Article Text

Abstract
BACKGROUND Hypersensitivity to distension of the stomach is a frequent finding in functional dyspepsia. During gastric distension studies both wall tension and elongation are increased.
AIM We wished to distinguish changes in wall tension from changes in elongation in the genesis of perception of mechanical stimuli originating from the proximal stomach in healthy subjects.
SUBJECTS AND METHODS Twenty six volunteers were studied using gastric barostat and antroduodenal manometry. In 14 subjects, stepwise isobaric and isovolumetric distensions were performed before and during erythromycin infusion. In all volunteers, on a separate occasion, phasic contractions of the proximal stomach were detected as intraballoon pressure increases during fixed volume inflation. These contractions were matched with perception changes during two 10 minute periods, before and during administration of erythromycin.
RESULTS Erythromycin significantly lowered the perception and discomfort thresholds during stepwise gastric distension. During fixed volume inflation, erythromycin increased the number and amplitude of fundic contractions and enhanced their perception from 51.1 (7.4)% to 64.0 (4.7)%. The proportion of perception score increases coinciding with fundic contractions increased from 47.3 (0.7)% to 81.5 (0.5)%. The amplitude of correctly identified isolated fundic pressure waves was higher compared with non-identified waves.
CONCLUSIONS These results support the hypothesis that changes in gastric wall tension may be involved in the genesis of symptoms originating from the stomach.
- visceral hypersensitivity
- stomach physiology
- mechanoreceptors
- wall tension
- erythromycin
- barostat
Abbreviations used in this paper
- Ery
- erythromycin
- MDP
- minimal distending pressure
Statistics from Altmetric.com
Functional dyspepsia is still an ill defined clinical syndrome.1 The characteristic feature of patients diagnosed with functional dyspepsia is the presence of recurrent upper abdominal pain or discomfort without identifiable cause by conventional diagnostic means.2 The symptoms are related to ingestion of a meal in 62% of patients.3 Several pathophysiological mechanisms have been proposed, and recent research has proposed an important role for visceral hypersensitivity in symptom production of functional gastrointestinal disorders.4 ,5
In patients with functional dyspepsia, balloon distension of the proximal stomach can reproduce the symptoms from which they commonly complain.6 In these patients, first perception and discomfort during distension of the proximal stomach with a balloon occur at lower thresholds than in healthy subjects.7-10Even though the reasons for this hypersensitivity to distension of the proximal stomach are unclear, mechanoreceptors receptive to either changes in elongation or wall tension, or both, must be activated to transduce the distending stimulus. It has been proposed that the gastric wall contains two types of mechanoreceptors (fig1).11 In animals, serosal mechanoreceptors arranged in a parallel fashion respond to stimuli that elongate the stomach wall.12 Mechanoreceptors arranged in series respond to stimuli that increase or decrease the tension of the stomach wall.13 ,14 Gastric distension in humans increases both elongation and wall tension of the stomach. Hence distension studies do not allow distinction between these mechanoreceptors for induction of perception (fig 1).11 Recently it was suggested that the simplified law of Laplace can be used to estimate wall tension during gastric barostat studies, and that this level of wall tension determined the level of perception during distension studies.15 Others however found that most of the variance in sensation scores during a pharmacological study of gastric sensitivity was not accounted for by changes in wall tension, estimated by Laplace's law.16 ,17 All of these studies compared the sensitivity to gastric distension before and after administration of agents that relax the proximal stomach. A combination of gastric distension and relaxation is invariably associated with elongation of the proximal stomach but may have opposing effects on tension receptors. An alternative way to assess the role of volume (elongation) versus tension in gastric sensation might be to evaluate the influence of an agent that contracts the proximal stomach. An additional method to distinguish between the roles of elongation and tension may be to use volume clamping by fixed volume inflation of an intragastric balloon. When the proximal stomach contracts isometrically against the fixed volume balloon, elongation is unchanged while changes in intraballoon pressure directly reflect changes in wall tension.
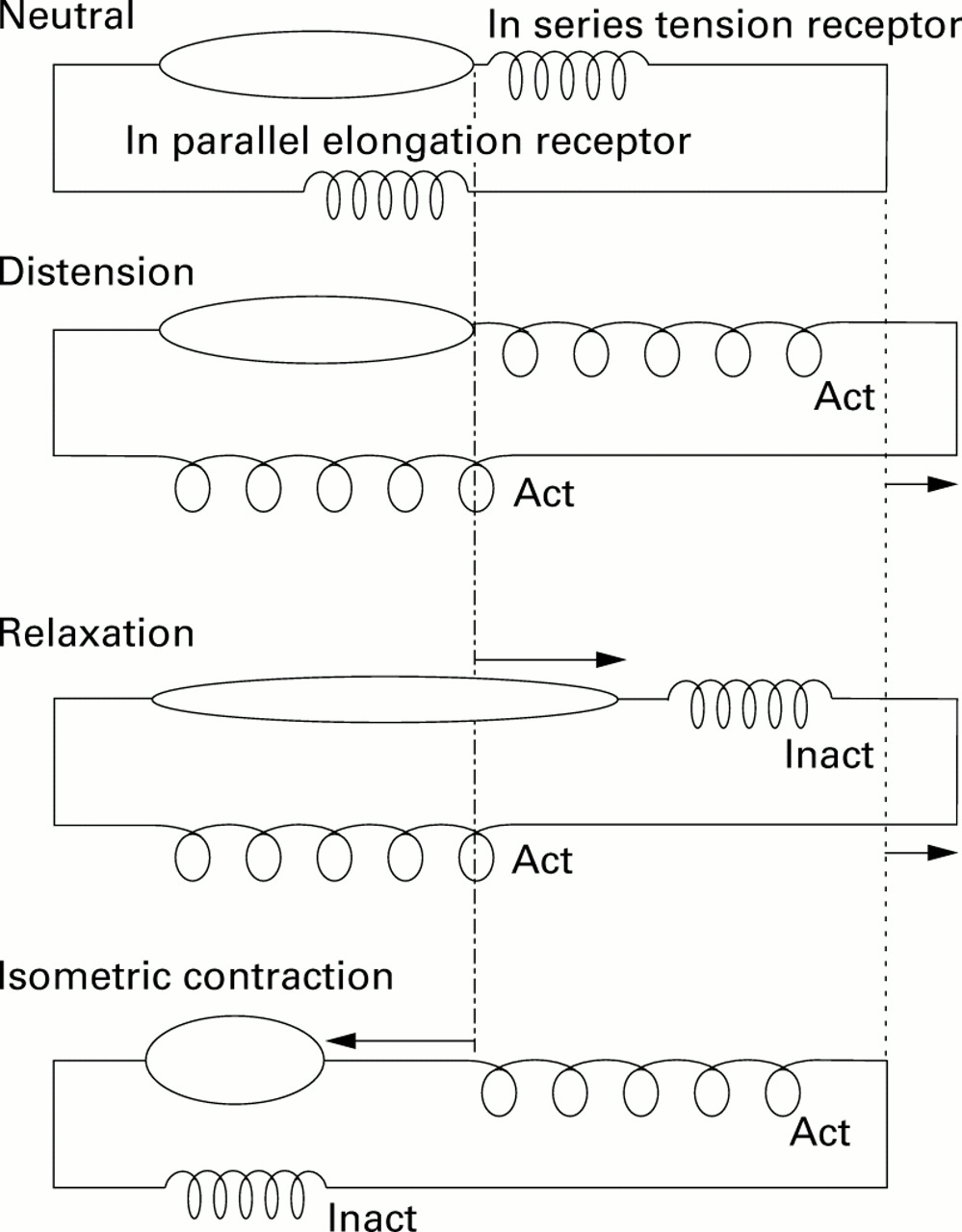
Schematic model of the proximal stomach wall with muscular component, in series tension receptor, and in parallel elongation receptor. The four panels represent the behaviour of the model in various experimental conditions. Top: Neutral condition; second panel: during distension both elongation and tension receptors are activated (Act). Muscular contraction status is unchanged; third panel: during relaxation, elongation but not tension receptors are activated. The muscular component is lengthened; bottom: during isometric contraction only tension receptors but not elongation receptors are activated. The muscular component is shortened. Inact, inactivated.
Our aim was to distinguish between changes in wall tension and changes in elongation in the genesis of perception of mechanical stimuli originating from the proximal stomach in healthy subjects. Perception of graded distensions or of a continuous distending stimulus in the presence or absence of erythromycin (Ery) was studied with two different protocols that included gastric barostat and antroduodenal manometry methodology. To achieve an in vivo model of isometric contraction of the proximal stomach, we used Ery to increase circumferential fundic wall tension and to induce fundic phasic contractions in the presence of a fixed volume inflated balloon placed in the proximal stomach.
Methods
STUDY SUBJECTS
Twenty six healthy volunteers (18 men and eight women; mean age 24.0 (2.0) years) were included. None of the subjects had symptoms or a history of gastrointestinal disease or drug allergies, or were receiving any medication. Informed consent was obtained from each participant. The ethics committee of the University Hospital had previously approved the protocol.
STUDY TECHNIQUE
After an overnight fast of at least 12 hours, volunteers were orally intubated with a stationary perfused antroduodenal manometry catheter, with recording sites located 6, 4, and 2 cm above and 2 and 4 cm below a radio-opaque marker that was placed at the pylorus under fluoroscopic control. Afterwards, a double lumen polyvinyl tube (Salem sump tube 14 Ch; Sherwood Medical, Petit Rechain, Belgium) with an adherent plastic bag (1200 ml capacity; 17 cm maximal diameter) finely folded was introduced through the mouth. The position of the bag in the gastric fundus and of the manometry catheter were checked fluoroscopically. Both probes were secured to the subject's chin with adhesive tape.
The antroduodenal manometry catheter was connected to a low compliance hydraulic capillary infusion pump. The polyvinyl tube with the bag was then connected to a computer driven programmable volume displacement barostat device (Synectics Visceral Stimulator; Synectics, Stockholm, Sweden). The barostat device can deliver volume ramps or pressure steps at different rates while simultaneously monitoring pressure and volume. Intrabag pressure, bag volume, and six antroduodenal manometry channels were recorded and monitored online using a specially designed software program (Polygram for Windows; Synectics). Sampling rate for all variables was 8/second. To unfold the intragastric bag, a fixed volume of 500 ml air was inflated over two minutes with the subject in a recumbent position. After a 10 minute equilibration period, subjects were positioned in a comfortable sitting position with the knees slightly bent (80°), in a bed specifically designed for that purpose. Finally, an intravenous catheter was placed in an antecubital vein and flushed with saline.
STUDY PROTOCOL
Study 1: perception of stepwise gastric distensions before and after erythromycin and effect of erythromycin on tone of the proximal stomach
The effect of Ery on the perception of stepwise distension of the proximal stomach was studied in 14 volunteers. After a 30 minute accommodation period, minimal intragastric distending pressure (MDP) was first determined as the lowest pressure level that provided an intrabag volume of 30 ml or more.11 This pressure level equilibrates intra-abdominal pressure and was determined with subjects in the sitting position by increasing intrabag pressure with 1 mm Hg every three minutes. After a 30 minute accommodation period, we performed one series of stepwise isobaric distensions and one series of isovolumetric distensions. The sequence of the type of distensions was randomised using sealed envelopes so that half of the subjects underwent isobaric distensions first followed by isovolumetric distensions, and the other half underwent distensions in reverse order. During isobaric distensions the selected pressure was increased by 2 mm Hg every two minutes starting from MDP, whereas during isovolumetric distensions balloon volume was increased by 100 ml and kept constant during the whole two minute distension step. During the distension protocols, at the end of each distending step, subjects were instructed to score their perception of upper abdominal sensations induced by either isobaric or isovolumetric distension. Perception was graded on a graphic rating scale that combined verbal descriptors on a scale graded 0–6.11 The end point of each sequence of distensions was established at an intrabag volume of 1000 ml or when the subjects reported discomfort or pain (score 5 or 6). Previously, we have demonstrated the reproducibility of the responses and perception scores to gastric distensions performed according to this protocol.18 After performing both series of distensions, the pump was switched to barostat mode (isobaric conditions) and the pressure level was adjusted to obtain an intrabag volume of approximately 400 ml. This corresponded most often to MDP+4 mm Hg. After 30 minutes of baseline recording, an infusion of 10 mg/min of erythromycin lactobionate (Erythrocine; Abbott, Ottignies-LLN, Belgium) was started. Ten minutes after initiation of the infusion, graded distensions were repeated in the same order as before administration of Ery.
Data analysis and statistics
To evaluate the effect of Ery on gastric tone, mean intrabag volumes during the five minute period before and during the initial two five minute periods while the drug was administered were compared using the paired Student'st test. To evaluate the effect of Ery on the mechanical characteristics of the wall of the proximal stomach during gastric distension, for each two minute distending period the average of the dependent variable (volume or pressure) was calculated. Pressure-volume curves of isobaric distensions and volume-pressure curves of isovolumetric distensions before and after Ery were compared by two way ANOVA.
Perception threshold was defined as the first level of pressure (during isobaric distensions) or volume (during isovolumetric distensions) that evoked a perception score of 1 or more. Discomfort or pain threshold was defined as the first level of pressure (during isobaric distensions) or volume (during isovolumetric distensions) that provoked a perception score of 5 or more. The perception and discomfort thresholds before and after Ery were compared using the paired Student's t test. In addition, areas under the curve of the pressure-perception and volume-perception relationships before and after Ery were also compared using the paired Student's t test. All data are expressed as mean (SEM). Differences were considered significant at the 5% level.
Study 2: perception of phasic pressure waves before and after erythromycin
Perception of phasic pressure waves of the proximal stomach was studied in all 26 volunteers. Fourteen of these 26 volunteers had undergone the first study on a separate day at least 72 hours before. After an accommodation period of 30 minutes after the unfolding of the bag, subjects underwent isovolumetric distension with the same protocol as in study 1. Subsequently, the balloon was kept deflated during 20 minutes. After this resting period the balloon was inflated at a fixed volume corresponding to the perception threshold determined during the initial distension procedure. Volunteers were asked to indicate perception of upper abdominal symptoms using a keypad connected to the recording computer, with the same rating scale as in study 1. They were instructed to score every 30 seconds or earlier if they noticed any change in perception. The balloon was kept inflated for 10 minutes and intraballoon pressure was constantly recorded. Twenty minutes after balloon deflation an intravenous infusion of 10 mg/min Ery was started. Ten minutes after the start of Ery, the balloon was inflated to the same volume as before for a new period of 10 minutes, while subjects were asked to score their symptoms again.
Data analysis and statistics
The intraballoon pressure baseline was calculated using dedicated software developed in our own laboratory (Andrioli, KULeuven). A phasic pressure wave of the proximal stomach was defined as an increase in intraballoon pressure of 5 mm Hg above baseline for at least five seconds. For each pressure wave, the amplitude and area under the curve were calculated. If the onset of this pressure wave was followed by a rise in perception score within 10 seconds it was considered as recognised. Every antral and duodenal channel of the perfusion manometry tracings was analysed in a similar fashion to intraballoon pressure. The proportion of perceived fundic, antral, and combined fundic and antral contractions before and during infusion of Ery was compared using the χ2 test. To rule out non-specific increases in score, the proportion of score increases effectively corresponding to pressure waves was calculated and compared using the χ2 test. All results are expressed as mean (SEM).
Results
EFFECT OF ERYTHROMYCIN ON TONE OF THE PROXIMAL STOMACH
MDP was 8.1 (1.5) mm Hg. Before Ery, mean volume of the intragastric barostat balloon was 425 (30) ml. The drug induced a profound and significant tone enhancement of the proximal stomach reflected by a decrease in balloon volume to 266 (30) and 126 (35) ml (p<0.001, p<0.001), respectively, during the first and second five minute periods following the start of infusion (fig 2). Ery induced fundic tone enhancement occurred significantly earlier than antral phase III-like activity (85 (9) v 224 (30) seconds after infusion was started; p<0.01) (fig 3). Antral contractions were not accompanied by phasic changes in intraballoon volume.

Influence of intravenous (IV) erythromycin on tone of the proximal stomach. Gastric tone is reflected by the volume of a barostat balloon in the proximal stomach. Intraballoon pressure is kept constant at a fixed pressure selected to obtain an initial volume of approximately 400 ml. Values are mean (SEM). Student's t test: **p<0.01 (n=14).
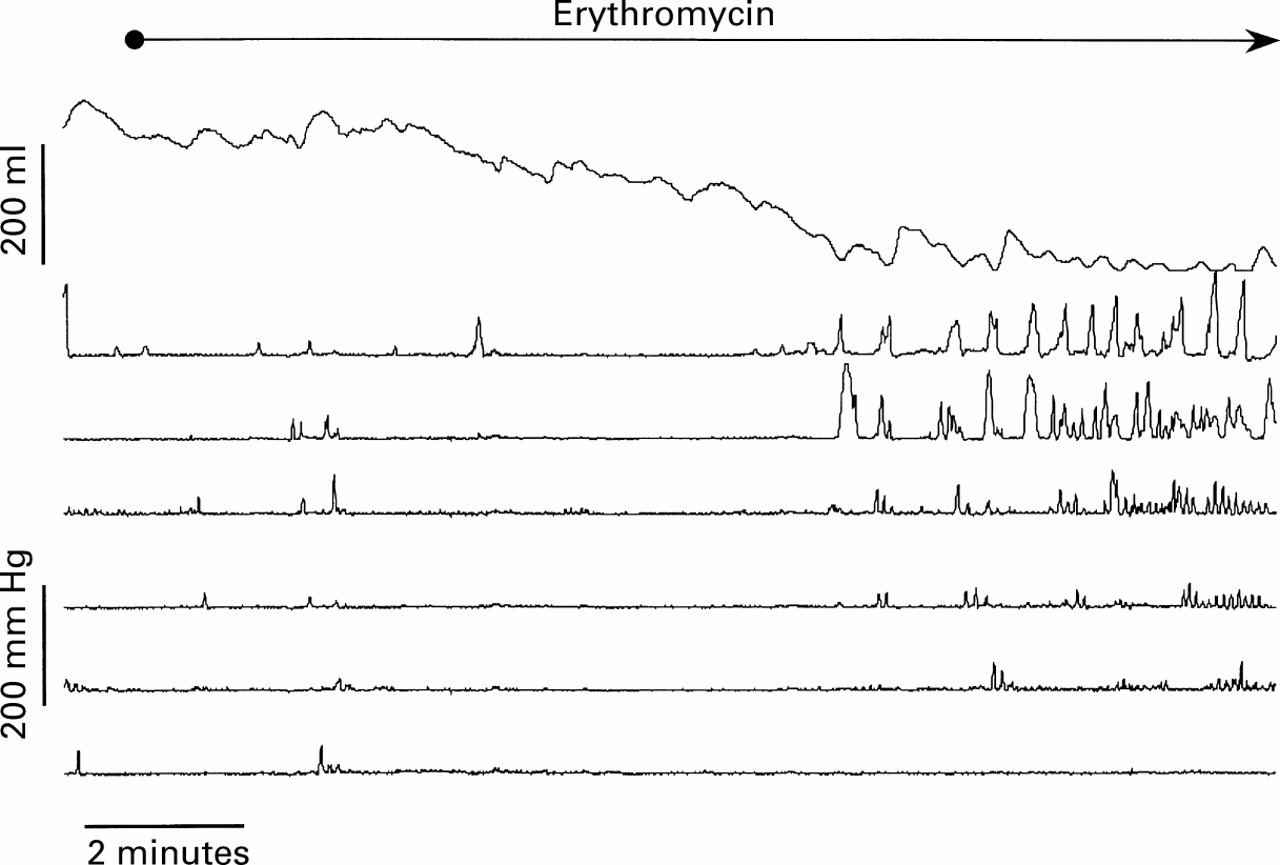
Influence of erythromycin 10 mg/min given intravenously on motor activity of the stomach and duodenum. Combined barostat of the proximal stomach and antroduodenal manometry in a healthy volunteer. The highest trace represents intraballoon volume. The second and third channels show antral pressure, and the four other channels duodenal pressure. Erythromycin induced enhancement of fundic tone (represented as a decrease in intraballoon volume) which preceded the appearance of antral phase III-like contractions.
INFLUENCE OF ERYTHROMYCIN ON DISTENSION OF THE PROXIMAL STOMACH
During isobaric distensions, at identical distending pressures, intragastric volumes during Ery were significantly lower than the corresponding volumes prior to drug administration (p<0.05). Similarly, duringisovolumetric distensions, higher intragastric pressures were recorded at every distension step during administration of the drug (p<0.05).
Ery significantly decreased the pressure at threshold perception (4.3 (0.8) v 2.3 (0.7) mm Hg above MDP; p=0.05) or discomfort (9.2 (0.7) v 7.8 (0.8) mm Hg above MDP; p=0.01) during isobaric distensions. Similar results were obtained duringisovolumetric distensions: mean perception threshold (264 (41) v 157 (36) ml; p<0.01) and mean discomfort threshold (700 (38) v521 (59) ml; p<0.01) were both lowered during administration of Ery. The areas under the curve of the pressure-perception and volume-perception relationships were significantly higher during Ery (103.8 (3.9) v 114.0 (3.4) mm Hg above MDP×perception score unit (p<0.01) and 2950 (150)v 3678 (203) ml×perception score unit (p<0.01), respectively) (fig 4).

Distension-perception relation during isovolumetric distensions of the proximal stomach. A barostat balloon placed in the proximal stomach is inflated stepwise with increasing volumes (step increment 100 ml, step duration two minutes). Perception of abdominal discomfort is recorded at the end of each distension step on a scale ranging from 0 to 6, before and during intravenous infusion of erythromycin. Erythromycin (10 mg/min) significantly enhanced perception of gastric distension. Values are mean (SEM) perception scores (area under the curve; p<0.01) (n=14).
PERCEPTION OF PHASIC ACTIVITY OF THE PROXIMAL STOMACH
The balloon was inflated at a fixed volume of 265 (21) ml which was the perception threshold determined during the initial stepwise distension protocol.
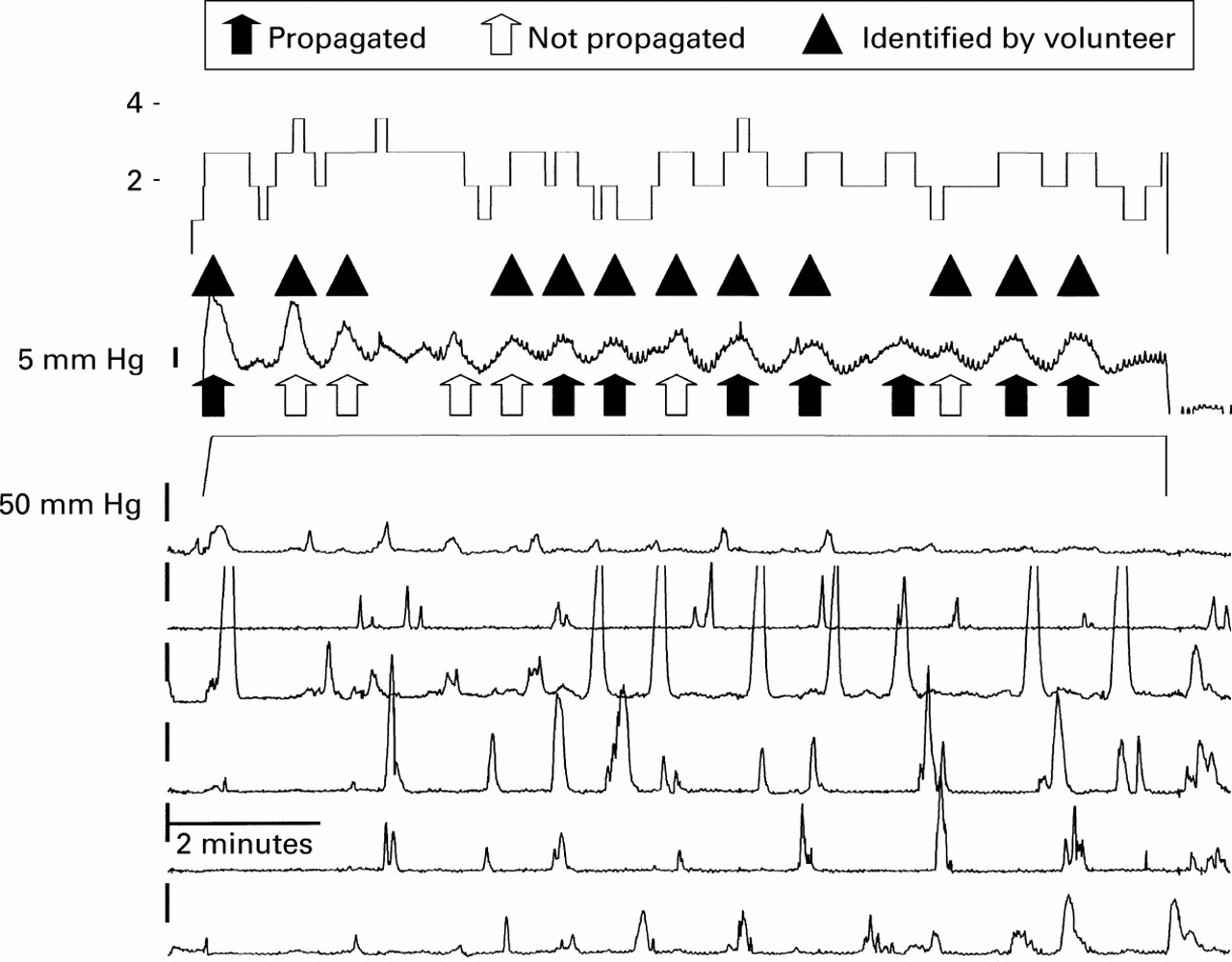
During the first perception period of 10 minutes, a mean of 4.5 (0.7) phasic pressure waves of the fundus occurred. Thirty two per cent of these were followed by an antral pressure wave. Only 0.8 (0.4) isolated antral pressure waves occurred during the same period. There were no differences in amplitude between the isolated fundic and fundic pressure waves propagated to the antrum. Ery significantly increased both the amplitude (20.6 (0.5) v 22.8 (0.3) mm Hg; p<0.01) and number (4.5 (0.7) v 12.4 (0.8); p<0.01) of fundic pressure waves.
When consciously perceived by volunteers, phasic contractions of the proximal stomach were most frequently described as a sensation of increasing fullness. Using the fluctuations in this perception, volunteers could correctly identify 51.1 (7.4)% of fundic pressure waves in contrast with only 6.0 (4.2)% of isolated antral contractions. A characteristic tracing is depicted in fig 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Perception of phasic activity of the proximal stomach. Combined barostat of the proximal stomach and antroduodenal manometry in a healthy volunteer. The highest trace represents perception score. The second and third traces shows intraballoon pressure and volume, respectively. The six other traces represent antroduodenal manometry. This tracing illustrates fundic pressure waves propagated or not to the antrum. Some of the fundic pressure waves were identified by the volunteer.
During Ery, the proportion of perceived phasic contractions of the proximal stomach compared with those identified on the intraballoon pressure tracing significantly increased to 64.0 (4.7)% (p<0.01). Accuracy, expressed as the proportion of score increases corresponding to fundic pressure waves, increased from 47.3 (0.7)% to 81.5 (0.5)% (p<0.01).
The amplitude and area under the curve of the correctly identified isolated fundic pressure waves was higher compared with non-perceived pressure waves (23.2 (0.5) v 21.9 (0.5) mm Hg (p=0.06) and 95.9 (4.1) mm Hg×seconds v109.5 (4.0) mm Hg×seconds (p=0.02), respectively).
Discussion
Hypersensitivity to distension of the proximal stomach is found in a large proportion of patients presenting with functional dyspepsia.6 ,8 ,18 The mechanism underlying this hypersensitivity is not fully understood.19 In theory, dysfunction leading to visceral hypersensitivity may be located at one or more of the levels involved in transduction of a stimulus such as distension of the proximal stomach. Defective processing may occur at the level of mechanoreceptors in the gastric wall, or of afferent nerves or their targets in the central nervous system and result in the perception of discomfort or pain of an otherwise normal sensorial stimulus. In this study, we focused on the distinction between changes in wall tension and changes in elongation as the initiating stimuli activating the brain-gut axis.
It has been shown previously that changes in gastric tone have a major influence on the perception of stepwise gastric distensions.11 In agreement with the results of Bruley des Varannes et al, administration of Ery resulted in a significant increase in gastric tone.20 When we repeated gastric distensions during Ery infusion (that is, under conditions of increased tone of the proximal stomach) subjects reported significantly higher perception scores at identical distending volumes or pressures. Gastric distension causes both elongation and increase in tension of the gastric wall. Isobaric and isovolumetric distensions have different effects on elongation and tension. Under isobaric conditions, at equal distension levels but different levels of gastric tone, both elongation and tension are influenced. In contrast, under isovolumetric conditions, at equal distension levels but different levels of gastric tone, only tension varies in the segments in close apposition to the balloon. The fact that we measured significantly increased perception of gastric distension during Ery infusion also in isovolumetric mode supports the concept that changes in gastric wall tension without simultaneous changes in elongation are sufficient to activate the brain-gut axis. This finding is also consistent with the observation that decreasing gastric tone with the 5-HT1pagonist sumatriptan also decreases sensitivity to gastric isovolumetric distension.17 ,21
If gastric wall tension seems to be an important element in the transduction of mechanical stimuli, it would be tempting to calculate absolute values for this parameter. Indeed, several authors have chosen this approach.6 ,7 ,11 ,15 We have preferred not to calculate absolute values for gastric wall tension but to measure relative changes over time of wall tension for the following reasons. In a static model of distension, circumferential wall tension can be approximated using the simplified law of Laplace (T=ΔP(r/2)). Applying this formula to the gastric wall requires a number of assumptions which are not necessarily fulfilled: the stomach has a spherical shape, the gastric wall is infinitely thin, and no active contractile activity occurs.22 Alternatively, when intraballoon volume is kept constant, isometric contractions (against an intragastric balloon with fixed volume) of the proximal stomach in close apposition to the balloon generate increases in intraballoon pressure. These changes in pressure reflect changes in gastric wall tension, and the need for calculation of absolute values of wall tension is overcome. Using this technique, we observed that spontaneous phasic changes in wall tension of the proximal stomach can indeed be perceived. Moreover, increasing the intensity and frequency of the stimulus with Ery resulted in a significant increase in the proportion of perceived contractions. Antral and duodenal contractions were most often not perceived. To date there is no evidence that Ery may influence afferent pathways at any level. Therefore, and in addition to the results obtained with the distension studies, the findings support the concept that changes in tension are sufficient to activate afferent sensorial pathways.
Logically, any change in tension or elongation must be sensed and relayed by mechanoreceptors in the gastric wall. It has been proposed that the gastric wall contains two types of mechanoreceptors.11 Mechanoreceptors arranged in a parallel fashion respond to stimuli that elongate the stomach wall; mechanoreceptors arranged in series respond to stimuli that increase the tension of the stomach wall.13 ,14 In series and in parallel mechanoreceptors in the gastric wall have been functionally identified in vitro in animal studies.23 Recently, Distrutti et al reported that gastric wall tension, measured according to the simplified law of Laplace, is determining the perception of gastric distension below the pain threshold.15 Our observations are consistent with a model in which activation of in series mechanoreceptors is sufficient to transduce perception of changes in gastric wall tension.
The findings of this study may be relevant to a better understanding of the pathophysiology and treatment of functional dyspepsia. Hypersensitivity to mechanical distension is considered an important mechanism of symptom production in functional dyspepsia. Even if dysfunction leading to hypersensitivity is located at higher levels of the brain-gut axis, mechanoreceptors in the gastric wall must be involved in the process of perception of a mechanical stimulus. Furthermore, impaired accommodation of the proximal stomach to a meal, a frequent finding in patients with functional dyspepsia,21 ,24 ,25 may increase gastric wall tension and lead to the perprandial and early postprandial symptoms associated with ingestion of meals. Fundus relaxing agents can decrease wall tension of the proximal stomach and thus may decrease symptoms.
In summary, in the present studies we have demonstrated that Ery increases tone and phasic contractile activity in the proximal stomach. Both tonic and phasic contractions are accompanied by changes in wall tension of the proximal stomach, leading to increased sensitivity to distension and enhanced perception of phasic contractions. Changes in wall tension, but not necessarily changes in elongation, of the proximal stomach are required for perception of a distending stimulus. Our observations support the hypothesis that changes in gastric wall tension may be involved in the genesis of symptoms in functional dyspepsia.
Abbreviations used in this paper
- Ery
- erythromycin
- MDP
- minimal distending pressure