Article Text

Abstract
BACKGROUND Helicobacter pylori infection is less prevalent and atrophic gastritis is less extensive in patients with reflux oesophagitis than those without it, but few studies have examined this relationship directly.
AIMS We investigated the relationship between H pylori infection, acid secretion, and reflux oesophagitis in Japanese subjects.
SUBJECTS A total of 105 patients with erosive reflux oesophagitis were compared with 105 sex and age matched patients without reflux oesophagitis.
METHODS The diagnosis of H pylori infection was made by histological examination of gastric mucosal biopsy specimens, rapid urease test, and detection of serum IgG antibodies. Acid secretion was assessed by the endoscopic gastrin test.
RESULTS H pylori infection was present in 36 patients with erosive reflux oesophagitis (34.3%) and in 80 control subjects (76.2%) (odds ratio 0.163, 95% confidence interval 0.09–0.29). Overall acid secretion was significantly greater in patients with reflux oesophagitis. AmongH pylori positive patients, acid secretion was greater in patients with reflux oesophagitis than those without oesophagitis.
CONCLUSION In Japan, erosive reflux oesophagitis occurs most often in the absence ofH pylori infection and gastric hyposecretion. Even in the presence of H pylori infection, reflux oesophagitis is more likely to develop in patients without gastric hyposecretion. H pylori infection may inhibit reflux oesophagitis by inducing hypoacidity.
- Helicobacter pylori
- gastro-oesophageal reflux disease
- reflux oesophagitis
- acid secretion
Abbreviations used in this paper
- EGT
- endoscopic gastrin test
Statistics from Altmetric.com
Regurgitation of acidic gastric contents into the oesophagus is a key mechanism of reflux oesophagitis secondary to gastro-oesophageal reflux disease.1-4 Recent studies have shown thatHelicobacter pylori infection is one of the most important factors contributing to the development of gastritis and atrophy that involves the gastric corpus.5 ,6 Our group and others have reported that H pyloriinfection was less prevalent and atrophic gastritis was less severe in patients with reflux oesophagitis than those without oesophagitis.7-9 Thus H pyloriinfection may suppress the development of reflux oesophagitis by inducing atrophic gastritis and therefore gastric hyposecretion.10 However, few studies have examined directly whether or not gastric hyposecretion caused byH pylori reduces the incidence of reflux oesophagitis.
The aim of this study was to investigate the relationship betweenH pylori infection, acid secretion, and reflux oesophagitis in Japanese subjects.
Subjects and methods
SUBJECTS
Patients who were self and physician referred to our university hospital between July 1996 and December 1998 were enrolled in the present study. The reflux oesophagitis group included 105 patients (58 men and 47 women; mean age 59.1 (13.9) years, range 18–82) who were diagnosed endoscopically as having erosive reflux oesophagitis but no other localised lesions in the upper gastrointestinal tract. The degree of reflux oesophagitis was graded from A (least severe) to D (most severe) according to the Los Angeles Classification11(grade A, 26 patients; grade B, 57 patients; grade C, 20 patients; and grade D, two patients). For each patient with oesophagitis, we randomly selected age and sex matched asymptomatic control subjects (total 105 patients; 58 men and 47 women; mean age 59.1 (13.9) years, range 18–82) from those who consulted the outpatient clinic of our university hospital during the same period and hoped to undergo endoscopic examination for screening of upper gastrointestinal diseases. These individuals showed no localised lesions in the oesophagus, stomach, or duodenum on endoscopy. They also denied a history of upper gastrointestinal diseases or symptoms related to reflux disease, including heartburn and acid regurgitation. Patients were excluded if they had taken antibiotics, H2 receptor antagonists, or proton pump inhibitors within four weeks before endoscopic examination. Informed consent was obtained from every subject. The study was approved by the Ethics Committee for Human Research of Tohoku University School of Medicine.
STUDY DESIGN
Diagnosis of H pylori infection
Biopsy specimens of the stomach were taken endoscopically from the gastric antrum and upper body along the greater curvature from all subjects for standard haematoxylin and eosin staining and rapid urease test. In addition, blood samples were obtained to determine the titre of serum IgG antibodies against H pylori. To avoid false negative results, patients were considered to beH pylori positive if one or more of the diagnostic methods applied were positive, and Hpylori negative if all methods showed negative results.
Histology
Biopsy specimens obtained from the gastric antrum and upper portion of the corpus along the greater curvature were evaluated histologically. Histological assessment was performed by two pathologists (TK and HS) independently and in a blinded manner. Using the updated Sydney system,12 the degrees of inflammation, activity, and atrophy were scored from 0 (absent) to 3 (most severe). The inflammation score and activity scores were summed and expressed as the gastritis score.
Gastric acid secretion
Detailed procedures for the endoscopic gastrin test (EGT) have been reported previously.13 Briefly, after an overnight fast, subjects were injected intramuscularly with tetragastrin (Gastopsin; Nippon Kayaku, Tokyo, Japan) 4 μg/kg before endoscopy. Endoscopy was begun about 15 minutes after tetragastrin injection. After the endoscope entered the stomach, pooled gastric fluid was aspirated and discarded. Gastric fluid secreted between 20 and 30 minutes after tetragastrin injection was aspirated and collected under direct visualisation during routine endoscopic examination of the stomach and duodenal bulb. Biopsy specimens were then taken when indicated, and the endoscope was removed. The volume of sample collected over the 10 minute period was recorded, and its H+ concentration was determined by titration. Acid output in the 10 minute period was calculated by multiplying the volume by the H+ concentration, and the EGT value was expressed as H+ mEq/10 minutes. We have shown previously that the EGT value correlated very closely with peak acid output determined by the conventional method (correlation coefficient 0.92) and showed high reproducibility (coefficient of variation 5.6%).
STATISTICAL ANALYSIS
Results are expressed as mean (SD). For statistical analysis, the χ2 test or the Mann-Whitney U test was used; p values <0.01 were considered statistically significant.
Results
H PYLORI INFECTION
Table 1 shows H pylori infection diagnosed by histology, rapid urease test, and IgG antibodies againstH pylori. In this study, subjects who showed serologically positive results were also positive in other tests.H pylori infection was diagnosed in 36 of 105 patients with erosive reflux oesophagitis (34.3%) and in 80 of 105 matched control subjects (76.2%). The prevalence of infection was significantly lower in patients with reflux oesophagitis than in control subjects (odds ratio 0.163, 95% confidence interval 0.09–0.29; p<0.01, χ2 test).
Diagnosis of Helicobacter pylori infection
HISTOLOGY
The atrophy score of the antrum assessed by the updated Sydney system was significantly lower in patients with reflux oesophagitis than in control subjects (0.52 (0.86) v 1.20 (0.98); p<0.01, Mann-Whitney U test) (fig 1A). Similarly, the atrophy score of the gastric body was significantly lower in patients with reflux oesophagitis than in controls (0.09 (0.29)v 0.54 (0.89); p<0.01, Mann-Whitney U test) (fig 1A). Then, the reflux oesophagitis patients and control subjects were divided into two groups according to the presence (H pylori positive, n=116) or absence (H pylori negative, n=94) of infection, and the pattern of atrophy scores was compared. The atrophy score of the antrum in H pylori negative subjects was not different between the reflux oesophagitis and control groups but the score in H pylori positive subjects was significantly lower in the reflux oesophagitis group than in the control group (0.97 (0.90) v 1.59 (0.81); p<0.01, Mann-Whitney U test) (fig 2B). Similarly, the atrophy score of the gastric body in H pylori negative subjects was not different between the two groups but the score in theH pylori positive subjects was significantly lower in the oesophagitis group than in the control group (0.21 (0.41)v 0.72 (0.96); p<0.01, Mann-Whitney U test) (fig 1B).
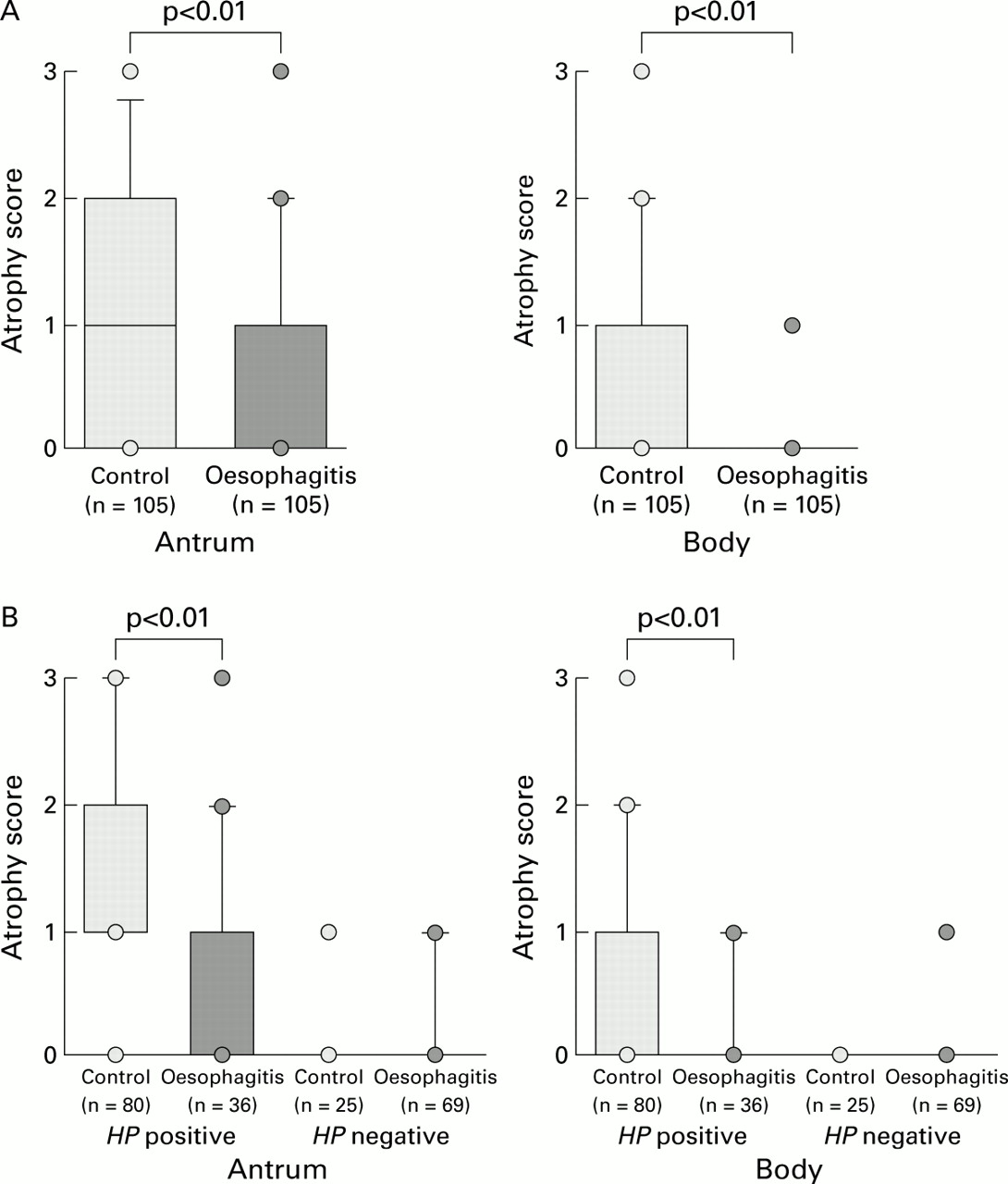
(A) Atrophy scores in the antrum (left) and body (right) assessed by the updated Sydney system were significantly lower in patients with reflux oesophagitis than in control subjects (antrum 0.52 (0.86) v 1.20 (0.98), p<0.01; body 0.09 (0.29) v 0.54 (0.89), p<0.01 by Mann-Whitney U test). (B) Atrophy scores of both the antrum (left) and body (right) were not different between the reflux oesophagitis and control groups among the Helicobacter pylori (HP) negative subjects while they were significantly lower in the former than the latter when compared in HP positive individuals (antrum 0.97 (0.90) v 1.59 (0.81), p<0.01; body 0.21 (0.41) v 0.72 (0.96), p<0.01 by Mann-Whitney U test).

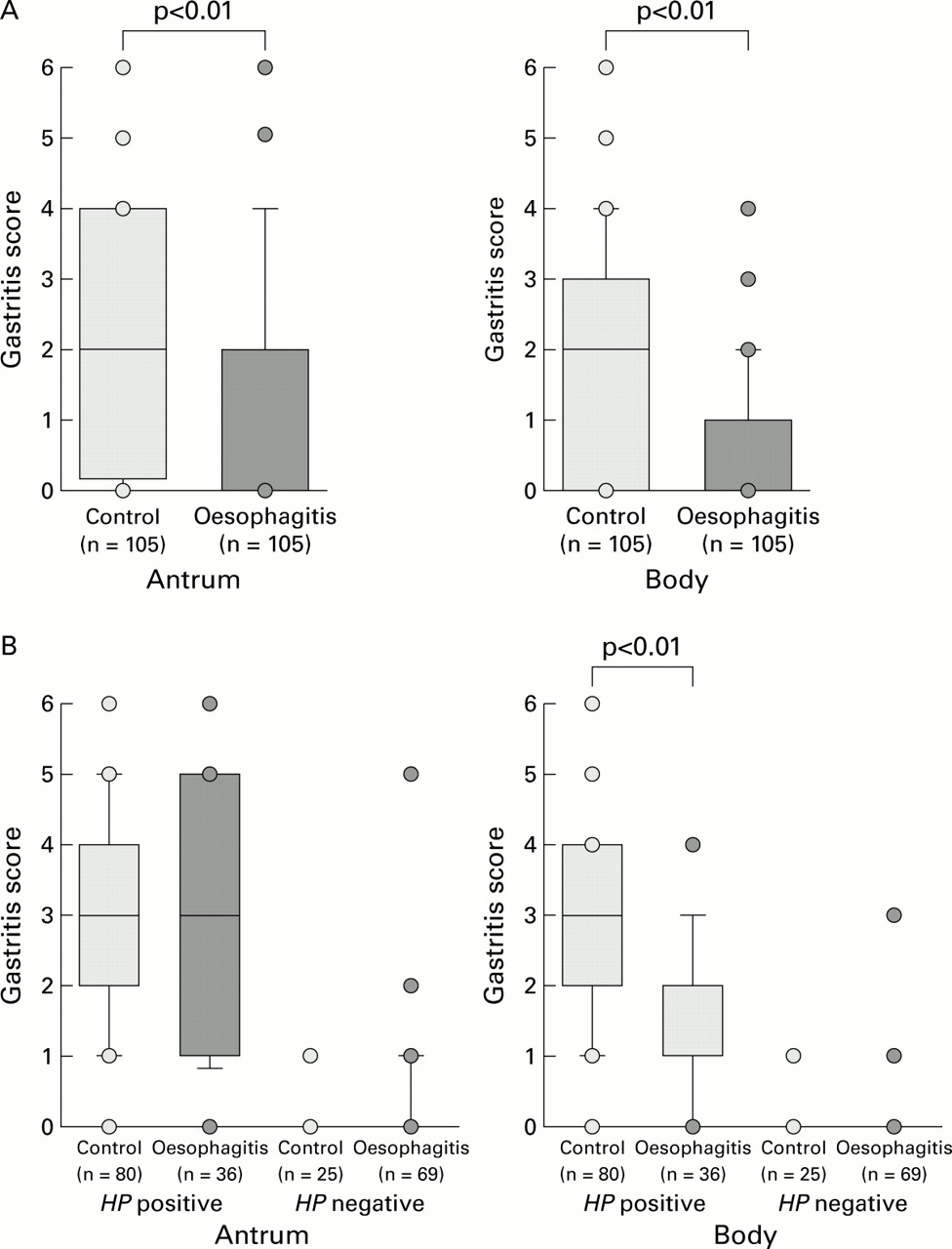
(A) Gastritis scores in the antrum (left) and the body (right) assessed by the updated Sydney system were significantly lower in patients with reflux oesophagitis than in control subjects (antrum 1.16 (1.73) v 2.20 (1.70), p<0.01; body 0.57 (1.01) v 1.98 (1.56), p<0.01 by Mann-Whitney U test). (B) Gastritis scores in the antrum (left) and body (right) were not different between the reflux oesophagitis group and control group in the Helicobacter pylori (HP) negative subjects. However, gastritis score of the corpus was significantly lower in patients with oesophagitis than in controls in HP positive subjects (1.47 (1.13) v 2.63 (1.23), p<0.01 by Mann-Whitney U test) although the difference in the antrum was not significant in the HP positive subjects.
Gastritis score of the antrum was significantly lower in patients with reflux oesophagitis than in control subjects (1.16 (1.73)v 2.20 (1.70); p<0.01, Mann-Whitney U test) (fig 2A). Similarly, the gastritis score of the gastric body was significantly lower in patients with reflux oesophagitis than in controls (0.57 (1.01) v 1.98 (1.56); p<0.01, Mann-Whitney U test) (fig 2A). Again, all oesophagitis patients and control subjects were divided into two groups according to the presence or absence of H pyloriinfection, and the pattern of gastritis scores was compared. The gastritis score of the antrum was not different between the reflux oesophagitis and control groups in both the H pylori negative and positive subjects (Mann-Whitney U test) (fig2B). On the other hand, while the gastritis score of the stomach body was not different between the oesophagitis and control groups when examined in the H pylori negative subjects, the score for the H pylori positive subjects was significantly lower in the oesophagitis group than in the control group (1.47 (1.13) v 2.63 (1.23); p<0.01, Mann-Whitney U test) (fig 2B).
GASTRIC ACID SECRETION
The EGT value was significantly higher in patients with erosive reflux oesophagitis than in control subjects (3.65 (2.17) mEq/10 minutes v 1.86 (1.77); p<0.01, Mann-Whitney U test) (fig 3A). Patients with oesophagitis and control subjects were divided into two groups according to the presence (H pylori positive, n=116) or absence (H pylori negative, n=94) ofH pylori infection, and their EGT values compared. The EGT value was not different between patients with reflux oesophagitis and control subjects when compared withH pylori negative subjects but it was significantly higher in patients with oesophagitis than in controls inH pylori positive subjects (3.08 (2.18)v 1.44 (1.70); p<0.01, Mann-Whitney U test) (fig 3B).

{kind=link}
{kind=link}
{kind=link}
(A) The endoscopic gastrin test (EGT) value was significantly higher in patients with reflux oesophagitis than in control subjects (3.65 (2.17) mEq/10 minutes v 1.86 (1.77); p<0.01 by Mann-Whitney U test). (B) The EGT value was not different between patients with and without reflux oesophagitis among the Helicobacter pylori (HP) negative individuals but it was significantly higher in patients with reflux oesophagitis than in controls in HP positive subjects (3.08 (2.18) mEq/10 minutes v 1.44 (1.70); p<0.01 by Mann-Whitney U test).
Discussion
The pathophysiology of reflux oesophagitis has been studied extensively. Important factors predisposing to this disease include the presence of hiatal hernia,14 transient relaxation of the lower oesophageal sphincter,1-4 and impaired clearance of regurgitated gastric contents in the oesophagus.15 Acidity in the oesophagus is a key factor for the pathogenesis of reflux oesophagitis, and hence effective treatments have been based on suppression of gastric acid secretion.16-18
On the other hand, recent studies have shown that H pylori infection is one of the most important causes contributing to gastritis and atrophy of the gastric corpus, resulting in gastric hyposecretion.5 ,6 Our group and others have reported that the prevalence of H pyloriinfection and the degree of atrophic gastritis were significantly lower in patients with reflux oesophagitis than control subjects.7-9 Therefore, we hypothesised thatH pylori infection may have protective effects against reflux oesophagitis through induction of gastric hyposecretion. However, few studies have examined directly the relationship between gastric hyposecretion due to H pylori infection and the risk of reflux oesophagitis. The aim of this study therefore was to examine directly gastric acid secretion andH pylori infection. Although analysis of the acidity in the oesophagus and stomach is the best method of studying the pathogenesis of gastro-oesophageal reflux disease, it is difficult to perform 24 hour pH monitoring in a large number of patients. Therefore, we used the EGT, a new technique that has been proved to be very useful for evaluating endoscopic findings and gastric acid secretion simultaneously in large numbers of patients.
We have demonstrated clearly that the prevalence ofH pylori infection was significantly lower in patients with erosive reflux oesophagitis than in age matched control subjects who did not have reflux oesophagitis. Several controlled studies have investigated this issue but the results were somewhat conflicting. Some reports found no difference in the prevalence of H pylori infection between reflux oesophagitis and those lacking upper gastrointestinal tract lesions19 ,20 while others have shown a significantly lower prevalence in patients with oesophagitis than controls.21 ,22 The discordance appeared to be caused by the different prevalence rates of H pyloriinfection in the control groups of the respective studies. In the present study, the prevalence of H pyloriinfection in control subjects was higher than that found in previous studies in Western populations but was similar to that reported previously in Japan.5 Werdmuller and Loffeld observed a significantly lower incidence of H pyloriinfection in patients with oesophagitis than control subjects but they concluded that H pylori did not play a direct or indirect role in the pathogenesis of reflux oesophagitis because the infection did not correlate with the severity of oesophagitis.21 Moreover, the authors did not evaluate the severity of gastritis or atrophy in the corpus, nor did they measure acid secretion. In the present study, the severity of gastritis and atrophy in the body were milder in the erosive reflux oesophagitis group than in the control group. Although subjects in our previous report were different from those in this study, the results ofH pylori infection and atrophic score were similar. This study has also demonstrated greater acid secretion in the reflux oesophagitis group than in the control group. A previous study in Western subjects showed that there was no difference in gastric acid secretion between patients with reflux oesophagitis and matched controls.23 One reason for the discrepancy between our results and theirs may be a difference in acid secretion between the control groups of the two studies. Gastritis and atrophy in the corpus is more common in Japanese than Western subjects because of the higher incidence of H pylori infection in Japan.5 In fact, acid secretion was not different between the reflux oesophagitis and control groups when examined inH pylori negative Japanese subjects, even in this study in Japanese patients. However, because acid secretion in our control subjects was low, overall acid secretion in patients with reflux oesophagitis was significantly higher than that of control subjects.
When the analysis was performed on the limited number of patients withH pylori infection, severity of gastritis and atrophy in the corpus was milder and acid secretion was higher in patients with reflux oesophagitis than those without oesophagitis. Although the reason for varied acid secretion in patients withH pylori infection remains unclear, differences in the strain of H pylori, including the cytotoxin associated antigen (cagA) phenotype,24 ,25 or differences in the host response would have influenced acid secretion.26-28
This study suggested that most Japanese patients with reflux oesophagitis do not have H pylori infection and therefore do not develop gastritis, atrophy of the gastric corpus, or gastric hyposecretion. In addition, even if the analysis was performed on the limited patients with H pylori infection, reflux oesophagitis tended to occur more frequently in patients with milder gastritis of the gastric body and in those with milder atrophy and consequently better preservation of acid secretion. As a result, H pylori infection could be a protective factor against the development of reflux oesophagitis.
The prevalence of H pylori infection in Japan has been found to increase with advancing age5; the incidence rises by approximately 1% per year in those born after 1950, while it is high and relatively constant (70–80%) in those born before 1950. A decreased prevalence of H pylori due to the westernised life style and eradication ofH pylori in Japan will eventually lead to a reduction in the prevalence of gastric hyposecretion.
Although reflux oesophagitis in Japan is, at present, less common and milder than that in Western countries,29 our data predict that a future decrease in the prevalence of H pylori may ultimately result in increases in the prevalence and severity of reflux oesophagitis in our country.
In summary, the present study confirmed that the prevalence ofH pylori infection is significantly lower in patients with erosive reflux oesophagitis than control subjects, and that acid secretion is significantly higher in patients with erosive reflux oesophagitis. Thus, H pyloriinfection and the consequent gastric hyposecretion may be important for preventing the development of erosive reflux oesophagitis.
Abbreviations used in this paper
- EGT
- endoscopic gastrin test
References
Linked Articles
- Commentary