dichotomised. Birth week No was included as an independent variable only in birth weight analyses.
In the analyses we adjusted for maternal age (mothers were divided into four groups of equal size (15–26, 27–29, 30–32, and 33–47 years)), primipara/multipara, coffee use (levels I–V), maternal education (levels I–VI), family situation (“single”v “living together with the child's father”), and two psychological factors: “sufficient support (for the mother and her future child) from friends and family during pregnancy” and “exposure to life event during pregnancy” (for example, close relative died, separation from partner).
Parental weight was not registered in the perinatal questionnaire and therefore was not included among our independent variables. At the stage of writing 4166 follow up questionnaires (the child being one year old) with data on parental weight (mother and father) have been scanned and were available for analysis. In this sample we found no relationship between CD and parental weight. Characteristics of the mothers in the study cohort are presented in table1.
Characteristics of the mothers in the ABIS study cohort—single births
Election of independent variables
The main purpose of the investigation was to study the effects of CD on the newborn. The purpose of the regression analyses was to adjust for confounders and not to create predictive models for neonatal outcome. Selection of variables was based on literary reviews. We kept the same variables in all regression models, except for birth week (included in the birth weight analyses only).
Comparison with other autoimmune diseases (table 3)
We compared neonatal outcome in infants whose mother suffered from CD (MCD infants) with that of 337 infants whose mother suffered from non-diabetic autoimmune diseases (Hashimoto's disease/hypothyreosis 156, Grave's disease/hyperthyreosis 68, B12 anaemia 40, SLE/lupus erythematosus 8, Mb Addison 4, and rheumatoid arthritis 96 (number of diagnoses in 337 mothers was 372)).
Coeliac disease versus autoimmune diseases and neonatal outcome
The outcome of the MCD infants was also compared with that of 89 infants whose mother suffered from type 1 diabetes mellitus. We did not include these 89 infants in the “autoimmune control group” as infants whose mother suffers from diabetes have an increased risk of fetal complications.23
Infants whose father suffered from CD (FCD infants) were compared with 199 infants whose father suffered from other autoimmune diseases (Hashimoto's disease/hypothyreosis 27, Grave's disease/hyperthyreosis 14, B12 anaemia 23, SLE/lupus erythematosus 7, Mb Addison 4, rheumatoid arthritis 41, and diabetes mellitus type 1, 107 (number of diagnoses in 199 fathers was 223)). None of the controls had CD.
STATISTICAL ANALYSES
The Pearson χ2 test (with Yates' correction) or Fisher's exact test (in 2×2 tables where the expected value of one of the four cells was <5) was used to compare proportions. The unpaired Student's t test was used to compare the means of normally distributed variables. Equality of variances was tested with the Levene's test.24 The type 1 error was set to p=0.05.
Multiple linear regression was adopted for the adjusted analyses of differences in birth week, birth weight, and birth length. Binary logistic regression was used for calculation of adjusted odds ratios (AOR) of the dichotomous variables preterm birth, LBW, caesarean section, and neonatal hospital care. Statistics were calculated on a PC computer using the SPSS 9.0.0.25
ETHICS
This study was part of the ABIS project which was approved by the research ethics committees of the Faculty of Health Sciences, Linköping University and the Medical Faculty of Lund University. Mothers gave their consent after careful written as well as oral information and information via videotape.
Results
PRIMARY OUTCOME VARIABLES
Infants whose father suffered from CD had a lower birth weight, more often belonged to the LBW category, and were shorter than controls (table 2). On average these infants weighed 3273 g compared with the general average birth weight of 3596 g. The adjusted mean difference in birth weight (−266 g) was highly significant (p=0.007).
Coeliac disease in the family and neonatal outcome in single births
Coeliac mothers gave birth to infants with an average birth weight of 3447 g. The 95% CI for the crude difference in birth weight (MCD infants) did not reach significance (−299, 2 g) but adjusting for confounders revealed a difference associated with CD (−370, −74 g). There was no difference in birth weight between MCD and FCD infants.
The risk of LBW among FCD infants was five times higher than that in the general population (adjusted for confounders); 11.1% of FCD infants (3/27) were classified as LBW while the corresponding value among controls was 2.5% (265/10 526). The risk of LBW in MCD infants was even higher, with an AOR above 6 (95% CI AOR 2.60–15.08). Two infants had both a coeliac mother and a coeliac father. These infants were born after 40 and 41 weeks, respectively, and did not suffer from LBW.
Pregnancy duration for infants whose father suffered from CD was shorter than among other infants. The proportion of preterm births in FCD infants was increased and close to significant, with an AOR of 3.32. The average duration of pregnancy in MCD infants did not differ from that in the general population, and the proportions of infants classified as preterm in the MCD infants and controls were identical (4.1% v 4.2%).
In the control group, one of nine pregnant women underwent a caesarean section; a similar proportion was found in MCD infants, SCD infants (infants whose sibling suffered from CD), and RCD infants (infants whose relative (grandmother/grandfather) suffered from CD).
Infants whose mother suffered from CD were more prone than control infants to spend time in the neonatal ward; 9/53 (17%) of these infants were hospitalised. Of 53 MCD infants, four were hospitalised due to LBW (other reasons were respiratory distress, infection, birth defect, and surveillance). Because of the small number of events in individual categories of neonatal complications, we have refrained from statistical comparisons. Of 27 FCD infants, three were hospitalised due to low birth weight and two due to jaundice.
Infants whose sibling/siblings or other close relative had CD did not differ from controls for any outcome variable (table 2).
Further regression analyses
When we performed a backward regression analysis of birth weight, the following independent variables were left in the final model of FCD infants: smoking, mother's age, previous infant, birth week, and CD in the father. Also, in this model, CD in the father correlated with a lower birth weight in the infant (95% CI for adjusted difference (Ajd diff) −459, −72 g; p=0.007). The adjusted difference in birth weight for FCD infants did not change when parental weight (of both mother and father; Ajd diff −370 g; 95% CI −706, −34 g) or infant's sex (Ajd diff −370 g; 95% CI −580, −160 g) was included in the multiple linear regression analyses. Regression analyses including parental weight were based on a smaller sample than the other analyses (eight coeliac fathers and 22 coeliac mothers).
Pregnancy duration of FCD infants did not change when “sex of the infant” was added to the list of independent variables in the regression analysis (−0.81 weeks; 95% CI −1.53, −0.08 weeks).
COMPARISON WITH OTHER AUTOIMMUNE DISEASES
MCD infants were more often LBW than the 337 infants whose mother suffered from non-coeliac and non-diabetic autoimmune diseases.
Infants to coeliac mothers had, as expected, a lower mean birth weight than infants to diabetic mothers (table 3). The difference in birth weight between MCD infants and the control group (diabetic mothers not included) was not significant at the 95% CI level but was significant at the 94% CI level (−349, 0 g). The risk of LBW was five times higher in MCD infants than in infants to diabetic mothers. Caesarean section, short pregnancy duration, and neonatal hospital care were more common in infants with diabetic mothers.
FCD infants had a lower birth weight than infants whose father suffered from non-coeliac autoimmune diseases (table 3). The odds ratio (OR) for LBW was just below the 95% significance level but reached significance at the 94% CI level (OR 4.02, 1.00–16.15). Adjusting for differences in variance (Levene's test) reduced the difference in pregnancy duration between FCD infants and the control group, and the “adjusted for variance” difference was not significant. FCD infants did not differ from their autoimmune controls regarding frequency of caesarean section, neonatal hospital care, or prevalence of preterm birth.
A comparison between FCD infants and infants whose father suffered from diabetes showed an increase in the incidence of LBW (OR 13.37, 95% CI OR 1.33–134.12; p=0.007) and a lower birth weight (difference −327 g; 95% CI difference −564, −90 g; p=0.0275) in FCD infants. Except for a shorter height (birth length) in FCD infants, the two groups did not differ in terms of preterm birth rate, caesarean section rate, or use of neonatal hospital care.
ADDITIONAL ANALYSES
The flowchart in fig 1 presents the number of interrelationships between groups with coeliac patients. Almost 30% of FCD infants also had other close relatives with CD (p<0.001). Ten per cent of mothers with CD had at least one other child with CD and two infants had both a coeliac mother and a coeliac father. The correlations between MCD infants (and other coeliac groups—that is, FCD, SCD, and RCD infants), FCD infants (and other coeliac groups), SCD infants (and other coeliac groups), and RCD infants (and other coeliac groups) were all significant (<0.02), as assessed using the χ2test/Fisher's exact test. There were no significant differences in the proportions of twins between the coeliac groups and the control group (χ2) (number of twins: mother with CD 0/53; father with CD 0/27; sibling with CD 2/72; relative with CD 12/454; all study cohort 271/10 868).
The proportion of smokers, as tested with Fisher's exact test, did not differ between mothers with CD and controls (p=0.829).
There were no differences in mother's age at delivery between coeliac mothers and controls (95% CI crude difference −2.27, 0.40 years). Neither did age of the mother with coeliac partners differ from that of controls (95% CI crude difference −1.42, 2.23 years). Fathers with CD were the same age at delivery as the control group (95% CI crude difference −3.12, 1.18 years).
Discussion
Our study suggests that infants whose father suffers from CD have a lower birth weight and shorter pregnancy duration than controls. These infants suffer a five times higher risk of LBW (⩽2499 g). Infants to coeliac mothers suffered an even higher risk of LBW (OR 6.26). None of our neonatal outcome parameters were affected by having a sibling or other close relative with CD. Compared with autoimmune controls, even when type 1 diabetes was excluded, CD in either the mother or father affected birth weight. The affected LBW infant suffers an increased risk of future adult disease,5 including cardiovascular diseases such as stroke,26 and diabetes mellitus.27
This study was a prospective population based cohort study, encompassing more than 10 000 infants. Hence we have avoided skewed recruitment of controls. The data are up to date in that all data originate from births after 1 October 1997. Our regression analyses included several important confounders, which in earlier studies on CD and neonatal outcome were neglected.14 Adjustment for smoking, coffee use, and psychological factors for example resulted in a an adjusted 95% CI for birth weight in MCD infants below zero, while the crude 95% CI was not significant. Differences between our results and earlier studies may be explained at least in part by our adjustment procedure.
Smoking may play an important role in both CD21 and neonatal outcome.22 ,28 In contrast with the study of Snook et al we did not find a decreased prevalence of smokers among coeliac mothers (9.4%v 11.5% in the general population).21
The diagnosis of CD was based on the mothers' answers to the ABIS questionnaire. This questionnaire was answered some days after delivery when the mother was physically and mentally in a position to go home and take care of her child. We also verified the coeliac diagnosis in the clinical records of a sample of patients.
Sweden has one of the highest prevalences of CD in the world.29 With this goes an awareness of the disease and we do not expect to have missed a significant number of diagnosed mothers or fathers with CD. However, there may have been “silent” coeliac patients in our cohort. In our study, adverse neonatal outcome was seen in mothers with known CD. To our knowledge, no large scale screening programme for CD has been performed in the last 30 years in the study area. Most mothers and fathers with CD in the ABIS study would therefore have been diagnosed due to symptomatic disease (with gluten containing diet). The prevalence of CD in the adult ABIS population ((53+27)/(2×10 597)=3.8/1000) is in agreement with earlier data from Sweden.29 Focusing on the living child may however underestimate the true prevalence of CD as the disease is associated with abortions and stillbirths.9 ,10 ,13 ,16
In spite of an assumed gluten free diet, single birth infants from mothers with known CD had lower birth weights than controls. Previous studies have identified a decrease in birth weight in infants born to mothers before diagnosis (assuming that the mother suffered from CD at the time of that delivery) but not after diagnosis.14 ,16The before versus after phenomenon has been explained by diet counselling and general health advice. An explanatory model focusing on (low) diet compliance does not however address the adverse outcome in FCD infants. In fact our AOR for LBW for MCD/FCD infants was almost identical to that of the study of Ciacci et al,16 although we studied treated coeliac parents.
The large number of regression analyses increases the risk of mass significance. However, our data showed a strong relationship between CD in the father and an increased proportion of LBW infants (positive Fisher's exact test) (AOR 5.05, p=0.010). The reduction in birth weight (crude difference coeliac fathers −323 g) was very close to the difference in birth weight between cases and controls in the study of Martinelli et al, had the three extreme premature infants in that study (24, 24, and 26 weeks) been excluded (−312 g) (these infants died soon after birth and no Apgar score at one and five minutes of age had been recorded).13Our results suggest that malnutrition cannot be the sole or even the major cause of adverse outcome in newborns with coeliac parents.
CD in either parent influenced birth weight compared with the general population or autoimmune controls. Autoimmune reactions may explain LBW in coeliac mothers. Gliadin per se in coeliac patients induces cytokine production in peripheral blood mononuclear cells30 and accompanying cytokines such as tumour necrosis factor α and interleukin 12 could perhaps have an adverse effect on fetal outcome.31 Gluten induced enteral inflammation would have ceased on a gluten free diet; also, FCD infants were affected. A hypothesis based on ongoing enteral intestinal inflammation due to gluten intake in the mother (affecting birth weight) is not valid for FCD infants.
With increasing distance to a coeliac relative the influence of CD on birth weight in this study tapered. This finding supports our hypothesis that genetics plays an important role in neonatal outcome for infants with either a coeliac mother or a coeliac father.
It is well known that CD is closely related to certain HLA types20 but these HLA types are also closely related to other autoimmune diseases32 ,33: we found no decrease in birth weight in these other diseases. FCD infants had a lower birth weight than children of fathers with other autoimmune diseases, including type 1 diabetes. Thus if HLA is not the genetic locus conferring LBW, this indicates that other genetic factors in CD are related to LBW. Non-HLA genetic loci play an important role in CD although three published sibling pair linkage studies have not agreed on the location of these genes.34-36
Both parental genomes are needed for normal embryonic development although the mechanisms in the case of the coeliac parent and adverse neonatal outcome are not clear. Genomic imprinting refers to marking of genes that results in monoallelic expression (either maternal or paternal).37 Imprinted genes, sometimes occurring in clusters (for example, chromosomes 11 and 1537) are crucial for placental development38 (for example, insulin-like growth factor 2 gene,39 Peg 3 gene40) and intrauterine growth. Fetal cytokine production also depends on genetic factors. The presence of tumour necrosis factor α promoter polymorphism is higher in coeliac patients (32%) than in controls (8%) and independent of the linkage disequilibrium with the DQA1*0501*allele.41 Inheritance of such promoter genes could perhaps affect fetal development.
In conclusion, the results of this study indicate the importance of non-nutritional factors for neonatal outcome in infants to men and women with CD. Genetic factors play a role not only in the risk of developing CD but perhaps also for neonatal outcome in couples where either of the parents suffers from the disease.
Acknowledgments
We thank the paediatricians Eric Carlsson, Kalmar, Hans Edenvall, Karlskrona, Stig Edvardsson, Växjö, Jan Hammersjö, Västervik, Calle Johansson, Jönköping, and Maria Nordvall, Norrköping, who have been important for motivating the different regions to participate in ABIS. We are grateful to all children and parents participating in ABIS, to all staff at mother and baby health care centres and at obstetric departments whose willingness to collaborate has been of crucial importance. Many thanks to the ABIS nurses Caroline Berggren, Christina Larsson, and Iris Franzén who have been so enthusiastic and encouraging, and to Inger Hagström and her team for scanning the questionnaires so carefully. This study was generously supported by the JDF-Wallenberg Foundation, the Swedish Medical Research Council (MFR) K99-72X-11242-05A, the Swedish Child Diabetes Foundation (Barndiabetesfonden), the Söderbergs Foundation, and the Novo Nordisk Foundation.
Abbreviations used in this paper
- CD
- coeliac disease
- MCD
- mother with coeliac disease
- FCD
- father with coeliac disease
- SCD
- sibling with coeliac disease
- RCD
- other close relative with coeliac disease (grandparents). MCD, FCD, SCD RCD infants, infants whose mother, father, sibling, or relative suffered from coeliac disease, respectively
- AOR
- adjusted odds ratio
- Ajd diff
- adjusted difference
- LBW
- low birth weight
References
Linked Articles
- Commentary